Suicidal Presentations to Emergency Departments in a Large Australian Public Health Service over 10 Years


Abstract
:1. Introduction
- To analyze trends in suicidal presentations over a 10-year period;
- To analyze sociodemographic information of consumers with suicidal presentations (age, sex, ethnicity);
- To analyze the frequency of suicidal re-presentations; and
- To identify seasonal patterns of suicidal presentations.
2. Materials and Methods
2.1. Context
2.2. Identification of Suicidal Presentations
2.3. Statistical Analysis
2.4. Research Ethics
3. Results
3.1. Rates of Suicidal Presentations
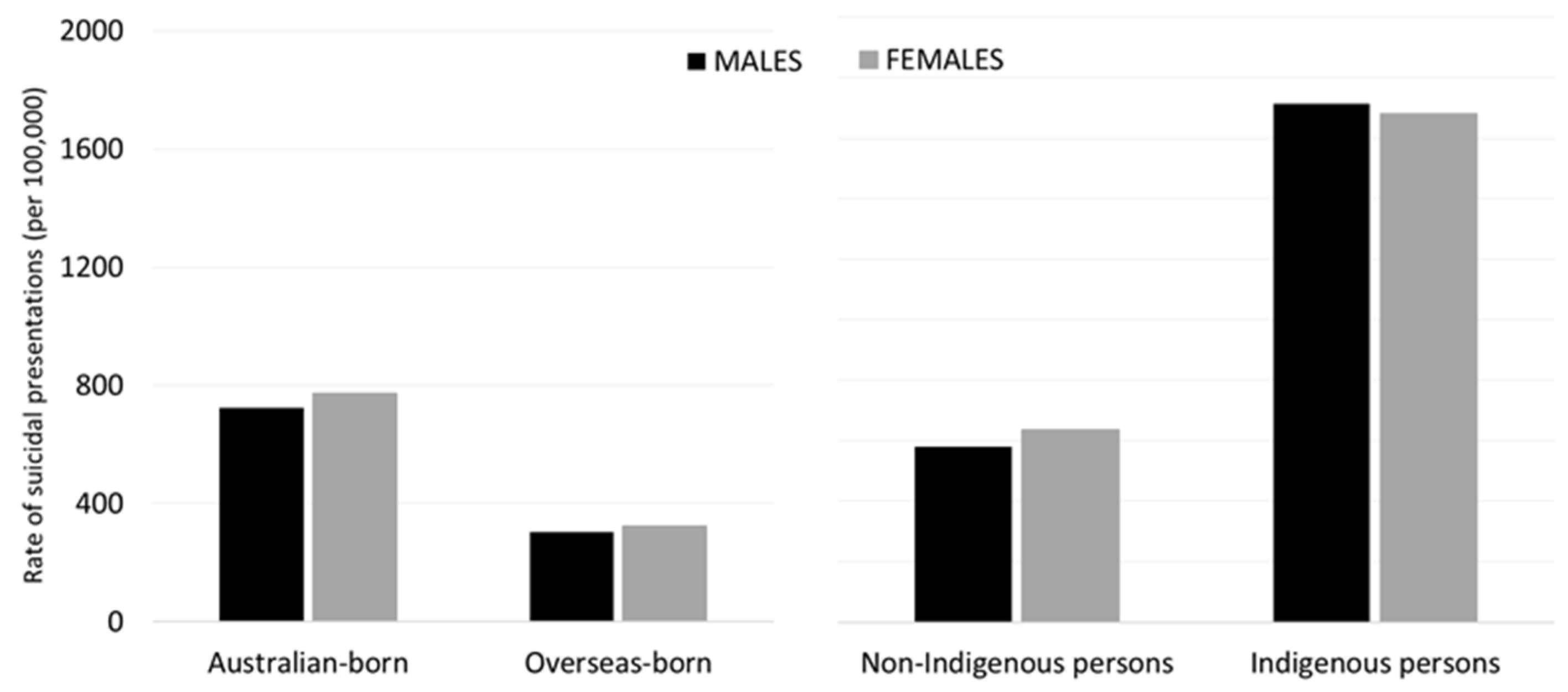
3.2. Demographic Characteristics
3.3. Repeated Suicidal Presentations
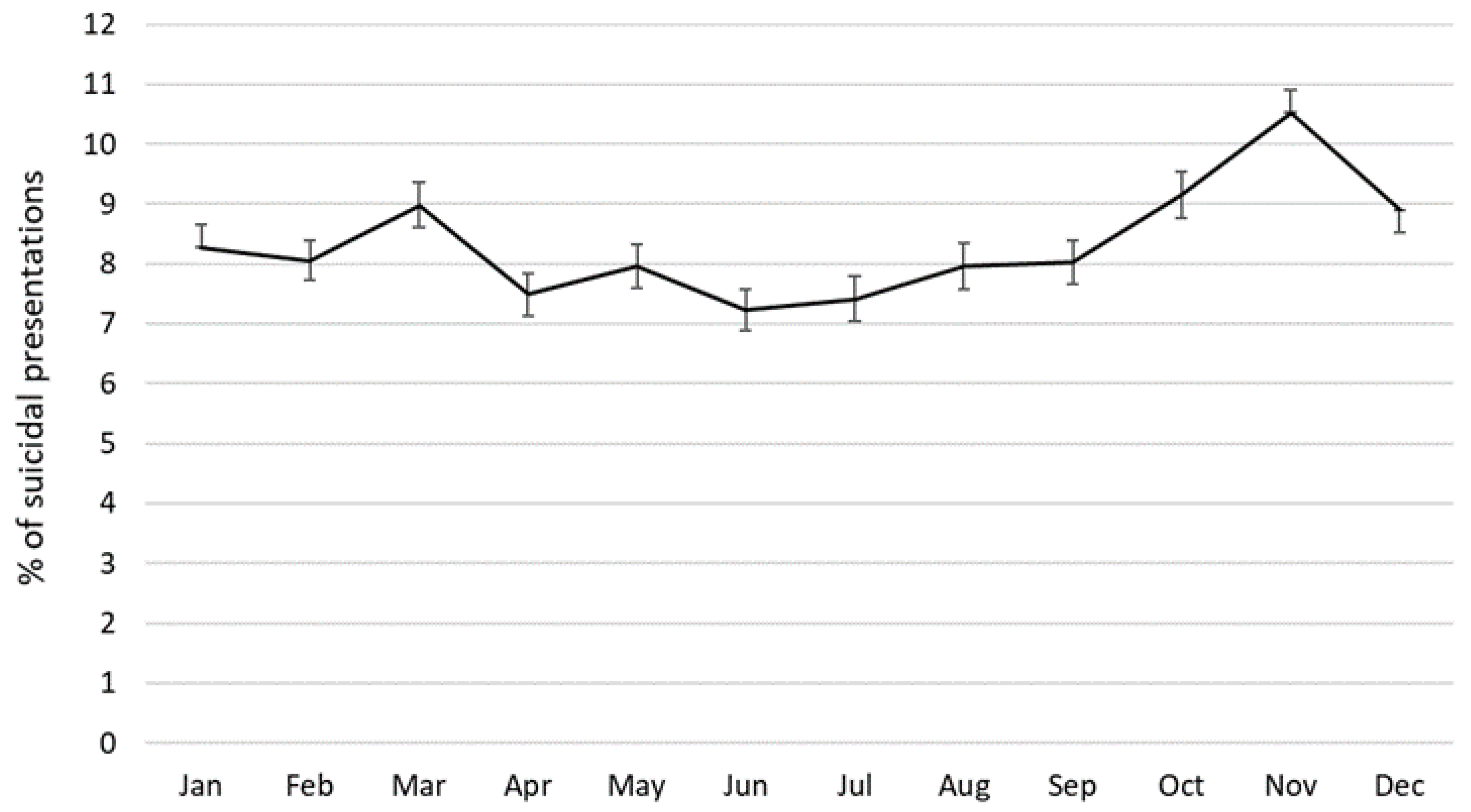
3.4. Seasonality of Suicidal Presentations
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation (WHO). Preventing Suicide: A Global Imperative; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Australian Bureau of Statistics (ABS). Causes of Death, Australia, 2018; ABS: Canberra, Australia, 2019. [Google Scholar]
- Perry, I.J.; Corcoran, P.; Fitzgerald, A.P.; Keeley, H.S.; Reulbach, U.; Arensman, E. The incidence and repetition of hospital-treated deliberate self harm: Findings from the world’s first national registry. PLoS ONE 2012, 7, e31663. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; De Leo, D. Who seeks treatment where? Suicidal behaviors and health care: Evidence from a community survey. J. Nerv. Ment. Dis. 2010, 198, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Leo, D.; Cerin, E.; Spathonis, K.; Burgis, S. Lifetime risk of suicide ideation and attempts in an Australian community: Prevalence, suicidal process, and help-seeking behaviour. J. Affect. Disord. 2005, 86, 215–224. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Preventing Suicide A Resource for Non-Fatal Suicidal Behaviour Case Registration; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Geulayov, G.; Casey, D.; Bale, L.; Brand, F.; Clements, C.; Farooq, B.; Kapur, N.; Ness, J.; Waters, K.; Tsiachristas, A.J.T.L.P. Suicide following presentation to hospital for non-fatal self-harm in the Multicentre Study of Self-harm: A long-term follow-up study. Lancet Psychiatry 2019, 6, 1021–1030. [Google Scholar] [CrossRef] [Green Version]
