Suboptimal Serum 25-Hydroxy-Vitamin D Is Associated with a History of Recent Disease Exacerbation in Pediatric Patients with Bronchial Asthma or Asthma-Suggestive Recurrent Wheezing

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
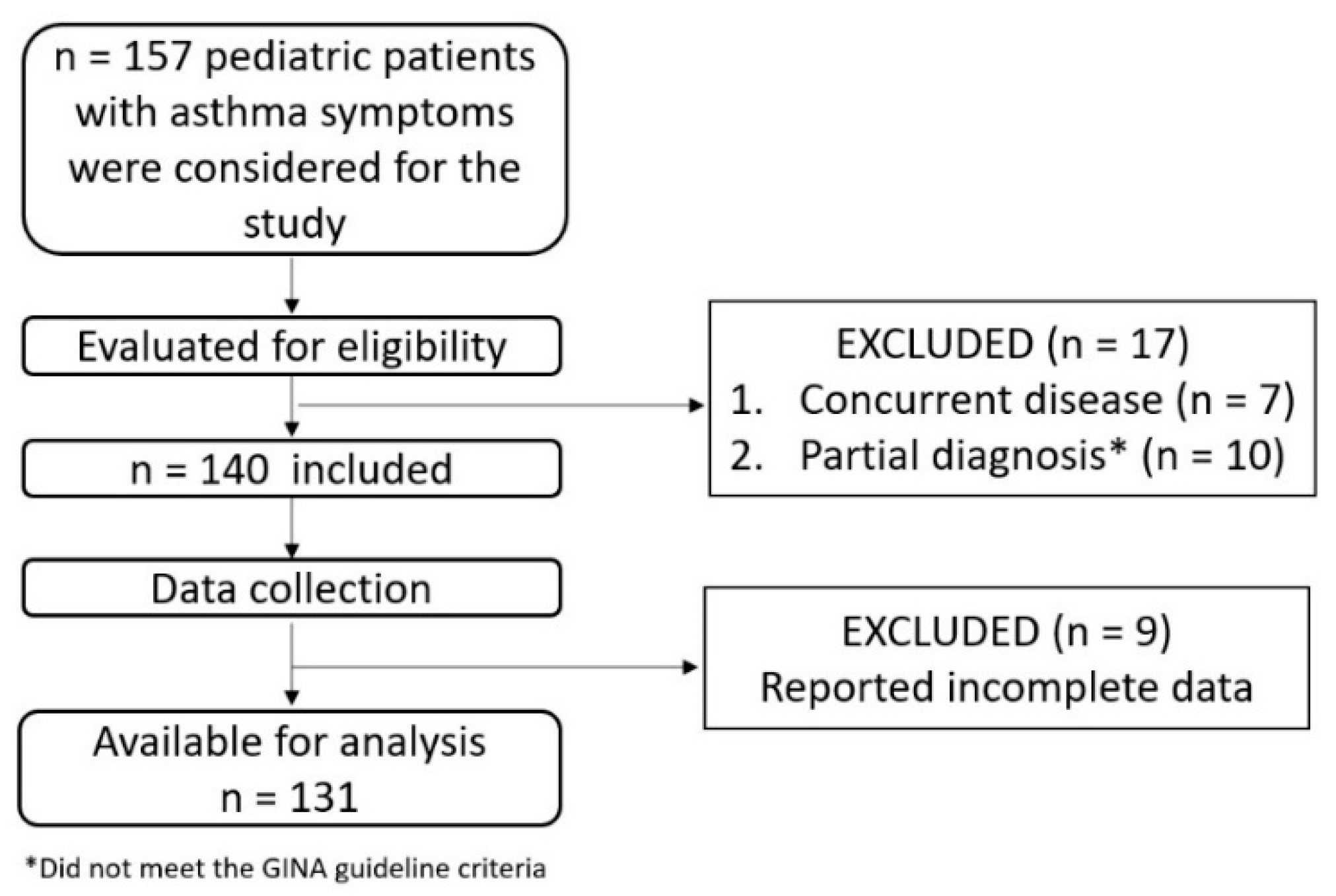
3.1. Characteristics of the Studied Cohort and Prevalence of Suboptimal Vitamin D Level
3.2. Associations Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Serebrisky, D.; Wiznia, A. Pediatric Asthma: A Global Epidemic. Ann. Glob. Health 2019, 85, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallol, J.; Crane, J.; von Mutius, E.; Odhiambo, J.; Keil, U.; Stewart, A. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: A Global Synthesis. Allergol. Immunopathol. (Madr) 2013, 41, 73–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masoli, M.; Fabian, D.; Holt, S.; Beasley, R. The Global Burden of Asthma: Executive Summary of the GINA Dissemination Committee Report. Allergy Eur. J. Allergy Clin. Immunol. 2004, 59, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Raedler, D.; Schaub, B. Immune Mechanisms and Development of Childhood Asthma. Lancet Respir. Med. 2014, 2, 647–656. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2015, 96, 365–408. [Google Scholar] [CrossRef]
- Saggese, G.; Vierucci, F.; Boot, A.M.; Czech-Kowalska, J.; Weber, G.; Camargo, C.A.; Mallet, E.; Fanos, M.; Shaw, N.J.; Holick, M.F. Vitamin D in Childhood and Adolescence: An Expert Position Statement. Eur. J. Pediatr. 2015, 174, 565–576. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, J.; DeLuca, H.F. Where Is the Vitamin D Receptor? Arch. Biochem. Biophys. 2012, 523, 123–133. [Google Scholar] [CrossRef]
- Gil, Á.; Plaza-Diaz, J.; Mesa, M.D. Vitamin D: Classic and Novel Actions. Ann. Nutr. Metab. 2018, 72, 87–95. [Google Scholar] [CrossRef]
- Ramos-Martínez, E.; López-Vancell, M.R.; de Córdova-Aguirre, J.C.F.; Rojas-Serrano, J.; Chavarría, A.; Velasco-Medina, A.; Velázquez-Sámano, G. Reduction of Respiratory Infections in Asthma Patients Supplemented with Vitamin D Is Related to Increased Serum IL-10 and IFNγ Levels and Cathelicidin Expression. Cytokine 2018, 108, 239–246. [Google Scholar] [CrossRef]
