Association of Liver Transaminase Levels and Long-Term Blood Pressure Variability in Military Young Males: The CHIEF Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurements of Anthropometric and Biochemical Blood Tests
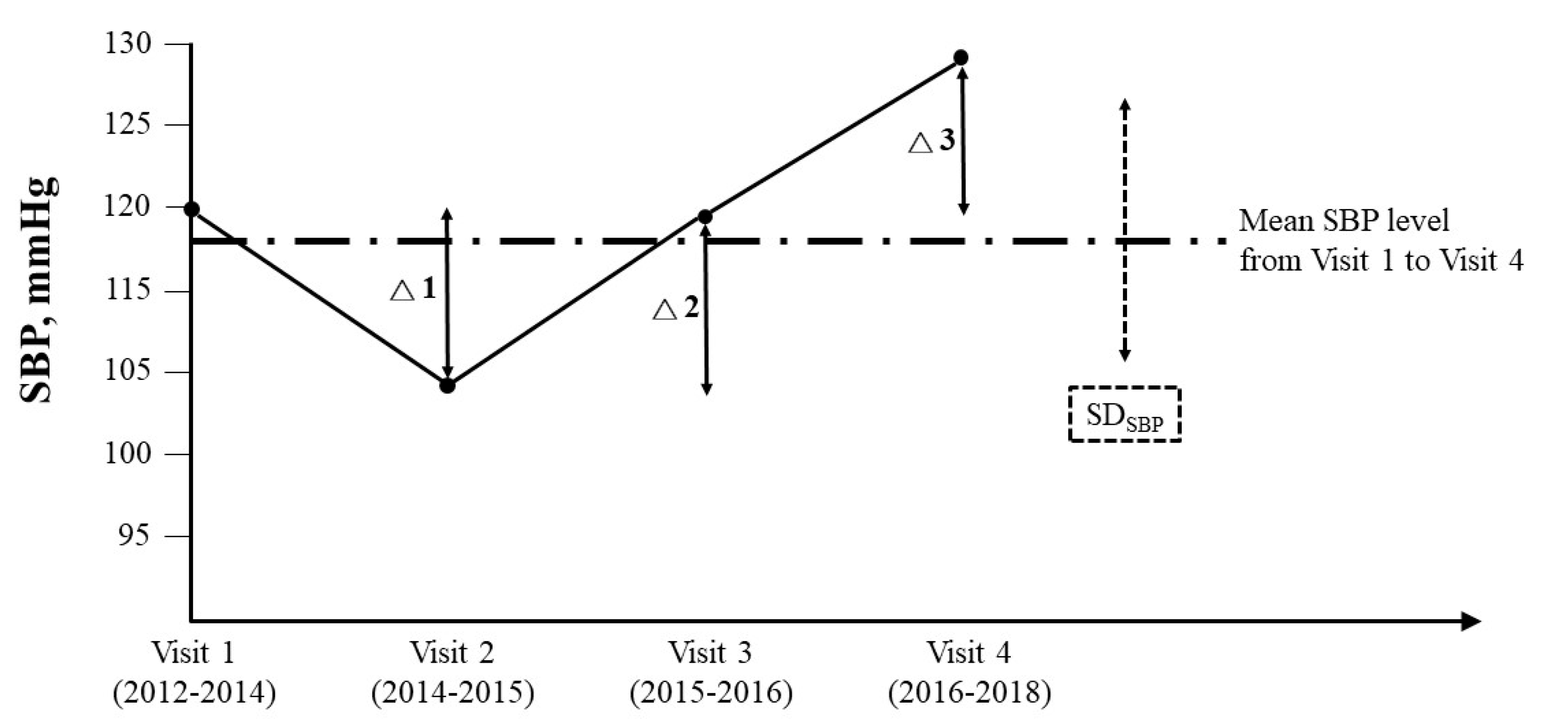
2.3. Measurements of Long-Term BPV
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Arndt, V.; Brenner, H.; Rothenbacher, D.; Zschenderlein, B.; Fraisse, E.; Fliedner, T.M. Elevated liver enzyme activity in construction workers: Prevalence and impact on early retirement and all-cause mortality. Int. Arch. Occup. Environ. Health 1998, 71, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Nam, C.M.; Jee, S.H.; Han, K.H.; Oh, D.K.; Suh, I.I. Normal serum amino-transferase concentration and risk of mortality from liver diseases: Prospective cohort study. Br. Med. J. 2004, 328, 983. [Google Scholar]
- Ford, I.; Mooijaart, S.P.; Lloyd, S.; Murray, H.M.; Westendorp, R.G.J.; de Craen, A.J.M.; Packard, C.J.; Buckley, B.; Barlow, C.; Preiss, D.; et al. The inverse relationship between alanine aminotransferase in the normal range and adverse cardiovascular and non-cardiovascular outcomes. Int. J. Epidemiol. 2011, 40, 1530–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Okamura, T.; Kanda, H.; Hayakawa, T.; Okayama, A.; Ueshima, H. The value of combining serum alanine amino-transferase levels and body mass index to predict mortality and medical costs: A 10-year follow-up study of National Health Insurance in Shiga, Japan. J. Epidemiol. 2006, 16, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruhl, C.E.; Everhart, J.E. Elevated serum alanine aminotransferase and gamma-glutamyltransferase and mortality in the United States population. Gastroenterology 2009, 136, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunutsor, S.K.; Apekey, T.A.; Khan, H. Liver enzymes and risk of cardiovascular disease in the general population: A meta-analysis of prospective cohort studies. Atherosclerosis 2014, 236, 7–17. [Google Scholar] [CrossRef]
- Tonelli, M.; Curhan, G.; Pfeffer, M.; Sacks, F.; Thadhani, R.; Melamed, M.L.; Wiebe, N.; Muntner, P. Relation between alkaline phosphatase, serum phosphate, and all-cause or cardiovascular mortality. Circulation 2009, 120, 1784e92. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, Y.; Imano, H.; Ohira, T.; Kitamura, A.; Kiyama, M.; Okada, T.; Ishikawa, Y.; Shimamoto, T.; Yamagishi, K.; Tanigawa, T.; et al. Alkaline phosphatase and risk of stroke among Japanese: The circulatory risk in communities study (CIRCS). J. Stroke Cerebrovasc. Dis. 2012, 22, 1046e55. [Google Scholar] [CrossRef]
