Mental Health Problems and Associated Factors in Chinese High School Students in Henan Province: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
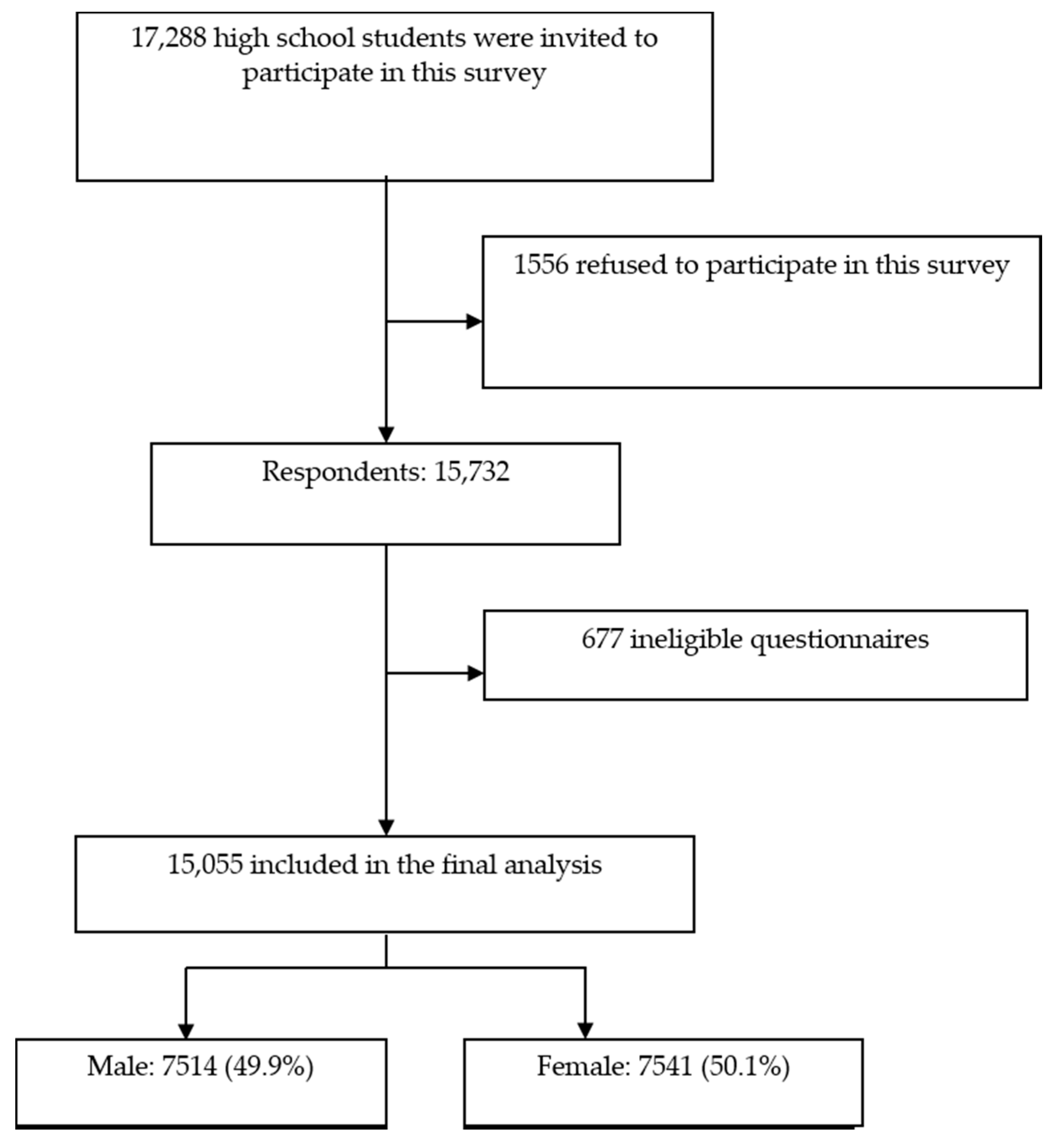
2.1. Sample and Setting
2.2. Ethical Considerations
2.3. Instrumentation
2.3.1. Demographic Information
2.3.2. Mental Health Inventory of Middle School Students
2.4. Data Analysis
3. Results
3.1. Demographic Information
3.2. Positive Rate of Mental Health Problems
3.3. Factors Associated with Mental Health Problems
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Global Mental Health 2 Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- World Health Organization. Adolescent Mental Health. Available online: https://www.who.int/mental_health/maternal-child/adolescent/en/ (accessed on 28 September 2018).