- Ceniti, A.K.; Heinecke, N.; McInerney, S.J. Examining suicide-related presentations to the emergency department. Gen. Hosp. Psychiatry 2020, 63, 152–157. [Google Scholar] [CrossRef]
- Kõlves, K.; Crompton, D.; Turner, K.; Stapelberg, N.J.; Khan, A.; Robinson, G.; De Leo, D. Trends and repetition of non-fatal suicidal behaviour: Analyses of the Gold Coast University Hospital’s Emergency Department. Australas. Psychiatry 2018, 26, 170–175. [Google Scholar] [CrossRef]
- Boisseau, C.L.; Yen, S.; Markowitz, J.C.; Grilo, C.M.; Sanislow, C.A.; Shea, M.T.; Zanarini, M.C.; Skodol, A.E.; Gunderson, J.G.; Morey, L.C. Individuals with single versus multiple suicide attempts over 10 years of prospective follow-up. Compr. Psychiatry 2013, 54, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Griffin, E.; Bonner, B.; O’Hagan, D.; Kavalidou, K.; Corcoran, P. Hospital-presenting self-harm and ideation: Comparison of incidence, profile and risk of repetition. Gen. Hosp. Psychiatry 2019, 61, 76–81. [Google Scholar] [CrossRef]
- Owens, P.L.; Fingar, K.R.; Heslin, K.C.; Mutter, R.; Booth, C.L.J. Emergency Department Visits Related to Suicidal Ideation, 2006–2013: Statistical Brief.# 220; Agency for Healthcare Research: Rockville, MD, USA, 2017. [Google Scholar]
- Cooper, J.; Murphy, E.; Webb, R.; Hawton, K.; Bergen, H.; Waters, K.; Kapur, N. Ethnic differences in self-harm, rates, characteristics and service provision: Three-City cohort study. Br. J. Psychiatry 2010, 197, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, A.E.; Walsh, R.F.; Liu, R.T. Racial and ethnic differences in mental health service utilization in suicidal adults: A nationally representative study. J. Psychiatr Res. 2018, 107, 114–119. [Google Scholar] [CrossRef]