- Emdin, M.; Pompella, A.; Paolicchi, A. Gamma-glutamyltransferase, atherosclerosis, and cardiovascular disease: Triggering oxidative stress within the plaque. Circulation 2005, 112, 2078–2080. [Google Scholar] [CrossRef] [Green Version]
- Franzini, M.; Corti, A.; Martinelli, B.; Corso, A.D.; Emdin, M.; Parenti, G.F.; Glauber, M.; Pompella, A.; Paolicchi, A. Gamma-glutamyltransferase activity in human atherosclerotic plaques-biochemical similarities with the circulating enzyme. Atherosclerosis 2009, 202, 119–127. [Google Scholar] [CrossRef]
- Yesilova, Z.; Serdar, M.; Ercin, C.N.; Gunay, A.; Kilciler, G.; Hasimi, A.; Uygun, A.; Kurt, I.; Erbil, M.K.; Dagalp, K. Decreased oxidation susceptibility of plasma low density lipoproteins in patients with Gilbert’s syndrome. J. Gastroenterol. Hepatol. 2008, 23, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Sedlak, T.W.; Saleh, M.; Higginson, D.S.; Paul, B.D.; Juluri, K.R.; Snyder, S.H. Bilirubin and glutathione have complementary antioxidant and cytoprotective roles. Proc. Natl. Acad. Sci. USA 2009, 106, 5171–5176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.P.; Vitek, L.; Schwertner, H.A. Serum bilirubin and genes controlling bilirubin concentrations as biomarkers for cardiovascular disease. Clin. Chem. 2010, 56, 1535–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.P.; O’Donnell, C.J.; Schwaiger, J.P.; Cupples, L.A.; Lingenhel, A.; Hunt, S.C.; Yang, S.; Kronenberg, F. Association between the UGT1A1*28 allele, bilirubin levels, and coronary heart disease in the Framingham Heart Study. Circulation 2006, 114, 1476–1481. [Google Scholar] [CrossRef] [Green Version]
- Horsfall, L.J.; Rait, G.; Walters, K.; Swallow, D.M.; Pereira, S.P.; Nazareth, I.; Petersen, I. Serum bilirubin and risk of respiratory disease and death. JAMA 2011, 305, 691–697. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.J.; Chen, K.W.; Shih, Y.L.; Su, F.Y.; Lin, Y.P.; Meng, F.C.; Lin, F.; Yu, Y.S.; Han, C.L.; Wang, C.H.; et al. Chronic hepatitis B, nonalcoholic steatohepatitis and physical fitness of military males: CHIEF study. World J. Gastroenterol. 2017, 23, 4587–4594. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, Y.J.; Zhou, Y.; Li, Y.; Zhou, T.; Zheng, J.; Zhang, J.J.; Li, S.; Xu, D.P.; Li, H.B. Effects of beverages on alcohol metabolism: Potential health benefits and harmful impacts. Int. J. Med. Sci. 2016, 17, 354. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Razi, B.; Alizadeh, S.; Omidkhoda, A.; Imani, D.; Rezaei, R. Association of chronic hepatitis B infection with metabolic syndrome and its components: Meta-analysis of observational studies. Diabetes Metab. Syndr. 2017, 11, S939–S947. [Google Scholar] [CrossRef]
- Perumpail, B.J.; Khan, M.A.; Yoo, E.R.; Cholankeril, G.; Kim, D.; Aijaz Ahmed, A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 8263–8276. [Google Scholar] [CrossRef]