- Wagner, G.; Zeiler, M.; Waldherr, K.; Philipp, J.; Truttmann, S.; Dür, W.; Treasure, J.L.; Karwautz, A.F.K. Mental health problems in Austrian adolescents: A nationwide, two-stage epidemiological study applying DSM-5 criteria. Eur. Child Adolesc. Psychiatry 2017, 26, 1483–1499. [Google Scholar] [CrossRef] [Green Version]
- Cvetkovski, S.; Reavley, N.J.; Jorm, A.F. The prevalence and correlates of psychological distress in Australian tertiary students compared to their community peers. Aust. N. Z. J. Psychiatry 2012, 46, 457–467. [Google Scholar] [CrossRef]
- Louis-Jacques, J.; Samples, C. Caring for teens with chronic illness: Risky business? Curr. Opin. Pediatrics 2011, 23, 367–372. [Google Scholar] [CrossRef]
- Neinstein, L.S. Adolescent Health Care: A Practical Guide, 5th ed; Neinstein, L.S., Gordon, C.M., Katzman, D.K., Rosen, D.S., Woods, E.R., Eds.; Lippincott WIlliams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Hale, D.R.; Bevilacqua, L.; Viner, R.M. Adolescent Health and Adult Education and Employment: A Systematic Review. Pediatrics 2015, 136, 128–140. [Google Scholar] [CrossRef] [Green Version]
- Ng, P.; Chan, K.F.; Ho, W.C. A study on mental health of secondary school students in three metropolitan cities in China: Hong Kong, Shanghai, and Beijing. Int. J. Adolesc. Med. Health 2008, 20, 53–62. [Google Scholar] [CrossRef]
- Emami, H.; Ghazinour, M.; Rezaeishiraz, H.; Richter, J. Mental health of adolescents in Tehran, Iran. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2007, 41, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Safipour, J.; Schopflocher, D.; Higginbottom, G.; Emami, A. Socioeconomic factors and mental health of Swedish adolescents–a cross-sectional study among Stockholm high-school students aged 15–19 years. Vulnerable Child. Youth Stud. 2013, 8, 120–134. [Google Scholar] [CrossRef]
- Wang, H.; Yang, C.; He, F.; Shi, Y.; Qu, Q.; Rozelle, S.; Chu, J. Mental health and dropout behavior: A cross-sectional study of junior high students in northwest rural China. Int. J. Educ. Dev. 2015, 41, 1–12. [Google Scholar] [CrossRef]
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. (1982) 2013, 90, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Li, Z.; Patel, V. Global child and adolescent mental health: The orphan of development assistance for health. PLoS Med. 2018, 15, e1002524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rishel, C.W. Evidence-based prevention practice in mental health: What is it and how do we get there? Am. J. Orthopsychiatry 2007, 77, 153–164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health Action Plan 2013–2020. Available online: https://www.who.int/mental_health/publications/action_plan/en/ (accessed on 8 October 2013).
- Kaushik, A.; Kostaki, E.; Kyriakopoulos, M. The stigma of mental illness in children and adolescents: A systematic review. Psychiatry Res. 2016, 243, 469–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. mhGAP Intervention Guide for Mental, Neurological and Substance Use Disorders in Non-Specialized Health Settings: Mental Health Gap Action Programme (mhGAP). Available online: https://www.who.int/mental_health/publications/mhGAP_intervention_guide/en/ (accessed on 10 October 2016).