- Oddy, W.H.; de Klerk, N.H.; Sly, P.D.; Holt, P.G. The Effects of Respiratory Infections, Atopy, and Breastfeeding on Childhood Asthma. Eur. Respir. J. 2002, 19, 899–905. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, P.E.; Chen, Y.H.; Woszczek, G.; Matthews, N.C.; Chevretton, E.; Gupta, A.; Saglani, S.; Bush, A.; Corrigan, C.; Cousins, D.J.; et al. Vitamin D Enhances Production of Soluble ST2, Inhibiting the Action of IL-33. J. Allergy Clin. Immunol. 2015, 135, 824–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saggese, G.; Vierucci, F.; Prodam, F.; Cardinale, F.; Cetin, I.; Chiappini, E.; De Angelis, G.L.; Massari, M.; Del Giudice, E.M.; Del Giudice, M.M.; et al. Vitamin D in Pediatric Age: Consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, Jointly with the Italian Federation of Pediatricians. Ital. J. Pediatr. 2018, 44, 1–40. [Google Scholar] [CrossRef] [Green Version]
- Mo, M.; Wang, S.; Chen, Z.; Muyiduli, X.; Wang, S.; Shen, Y.; Shao, B.; Li, M.; Chen, D.; Chen, Z.; et al. A Systematic Review and Meta-Analysis of the Response of Serum 25-Hydroxyvitamin D Concentration to Vitamin D Supplementation from RCTs from around the Globe. Eur. J. Clin. Nutr. 2019, 73, 816–834. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L.; Drezner, M.K.; Binkley, N.C. Circulating Vitamin D3 and 25-Hydroxyvitamin D in Humans: An Important Tool to Define Adequate Nutritional Vitamin D Status. J. Steroid Biochem. Mol. Biol. 2007, 103, 631–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazahery, H.; von Hurst, P.R. Factors Affecting 25-Hydroxyvitamin D Concentration in Response to Vitamin D Supplementation. Nutrients 2015, 7, 5111–5142. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Asthma. Global Stategy for Asthma Management and Prevention; Global Initiative for Asthma: Fontana, WI, USA, 2020; pp. 19–40, 139–161. Available online: https://ginasthma.org/wp-content/uploads/2020/04/GINA-2020-full-report_-final-_wms.pdf (accessed on 8 September 2020).
