The Association between Parental Involvement Behavior and Self-Esteem among Adolescents Living in Poverty: Results from the K-CHILD Study


Abstract
:1. Introduction
2. Materials and Methods
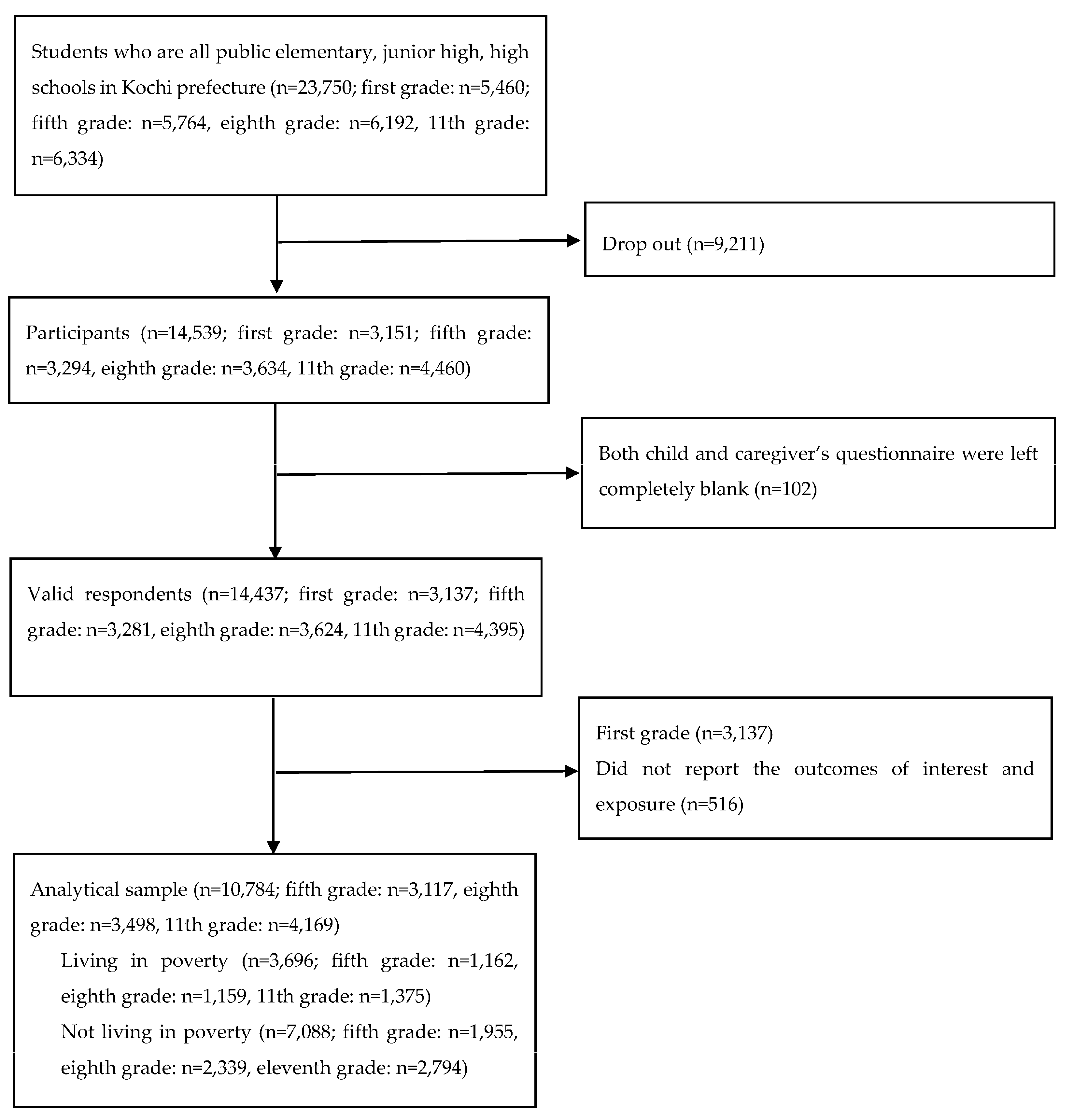
2.1. Participants
2.2. Measurements
2.2.1. Child Poverty
2.2.2. Parental Involvement Behaviors
2.2.3. Self-Esteem
2.2.4. Covariates
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants in This Study
3.2. Distribution of Parental Involvement Behaviors
3.3. Association between Parental Involvement Behaviors and Self-Esteem among Adolescents Living in Poverty and not Living in Poverty
3.4. Association between Parental Interaction with Child and Self-Esteem among Adolescents Living in Poverty and not Living in Poverty
3.5. Association between Parental Care for Child’s Physical Health and Self-Esteem among Adolescents Living in Poverty and not Living in Poverty
3.6. Comparison among Effect Size of Parental Interaction with Child and Parental Care for Child’s Physical Health
3.7. Interaction between Poverty and Paretal Involvement Behaviors
3.8. Association between Each Parental Involvement Behaviors and Self-Esteem among Adolescents Living in Poverty and not Living in Poverty
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- OECD. Child Poverty; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Sasaki, M.; Yoshida, K.; Adachi, Y.; Furukawa, M.; Itazawa, T.; Odajima, H.; Akasawa, A. Environmental factors associated with childhood eczema: Findings from a national web-based survey. Allergol. Int. 2016, 65, 420–424. [Google Scholar] [CrossRef] [Green Version]
- Lynch, S.V.; Wood, R.A.; Boushey, H.; Bacharier, L.B.; Bloomberg, G.R.; Kattan, M.; O’Connor, G.T.; Sandel, M.T.; Calatroni, A.; Matsui, E.; et al. Effects of early-life exposure to allergens and bacteria on recurrent wheeze and atopy in urban children. J. Allergy Clin. Immunol. 2014, 134, 593–601.e2. [Google Scholar] [CrossRef] [Green Version]
- Amemiya, A.; Fujiwara, T. Association of low family income with lung function among children and adolescents: Results of the J-SHINE study. J. Epidemiol. 2018, 29, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Angulo, E.K.; Hobdell, M.H.; Bernabe, E. Poverty, social exclusion and dental caries of 12-year-old children: A cross-sectional study in Lima, Peru. BMC Oral Health 2009, 9, 16. [Google Scholar] [CrossRef] [Green Version]
- Peres, M.A.; de Oliveira Latorre Mdo, R.; Sheiham, A.; Peres, K.G.; Barros, F.C.; Hernandez, P.G.; Maas, A.M.; Romano, A.R.; Victora, C.G. Social and biological early life influences on severity of dental caries in children aged 6 years. Community Dent. Oral Epidemiol. 2005, 33, 53–63. [Google Scholar] [CrossRef]
- Tanaka, K.; Miyake, Y.; Sasaki, S.; Hirota, Y. Socioeconomic status and risk of dental caries in Japanese preschool children: The Osaka Maternal and child health study. J. Public Health Dent. 2013, 73, 217–223. [Google Scholar] [CrossRef]
- Slade, G.D.; Sanders, A.E. Two decades of persisting income-disparities in dental caries among U.S. children and adolescents. J. Public Health Dent. 2018, 78, 187–191. [Google Scholar] [CrossRef]
- Fujiwara, T. Socioeconomic status and the risk of suspected autism spectrum disorders among 18-month-old toddlers in Japan: A population-based study. J. Autism Dev. Disord. 2014, 44, 1323–1331. [Google Scholar] [CrossRef]
- Arat, A.; Norredam, M.; Baum, U.; Jonsson, S.H.; Gunlaugsson, G.; Wallby, T.; Hjern, A. Organisation of preventive child health services: Key to socio-economic equity in vaccine uptake? Scand. J. Public Health 2020, 48, 491–494. [Google Scholar] [CrossRef]
- Klevens, R.M.; Luman, E.T. US children living in and near poverty: Risk of vaccine-preventable diseases. Am. J. Prev. Med. 2001, 20, 41–46. [Google Scholar] [CrossRef]