- Xing, X.Y.; Tao, F.; Wan, Y.H.; Xing, C.; Qi, X.Y.; Hao, J.H.; Su, P.Y.; Pan, H.F.; Huang, L. Family factors associated with suicide attempts among Chinese adolescent students: A national cross-sectional survey. J. Adolesc. Health 2010, 46, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Filion, N.; Fenelon, A.; Boudreaux, M. Immigration, citizenship, and the mental health of adolescents. PLoS ONE 2018, 13, e0196859. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.Y.; Choi, Y.J. Association of school, family, and mental health characteristics with suicidal ideation among Korean adolescents. Res. Nurs. Health 2015, 38, 301–310. [Google Scholar] [CrossRef]
- Veltro, F.; Ialenti, V.; Morales García, M.A.; Bonanni, E.; Iannone, C.; D’Innocenzo, M.; Gigantesco, A. Promoting Mental Health in Italian Middle and High School: A Pilot Study. Biomed Res. Int. 2017, 2017, 2546862. [Google Scholar] [CrossRef]
- Yuen, W.W.Y.; Liu, L.L.; Tse, S. Adolescent Mental Health Problems in Hong Kong: A Critical Review on Prevalence, Psychosocial Correlates, and Prevention. J. Adolesc. Health 2019, 64, S73–s85. [Google Scholar] [CrossRef]
- Li, J.; Li, J.; Jia, R.; Wang, Y.; Qian, S.; Xu, Y. Mental health problems and associated school interpersonal relationships among adolescents in China: A cross-sectional study. Child Adolesc. Psychiatry Ment. Health 2020, 14, 12. [Google Scholar] [CrossRef]
- Sun, J.; Dunne, M.P.; Hou, X.Y. Academic stress among adolescents in China. Australas. Epidemiol. 2012, 19, 9–12. [Google Scholar]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J. Youth Risk Behavior Surveillance-United States, 2017. Morb. Mortal. Wkly. Rep. Surveill. Summ. (Wash. DC 2002) 2018, 67, 1–114. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Happell, B. The high prevalence of poor physical health and unhealthy lifestyle behaviours in individuals with severe mental illness. Issues Ment. Health Nurs. 2011, 32, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Krossbakken, E.; Pallesen, S.; Mentzoni, R.A.; King, D.L.; Molde, H.; Finseras, T.R.; Torsheim, T. A Cross-Lagged Study of Developmental Trajectories of Video Game Engagement, Addiction, and Mental Health. Front. Psychol. 2018, 9, 2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockdale, L.; Coyne, S.M. Video game addiction in emerging adulthood: Cross-sectional evidence of pathology in video game addicts as compared to matched healthy controls. J. Affect. Disord. 2018, 225, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents. Chin. J. Epidemiol. 2004, 25, 97–102. [Google Scholar]
- Wang, J.; Li, Y.; He, E. Development and Standardization of Mental Health scale for Middle School students in China. Psychosoc. Sci. 1997, 4, 15–20. [Google Scholar]
- Gu, J.; Wu, W.; Tian, T. The Effects of Grandparenting on the Mental Health of Junior High School Students in Sichuan, China. Int. Samanm J. Bus. Soc. Sci. 2013, 1, 24–30. [Google Scholar]
- Zhao, S.; Liao, C. Mental Health and Life Events of Overseas Children Left-Behind in China. Psychology 2016, 7, 1934–1946. [Google Scholar] [CrossRef] [Green Version]
- Du, J.; Li, Z.; Jia, G.; Zhang, Q.; Chen, W. Relationship between mental health and awareness of the knowledge on mental health in left-behind middle school students. Medicine 2019, 98, 1–5. [Google Scholar] [CrossRef]