- Care, C.; Improvement, Q. PediTools Electronic Growth Chart Calculators: Applications in Clinical Care, Research, and Quality Improvement. J. Med. Internet Res. 2020, 22, e16204. [Google Scholar] [CrossRef]
- Licari, A.; Marseglia, G.L.; Ciprandi, G. Vitamin D3 in Children with Allergic Asthma in Clinical Practice. Pediatr. Pulmonol. 2019, 54, 225–227. [Google Scholar] [CrossRef]
- Bose, S.; Diette, G.B.; Woo, H.; Koehler, K.; Romero, K.; Rule, A.M.; Detrick, B.; Brigham, E.; McCormack, M.C.; Hansel, N.N. Vitamin D Status Modifies the Response to Indoor Particulate Matter in Obese Urban Children with Asthma. J. Allergy Clin. Immunol. Pract. 2019, 7, 1815–1822. [Google Scholar] [CrossRef]
- Özdoğan, Ş. Seasonal, Sex Variations in Vitamin d Levels and Their Association with Pulmonary Function in Children with Asthma. Turk. J. Med. Sci. 2019, 49, 1534–1539. [Google Scholar] [CrossRef]
- Peçanha, M.B.; Freitas, R.B.; Moreira, T.R.; Silva, L.S.; de Oliveira, L.L.; Cardoso, S.A. Prevalence of Vitamin D Deficiency and Its Relationship with Factors Associated with Recurrent Wheezing. J. Bras. Pneumol. 2019, 45, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Chirita-Emandi, A.; Socolov, D.; Haivas, C.; Calapiş, A.; Gheorghiu, C.; Puiu, M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS ONE 2015, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Pittaway, J.K.; Ahuja, K.D.K.; Beckett, J.M.; Bird, M.L.; Robertson, I.K.; Ball, M.J. Make Vitamin D While the Sun Shines, Take Supplements When It Doesn′t: A Longitudinal, Observational Study of Older Adults in Tasmania, Australia. PLoS ONE 2013, 8, e59063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmlund-Suila, E.; Koskivirta, P.; Metso, T.; Andersson, S.; Mäkitie, O.; Viljakainen, H.T. Vitamin D Deficiency in Children with a Chronic Illness-Seasonal and Age-Related Variations in Serum 25-Hydroxy Vitamin D Concentrations. PLoS ONE 2013, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mavroeidi, A.; Aucott, L.; Black, A.J.; Fraser, W.D.; Reid, D.M.; Macdonald, H.M. Seasonal Variation in 25(OH)D at Aberdeen (57°N) and Bone Health Indicators- Could Holidays in the Sun and Cod Liver Oil Supplements Alleviate Deficiency? PLoS ONE 2013, 8, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaykhaei, M.A.; Khodadoost, M.; Dashipour, A.R.; Haidari, Z.; Karimkoshteh, A.; Sandoughi, M. Baseline Levels Determine Magnitude of Increment in 25 Hydroxy Vitamin D Following Vitamin D3 Prescription in Healthy Subjects. Endocrine 2019, 64, 378–383. [Google Scholar] [CrossRef]
- Wu, Z.; Camargo, C.A., Jr.; Reid, I.R.; Beros, A.; Sluyter, J.D.; Waayer, D.; Lawes, C.M.M.; Toop, L.; Khaw, K.; Scragg, R. What Factors Modify the Effect of Monthly Bolus Dose Vitamin D Supplementation on 25-Hydroxyvitamin D Concentrations? J. Steroid Biochem. Mol. Biol. 2020, 201, 105687. [Google Scholar] [CrossRef] [PubMed]