- Nagaoka, K.; Fujiwara, T. mpact of subsidies and socioeconomic status on Varicella Vaccination in greater Tokyo, Japan. Front. Pediatr. 2016, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- Sakai, Y. The Vaccination Kuznets Curve: Do vaccination rates rise and fall with income? J. Health Econ. 2018, 57, 195–205. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kondo, K.; Shirai, K.; Suzuki, K.; Kawachi, I. Associations of childhood socioeconomic status and adulthood height with functional limitations among Japanese older people: Results from the JAGES 2010 Project. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Gilman, S.E.; Kawachi, I.; Fitzmaurice, G.M.; Buka, S.L. Family disruption in childhood and risk of adult depression. Am. J. Psychiatry 2003, 160, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Dekhtyar, S.; Wang, H.X.; Scott, K.; Goodman, A.; Koupil, I.; Herlitz, A. A life-course study of cognitive reserve in dementia—From childhood to old age. Am. J. Geriatr. Psychiatry 2015, 23, 885–896. [Google Scholar] [CrossRef] [Green Version]
- Tani, Y.; Fujiwara, T.; Kondo, N.; Noma, H.; Sasaki, Y.; Kondo, K. Childhood socioeconomic status and onset of depression among Japanese older adults: The JAGES prospective cohort study. Am. J. Geriatr. Psychiatry 2016, 24, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Doi, S.; Fujiwara, T.; Isumi, A.; Ochi, M. Pathway of the association between child poverty and low self-esteem: Results from a population-based study of adolescents in Japan. Front. Psychol. 2019, 10, 937. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Bassett, S.M.; Takahashi, L.; Voisin, D.R. What does self-esteem have to do with behavioral health among low-income youth in Chicago? J. Youth Stud. 2018, 21, 999–1010. [Google Scholar] [CrossRef]
- Donnellan, M.B.; Trzesniewski, K.H.; Robins, R.W. Self-esteem: Enduring issues and controversies. In Handbook of Individual Differences; Chamorro-Premuzic, S., Stumm, V., Furnham, A., Eds.; Wiley-Blackwell: New York, NY, USA, 2011; pp. 718–746. [Google Scholar]
- Hedayati, S.S.; Yalamanchili, V.; Finkelstein, F.O. A practical approach to the treatment of depression in patients with chronic kidney disease and end-stage renal disease. Kidney Int. 2012, 81, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Mann, M.; Hosman, C.M.; Schaalma, H.P.; De Vries, N.K. Self-esteem in a broad-spectrum approach for mental health promotion. Health Educ. Res. 2004, 19, 357–372. [Google Scholar] [CrossRef] [Green Version]
- Poorgholami, F.; Javadpour, S.; Saadatmand, V.; Jahromi, M.K. Effectiveness of Self-Care Education on the Enhancement of the Self-Esteem of Patients Undergoing Hemodialysis. Glob. J. Health Sci. 2015, 8, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Claro, S.; Paunesku, D.; Dweck, C.S. Growth mindset tempers the effects of poverty on academic achievement. Proc. Natl. Acad. Sci. USA 2016, 113, 8664–8668. [Google Scholar] [CrossRef] [Green Version]
- Hair, N.L.; Hanson, J.L.; Wolfe, B.L.; Pollak, S.D. Association of Child Poverty, Brain Development, and Academic Achievement. JAMA Pediatr. 2015, 169, 822–829. [Google Scholar] [CrossRef]
- Sirin, S.R. Socioeconomic status and academic achievement: A meta-analytic review of research. Rev. Educ. Res. 2005, 75, 417–453. [Google Scholar] [CrossRef] [Green Version]
- Sowislo, J.F.; Orth, U. Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychol. Bull. 2013, 139, 213–240. [Google Scholar] [CrossRef]
- Steiger, A.E.; Allemand, M.; Robins, R.W.; Fend, H.A. Low and decreasing self-esteem during adolescence predict adult depression two decades later. J. Pers. Soc. Psychol. 2014, 106, 325–338. [Google Scholar] [CrossRef]
- Van Tuijl, L.A.; de Jong, P.J.; Sportel, B.E.; de Hullu, E.; Nauta, M.H. Implicit and explicit self-esteem and their reciprocal relationship with symptoms of depression and social anxiety: A longitudinal study in adolescents. J. Behav. Ther. Exp. Psychiatry 2014, 45, 113–121. [Google Scholar] [CrossRef]