- Mahli, A.; Hellerbrand, C. Alcohol and obesity: A dangerous association for fatty liver disease. Dig. Dis. 2016, 34, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCallum, L.; Panniyammakal, J.; Hastie, C.E.; Hewitt, J.; Rajan Patel, R.; Jones, G.C.; Muir, S.; Walters, M.; Sattar, N.; Dominiczak, A.F.; et al. Longitudinal blood pressure control, long-term mortality, and predictive utility of serum liver enzymes and bilirubin in hypertensive patients. Hypertension 2015, 66, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Ochoa, J.E.; Lombardi, C.; Bilo, G. Assessment and management of blood-pressure variability. Nat. Rev. Cardiol. 2013, 10, 143–155. [Google Scholar] [CrossRef]
- Lin, G.M.; Tsai, K.Z.; Lin, C.S.; Han, C.L. Physical fitness and long-term blood pressure variability of young male military personnel. Curr. Hypertens. Rev. 2019, 140, A14908. [Google Scholar] [CrossRef]
- Lin, G.M.; Li, Y.H.; Lee, C.J.; Shiang, J.C.; Lin, K.H.; Chen, K.W.; Chen, Y.J.; Wu, C.F.; Lin, B.S.; Yu, Y.S.; et al. Rationale and design of the cardio- respiratory fitness and hospitalization events in armed forces study in Eastern Taiwan. World J. Cardiol. 2016, 8, 464–471. [Google Scholar] [CrossRef]
- Tsai, K.Z.; Lin, J.W.; Lin, F.; Su, F.Y.; Li, Y.H.; Lin, Y.P.; Lin, Y.K.; Han, C.L.; Hsieh, C.B.; Lin, G.M. Association of betel nut chewing with exercise performance in a military male cohort: The CHIEF study. J. R. Army Med. Corps 2018, 164, 399–404. [Google Scholar] [CrossRef]
- Tsai, K.Z.; Lai, S.W.; Hsieh, C.J.; Lin, C.S.; Lin, Y.P.; Tsai, S.C.; Chung, P.S.; Lin, Y.K.; Lin, T.C.; Ho, C.L.; et al. Association between mild anemia and physical fitness in a military male cohort: The CHIEF study. Sci. Rep. 2019, 9, 11165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, W.H.; Su, F.Y.; Lin, F.; Yu, Y.S.; Lin, G.M. Association of electrocardiographic left and right ventricular hypertrophy with physical fitness of military males: The CHIEF study. Eur. J. Sport Sci. 2019, 19, 1214–1220. [Google Scholar] [CrossRef]
- Su, F.Y.; Wang, S.H.; Lu, H.H.; Lin, G.M. Association of tobacco smoking with physical fitness of military males in taiwan: The CHIEF study. Can. Respir. J. 2020, 2020, 5968189. [Google Scholar] [CrossRef]
- Lu, S.C.; Liu, F.Y.; Hsieh, C.J.; Su, F.Y.; Wong, T.Y.; Tai, M.C.; Chen, J.T.; Lin, G.M. Quantitative physical fitness measures inversely associated with myopia severity in military males: The CHIEF study. Am. J. Men Health 2019, 13, 1557988319883766. [Google Scholar] [CrossRef]