- Searing, D.A.; Zhang, Y.; Murphy, J.R.; Hauk, P.J.; Goleva, E.; Leung, D.Y.M. Decreased Serum Vitamin D Levels in Children with Asthma Are Associated with Increased Corticosteroid Use. J. Allergy Clin. Immunol. 2010, 125, 995–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solidoro, P.; Bellocchia, M.; Aredano, I.; Mattei, A.; Pivetta, E.; Patrucco, F.; Boita, M.; de Blasio, F.; Brussino, L.; Rolla, G.; et al. Asthmatic Patients with Vitamin D Deficiency Have Decreased Exacerbations after Vitamin Replacement. Nutrients 2017, 9, 1234. [Google Scholar] [CrossRef] [Green Version]
- Martineau, A.R.; Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Griffiths, C.J.; Camargo, C.A.; Kerley, C.P.; Jensen, M.E.; Mauger, D.; Stelmach, I.; et al. Vitamin D Supplementation to Prevent Asthma Exacerbations: A Systematic Review and Meta-Analysis of Individual Participant Data. Lancet Respir. Med. 2017, 5, 881–890. [Google Scholar] [CrossRef] [Green Version]
- Hata, M.D.T.R.; Kotol, B.S.P.; Jackson, M.D.M.; Nguyen, B.S.M.; Paik, M.D.A.; Don Udall, M.D.; Kanada, B.S.K.; Yamasaki, M.D.K.; Alexandrescu, M.D.; Richard, L.; et al. Administration of Oral Vitamin D Induces Cathelicidin Production in Atopic Individuals. J. Allergy Clin. Immunol. 2008, 122, 829–831. [Google Scholar] [CrossRef] [Green Version]
- Reinehr, T.; Langrock, C.; Hamelmann, E.; Lücke, T.; Koerner-Rettberg, C.; Holtmann, M.; Legenbauer, T.; Gest, S.; Frank, M.; Schmidt, B.; et al. 25-Hydroxvitamin D Concentrations Are Not Lower in Children with Bronchial Asthma, Atopic Dermatitis, Obesity, or Attention-Deficient/Hyperactivity Disorder than in Healthy Children. Nutr. Res. 2018, 52, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Hon, K.L.; Kong, A.P.; Pong, H.N.S.; Wong, G.W.H.; Leung, T.F.K. Vitamin D Deficiency Is Associated with Diagnosis and Severity of Childhood Atopic Dermatitis. Pediatr. Allergy Immunol. 2014, 25, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Schünemann, H.J.; Samolinski, B.; Demoly, P.; Baena-Cagnani, C.E.; Bachert, C.; Bonini, S.; Boulet, L.P.; Bousquet, P.J.; Brozek, J.L.; et al. Allergic Rhinitis and Its Impact on Asthma (ARIA): Achievements in 10 Years and Future Needs. J. Allergy Clin. Immunol. 2012, 130, 1049–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Cara, G.; Carelli, A.; Latini, A.; Panfili, E.; Bizzarri, I.; Ciprandi, G.; Buttafava, S.; Frati, F.; Verrotti, A. Severity of Allergic Rhinitis and Asthma Development in Children. World Allergy Organ. J. 2015, 8, 6–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sears, M.R. Predicting Asthma Outcomes. J. Allergy Clin. Immunol. 2015, 136, 829–836. [Google Scholar] [CrossRef] [Green Version]
- Aryan, Z.; Rezaei, N.; Camargo, C.A. Vitamin D Status, Aeroallergen Sensitization, and Allergic Rhinitis: A Systematic Review and Meta-Analysis. Int. Rev. Immunol. 2017, 36, 41–53. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, K.W.; Kim, M.J.; Sol, I.S.; Yoon, S.H.; Ahn, H.S.; Kim, H.J.; Sohn, M.H.; Kim, K.E. Vitamin D Levels in Allergic Rhinitis: A Systematic Review and Meta-Analysis. Pediatr. Allergy Immunol. 2016, 27, 580–590. [Google Scholar] [CrossRef]
- Castro-Rodríguez, J.A.; Holberg, C.J.; Wright, A.L.; Martinez, F.D. A Clinical Index to Define Risk of Asthma in Young Children with Recurrent Wheezing. Am. J. Respir. Crit. Care Med. 2000, 162, 1403–1406. [Google Scholar] [CrossRef] [Green Version]