- McGee, R.O.B.; Williams, S. Does low self-esteem predict health compromising behaviours among adolescents? J. Adolesc. 2000, 23, 569–582. [Google Scholar] [CrossRef]
- Trzesniewski, K.H.; Donnellan, M.B.; Moffitt, T.E.; Robins, R.W.; Poulton, R.; Caspi, A. Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Dev. Psychol. 2006, 42, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Duncan, G.J.; Ziol-Guest, K.M.; Kalil, A. Early-childhood poverty and adult attainment, behavior, and health. Child Dev. 2010, 81, 306–325. [Google Scholar] [CrossRef]
- Raphael, D. Poverty in childhood and adverse health outcomes in adulthood. Maturitas 2011, 69, 22–26. [Google Scholar] [CrossRef]
- Conger, R.D.; Conger, K.J.; Elder, G.H., Jr.; Lorenz, F.O.; Simons, R.L.; Whitbeck, L.B. A family process model of economic hardship and adjustment of early adolescent boys. Child Dev. 1992, 63, 526–541. [Google Scholar] [CrossRef]
- Krauss, S.; Orth, U.; Robins, R.W. Family environment and self-esteem development: A longitudinal study from age 10 to 16. J. Pers. Soc. Psychol. 2020, 119, 457–478. [Google Scholar] [CrossRef]
- Yoder, K.A.; Hoyt, D.R. Family economic pressure and adolescent suicidal ideation: Application of the family stress model. Suicide Life Threat. Behav. 2005, 35, 251–264. [Google Scholar]
- Fernandez, M.A.; Butler, A.M.; Eyberg, S.M. Treatment outcome for low socioeconomic status African American families in parent-child interaction therapy: A pilot study. Child Fam. Behav. Ther. 2011, 33, 32–48. [Google Scholar] [CrossRef]
- Harris, S.E.; Fox, R.A.; Love, J.R. Early pathways therapy for young children in poverty: A randomized controlled trial. Couns. Outcome Res. Eval. 2015, 6, 3–17. [Google Scholar] [CrossRef]
- Reid, M.J.; Webster-Stratton, C.; Beauchaine, T.P. Parent training in head start: A comparison of program response among African American, Asian American, Caucasian, and Hispanic mothers. Prev. Sci. 2001, 2, 209–227. [Google Scholar] [CrossRef]
- Mattek, R.J.; Harris, S.E.; Fox, R.A. Predicting treatment success in child and parent therapy among families in poverty. J. Genet. Psychol. 2016, 177, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Timmer, S.G.; Urquiza, A.J.; Zebell, N.M.; McGrath, J.M. Parent-child interaction therapy: Application to maltreating parent-child dyads. Child Abus. Negl. 2005, 29, 825–842. [Google Scholar] [CrossRef]
- Harwood, M.D.; Eyberg, S.M. Child-directed interaction: Prediction of change in impaired mother-child functioning. J. Abnorm. Child Psychol. 2006, 34, 335–347. [Google Scholar] [CrossRef]
- Brestan, E.V.; Eyberg, S.M. Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5272 kids. J. Clin. Child Psychol. 1998, 27, 180–189. [Google Scholar] [CrossRef]
- O’Sullivan, T.A.; Robinson, M.; Kendall, G.E.; Miller, M.; Jacoby, P.; Silburn, S.R.; Oddy, W.H. A good-quality breakfast is associated with better mental health in adolescence. Public Health Nutr. 2009, 12, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Oddy, W.H.; Robinson, M.; Ambrosini, G.L.; O’Sullivan, T.A.; de Klerk, N.H.; Beilin, L.J.; Silburn, S.R.; Zubrick, S.R.; Stanley, F.J. The association between dietary patterns and mental health in early adolescence. Prev. Med. 2009, 49, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Kochi Labor Bureau. The Recent Employment Unemployed Situation; Kochi Labor Bureau: Kochi, Japan, 2016. [Google Scholar]
- Doi, S.; Fujiwara, T.; Isumi, A. Association between maternal adverse childhood experiences and child’s self-rated academic performance: Results from the K-CHILD study. Child. Abus. Negl. 2020, 104, 104478. [Google Scholar] [CrossRef]