- Nkuba, M.; Hermenau, K.; Goessmann, K.; Hecker, T. Mental health problems and their association to violence and maltreatment in a nationally representative sample of Tanzanian secondary school students. Soc. Psychiatry Psychiatr Epidemiol. 2018, 53, 699–707. [Google Scholar] [CrossRef]
- Bakhteyar, K.; Bastami, F.; Ebrahimzadeh, F.; Almasian, M.; Hosseinabadi, R.; Farhadi, A. Factors associated with mental health of high-school students in the Islamic Republic of Iran. East. Mediterr. Health J. 2018, 24, 368–376. [Google Scholar] [CrossRef]
- Wainberg, M.L.; Scorza, P.; Shultz, J.M.; Helpman, L.; Mootz, J.J.; Johnson, K.A.; Neria, Y.; Bradford, J.E.; Oquendo, M.A.; Arbuckle, M.R. Challenges and Opportunities in Global Mental Health: A Research-to-Practice Perspective. Curr. Psychiatry Rep. 2017, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Chen, X.L.; Ni, C.P.; Yang, P.; Huang, Y.Q.; Liu, Z.R.; Wang, B.; Yan, Y.P. Survey on the use of mental health services and help-seeking behaviors in a community population in Northwestern China. Psychiatry Res. 2018, 262, 135–140. [Google Scholar] [CrossRef]
- Ali, N.M.; Nowshad, N.A.; Mansoor, K.M.; Ibnouf, R.A.; Albehiery, R.M.; Carrick, F.R.; Abdulrahman, M. Perceived Academic and Psychological Stress among Adolescents in United Arab Emirates: Role of gender, age, depression, and high expectation of parents. Psychiatr. Danub. 2019, 31, 331–337. [Google Scholar]
- Jayanthi, P.; Thirunavukarasu, M.; Rajkumar, R. Academic stress and depression among adolescents: A cross-sectional study. Indian Pediatrics 2015, 52, 217–219. [Google Scholar] [CrossRef] [Green Version]
- Rentala, S.; Nayak, R.B.; Patil, S.D.; Hegde, G.S.; Aladakatti, R. Academic stress among Indian adolescent girls. J. Educ. Health Promot. 2019, 8, 158. [Google Scholar] [CrossRef]
- Abdi, B.; Roozbahani, K.M.; Paeezy, M. A qualitative assessment of stressors among Iranian applicants to the university: An exploratory study. Procedia Soc. Behav. Sci. 2010, 5, 1171–1174. [Google Scholar] [CrossRef] [Green Version]
- Morioka, H.; Itani, O.; Kaneita, Y.; Iwasa, H.; Ikeda, M.; Yamamoto, R.; Osaki, Y.; Kanda, H.; Nakagome, S.; Ohida, T. Factors affecting unhappiness at school among Japanese adolescents: An epidemiological study. PloS ONE 2014, 9, e111844. [Google Scholar] [CrossRef]
- Okada, M.; Suzue, T.; Jitsunari, F. Association between interpersonal relationship among high-school students and mental health. Environ. Health Prev. Med. 2009, 15, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.Y.; Chou, Y.C.; Tzeng, N.S.; Chang, H.A.; Kuo, S.C.; Pan, P.Y.; Yeh, Y.W.; Yeh, C.B.; Mao, W.C. Effects of a selective educational system on fatigue, sleep problems, daytime sleepiness, and depression among senior high school adolescents in Taiwan. Neuropsychiatr. Dis. Treat. 2015, 11, 741–750. [Google Scholar] [CrossRef] [Green Version]
- Hazama, G.I.; Inoue, Y.; Kojima, K.; Ueta, T.; Nakagome, K. The prevalence of probable delayed-sleep-phase syndrome in students from junior high school to university in Tottori, Japan. Tohoku J. Exp. Med. 2008, 216, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Tang, Y.-R.; Xie, C.; Yu, T.; Xiong, W.-J.; Lin, L. Influence of sleep disorders on somatic symptoms, mental health, and quality of life in patients with chronic constipation. Medicine 2017, 96. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Paksarian, D.; Lamers, F.; Hickie, I.B.; He, J.; Merikangas, K.R. Sleep Patterns and Mental Health Correlates in US Adolescents. J. Pediatrics 2017, 182, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, E.L.; Andersson, H.W.; Bjorngaard, J.H.; Pape, K. Anxiety and depression symptoms and alcohol use among adolescents—A cross sectional study of Norwegian secondary school students. BMC Public Health 2017, 17, 494. [Google Scholar] [CrossRef]
