Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking


Abstract
:1. Introduction
2. Methods
2.1. Characteristics of Participants
2.2. Screening Questionnaire
2.3. Healthcare
2.4. Statistical Analysis
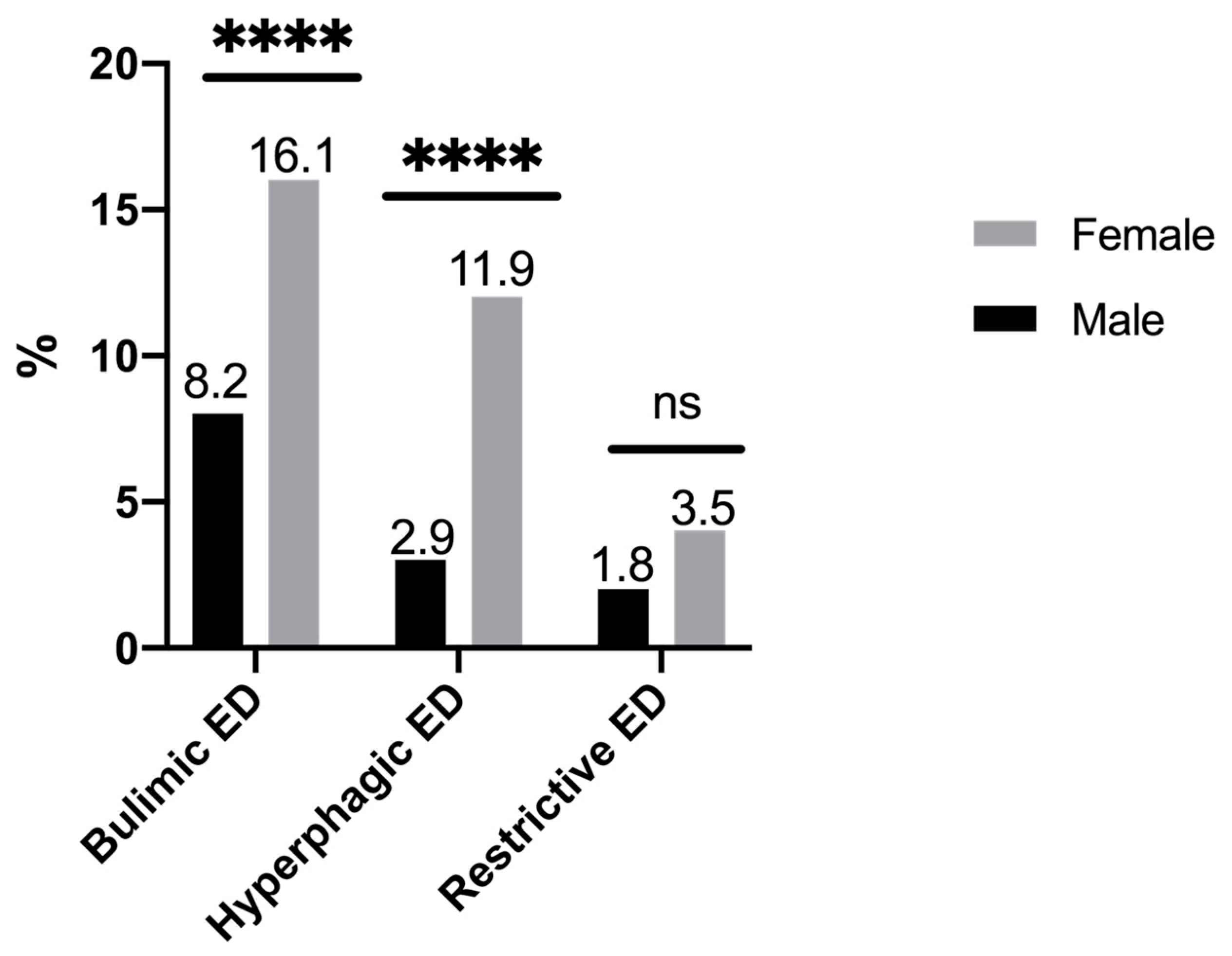
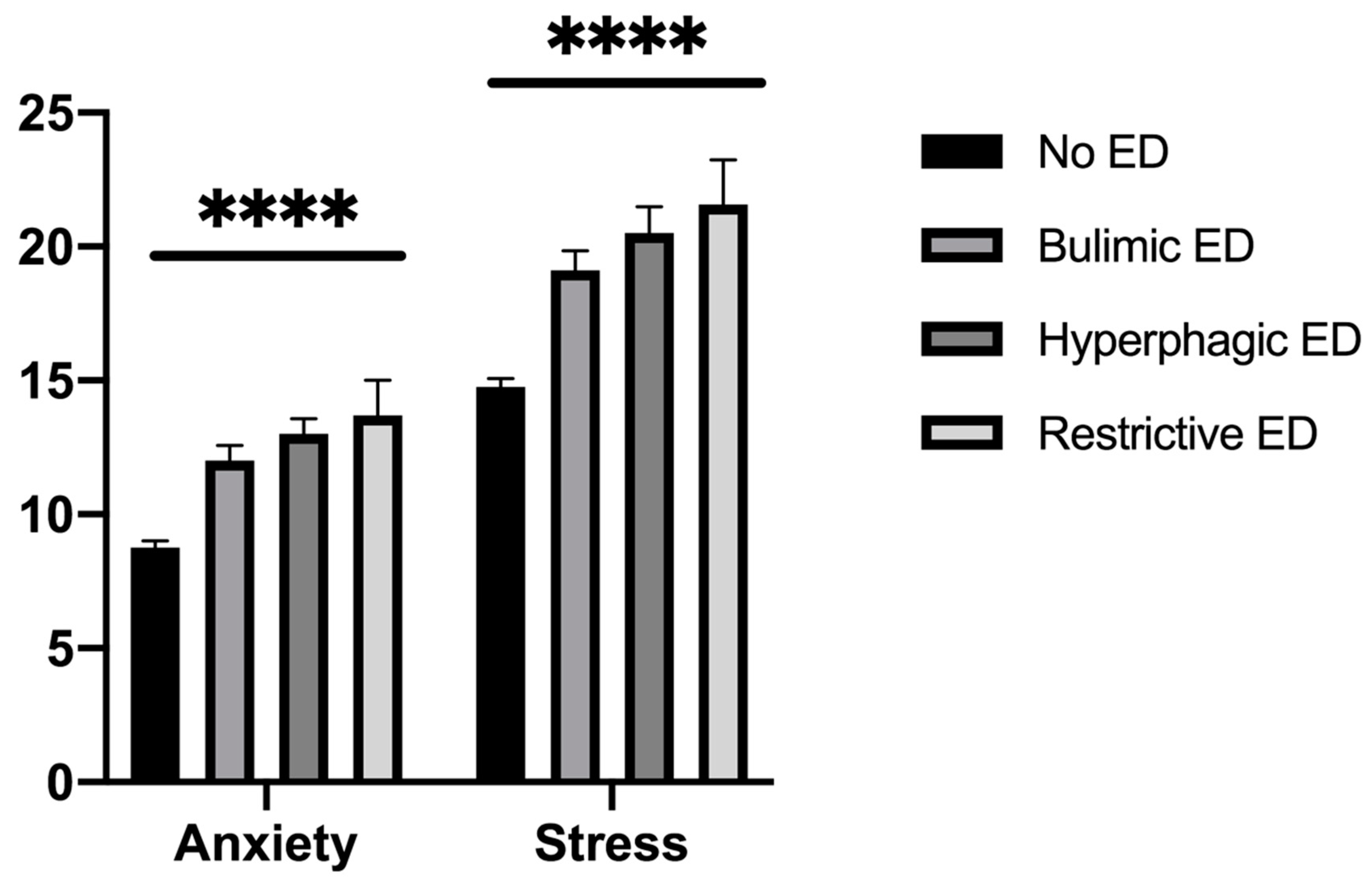
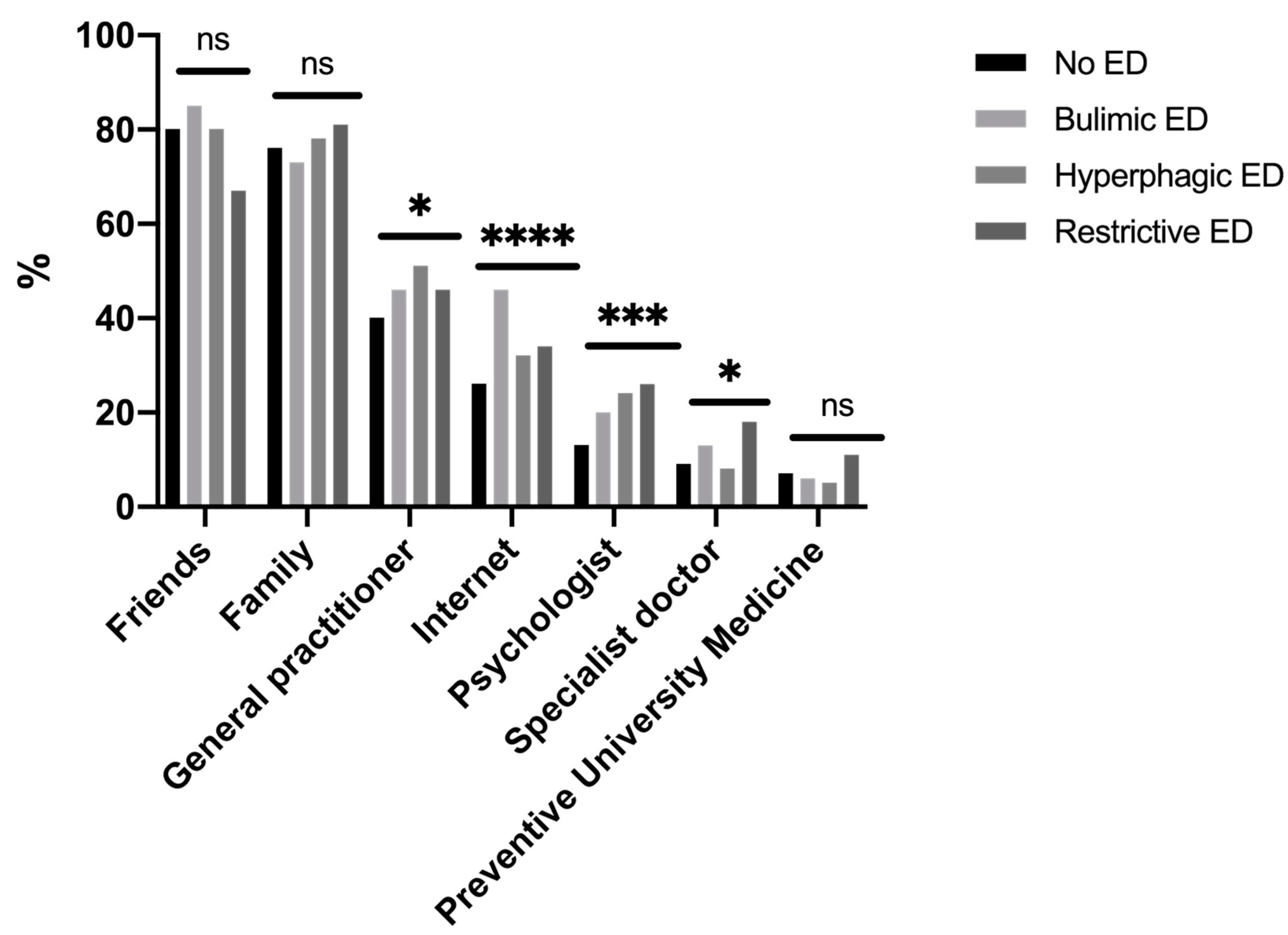
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM–5; American Psychiatric Pub: Arlington, VA, USA, 2013. [Google Scholar]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 5, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Potterton, R.; Richards, K.; Allen, K.; Schmidt, U. Eating disorders during emerging adulthood: A systematic scoping review. Front. Psychol. 2020, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 7, 714–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipson, S.; Sonneville, K. Eating disorder symptoms among undergraduate and graduate students at 12 U.S. colleges and universities. Eat. Behav. 2017, 24, 81–88. [Google Scholar] [CrossRef]
- Tavolaccci, M.-P.; Grigioni, S.; Richard, L.; Meyrignac, G.; Déchelotte, P.; Ladner, J. Eating disorders and behaviors among college students. J. Nutr. Educ. Behav. 2015, 47, 412–420. [Google Scholar] [CrossRef]
- Andreeva, V.A.; Tavolacci, M.-P.; Galan, P.; Ladner, J.; Buscail, C.; Péneau, S.; Galmiche, M.; Hercberg, S.; Déchelotte, P.; Julia, C. Sociodemographic correlates of eating disorder subtypes among men and women in France, with a focus on age. J. Epidemiol. Community Health 2018, 73, 56–64. [Google Scholar] [CrossRef]
- Arnett, J.J.; Jensen, A.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Misra, R.; McKean, M. College students’academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am. J. Health Stud. 2000, 16, 41–51. [Google Scholar]