- Doi, S.; Fujiwara, T.; Isumi, A. Association between maternal adverse childhood experiences and mental health problems in offspring: An intergenerational study. Dev. Psychopathol. 2020. [Google Scholar] [CrossRef]
- Townsend, P. Poverty in the United Kingdom: A Survey of Household Resources and Standards of Living; University of California Press: Berkeley, CA, USA, 1979. [Google Scholar]
- Nolan, B.; Whelan, C.T. Using non-monetary deprivation indicators to analyze poverty and social exclusion: Lessons from Europe? J. Policy Anal. Manag. 2010, 29, 305–325. [Google Scholar] [CrossRef]
- Nawa, N.; Isumi, A.; Fujiwara, T. Community-level social capital, parental psychological distress, and child physical abuse: A multilevel mediation analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1221–1229. [Google Scholar] [CrossRef]
- Sakurai, S. The investigation of self-consciousness in the 5th-and 6th-grade children. Jpn. J. Exp. Soc. Psychol. 1992, 32, 85–94. [Google Scholar] [CrossRef]
- Harter, S. The perceived competence scale for children. Child. Dev. 1982, 53, 87–97. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakae, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Conger, R.D.; Elder, G.H. Families in Troubled Times; Aldine De Gruyter: New York, NY, USA, 1994. [Google Scholar]
- Cobb-Clark, D.A.; Salamanca, N.; Zhu, A. Parenting style as an investment in human development. J. Popul. Econ. 2019, 32, 1315–1352. [Google Scholar] [CrossRef] [Green Version]
- Baumrind, D. The influence of parenting style on adolescent competence and substance use. J. Early Adolesc. 1991, 11, 56–59. [Google Scholar] [CrossRef]
- Pinquart, M. Associations of parenting dimensions and styles with externalizing problems of children and adolescents: An updated meta-analysis. Dev. Psychol. 2017, 53, 873–932. [Google Scholar] [CrossRef]
- Pinquart, M.; Gerke, D.C. Associations of parenting styles with self-esteem in children and adolescents: A meta-analysis. J. Child. Fam. Stud. 2019, 28, 1–19. [Google Scholar] [CrossRef]
- Uji, M.; Sakamoto, A.; Adachi, K.; Kitamura, T. The impact of authoritative, authoritarian, and permissive parenting styles on children’s later mental health in Japan: Focusing on parent and child gender. J. Child. Fam. Stud. 2014, 23, 293–302. [Google Scholar] [CrossRef]
- Veldhuis, L.; van Grieken, A.; Renders, C.M.; Hirasing, R.A.; Raat, H. Parenting style, the home environment, and screen time of 5-year-old children; the ‘be active, eat right’ study. PLoS ONE 2014, 9, e88486. [Google Scholar] [CrossRef] [Green Version]
- Collins, C.; Duncanson, K.; Burrows, T. A systematic review investigating associations between parenting style and child feeding behaviours. J. Hum. Nutr. Diet. 2014, 27, 557–568. [Google Scholar] [CrossRef]
- Chow, C.K.; Islam, S.M.; Farmer, A.; Bobrow, K.; Maddision, R.; Whittaker, R.; Dale, L.P.; Lechner, A.; Niessen, L.; Lear, S.A.; et al. Text2PreventCVD: Protocol for a systematic review and individual participant data meta-analysis of text message-based interventions for the prevention of cardiovascular diseases. BMJ Open 2016, 6, e012723. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, M.A.; Loken, B.; Hornik, R.C. Use of mass media campaigns to change health behaviour. Lancet 2010, 376, 1261–1271. [Google Scholar] [CrossRef] [Green Version]
- Muench, F.; van Stolk-Cooke, K.; Morgenstern, J.; Kuerbis, A.N.; Markle, K. Understanding messaging preferences to inform development of mobile goal-directed behavioral interventions. J. Med. Internet Res. 2014, 16, e14. [Google Scholar] [CrossRef] [Green Version]
- Tani, Y.; Fujiwara, T.; Doi, S.; Isumi, A. Home Cooking and Child Obesity in Japan: Results from the A-CHILD Study. Nutrients 2019, 11, 2859. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Total (n = 10,784) | Not Living in Poverty (n = 7088; 65.7%) | Living in Poverty (n = 3696; 34.3%) | |||||