- Lin, G.M.; Lu, H.H. A 12-lead ECG-based system with physiological parameters and machine learning to identify right ventricular hypertrophy in young adults. IEEE J. Transl. Eng. Health Med. 2020, 8, 1900510. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.M.; Liu, K. An electrocardiographic system with anthropometrics via machine learning to screen left ventricular hypertrophy among young adults. IEEE J. Transl. Eng. Health Med. 2020, 8, 1800111. [Google Scholar] [CrossRef]
- Yano, Y.; Ning, H.; Allen, N.; Reis, J.P.; Launer, L.J.; Liu, K.; Yaffe, K.; Greenland, P.; Lloyd-Jones, D.M. Long-term blood pressure variability throughout young adulthood and cognitive function in midlife: The coronary artery risk development in young adults (CARDIA) study. Hypertension 2014, 64, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yano, Y.; Griswold, M.; Wang, W.; Greenland, P.; Lloyd-Jones, D.M.; Heiss, G.; Gottesman, R.F.; Mosley, T.H. Long-term blood pressure level and variability from midlife to later life and subsequent cognitive change: The ARIC neurocognitive study. J. Am. Heart Assoc. 2018, 7, e009578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.W.; Meng, F.C.; Shih, Y.L.; Su, F.Y.; Lin, Y.P.; Lin, F.; Lin, J.W.; Chang, W.K.; Lee, C.J.; Li, Y.H.; et al. Sex-specific association between metabolic abnormalities and elevated alanine aminotransferase levels in a military cohort: The CHIEF study. Int. J. Environ. Res. Publ. Health 2018, 15, 545. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.R.; Han, M.A. Association between serum liver enzymes and metabolic syndrome in Korean adults. Int. J. Environ. Res. Publ. Health 2018, 15, 1658. [Google Scholar] [CrossRef] [Green Version]
- Porter, S.A.; Pedley, A.; Massaro, J.M.; Vasan, R.S.; Hoffmann, U.; Fox, C.S. Aminotransferase levels are associated with cardiometabolic risk above and beyond visceral fat and insulin resistance: The framingham heart study. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Guo, X.; Zhang, X.; Yu, S.; Yang, H.; Jiang, M. Association between elevated serum alanine aminotransferase and cardiometabolic risk factors in rural Chinese population: A cross-sectional study. BMC Cardiovasc. Disord. 2015, 15, 65. [Google Scholar] [CrossRef] [Green Version]
- Park, H.K.; Hwang, J.S.; Moon, J.S.; Lee, J.A.; Kim, D.H.; Lim, J.S. Healthy range of serum alanine aminotransferase and its predictive power for cardiovascular risk in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 686–691. [Google Scholar] [CrossRef]
- Fu, S.; Lin, Y.; Luo, L.; Ye, P. The relationship of serum alanine aminotransferase normal-range levels to arterial stiffness and metabolic syndrome in non-drinkers and drinkers: A Chinese community-based analysis. BMC Gastroenterol. 2017, 17, 49. [Google Scholar] [CrossRef] [Green Version]