- Trigueros, R.; Aguilar-Parra, J.; Cangas, A.J.; Bermejo, R.; Ferrandiz, C.; López-Liria, R. Influence of emotional intelligence, motivation and resilience on academic performance and the adoption of healthy lifestyle habits among adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2810. [Google Scholar] [CrossRef] [Green Version]
- Claydon, E.; Zullig, K.J. Eating disorders and academic performance among college students. J. Am. Coll. Health 2019, 68, 320–325. [Google Scholar] [CrossRef]
- Keski-Rahkonen, A.; Mustelin, L. Epidemiology of eating disorders in Europe. Curr. Opin. Psychiatry 2016, 29, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, J.; Behan, L.; Kelly, P.; McCarthy, K.; Horgan, A. Help-seeking behaviors and mental well-being of first year undergraduate university students. Psychiatry Res. Neuroimaging 2016, 246, 129–135. [Google Scholar] [CrossRef]
- Després, C.; Dourgnon, P.; Fantin, R.; Jusot, F. Healthcare renunciation: A socio-anthropological approach. Health Econ. 2011, 169, 1–7. [Google Scholar]
- Baggio, S.; Iglesias, K.; Fernex, A. Healthcare renunciation among young adults in French higher education: A population-based study. Prev. Med. 2017, 99, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Lipson, S.K.; Jones, J.M.; Taylor, C.B.; Wilfley, D.E.; Eichen, D.M.; Fitzsimmons-Craft, E.E. Eisenberg D6 understanding and promoting treatment-seeking for eating disorders and body image concerns on college campuses through online screening, prevention and intervention. Eat Behav. 2017, 25, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, D.; Workman, C.; Mehler, P.S. Medical complications of anorexia nervosa and bulimia nervosa. Psychiatr. Clin. North Am. 2019, 2, 263–274. [Google Scholar] [CrossRef]