|---|---|---|---|---|---|---|---|---|
| n | % or Mean (SD) | n | % or Mean (SD) | n | % or Mean (SD) | p for t-Test or Chi-Squared Test | ||
| Basic demographics | ||||||||
| Respondent | Mother | 9384 | 87.0 | 6153 | 86.8 | 3231 | 87.4 | 0.005 |
| Father | 1130 | 10.5 | 775 | 10.9 | 355 | 9.6 | ||
| Grandparent | 110 | 1.0 | 58 | 0.8 | 52 | 1.4 | ||
| Others | 60 | 0.6 | 34 | 0.5 | 26 | 0.7 | ||
| Missing | 100 | 0.9 | 68 | 1.0 | 32 | 0.9 | ||
| Child sex | Male | 5025 | 46.6 | 3317 | 46.8 | 1708 | 46.2 | 0.675 |
| Female | 5525 | 51.2 | 3613 | 51 | 1912 | 51.7 | ||
| Missing | 234 | 2.2 | 158 | 2.2 | 76 | 2.1 | ||
| Grade | 5th | 3117 | 28.9 | 1955 | 27.6 | 1162 | 31.4 | <0.001 |
| 8th | 3498 | 32.4 | 2339 | 33 | 1159 | 31.4 | ||
| 11th | 4169 | 38.7 | 2794 | 39.4 | 1375 | 37.2 | ||
| Maternal age | <40 years | 1837 | 17.0 | 994 | 14.0 | 843 | 22.8 | <0.001 |
| 40 years–<50 years | 6841 | 63.4 | 4689 | 66.2 | 2152 | 58.2 | ||
| 50 years+ | 1344 | 12.5 | 971 | 13.7 | 373 | 10.1 | ||
| Missing | 762 | 7.1 | 434 | 6.1 | 328 | 8.9 | ||
| Marital status | Married | 8696 | 80.6 | 6213 | 87.7 | 2483 | 67.2 | <0.001 |
| Unmarried/divorced/widowed | 1974 | 18.3 | 802 | 11.3 | 1172 | 31.7 | ||
| Missing | 114 | 1.1 | 73 | 1.0 | 41 | 1.1 | ||
| Having older sibling | No | 6175 | 57.3 | 4121 | 58.1 | 2054 | 55.6 | 0.011 |
| Yes | 4609 | 42.7 | 2967 | 41.9 | 1642 | 44.4 | ||
| Having younger sibling | No | 5527 | 51.3 | 3716 | 52.4 | 1811 | 49.0 | 0.001 |
| Yes | 5257 | 48.7 | 3372 | 47.6 | 1885 | 51.0 | ||
| Caregiver’s childhood socioeconomic status | ||||||||
| Economic difficulties in childhood | No | 8739 | 81.0 | 6023 | 85.0 | 2716 | 73.5 | <0.001 |
| Yes | 2045 | 19.0 | 1065 | 15.0 | 980 | 26.5 | ||
| Maternal education | High school or less | 3944 | 36.6 | 2111 | 29.8 | 1833 | 49.6 | <0.001 |
| Some college | 4654 | 43.2 | 3331 | 47.0 | 1323 | 35.8 | ||
| College or more | 1448 | 13.4 | 1207 | 17.0 | 241 | 6.5 | ||
| Other/Unknown | 53 | 0.5 | 31 | 0.4 | 22 | 0.6 | ||
| Missing | 685 | 6.4 | 408 | 5.8 | 277 | 7.5 | ||
| Caregiver’s other possible confounders | ||||||||
| Psychological distress (K6) | 0–<5 | 7441 | 69.0 | 5344 | 75.4 | 2097 | 56.7 | |
| 5–<13 | 2442 | 22.6 | 1323 | 18.7 | 1119 | 30.3 | <0.001 | |
| 13+ | 526 | 4.9 | 192 | 2.7 | 334 | 9.0 | ||
| Missing | 375 | 3.5 | 229 | 3.2 | 146 | 4.0 | ||
| Relationship with neighborhood | High | 3109 | 28.8 | 2144 | 30.2 | 965 | 26.1 | <0.001 |
| Low | 7153 | 66.3 | 4606 | 65.0 | 2547 | 68.9 | ||
| Missing | 522 | 4.8 | 338 | 4.8 | 184 | 5.0 | ||
| Parental Involvement Behaviors | Not Living in Poverty (n = 7088; 65.7%) | Living in Poverty (n = 3696; 34.3%) | p for Chi-Squared Test | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Parental interaction with child | ||||||
| Helping child study | <1 a week | 4775 | 67.4 | 2424 | 65.6 | 0.175 |
| 1+ a week | 2039 | 28.8 | 1120 | 30.3 | ||
| Missing | 274 | 3.9 | 152 | 4.1 | ||
| Talking about school life | <5 a week | 3098 | 43.7 | 1812 | 49.0 | <0.001 |
| Almost everyday | 3728 | 52.6 | 1746 | 47.2 | ||
| Missing | 262 | 3.7 | 138 | 3.7 | ||
| Talking about news | <3 a week | 4648 | 65.6 | 2634 | 71.3 | <0.001 |
| 3+ a week | 2156 | 30.4 | 916 | 24.8 | ||
| Missing | 284 | 4.0 | 146 | 3.9 | ||
| Playing with child (physical activity) | Rarely | 4754 | 67.1 | 2500 | 67.6 | 0.549 |
| 1+ a month | 2043 | 28.8 | 1045 | 28.3 | ||
| Missing | 291 | 4.1 | 151 | 4.1 | ||
| Talking about TV shows with child | <5 a week | 4281 | 60.4 | 2232 | 60.4 | 0.924 |
| Almost everyday | 2538 | 35.8 | 1320 | 35.7 | ||
| Missing | 269 | 3.8 | 144 | 3.9 | ||
| Cooking with child | <3 a month | 5526 | 78.0 | 2744 | 74.2 | <0.001 |
| 1+ a week | 1279 | 18.0 | 808 | 21.9 | ||
| Missing | 283 | 4.0 | 144 | 3.9 | ||
| Going out with child | <3 a month | 3259 | 45.9 | 1578 | 42.7 | 0.001 |