- Sogabe, M.; Okahisa, T.; Nakagawa, T.; Fukuno, H.; Nakasono, M.; Tomonari, T.; Tanaka, T.; Tanaka, H.; Taniguchi, T.; Muguruma, N.; et al. Influence of light alcohol consumption on lifestyle-related diseases: A predictor of fatty liver with liver enzyme elevation in Japanese females with metabolic syndrome. BMC Gastroenterol. 2016, 16, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.C.; McLean, A.J.; Le Couteur,, D.G. Age-related alteration in hepatic disposition of the neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine and pesticides. Pharmacol. Toxicol. 2002, 90, 203–207. [Google Scholar] [CrossRef]
- Wagenmakers, A.J. Muscle amino acid metabolism at rest and during exercise: Role in human physiology and metabolism. Exerc. Sport Sci. Rev. 1998, 26, 287–314. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Borgioni, C.; Ciucci, A.; Gattobigio, R.; Schillaci, G.; Sacchi, N.; Santucci, A.; Santucci, C.; Reboldi, G.; Porcellati, C. Prognostic significance of blood pressure variability in essential hypertension. Blood Press. Monit. 1996, 1, 3–11. [Google Scholar] [CrossRef]
- Gómez-Angelats, E.; de la Sierra, A.; Sierra, C.; Parati, G.; Mancia, G.; Coca, A. Blood pressure variability and silent cerebral damage in essential hypertension. Am. J. Hypertens. 2004, 17, 696–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaubert, M.P.; Jin, Z.; Russo, C.; Schwartz, J.E.; Homma, S.; Elkind, M.S.V.; Rundek, T.; Sacco, R.L.; Di Tullio, M.R. Alcohol consumption and ambulatory blood pressure: A community-based study in an elderly cohort. Am. J. Hypertens. 2014, 27, 688–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierksma, A.; Lebrun, C.E.; van der Schouw, Y.T.; Grobbee, D.E.; Lamberts, S.W.J.; Hendriks, H.F.J.; Bots, M.L. Alcohol consumption in relation to aortic stiffness and aortic wave reflections: A cross-sectional study in healthy postmenopausal women. Arterioscler Thromb Vasc. Biol. 2004, 24, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J.; Chen, C.M.; Rao, S.R.; Breslow, R.A. Alcohol consumption and cardiovascular mortality among U.S. adults, 1987 to 2002. J. Am. Coll. Cardiol. 2010, 55, 1328–1335. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | ALT ≥ 30 U/L (N = 254) | ALT < 30 U/L (N = 858) | p-Value |
|---|---|---|---|
| Age (yr) | 32.71 ± 3.74 | 32.07 ± 3.91 | 0.02 |
| BMI (kg/m2) | 26.81 ± 2.48 | 24.64 ± 2.83 | <0.001 |
| Waist circumference (cm) | 88.51 ± 6.12 | 83.10 ± 7.09 | <0.001 |
| SBP (mmHg) | 121.31 ± 13.40 | 117.47 ± 13.26 | <0.001 |
| DBP (mmHg) | 73.22 ± 10.60 | 71.12 ± 9.89 | 0.004 |
| Heart rate (beats/minute) | 75.74 ± 11.16 | 74.81 ± 10.43 | 0.22 |
| Serum triglycerides (mg/dL) | 164.01 ± 136.37 | 110.88 ± 91.09 | <0.001 |