- Sysko, R.; Walsh, B.T. Does the broad categories for the diagnosis of eating disorders (BCD-ED) scheme reduce the frequency of eating disorder not otherwise specified? Int. J. Eat. Disord. 2010, 44, 625–629. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.E.; Jd, A.H.A.; Ba, A.P.; Fay, K.; Striegel-Moore, R.H. A qualitative study of perceived social barriers to care for eating disorders: Perspectives from ethnically diverse health care consumers. Int. J. Eat. Disord. 2009, 43, 633–647. [Google Scholar] [CrossRef] [Green Version]
- Ali, K.; Farrer, L.; Fassnacht, D.B.; Gulliver, A.; Griffiths, K.M.; Bauer, S. Perceived barriers and facilitators towards help-seeking for eating disorders: A systematic review. Int. J. Eat. Disord. 2016, 50, 9–21. [Google Scholar] [CrossRef]
- Garcia, F.D.; Grigioni, S.; Allais, E.; Houy-Durand, E.; Thibaut, F.; Déchelotte, P. Detection of eating disorders in patients: Validity and reliability of the French version of the SCOFF questionnaire. Clin. Nutr. 2011, 30, 178–181. [Google Scholar] [CrossRef]
- Botella, J.; Sepúlveda, A.R.; Huang, H.; Gambara, H. A Meta-Analysis of the Diagnostic Accuracy of the SCOFF. Span. J. Psychol. 2013, 16, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavolacci, M.-P.; Gillibert, A.; Soubise, A.Z.; Grigioni, S.; Déchelotte, P. Screening four broad categories of eating disorders: Suitability of a clinical algorithm adapted from the SCOFF questionnaire. BMC Psychiatry 2019, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression, Anxiety, Stress, Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 2004. [Google Scholar]