| 1+ a week | 3577 | 50.5 | 1987 | 53.8 | ||
| Missing | 252 | 3.6 | 131 | 3.5 | ||
| Talking about child’s future | Sometimes or less | 4870 | 68.7 | 2630 | 71.2 | 0.031 |
| Frequently | 1989 | 28.1 | 959 | 25.9 | ||
| Missing | 229 | 3.2 | 107 | 2.9 | ||
| Hosting events for child | No | 41 | 0.6 | 103 | 2.8 | <0.001 |
| Yes | 6844 | 96.6 | 3499 | 94.7 | ||
| Missing | 203 | 2.9 | 94 | 2.5 | ||
| Parental care for child physical health | ||||||
| Having experience of not visiting the hospital for child | Yes | 743 | 10.5 | 670 | 18.1 | <0.001 |
| No | 6034 | 85.1 | 2860 | 77.4 | ||
| Missing | 311 | 4.4 | 166 | 4.5 | ||
| History of routine vaccination | No/unknown | 301 | 4.3 | 332 | 9.0 | |
| Yes | 6498 | 91.7 | 3209 | 86.8 | <0.001 | |
| Missing | 289 | 4.1 | 155 | 4.2 | ||
| Maternal smoking in front of child | Smoking in front of child | 788 | 11.1 | 955 | 25.9 | <0.001 |
| Never smoking/smoking but not in front of child | 5937 | 83.8 | 2466 | 66.7 | ||
| Missing | 363 | 5.1 | 275 | 7.4 | ||
| Paternal smoking in front of child | Smoking in front of child | 2333 | 32.9 | 1383 | 37.4 | <0.001 |
| Never smoking/smoking but not in front of child | 4004 | 56.5 | 1256 | 34.0 | ||
| Missing | 751 | 10.6 | 1057 | 28.6 | ||
| Cooking for child | <6 (days) week | 985 | 13.9 | 707 | 19.1 | <0.001 |
| Almost everyday | 5858 | 82.6 | 2867 | 77.6 | ||
| Missing | 245 | 3.5 | 122 | 3.3 | ||
| Living in Poverty | Not Living in Poverty | ||||||
|---|---|---|---|---|---|---|---|
| Crude | Model 1 a | Model 2 b | Crude | Model 1 a | Model 2 b | ||
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | ||
| Parental involvement behaviors | Total score (0–14) | 0.42 ** (0.33 to 0.50) | 0.29 ** (0.20 to 0.38) | 0.26 ** (0.17 to 0.35) | 0.48 ** (0.42 to 0.53) | 0.29 ** (0.23 to 0.35) | 0.27 ** (0.20 to 0.33) |
| Respondent | Mother | Ref | Ref | Ref | Ref | ||
| Father | 0.85 ** (0.07 to 1.62) | 0.71 (−0.05 to 1.48) | −0.12 (−0.58 to 0.34) | −0.22 (−0.68 to 0.24) | |||
| Grandparent | 0.56 (−1.13 to 2.24) | 0.28 (−1.38 to 1.95) | −1.41 (−3.02 to 0.20) | −1.74 ** (−3.36 to −0.11) | |||
| Others | −0.06 (−2.88 to 2.76) | −0.15 (−3.05 to 2.75) | −0.38 (−2.46 to 1.71) | −0.48 (−2.51 to 1.55) | |||
| Child sex | Male | Ref | Ref | Ref | Ref | ||
| Female | −1.37 ** (−1.76 to −0.96) | −1.38 ** (−1.78 to −0.97) | −1.39 ** (−1.67 to −1.12) | −1.38 ** (−1.66 to −1.10) | |||
| Grade | 5th | Ref | Ref | Ref | Ref | ||
| 8th | −2.40 ** (−2.95 to −1.85) | −2.40 ** (−2.95 to −1.85) | −2.60 ** (−2.98 to −2.23) | −2.61 ** (−2.99 to −2.24) | |||
| 11th | −2.67 ** (−3.25 to −2.10) | −2.69 ** (−3.27 to −2.12) | −3.20 ** (−3.26 to −2.79) | −3.26 ** (−3.66 to −2.85) | |||
| Maternal age | <40 years | Ref | Ref | Ref | Ref | ||
| 40 years–<50 years | 0.32 (−0.22 to 0.87) | 0.23 (−0.31 to 0.76) | −0.05 (−0.48 to 0.37) | −0.08 (−0.51 to 0.35) | |||
| 50 years+ | −0.16 (−0.99 to 0.67) | −0.24 (−1.06 to 0.59) | −0.44 (−1.02 to 0.14) | −0.46 (−1.04 to 0.12) | |||
| Marital status | Married | Ref | Ref | Ref | Ref | ||
| Unmarried/divorced/widowed | 0.34 (−0.13 to 0.81) | 0.35 (−0.11 to 0.82) | 0.25 (−0.24 to 0.73) | 0.25 (−0.23 to 0.75) | |||
| Having older sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | 0.04 (−0.41 to 0.48) | −0.05 (−0.49 to 0.39) | −0.29 (−0.59 to 0.02) | −0.32 * (−0.63 to −0.02) | |||
| Having younger sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | 0.24 (−0.21 to 0.69) | 0.16 (−0.28 to 0.27) | −0.28 (−0.59 to 0.04) | −0.33 * (−0.65 to −0.02) | |||
| Economic difficulties in childhood | No | Ref | Ref | Ref | Ref | ||
| Yes | −0.37 (−0.84 to 0.09) | −0.19 (−0.65 to 0.27) | −0.31 (−0.70 to 0.08) | −0.21 (−0.60 to 0.18) | |||
| Maternal education | High school or less | Ref | Ref | Ref | Ref | ||
| Some college | 0.33 (−0.12 to 0.78) | 0.33 (−0.12 to 0.77) | 0.33 * (0.003 to 0.65) | 0.33 * (0.01 to 0.65) | |||