| FPG (mg/dL) | 96.63 ± 16.20 | 93.87 ± 12.43 | 0.004 |
| Total cholesterol (mg/dL) | 191.93 ± 37.36 | 176.67 ± 30.43 | <0.001 |
| HDL-C (mg/dL) | 45.82 ± 9.69 | 48.66 ± 9.92 | <0.001 |
| ALT (U/L) | 48.04 ± 24.40 | 17.55 ± 5.74 | <0.001 |
| (Minimum–Maximum) | (30–213) | (5–29) | |
| AST (U/L) | 30.50 ± 13.54 | 18.45 ± 5.03 | <0.001 |
| (Minimum–Maximum) | (16–124) | (10–57) | |
| Physical activity | |||
| Never or occasionally | 42 [16.5] | 143 [16.7] | 0.99 |
| 1–2 times/week | 98 [38.6] | 329 [38.3] | |
| ≥3–5 times/week | 114 [44.9] | 386 [45.0] | |
| Current alcohol drinker (n [%]) | 121 [47.6] | 396 [46.2] | 0.67 |
| Current smoker (n [%]) | 99 [39.0] | 332 [38.7] | 0.93 |
| BPV Indexes | Unadjusted | Model 1 | Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β (SE) | p-Value | R2, % | β (SE) | p-Value | R2, % | β (SE) | p-Value | R2, % | |
| ALT levels | |||||||||
| ARVSBP | −0.217 (0.115) | 0.05 | 0.3 | −0.225 (0.114) | 0.04 | 1.8 | −0.253 (0.108) | 0.01 | 13.7 |
| ARVDBP | 0.240 (0.122) | 0.04 | 0.4 | 0.157 (0.123) | 0.20 | 1.6 | 0.087 (0.116) | 0.45 | 13.3 |
| SDSBP | −0.277 (0.149) | 0.06 | 0.3 | −0.297 (0.148) | 0.04 | 1.8 | −0.345 (0.140) | 0.01 | 13.8 |
| SDDBP | 0.362 (0.161) | 0.02 | 0.5 | 0.236 (0.164) | 0.15 | 1.7 | 0.151 (0.155) | 0.33 | 13.4 |
| AST levels | |||||||||
| ARVSBP | −0.114 (0.059) | 0.05 | 0.3 | −0.117 (0.059) | 0.04 | 1.9 | −0.115 (0.057) | 0.04 | 9.2 |
| ARVDBP | 0.139 (0.063) | 0.02 | 0.4 | 0.097 (0.064) | 0.12 | 1.8 | 0.071 (0.062) | 0.25 | 9.0 |
| SDSBP | −0.127 (0.077) | 0.09 | 0.2 | −0.135 (0.076) | 0.07 | 1.9 | −0.144 (0.074) | 0.05 | 9.2 |
| SDDBP | 0.187 (0.083) | 0.02 | 0.5 | 0.123 (0.085) | 0.14 | 1.8 | 0.096 (0.082) | 0.24 | 9.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, P.-Y.; Lin, Y.-K.; Chen, K.-W.; Tsai, K.-Z.; Lin, Y.-P.; Takimoto, E.; Lin, G.-M. Association of Liver Transaminase Levels and Long-Term Blood Pressure Variability in Military Young Males: The CHIEF Study. Int. J. Environ. Res. Public Health 2020, 17, 6094. https://doi.org/10.3390/ijerph17176094
Liu P-Y, Lin Y-K, Chen K-W, Tsai K-Z, Lin Y-P, Takimoto E, Lin G-M. Association of Liver Transaminase Levels and Long-Term Blood Pressure Variability in Military Young Males: The CHIEF Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6094. https://doi.org/10.3390/ijerph17176094
Chicago/Turabian StyleLiu, Pang-Yen, Yu-Kai Lin, Kai-Wen Chen, Kun-Zhe Tsai, Yen-Po Lin, Eiki Takimoto, and Gen-Min Lin. 2020. "Association of Liver Transaminase Levels and Long-Term Blood Pressure Variability in Military Young Males: The CHIEF Study" International Journal of Environmental Research and Public Health 17, no. 17: 6094. https://doi.org/10.3390/ijerph17176094