- Burstein, B.; Agostino, H.; Greenfield, B. Suicidal attempts and ideation among children and adolescents in US emergency departments, 2007–2015. JAMA Pediatr. 2019, 173, 598–600. [Google Scholar] [CrossRef] [PubMed]
- Plemmons, G.; Hall, M.; Doupnik, S.; Gay, J.; Brown, C.; Browning, W.; Casey, R.; Freundlich, K.; Johnson, D.P.; Lind, C. Hospitalization for suicide ideation or attempt: 2008–2015. Pediatrics 2018, 141, e20172426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, J.; Wand, T.; Bein, K.J.; Chalkley, D.; Ivers, R.; Steinbeck, K.S.; Shields, R.; Dinh, M.M. Presentations to NSW emergency departments with self-harm, suicidal ideation, or intentional poisoning, 2010–2014. Med. J. Aust. 2018, 208, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Sveticic, J.; Stapelberg, N.C.; Turner, K. Suicidal and self-harm presentations to emergency departments: The challenges of identification through diagnostic codes and presenting complaints. Health Inf. Manag. J. 2020, 49, 38. [Google Scholar] [CrossRef]
- Randall, J.R.; Roos, L.L.; Lix, L.M.; Katz, L.Y.; Bolton, J.M. Emergency department and inpatient coding for self-harm and suicide attempts: Validation using clinician assessment data. Int. J. Methods Psychiatr. Res. 2017, 26, e1559. [Google Scholar] [CrossRef] [Green Version]
- Walkup, J.T.; Townsend, L.; Crystal, S.; Olfson, M. A systematic review of validated methods for identifying suicide or suicidal ideation using administrative or claims data. Pharmacoepidemiol. Drug Saf. 2012, 21, 174–182. [Google Scholar] [CrossRef]
- Gold Coast Health. Gold Coast Mental Health Suicide Prevention Strategy 2016–2018; Gold Coast Hospital and Health Services: Southport, Queensland, Australia, 2016. [Google Scholar]
- Covington, D.; Hogan, M.; Abreu, J.; Berman, A.; Breux, P.; Coffey, E.; Comeau, C.; Comtois, K.; Damle, C.; Davidson, L. Suicide Care in Systems Framework, National Action Alliance, Clinical Care & Intervention Task Force. Available online: https://theactionalliance.org/resource/suicide-care-systems-framework (accessed on 10 July 2020).