- Rikkers, W.; Lawrence, D.; Hafekost, J.; Zubrick, S.R. Internet use and electronic gaming by children and adolescents with emotional and behavioural problems in Australia-results from the second Child and Adolescent Survey of Mental Health and Wellbeing. BMC Public Health 2016, 16, 399. [Google Scholar] [CrossRef] [Green Version]
- Tordon, R.; Svedin, C.G.; Fredlund, C.; Jonsson, L.; Priebe, G.; Sydsjo, G. Background, experience of abuse, and mental health among adolescents in out-of-home care: A cross-sectional study of a Swedish high school national sample. Nord. J. Psychiatry 2019, 73, 16–23. [Google Scholar] [CrossRef]
- Chen, N.; Pei, Y.; Lin, X.; Wang, J.; Bu, X.; Liu, K. Mental health status compared among rural-to-urban migrant, urban and rural school-age children in Guangdong Province, China. BMC Psychiatry 2019, 19, 383. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Lu, R.; Guo, L.; Liu, B. Social Capital and Mental Health in Rural and Urban China: A Composite Hypothesis Approach. Int. J. Environ. Res. Public Health 2019, 16, 665. [Google Scholar] [CrossRef] [Green Version]
- Mariu, K.R.; Merry, S.N.; Robinson, E.M.; Watson, P.D. Seeking professional help for mental health problems, among New Zealand secondary school students. Clin. Child Psychol. Psychiatry 2012, 17, 284–297. [Google Scholar] [CrossRef]
- Meyrose, A.K.; Klasen, F.; Otto, C.; Gniewosz, G.; Lampert, T.; Ravens-Sieberer, U. Benefits of maternal education for mental health trajectories across childhood and adolescence. Soc. Sci. Med. (1982) 2018, 202, 170–178. [Google Scholar] [CrossRef]
- Rajmil, L.; Herdman, M.; Ravens-Sieberer, U.; Erhart, M.; Alonso, J. Socioeconomic inequalities in mental health and health-related quality of life (HRQOL) in children and adolescents from 11 European countries. Int. J. Public Health 2014, 59, 95–105. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 15,058) No. (%) | No Mental Health Problems (n = 8768) No. (%) | With Mental Health Problems (n = 6287) No. (%) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 14–16 | 5881 (39.1) | 3493 (39.8) | 2388 (38.0) | 0.011 |
| 17–20 | 9174 (60.9) | 5275 (60.2) | 3899 (62.0) | ||
| Sex | Male | 7514 (49.9) | 4259 (48.6) | 3255 (51.8) | <0.001 |
| Female | 7541 (50.1) | 4509 (51.4) | 3032 (50.2) | ||
| BMI | Underweight | 1346 (9.1) | 782(9.0) | 564 (9.1) | 0.235 |
| Normal weight | 12,294 (81.7) | 7197(83.0) | 5097 (82.2) | ||
| Overweight | 1226 (8.2) | 687(7.9) | 539 (8.7) | ||
| Ethnicity | Han | 14,679 (97.5) | 8562 (97.7) | 6117 (97.3) | 0.093 |
| Minority | 376 (2.5) | 206 (2.3) | 170 (2.7) | ||
| Inhabitation | Urban | 5984 (39.7) | 3781 (43.1) | 2203 (35.0) | <0.001 |
| Rural | 8411 (55.9) | 4671 (53.3) | 3740 (59.5) | ||
| Rural–urban continuum | 660 (4.4) | 316(3.6) | 344 (5.5) | ||
| Grade | First year | 5279 (35.1) | 3173 (36.2) | 2106 (33.5) | 0.002 |
| Second year | 4009 (26.6) | 2328 (26.6) | 1681 (26.7) | ||
| Third year | 5620 (37.3) | 3190 (36.4) | 2430 (38.7) | ||
| Fourth year § | 147 (1.0) | 77 (0.9) | 70 (1.1) | ||
| Residence on campus | No | 4047 (26.9) | 2522 (28.8) | 1525 (24.3) | <0.001 |