- Vasiliou, J.E.; Lui, S.; Walker, S.A.; Chohan, V.; Xystrakis, E.; Bush, A.; Hawrylowicz, C.M.; Saglani, S.; Lloyd, C.M. Vitamin D Deficiency Induces Th2 Skewing and Eosinophilia in Neonatal Allergic Airways Disease. Allergy Eur. J. Allergy Clin. Immunol. 2014, 69, 1380–1389. [Google Scholar] [CrossRef] [Green Version]
- De Groot, J.C.; Van Roon, E.N.H.; Storm, H.; Veeger, N.J.G.M.; Zwinderman, A.H.; Hiemstra, P.S.; Bel, E.H.D.; Brinke, A.T. Vitamin D Reduces Eosinophilic Airway Inflammation in Nonatopic Asthma. J. Allergy Clin. Immunol. 2015, 135, 670–675. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Kilpin, K.; MacLaughlin, B.D.; Greiller, C.L.; Hooper, R.L.; Barnes, N.C.; Timms, P.M.; Rajakulasingam, R.K.; Bhowmik, A.; Choudhury, A.B.; et al. Prevalence, Determinants and Clinical Correlates of Vitamin D Deficiency in Adults with Inhaled Corticosteroid-Treated Asthma in London, UK. J. Steroid Biochem. Mol. Biol. 2018, 175, 88–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doǧru, M.; Seren, L.P. Serum 25-Hydroxyvitamin D Levels in Children with Recurrent Wheezing and Relation to the Phenotypes and Frequency of Wheezing. Eur. Ann. Allergy Clin. Immunol. 2017, 49, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lama, M.; Chatterjee, M.; Chaudhuri, T.K. Total Serum Immunoglobulin e in Children with Asthma. Indian J. Clin. Biochem. 2013, 28, 197–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, I.; Alhossan, A.; Lee, C.S.; Kutbi, H.; MacDonald, K. “Real-Life” Effectiveness Studies of Omalizumab in Adult Patients with Severe Allergic Asthma: Systematic Review. Allergy Eur. J. Allergy Clin. Immunol. 2016, 71, 593–610. [Google Scholar] [CrossRef] [PubMed]
- James, J.; Weaver, V.; Cantorna, M.T. Control of Circulating IgE by the Vitamin D Receptor In Vivo Involves B Cell Intrinsic and Extrinsic Mechanisms. J. Immunol. 2017, 198, 1164–1171. [Google Scholar] [CrossRef] [Green Version]
- Sandhu, M.S.; Casale, T.B. The Role of Vitamin D in Asthma. Ann. Allergy, Asthma Immunol. 2010, 105, 191–199. [Google Scholar] [CrossRef]
- Brehm, J.M.; Celedón, J.C.; Soto-Quiros, M.E.; Avila, L.; Hunninghake, G.M.; Forno, E.; Laskey, D.; Sylvia, J.S.; Hollis, B.W.; Weiss, S.T.; et al. Serum Vitamin D Levels and Markers of Severity of Childhood Asthma in Costa Rica. Am. J. Respir. Crit. Care Med. 2009, 179, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Simpson, A.; Soderstrom, L.; Ahlstedt, S.; Murray, C.S.; Woodcock, A.; Custovic, A. IgE Antibody Quantification and the Probability of Wheeze in Preschool Children. J. Allergy Clin. Immunol. 2005, 116, 744–749. [Google Scholar] [CrossRef]
- Nwosu, B.U.; Kum-Nji, P. Tobacco Smoke Exposure Is an Independent Predictor of Vitamin D Deficiency in US Children. PLoS ONE 2018, 13, 1–12. [Google Scholar] [CrossRef]
- Chinellato, I.; Piazza, M.; Sandri, M.; Paiola, G.; Tezza, G.; Boner, A.L. Correlation between Vitamin D Serum Levels and Passive Smoking Exposure in Children with Asthma. Allergy Asthma Proc. 2018, 39, e8–e14. [Google Scholar] [CrossRef]