- Stapelberg, N.C.; Randall, M.; Fugelli, P.; Sveticic, J.; Dave, H.; Turner, K. Data Mining for Records of Suicidal and Self-Harm Presentations to Hospital and Health Service Emergency Departments Using an Evolutionary Algorithm. Expert Syst. Appl. 2020. (under review). [Google Scholar]
- Australian Bureau of Statistics. ABS.Stat. Available online: http://stat.data.abs.gov.au/ (accessed on 1 July 2020).
- Lalkhen, A.G.; McCluskey, A. Clinical tests: Sensitivity and specificity. Anaesth. Crit. Care Pain 2008, 8, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Maxim, L.D.; Niebo, R.; Utell, M.J. Screening tests: A review with examples. Inhal. Toxicol. 2014, 26, 811–828. [Google Scholar] [CrossRef]
- Messam, L.L.M.; Branscum, A.J.; Collins, M.T.; Gardner, I.A. Frequentist and Bayesian approaches to prevalence estimation using examples from Johne’s disease. Anim. Health Res. Rev. 2008, 9, 1–23. [Google Scholar] [CrossRef]
- Lang, Z.; Reiczigel, J. Confidence limits for prevalence of disease adjusted for estimated sensitivity and specificity. Prev. Vet. Med. 2014, 113, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Sanogo, M.; Abatih, E.; Saegerman, C. Bayesian versus frequentist methods for estimating disease true prevalence and 4 diagnostic test performance. Vet. J. 2014, 202, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Joseph, L.; Gyorkos, T.W.; Coupal, L. Bayesian estimation of disease prevalence and the parameters of diagnostic tests in the absence of a gold standard. Am. J. Epidemiol. 1995, 141, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Sergeant, E. Epitools Epidemiological Calculators. Available online: http://epitools.ausvet.com (accessed on 1 July 2020).
- IBM. SPSS Statistics for Windows, Version 24; IBM: Armonk, NY, US, 2016. [Google Scholar]
- Haw, C.; Bergen, H.; Casey, D.; Hawton, K. Repetition of deliberate self-harm: A study of the characteristics and subsequent deaths in patients presenting to a general hospital according to extent of repetition. Suicide Life Threat. Behav. 2007, 37, 379–396. [Google Scholar] [CrossRef]
- Ting, S.A.; Sullivan, A.F.; Boudreaux, E.D.; Miller, I.; Camargo, C.A., Jr. Trends in US emergency department visits for attempted suicide and self-inflicted injury, 1993–2008. Gen. Hosp. Psychiatry 2012, 34, 557–565. [Google Scholar] [CrossRef]
- Milner, A.; Niven, H.; LaMontagne, A.D. Occupational class differences in suicide: Evidence of changes over time and during the global financial crisis in Australia. BMC Psychiatry 2015, 15, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Bruffaerts, R.; Demyttenaere, K.; Hwang, I.; Chiu, W.-T.; Sampson, N.; Kessler, R.C.; Alonso, J.; Borges, G.; de Girolamo, G.; de Graaf, R. Treatment of suicidal people around the world. Br. J. Psychiatry 2011, 199, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Hom, M.A.; Stanley, I.H.; Joiner, T.E., Jr. Evaluating factors and interventions that influence help-seeking and mental health service utilization among suicidal individuals: A review of the literature. Clin. Psychol. Rev. 2015, 40, 28–39. [Google Scholar] [CrossRef]
- Stanley, B.; Brown, G.K.; Currier, G.W.; Lyons, C.; Chesin, M.; Knox, K.L. Brief intervention and follow-up for suicidal patients with repeat emergency department visits enhances treatment engagement. Am. J. Public Health 2015, 105, 1570–1572. [Google Scholar] [CrossRef]
- Queensland Health. Suicide Prevention in Health Services Initiative, Year 1 Progress Report 2016–2017; Queensland Health: Brisbane, Australia, 2018. [Google Scholar]