| Yes | 11,008 (73.1) | 6246(71.2) | 4762 (75.7) | ||
| Smoking | No | 14,333 (95.2) | 8464 (96.5) | 5689 (93.4) | <0.001 |
| Yes | 722 (4.8) | 304 (3.5) | 418 (6.6) | ||
| Alcohol consumption | No | 13,091 (87.0) | 7895 (90.0) | 5196 (82.6) | <0.001 |
| Yes | 1964 (13.0) | 873 (10.0) | 1091 (17.4) | ||
| Sexual behavior | Never active | 14,381 (95.5) | 8457 (96.5) | 5924 (94.2) | <0.001 |
| Ever active | 674 (4.5) | 311 (3.5) | 363 (5.8) | ||
| Gaming addiction | No | 13,982 (92.9) | 8331 (95.0) | 5651 (89.9) | <0.001 |
| Yes | 1073 (7.1) | 437 (5.0) | 636 (10.1) | ||
| Physical disease | No | 14,086 (93.6) | 8395 (95.7) | 5691 (90.5) | <0.001 |
| Yes | 969 (6.4) | 373 (4.3) | 596 (9.5) | ||
| Chronic constipation | No | 13,471 (89.5) | 8142 (92.9) | 5329 (84.8) | <0.001 |
| Yes | 1584 (10.5) | 626 (7.1) | 958 (15.2) | ||
| Single parent | No | 14061 (93.4) | 8265 (94.3) | 5796 (92.2) | <0.001 |
| Yes | 994 (6.6) | 503 (5.7) | 491 (7.8) | ||
| Paternal education | High school and below | 10,790 (71.7) | 6061 (69.1) | 4729 (75.2) | <0.001 |
| Junior college | 2208 (14.7) | 1439 (16.4) | 769 (12.2) | ||
| Bachelor | 1700 (11.3) | 1064 (12.1) | 636 (10.1) | ||
| Master | 140 (0.9) | 85 (1.0) | 55 (0.9) | ||
| PhD | 217 (1.4) | 119 (1.4) | 98 (1.6) | ||
| Maternal education | High school and below | 11,436 (76.0) | 6482 (73.9) | 4954 (78.8) | <0.001 |
| Junior college | 1748 (11.6) | 1099 (12.5) | 649 (10.3) | ||
| Bachelor | 1569 (10.4) | 1037 (11.8) | 532 (8.5) | ||
| Master | 101 (0.7) | 45 (0.5) | 56 (0.9) | ||
| PhD | 201 (1.3) | 105 (1.2) | 96 (1.5) |
| Characteristics | Participants | Positive Rate (95%CI), % | Sort Number |
|---|---|---|---|
| Total scale | 6287 | 41.8 (41.0–42.6) | - |
| Academic stress | 8872 | 58.9 (58.1–59.8) | 1 |
| Emotional disturbance | 8355 | 55.5 (54.7–56.3) | 2 |
| Obsessive–compulsive tendencies | 8012 | 53.2 (52.4–54.0) | 3 |
| Anxiety | 7943 | 52.8 (52.0–53.6) | 4 |
| Maladaptation | 7158 | 47.5 (46.8–48.3) | 5 |
| Interpersonal sensitivity | 7103 | 47.2 (46.4–48.0) | 6 |
| Paranoid ideation | 6239 | 41.4 (40.7–42.2) | 7 |
| Depression | 6151 | 40.9 (40.1–41.6) | 8 |
| Hostility | 5108 | 33.9 (33.2–34.7) | 9 |
| Psychological imbalance | 4579 | 30.4 (29.8–31.2) | 10 |
| Variables | Positive Rate (95%CI) | OR (95%CI) | |
|---|---|---|---|
| Age (years) | 14–16 (ref.) | 40.6 (39.4–41.9) | |
| 17–20 | 42.5 (41.6–43.5) | 1.08 (1.01–1.16) | |
| Sex | Male (ref.) | 43.3 (42.2–44.4) | |
| Female | 40.2 (39.1–41.2) | 0.88 (0.83–0.94) | |
| BMI | Underweight (ref.) | 41.9 (38.1–53.4) | |
| Normal weight | 41.5 (40.6–42.2) | 0.98 (0.88–1.10) | |
| Overweight | 44.0 (41.1–46.8) | 1.09 (0.93–1.27) | |
| Ethnicity | Han (ref.) | 41.7 (40.8–42.5) | |
| Minority | 45.2 (39.6–50.5) | 1.16 (0.94–1.42) | |
| Inhabitation | Urban (ref.) | 36.8 (35.6–38.1) | |
| Rural | 44.5 (43.4–45.6) | 1.37 (1.28–1.47) | |
| Rural–urban continuum | 52.1 (48.3–56.2) | 1.87 (1.59–2.20) | |
| Grade | First year (ref.) | 39.9 (38.7–41.1) | |
| Second year | 41.9 (40.5–43.5) | 1.09 (1.00–1.18) | |
| Third year | 43.2 (41.9–44.4) | 1.15 (1.06–1.24) | |
| Fourth year | 47.6 (39.5–55.8) | 1.37 (0.97–1.90) | |
| Residence on campus | No (ref.) | 37.7 (36.1–39.2) | |
| Yes | 43.3 (42.3–44.2) | 1.26 (1.17–1.36) | |
| Smoking | No (ref.) | 40.9 (40.1–41.7) | |
| Yes | 57.9 (54.6–61.8) | 1.98 (1.70–2.31) | |
| Alcohol consumption | No (ref.) | 39.7 (38.9–40.5) | |