| College or more | 0.78 (−0.09 to 1.66) | 0.71 (−0.17 to 1.59) | 0.63 ** (0.19 to 1.07) | 0.66 ** (0.22 to 1.09) | |||
| Other/Unknown | 0.47 (−2.15 to 3.08) | 0.55 (−2.06 to 3.15) | 0.12 (−2.07 to 2.32) | 0.23 (−1.98 to 2.43) | |||
| Caregiver’s psychological distress (K6) | 0–<5 | Ref | Ref | ||||
| 5–<13 | 0.56 (−0.22 to 1.33) | 0.81 (−0.17 to 1.80) | |||||
| 13+ | 1.19 ** (0.44 to 1.94) | 1.51 ** (0.57 to 2.46) | |||||
| Caregiver’s relationship with neighborhood | High | Ref | Ref | ||||
| Low | 0.99 ** (0.52 to 1.46) | 0.50 ** (0.20 to 0.81) | |||||
| R2 | 0.029 | 0.087 | 0.100 | 0.040 | 0.116 | 0.122 | |
| Living in Poverty | Not Living in Poverty | ||||||
|---|---|---|---|---|---|---|---|
| Crude | Model 1 a | Model 2 b | Crude | Model 1 a | Model 2 b | ||
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | ||
| Parental interaction with child | Total score (0–9) | 0.47 ** (0.37 to 0.57) | 0.33 ** (0.22 to 0.44) | 0.30 ** (0.19 to 0.40) | 0.57 ** (0.50 to 0.63) | 0.34 ** (0.26 to 0.41) | 0.31 ** (0.24 to 0.38) |
| Respondent | Mother | Ref | Ref | Ref | Ref | ||
| Father | 0.87 * (0.09 to 1.65) | 0.71 (−0.05 to 1.48) | −0.12 (−0.58 to 0.34) | −0.22 (−0.68 to 0.24) | |||
| Grandparent | 0.61 (−1.09 to 2.31) | 0.28 (−1.38 to 1.95) | −1.45 (−3.05 to 0.16) | −1.76 ** (−3.38 to −0.14) | |||
| Others | −0.33 (−3.13 to 2.48) | −0.15 (−3.05 to 2.75) | −0.40 (−2.47 to 1.67) | −0.50 (−2.52 to 1.52) | |||
| Child sex | Male | Ref | Ref | Ref | Ref | ||
| Female | −1.40 ** (−1.81 to −1.00) | −1.38 ** (−1.78 to −0.97) | −1.42 ** (−1.70 to −1.14) | −1.41 ** (−1.68 to −1.13) | |||
| Grade | 5th | Ref | Ref | Ref | Ref | ||
| 8th | −2.39 ** (−2.94 to −1.84) | −2.40 ** (−2.95 to −1.85) | −2.56 ** (−2.93 to −2.18) | −2.56 ** (−2.94 to −2.19) | |||
| 11th | −2.69 ** (−3.27 to −2.12) | −2.69 ** (−3.27 to −2.12) | −3.18 ** (−3.59 to −2.78) | −3.23 ** (−3.64 to −2.83) | |||
| Maternal age | <40 years | Ref | Ref | Ref | Ref | ||
| 40 years–<50 years | 0.38 (−0.16 to 0.92) | 0.23 (−0.31 to 0.76) | 0.02 (−0.41 to 0.44) | −0.02 (−0.44 to 0.41) | |||
| 50 years+ | −0.04 (−0.88 to 0.79) | −0.24 (−1.06 to 0.59) | −0.33 (−0.91 to 0.25) | −0.35 (−0.94 to 0.23) | |||
| Marital status | Married | Ref | Ref | Ref | Ref | ||
| Unmarried/divorced/widowed | 0.15 (−0.32 to 0.61) | 0.35 (−0.11 to 0.82) | 0.02 (−0.46 to 0.50) | 0.05 (−0.43 to 0.53) | |||
| Having older sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | 0.03 (−0.42 to 0.47) | −0.05 (−0.49 to 0.39) | −0.27 (−0.58 to 0.03) | −0.31 * (−0.61 to −0.005) | |||
| Having younger sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | 0.26 (−0.19 to 0.71) | 0.16 (−0.28 to 0.27) | −0.24 (−0.55 to 0.07) | −0.30 (−0.61 to 0.01) | |||
| Economic difficulties in childhood | No | Ref | Ref | Ref | Ref | ||
| Yes | −0.42 (−0.88 to 0.04) | −0.19 (−0.65 to 0.27) | −0.32 (−0.71 to 0.07) | −0.22 (−0.61 to 0.17) | |||
| Maternal education | High school or less | Ref | Ref | Ref | Ref | ||
| Some college | 0.41 (−0.04 to 0.86) | 0.33 (−0.12 to 0.77) | 0.38 * (0.06 to 0.70) | 0.38 * (0.05 to 0.70) | |||
| College or more | 0.92 * (0.04 to 1.79) | 0.71 (−0.17 to 1.59) | 0.72 ** (0.28 to 1.15) | 0.73 ** (0.30 to 1.17) | |||
| Other/Unknown | 0.43 (−2.15 to 3.02) | 0.55 (−2.06 to 3.15) | 0.08 (−2.12 to 2.29) | 0.19 (−2.03 to 2.41) | |||
| Caregiver’s psychological distress (K6) | 0–<5 | Ref | Ref | ||||
| 5–<13 | 0.56 (−0.22 to 1.33) | 0.82 (−0.16 to 1.80) | |||||
| 13+ | 1.19 ** (0.44 to 1.94) | 1.55 ** (0.61 to 2.49) | |||||
| Caregiver’s relationship with neighborhood | High | Ref | Ref | ||||
| Low | 0.99 ** (0.52 to 1.46) | 0.49 ** (0.19 to 0.80) | |||||
| R2 | 0.026 | 0.087 | 0.100 | 0.042 | 0.116 | 0.122 | |
| Living in Poverty | Not Living in Poverty | ||||||
|---|---|---|---|---|---|---|---|
| Crude | Model 1 a | Model 2 b | Crude | Model 1 a | Model 2 b | ||