- Allison, K.C.; Spaeth, A.; Hopkins, C.M. Sleep and eating disorders. Curr. Psychiatry Rep. 2016, 18. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; Thurston, I.B.; Karazsia, B.T.; Woolridge, D.; Buckelew, S.M.; Murray, S.B.; Calzo, J.P. Self-reported eating disorders and sleep disturbances in young adults: A prospective cohort study. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kristanto, T.; Chen, W.S.; Thoo, Y.Y.; Tommy, K. Academic burnout and eating disorder among students in Monash University Malaysia. Eat. Behav. 2016, 22, 96–100. [Google Scholar] [CrossRef]
- Trigueros, R.; Padilla, A.M.; Aguilar-Parra, J.M.; Rocamora-Pérez, P.; Morales-Gázquez, M.J.; López-Liria, R. The influence of emotional intelligence on resilience, test anxiety, academic stress and the mediterranean diet. A Study with university students. Int. J. Environ. Res. Public Health 2020, 17, 2071. [Google Scholar] [CrossRef] [Green Version]
- Serra, R.; Kiekens, G.; Vanderlinden, J.; Vrieze, E.; Auerbach, R.P.; Benjet, C.; Claes, L.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; et al. Binge eating and purging in first-year college students: Prevalence, psychiatric comorbidity, and academic performance. Int. J. Eat. Disord. 2019, 53, 339–348. [Google Scholar] [CrossRef]
- Tillman, K.S.; Sell, D.M. Help-seeking intentions in college students: An exploration of eating disorder specific help-seeking and general psychological help-seeking. Eat. Behav. 2013, 14, 184–186. [Google Scholar] [CrossRef]
- Thomas, S.J.; Caputi, P.; Wilson, C.J. Specific attitudes which predict psychology students’ intentions to seek help for psychological distress. J. Clin. Psychol. 2014, 3, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Cadwallader, J.-S.; Godart, N.; Chastang, J.; Falissard, B.; Huas, C. Detecting eating disorder patients in a general practice setting: A systematic review of heterogeneous data on clinical outcomes and care trajectories. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2016, 21, 365–381. [Google Scholar] [CrossRef]