- Qin, P.; Agerbo, E.; Mortensen, P.B. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A national register–based study of all suicides in Denmark, 1981–1997. Am. J. Psychiatry 2003, 160, 765–772. [Google Scholar] [CrossRef]
- Mergl, R.; Havers, I.; Althaus, D.; Rihmer, Z.; Schmidtke, A.; Lehfeld, H.; Niklewski, G.; Hegerl, U. Seasonality of suicide attempts: Association with gender. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, R.; Epstein, S.; Dutta, R.; Ougrin, D. Social media, internet use and suicide attempts in adolescents. Curr. Opin. Psychiatry 2019, 32, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Larkin, G.L.; Smith, R.P.; Beautrais, A.L. Trends in US emergency department visits for suicide attempts, 1992–2001. Crisis 2008, 29, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kolves, K.; De Leo, D. Are immigrants responsible for the recent decline in Australian suicide rates? Epidemiol. Psychiatr Sci. 2015, 24, 241–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selkirk, M.; Quayle, E.; Rothwell, N. A systematic review of factors affecting migrant attitudes towards seeking psychological help. J. Health Care Poor Underserved 2014, 25, 94–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrelly, T. The Aboriginal suicide and self-harm help-seeking quandary. AIHWJ 2008, 32, 11. [Google Scholar]
- De Leo, D.; Sveticic, J.; Milner, A. Suicide in Indigenous people in Queensland, Australia: Trends and methods, 1994–2007. Aust. N. Z. J. Psychiatry 2011, 45, 532–538. [Google Scholar] [CrossRef]
- Vicary, D.; Westerman, T. That’s just the way he is’: Some implications of Aboriginal mental health beliefs. AeJAMH 2004, 3, 103–112. [Google Scholar] [CrossRef]
- Nagel, T. Involuntary mental health treatment in the remote Northern Territory. Psychiatry Psychol. Law 2003, 10, 171–178. [Google Scholar] [CrossRef]
- Cantor, C.; Hickey, P.; De Leo, D. Seasonal variation in suicide in a predominantly Caucasian tropical/subtropical region of Australia. Psychopath 2000, 33, 303–306. [Google Scholar] [CrossRef]
- Law, C.-K.; De Leo, D. Seasonal differences in the day-of-the-week pattern of suicide in Queensland, Australia. Int. J. Environ. Res. Public Health 2013, 10, 2825–2833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.C.; Huang, N.E.; Peng, C.-K.; Tsai, S.-J. Do seasons have an influence on the incidence of depression? The use of an internet search engine query data as a proxy of human affect. PLoS ONE 2010, 5, e13728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, J.; Jessup, M.; Crilly, J.; Green, D.; Lind, J.; Wallis, M.; Miller, P.; Fitzgerald, G. Predicting emergency department admissions. Emerg. Med. J. 2012, 29, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crilly, J.; Ranse, J.; Bost, N.; Donnelly, T.; Timms, J.; Gilmour, K.; Aitken, M.; Johnston, A. Emergency healthcare delivery for young adults during a planned mass gathering: A retrospective observational study. Emerg. Med. Australas 2020, 32, 250–257. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, M.; Harriss, L.; Mills, J.; Thompson, F.; McDermott, R. Validating Indigenous status in a regional Queensland hospital emergency department dataset with patient-linked data. Med. J. Aust. 2020, 212, 230–231. [Google Scholar] [CrossRef]
- Tran, D.T.; Jorm, L.; Lujic, S.; Bambrick, H.; Johnson, M. Country of birth recording in Australian hospital morbidity data: Accuracy and predictors. Aust. N. Z. J. Public Health 2012, 36, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Queensland Health. Aboriginal and Torres Strait Islander Mental Health Strategy 2016–2021; Aboriginal and Torres Strait Islander Health Branch, Department of Health: Brisbane, Australia, 2016. [Google Scholar]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Saxon, V.; Mukherjee, D.; Thomas, D. Behavioral Health Crisis Stabilization Centers: A New Normal. J. Ment. Health Clin. Psychol. 2018, 2, 23–26. [Google Scholar] [CrossRef]