| β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | β (95% CI) | ||
| Parental care for child’s physical health | Total score (0–5) | 0.41 ** (0.22 to 0.60) | 0.23 * (0.03 to 0.42) | 0.18 (−0.02 to 0.38) | 0.40 ** (0.26 to 0.54) | 0.24 * (0.09 to 0.39) | 0.20 * (0.05 to 0.35) |
| Respondent | Mother | Ref | Ref | Ref | Ref | ||
| Father | 0.70 (−0.08 to 1.48) | 0.57 (−0.19 to 1.34) | −0.27 (−0.73 to 0.19) | −0.37 (−0.83 to 0.10) | |||
| Grandparent | 0.21 (−1.51 to 1.93) | −0.05 (−1.75 to 1.65) | −1.54 (−3.19 to 0.10) | −1.93 * (−3.58 to −0.28) | |||
| Others | −0.18 (−2.99 to 2.63) | −0.27 (−3.16 to 2.63) | −0.39 (−2.40 to 1.63) | −0.51 (−2.46 to 1.45) | |||
| Child sex | Male | Ref | Ref | Ref | Ref | ||
| Female | −1.20 ** (−1.61 to −0.79) | −1.23 ** (−1.63 to −0.83) | −1.23 ** (−1.51 to −0.95) | −1.23 ** (−1.51 to −0.95) | |||
| Grade | 5th | Ref | Ref | Ref | Ref | ||
| 8th | −2.71 ** (−3.25 to −2.17) | −2.67 ** (−3.21 to −2.14) | −3.00 ** (−3.37 to −2.63) | −2.97 ** (−3.34 to −2.60) | |||
| 11th | −3.21 ** (−3.75 to −2.66) | −3.16 ** (−3.70 to −2.62) | −3.80 ** (−4.19 to −3.42) | −3.81 ** (−4.20 to −3.43) | |||
| Maternal age | <40 years | Ref | Ref | Ref | Ref | ||
| 40 years–<50 years | 0.29 (−0.25 to 0.83) | 0.19 (−0.35 to 0.73) | −0.08 (−0.51 to 0.35) | −0.10 (−0.53 to 0.33) | |||
| 50 years+ | −0.27 (−1.11 to 0.57) | −0.33 (−1.17 to 0.50) | −0.53 (−1.12 to 0.06) | −0.53 (−1.13 to 0.06) | |||
| Marital status | Married | Ref | Ref | Ref | Ref | ||
| Unmarried/divorced/widowed | 0.29 (−0.20 to 0.77) | 0.30 (−0.19 to 0.78) | 0.13 (−0.36 to 0.63) | 0.13 (−0.36 to 0.62) | |||
| Having older sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | −0.02 (−0.46 to 0.43) | −0.10 (−0.54 to 0.34) | −0.35 * (−0.65 to −0.04) | −0.38 * (−0.68 to −0.07) | |||
| Having younger sibling | No | Ref | Ref | Ref | Ref | ||
| Yes | 0.22 (−0.23 to 0.68) | 0.15 (−0.30 to 0.60) | −0.28 (−0.60 to 0.03) | −0.34 * (−0.66 to −0.03) | |||
| Economic difficulties in childhood | No | Ref | Ref | Ref | Ref | ||
| Yes | −0.39 (−0.85 to 0.08) | −0.19 (−0.66 to 0.27) | −0.32 (−0.71 to 0.08) | −0.21 (−0.61 to 0.18) | |||
| Maternal education | High school or less | Ref | Ref | Ref | Ref | ||
| Some college | 0.37 (−0.09 to 0.83) | 0.36 (−0.09 to 0.81) | 0.38 * (0.06 to 0.70) | 0.38 * (0.06 to 0.70) | |||
| College or more | 0.83 (−0.04 to 1.71) | 0.75 (−0.13 to 1.63) | 0.71 ** (0.27 to 1.16) | 0.74 ** (0.30 to 1.18) | |||
| Other/Unknown | 0.50 (−2.17 to 3.18) | 0.58 (−2.07 to 3.23) | 0.24 (−1.99 to 2.46) | 0.35 (−1.88 to 2.59) | |||
| Caregiver’s psychological distress (K6) | 0–<5 | Ref | Ref | ||||
| 5–<13 | 0.59 (−0.18 to 1.37) | 0.81 (−0.17 to 1.80) | |||||
| 13+ | 1.24 * (0.50 to 2.00) | 1.55 ** (0.61 to 2.50) | |||||
| Caregiver’s relationship with neighborhood | High | Ref | Ref | ||||
| Low | 1.12 ** (0.65 to 1.59) | 0.65 ** (0.34 to 0.95) | |||||
| R2 | 0.006 | 0.077 | 0.092 | 0.005 | 0.106 | 0.113 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doi, S.; Isumi, A.; Fujiwara, T. The Association between Parental Involvement Behavior and Self-Esteem among Adolescents Living in Poverty: Results from the K-CHILD Study. Int. J. Environ. Res. Public Health 2020, 17, 6277. https://doi.org/10.3390/ijerph17176277
Doi S, Isumi A, Fujiwara T. The Association between Parental Involvement Behavior and Self-Esteem among Adolescents Living in Poverty: Results from the K-CHILD Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6277. https://doi.org/10.3390/ijerph17176277
Chicago/Turabian StyleDoi, Satomi, Aya Isumi, and Takeo Fujiwara. 2020. "The Association between Parental Involvement Behavior and Self-Esteem among Adolescents Living in Poverty: Results from the K-CHILD Study" International Journal of Environmental Research and Public Health 17, no. 17: 6277. https://doi.org/10.3390/ijerph17176277