- Ali, K.; Fassnacht, D.B.; Farrer, L.; Rieger, E.; Feldhege, J.; Moessner, M.; Griffiths, K.M.; Bauer, S. What prevents young adults from seeking help? Barriers toward help-seeking for eating disorder symptomatology. Int. J. Eat. Disord. 2020, 53, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.P.; Bruffarets, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an internet—And app-based intervention for college students with elevated stress: Randomized controlled trial. J. Med. Internet Res. 2018, 20, e136. [Google Scholar] [CrossRef] [PubMed]
- Lindenberg, K.; Moessner, M.; Harney, J.; McLaughlin, O.; Bauer, S. E-Health for individualized prevention of eating disorders. Clin. Pr. Epidemiol. Ment. Health 2011, 7, 74–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindermann, S.; Moessner, M.; Ozer, F.; Bauer, S. Associations between eating disorder related symptoms and participants’ utilization of an individualized internet-based prevention and early intervention program. Int. J. Eat. Disord. 2017, 50, 1215–1221. [Google Scholar] [CrossRef]
- Utz, S.; Breuer, J. The relationship between use of social network sites, online social support, and well-being. J. Media Psychol. 2017, 29, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Nishida-Hikiji, E.; Okamoto, M.; Iwanaga, R.; Nakane, H.; Tanaka, G. Mental health literacy regarding eating disorders in female Japanese university students. Eat. Disord. 2019, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bullivant, B.; Rhydderch, S.; Griffiths, S.; Mitchison, D.; Mond, J.M. Eating disorders “mental health literacy”: A scoping review. J. Ment. Health 2020, 29, 336–349. [Google Scholar] [CrossRef]