| Yes | 55.5 (53.4–57.6) | 1.90 (1.73–2.09) | |
| Sexual behavior | Never active (ref.) | 41.2 (40.4–42.0) | |
| Ever active | 53.9 (50.0–57.6) | 1.67 (1.43–1.95) | |
| Gaming addiction | No (ref.) | 40.4 (39.6–41.1) | |
| Yes | 59.3 (56.2–62.2) | 2.15 (1.89–2.44) | |
| Physical disease | No (ref.) | 40.4 (39.6–41.2) | |
| Yes | 61.5 (58.4–64.4) | 2.36 (2.06–2.69) | |
| Chronic constipation | No (ref.) | 39.6 (38.7–40.4) | |
| Yes | 60.5 (58.0–62.9) | 2.34 (2.10–2.60) | |
| Single parent | No (ref.) | 41.2 (40.4–42.0) | |
| Yes | 49.4 (46.4–52.4) | 1.39 (1.22–1.58) | |
| Paternal education | High school and below (ref.) | 43.8 (42.9–44.8) | |
| Junior college | 34.8 (35.8–36.8) | 0.69 (0.62–0.75) | |
| Bachelor | 37.4 (35.1–39.9) | 0.77 (0.69–0.85) | |
| Master | 39.3 (32.1–47.1) | 0.83 (0.59–1.17) | |
| PhD | 45.2 (38.2–51.6) | 1.06 (0.81–1.38) | |
| Maternal education | High school and below (ref.) | 43.3 (42.4–44.2) | |
| Junior college | 37.1 (34.9–39.2) | 0.77 (0.70–0.86) | |
| Bachelor | 33.9 (31.5–36.3) | 0.67 (0.60–0.75) | |
| Master | 55.4 (45.5–65.3) | 1.63 (1.10–2.42) | |
| PhD | 47.8 (41.3–54.7) | 1.20 (0.91–1.58) |
| Variables | OR (95%CI) | |
|---|---|---|
| Age (years) | 14–16 (ref.) | |
| 17–20 | 0.97 (0.89–1.05) | |
| Sex | Male (ref.) | |
| Female | 0.96 (0.90–1.03) | |
| BMI | Underweight (ref.) | |
| Normal weight | 1.03 (0.91–1.16) | |
| Overweight | 1.10 (0.94–1.29) | |
| Inhabitation | Urban (ref.) | |
| Rural | 1.26 (1.16–1.36) | |
| Rural–urban continuum | 1.68 (1.42–1.99) | |
| Grade | First year (ref.) | |
| Second year | 1.15 (1.05–1.26) | |
| Third year | 1.13 (1.03–1.24) | |
| Fourth year | 1.11 (0.78–1.58) | |
| Residence on campus | No (ref.) | |
| Yes | 1.11 (1.02–1.21) | |
| Smoking | No (ref.) | |
| Yes | 1.12 (0.94–1.34) | |
| Alcohol consumption | No (ref.) | |
| Yes | 1.62 (1.45–1.81) | |
| Sexual behavior | Never active (ref.) | |
| Ever active | 1.31 (1.10–1.55) | |
| Gaming addiction | No (ref.) | |
| Yes | 1.79 (1.56–2.04) | |
| Physical disease | No (ref.) | |
| Yes | 2.04 (1.77–2.35) | |
| Chronic constipation | No (ref.) | |
| Yes | 2.02 (1.80–2.25) | |
| Single parent | No (ref.) | |
| Yes | 1.19 (1.04–1.37) | |
| Paternal education | High school and below (ref.) | |
| Junior college | 0.76 (0.68–086) | |
| Bachelor | 0.93 (0.80–1.07) | |
| Master | 0.73 (0.48–1.09) | |
| PhD | 0.61 (0.34–1.08) | |
| Maternal education | High school and below (ref.) | |
| Junior college | 0.91 (0.80–1.03) | |
| Bachelor | 0.80 (0.68–0.93) | |
| Master | 1.87 (1.17–2.99) | |
| PhD | 1.43 (0.79–2.57) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Y.; Cui, Z.; Zou, P.; Wang, K.; Lin, Z.; He, J.; Wang, J. Mental Health Problems and Associated Factors in Chinese High School Students in Henan Province: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 5944. https://doi.org/10.3390/ijerph17165944
Luo Y, Cui Z, Zou P, Wang K, Lin Z, He J, Wang J. Mental Health Problems and Associated Factors in Chinese High School Students in Henan Province: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5944. https://doi.org/10.3390/ijerph17165944
Chicago/Turabian StyleLuo, Yan, Zhenti Cui, Ping Zou, Kai Wang, Zihan Lin, Jinjie He, and Jing Wang. 2020. "Mental Health Problems and Associated Factors in Chinese High School Students in Henan Province: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 16: 5944. https://doi.org/10.3390/ijerph17165944