- Protano, C.; Andreoli, R.; Mutti, A.; Manigrasso, M.; Avino, P.; Vitali, M. Reference Intervals for Urinary Cotinine Levels and the Influence of Sampling Time and Other Predictors on Its Excretion among Italian Schoolchildren. Int. J. Environ. Res. Public Health 2018, 15, 817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, S.H.; Fenton, T.R.; Noseworthy, M.; Anselmo, M. Adequate Vitamin D Intake but Low Serum Levels in Pediatric Asthma Patients: A Pilot Study, Alberta Children’s Hospital. Can. Respir. J. 2016, 2016, 6982010. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Age | Gender | Residence | Premature Birth | |||||
|---|---|---|---|---|---|---|---|---|
| <5 Years | ≥5 Years | Female | Male | Urban | Rural | Yes | No | |
| n | 70 | 61 | 60 | 71 | 99 | 32 | 24 | 107 |
| % | 53.4 | 46.6 | 45.8 | 54.2 | 75.6 | 24.4 | 18.3 | 81.7 |
| Question | Suboptimal Serum 25-OH-VitD n = 77 | Optimal Serum 25-OH-VitD n = 54 | p Value |
|---|---|---|---|
| Vitamin D3 supplementation in infancy | 83.1% (64/77) | 90.7% (49/54) | 0.21 |
| Vitamin D3 supplementation in the cold season | 75.3% (58/77) | 88.8% (48/54) | 0.052 |
| Parental smoking | 32.4% (25/77) | 37% (20/54) | 0.58 |
| Personal history of atopic dermatitis | 54.5% (42/77) | 61.1% (33/54) | 0.45 |
| Personal history of seasonal allergic rhinitis | 38.5% (22/77) | 14.8% (8/54) | 0.06 |
| Elevated-for-age group serum IgE 1 | 44.1% (34/77) | 57.4% (31/54) | 0.13 |
| Eosinophil count >4% of total white blood count 1 | 31.1% (24/77) | 27.7% (15/54) | 0.23 |
| Hospitalization for asthma attack 2 | 22.0% (17/77) | 11.1% (6/54) | 0.1 |
| Oral corticosteroids for exacerbation therapy 2 | 37.6% (29/77) | 27.7% (15/54) | 0.23 |
| Recent asthma exacerbation 3 | 61.0% (47/77) | 40.7% (22/54) | 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adam-Bonci, T.-I.; Cherecheș-Panța, P.; Bonci, E.-A.; Man, S.C.; Cutaș-Benedec, A.; Drugan, T.; Pop, R.M.; Irimie, A. Suboptimal Serum 25-Hydroxy-Vitamin D Is Associated with a History of Recent Disease Exacerbation in Pediatric Patients with Bronchial Asthma or Asthma-Suggestive Recurrent Wheezing. Int. J. Environ. Res. Public Health 2020, 17, 6545. https://doi.org/10.3390/ijerph17186545
Adam-Bonci T-I, Cherecheș-Panța P, Bonci E-A, Man SC, Cutaș-Benedec A, Drugan T, Pop RM, Irimie A. Suboptimal Serum 25-Hydroxy-Vitamin D Is Associated with a History of Recent Disease Exacerbation in Pediatric Patients with Bronchial Asthma or Asthma-Suggestive Recurrent Wheezing. International Journal of Environmental Research and Public Health. 2020; 17(18):6545. https://doi.org/10.3390/ijerph17186545
Chicago/Turabian StyleAdam-Bonci, Teodora-Irina, Paraschiva Cherecheș-Panța, Eduard-Alexandru Bonci, Sorin Claudiu Man, Ancuța Cutaș-Benedec, Tudor Drugan, Raluca Maria Pop, and Alexandru Irimie. 2020. "Suboptimal Serum 25-Hydroxy-Vitamin D Is Associated with a History of Recent Disease Exacerbation in Pediatric Patients with Bronchial Asthma or Asthma-Suggestive Recurrent Wheezing" International Journal of Environmental Research and Public Health 17, no. 18: 6545. https://doi.org/10.3390/ijerph17186545