- Coffino, J.A.; Udo, T.; Grilo, C.M. Rates of help-seeking in us adults with lifetime dsm-5 eating disorders: Prevalence across diagnoses and differences by sex and ethnicity/race. Mayo Clin. Proc. 2019, 94, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Byrne, M.; Rodebaugh, T.L. Shame and guilt as shared vulnerability factors: Shame, but not guilt, prospectively predicts both social anxiety and bulimic symptoms. Eat. Behav. 2016, 22, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Mortier, P.; Kählke, F.; Bruffaerts, R.; Baumeister, H.; Auerbach, R.P.; Alonso, J.; Vilagut, G.; Martínez, K.U.; Lochner, C.; et al. Barriers of mental health treatment utilization among first-year college students: First cross-national results from the WHO world mental health international college student initiative. Int. J. Methods Psychiatr. Res. 2019, 28, e1782. [Google Scholar] [CrossRef] [Green Version]
- Harrer, M.; Adam, S.H.; Messner, E.; Baumeister, H.; Cuijpers, P.; Bruffaerts, R.; Auerbach, R.P.; Kessler, R.C.; Jacobi, C.; Taylor, C.B.; et al. Prevention of eating disorders at universities: A systematic review and meta-analysis. Int. J. Eat. Disord. 2020, 53, 813–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://formation-ve.univ-rouen.fr/synthese-des-effectifs-d-etudiants-603789.kjsp?RH=1377093897174 (accessed on 3 August 2020).
- Hauschildt, K.; Gwosć, K.; Netz, N.; Mishra, S. Social and Economic Conditions of Student Life in Europe. EUROSTUDENT V 2016–2018. Available online: https://www.eurostudent.eu/download_files/documents/EUROSTUDENT_VI_Synopsis_of_Indicators.pdf (accessed on 6 May 2020).