- Witt, K.; Robinson, J. Sentinel surveillance for self-harm. Crisis 2019, 40, 1–6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year | Suicidal Presentations N (95% CDI) | All ED Presentations | Suicidal Presentations as % of All ED | Gold Coast Population | Rates of Suicidal Presentations (Per 100,000 Population) | ||
|---|---|---|---|---|---|---|---|
| Males | Females | Persons | |||||
| 2009 | 1446 (1334–1557) | 111,201 | 1.3 | 495,835 | 258.0 | 299.8 | 291.6 |
| 2010 | 1652 (1542–1762) | 110,114 | 1.5 | 506,135 | 294.0 | 334.6 | 326.3 |
| 2011 | 2089 (2090–2205) | 116,055 | 1.8 | 515,202 | 374.9 | 411.3 | 405.5 |
| 2012 | 2467 (2468–2590) | 123,346 | 2.0 | 528,342 | 406.9 | 501.0 | 466.9 |
| 2013 | 2798 (2664–2931) | 133,231 | 2.1 | 540,687 | 450.6 | 533.7 | 517.5 |
| 2014 | 3376 (3230–3523) | 146,800 | 2.3 | 550,718 | 568.1 | 630.5 | 613.1 |
| 2015 | 3756 (3599–3912) | 156,487 | 2.4 | 561,629 | 597.6 | 709.6 | 668.7 |
| 2016 | 4246 (4083–4410) | 163,319 | 2.6 | 575,303 | 698.0 | 720.7 | 738.1 |
| 2017 | 4884 (4716–5052) | 168,416 | 2.9 | 591,356 | 785.7 | 809.0 | 825.9 |
| 2018 | 5380 (5207–5554) | 173,549 | 3.1 | 606,774 | 873.4 | 871.4 | 886.7 |
| 2009–2018 | 32,094 (30,855–35,063) | 1,402,521 | 2.2 | 5,471,981 | 542.5 | 594.8 | 586.5 |
| N1 (Persons) | 1 Presentation N(%) | 2–4 Presentations N(%) | 5 or More Presentations N(%) | |
|---|---|---|---|---|
| All persons | 21,220 | 14,974 (70.6%) | 5028 (23.7%) | 1218 (5.7%) |
| Sex | ||||
| Males | 10,341 | 7360 (71.2%) | 2402 (23.2%) | 579 (5.6%) |
| Females | 11,249 | 7928 (70.5%) | 2676 (23.8%) | 644 (5.7%) |
| Age groups 2 | ||||
| Under 15 | 886 | 558 (62.9%) | 231 (26.0%) | 98 (11.0%) |
| 15–24 | 6752 | 4542 (67.3%) | 1692 (25.1%) | 519 (7.7%) |
| 25–34 | 4738 | 3396 (71.7%) | 1070 (22.6%) | 273 (5.8%) |
| 35–44 | 4000 | 2831 (70.8%) | 978 (24.4%) | 192 (4.8%) |
| 45–54 | 2817 | 2030 (72.0%) | 623 (22.1%) | 165 (5.8%) |
| 55–64 | 1291 | 967 (74.9%) | 275 (21.3%) | 49 (3.8%) |
| 65 + | 953 | 831 (87.2%) | 112 (11.8%) | 10 (1.1%) |
| Country of birth | ||||
| Australian-born | 16,752 | 11,599 (69.2%) | 4126 (24.6%) | 1027 (6.1%) |
| Overseas-born | 4789 | 3651 (76.2%) | 943 (19.7%) | 194 (4.1%) |
| Indigenous status | ||||
| Indigenous | 746 | 450 (60.4%) | 223 (29.8%) | 73 (9.8%) |
| Non-Indigenous | 20,568 | 14,605 (71.0%) | 4817 (23.4%) | 1146 (5.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stapelberg, N.J.C.; Sveticic, J.; Hughes, I.; Turner, K. Suicidal Presentations to Emergency Departments in a Large Australian Public Health Service over 10 Years. Int. J. Environ. Res. Public Health 2020, 17, 5920. https://doi.org/10.3390/ijerph17165920
Stapelberg NJC, Sveticic J, Hughes I, Turner K. Suicidal Presentations to Emergency Departments in a Large Australian Public Health Service over 10 Years. International Journal of Environmental Research and Public Health. 2020; 17(16):5920. https://doi.org/10.3390/ijerph17165920
Chicago/Turabian StyleStapelberg, Nicolas J.C., Jerneja Sveticic, Ian Hughes, and Kathryn Turner. 2020. "Suicidal Presentations to Emergency Departments in a Large Australian Public Health Service over 10 Years" International Journal of Environmental Research and Public Health 17, no. 16: 5920. https://doi.org/10.3390/ijerph17165920