- Mitrofan, O.; Petkova, H.; Janssens, A.; Kelly, J.; Edwards, E.; Nicholls, D.; McNicholas, F.; Simic, M.; Eisler, I.; Ford, T.; et al. Care experiences of young people with eating disorders and their parents: Qualitative study. BJPsych Open 2019, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Markey, M.A.; Wal, J.S.V. The role of emotional intelligence and negative affect in bulimic symptomatology. Compr. Psychiatry 2007, 48, 458–464. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No Eating Disorder (n = 1123) | Bulimic EDs (n = 198) | Hyperphagic EDs (n = 129) | Restrictive EDs (n = 43) | Total (n = 1493) | p |
|---|---|---|---|---|---|---|
| Age mean (SD) | 20.1 (1.9) | 20.0 (1.9) | 20.3 (1.9) | 19.8 (1.9) | 20.1 (1.9) | 0.26 |
| Women (%) | 57.7 | 77.3 | 87.6 | 76.7 | 63.4 | <0.0001 |
| Living with parents (%) | 69.4 | 71.2 | 69.0 | 65.1 | 69.5 | 0.88 |
| Courses (%) | 0.003 | |||||
| University | 61.8 | 55.0 | 46.5 | 58.1 | 59.5 | |
| Engineering | 17.8 | 16.7 | 19.4 | 11.7 | 17.6 | |
| Healthcare | 20.4 | 28.3 | 34.1 | 30.2 | 22.9 | |
| Financial difficulties (%) | 21.5 | 31.8 | 33.3 | 27.9 | 24.0 | 0.001 |
| BMI, kg/m2 mean (SD) | 22.0 (3.3) | 22.3 (2.8) | 26.6 (5.1) | 19.5 (2.4) | 22.4 (3.7) | <0.0001 |
| Class of BMI (%) | <0.0001 | |||||
| Underweight | 9.5 | 0.0 | 0.0 | 51.2 | 8.6 | |
| Normal weight | 77.0 | 93.0 | 31.8 | 48.8 | 74.4 | |
| Overweight | 10.1 | 4.0 | 49.6 | 0.0 | 12.4 | |
| Obese | 3.4 | 3.0 | 18.6 | 0.0 | 4.6 | |
| Unbearable academic pressure (%) | 21.5 | 34.3 | 38.8 | 37.2 | 25.2 | <0.0001 |
| Restless sleep | 19.9 | 31.9 | 30.6 | 41.0 | 23.0 | <0.0001 |
| GP visit * (%) | 83.4 | 86.3 | 86.0 | 86.0 | 84.1 | 0.66 |
| Foregone care * (%) | 18.6 | 34.8 | 30.2 | 32.6 | 21.9 | <0.0001 |
| Characteristics | No eating Disorder (n = 1123) | Bulimic EDs (n = 198) AOR (95%CI) | Hyperphagic EDs (n = 129) AOR (95%CI) | Restrictive EDs (n = 43) AOR (95%CI) |
|---|---|---|---|---|
| Women | Ref | 2.20 (1.50–3.22) | 4.04 (2.32–7.03) | 1.83 (0.85–3.95) |
| Courses | Ref | |||
| University | Ref | Ref | Ref | |
| Engineering | 1.11 (0.71–1.74) | 1.51 (0.90–2.55) | 0.16 (0.02–1.21) | |
| Healthcare | 1.14 (0.77–1.68) | 1.50 (0.96–2.34) | 1.30 (0.63–2.68) | |
| Financial difficulties | Ref | 1.29 (0.90–1.84) | 1.48 (0.97–2.25) | 1.20 (0.58–2.45) |
| Unbearable academic pressure | Ref | 1.47 (1.03–2.09) | 1.76 (1.17–2.66) | 1.63 (0.82–3.24) |
| Restless sleep | Ref | 1.61 (1.12–2.31) | 1.56 (1.01–2.42) | 2.22 (1.12–4.40) |
| Healthcare renunciation | Ref | 1.91 (1.34–2.72) | 1.36 (0.88–2.10) | 1.66 (0.82–3.24) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavolacci, M.-P.; Déchelotte, P.; Ladner, J. Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking. Int. J. Environ. Res. Public Health 2020, 17, 5914. https://doi.org/10.3390/ijerph17165914
Tavolacci M-P, Déchelotte P, Ladner J. Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking. International Journal of Environmental Research and Public Health. 2020; 17(16):5914. https://doi.org/10.3390/ijerph17165914
Chicago/Turabian StyleTavolacci, Marie-Pierre, Pierre Déchelotte, and Joel Ladner. 2020. "Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking" International Journal of Environmental Research and Public Health 17, no. 16: 5914. https://doi.org/10.3390/ijerph17165914