1. Introduction
How crisis events affect mental health has been widely studied by academia [
1,
2,
3,
4,
5,
6,
7,
8]. Because crisis events may change people’s daily lives or even threaten their safety, the mental health of people suffering from such crises should be particularly noted. Currently, the world is experiencing a serious public health crisis: the spread of COVID-19. Because of the significant threat of this virus, for the first time in human history, the Chinese government decided to lock down Wuhan City from 23 January to 8 April 2020. This strategy was followed by many countries as the virus spread globally. To date, this public health crisis has had a significant impact on the global population. For example, since the outbreak of the virus, more than 4 million people have been infected, and nearly 500,000 people had died of infection by 28 June 2020 [
9]. Furthermore, the World Bank predicted that the world economy will shrink by 5.2% in 2020 because of this pandemic [
10].
The mental health of the public might be affected by the outbreak of COVID-19. Previous studies have investigated the effect on mental health of crisis events such as economic crises, natural disasters, and war and terrorist attacks [
3,
4,
6,
7,
11,
12,
13,
14,
15,
16,
17]. However, the effect of public health crises on mental health has not received sufficient attention. With the large number of casualties and significant economic losses resulting from the COVID-19 crisis, people who experience it may suffer great psychological distress. Furthermore, lockdown and quarantine policies cause substantial disturbance to people’s daily lives. Therefore, it is important to understand how these policies affect the mental health of people during this public health crisis. Under such circumstances, the aims of this study are to (1) construct a conceptual framework for risk perception and depression of people in a public health crisis, (2) examine how the mental health of people in the COVID-19 crisis is affected by risk perception and its associated factors, including distance perception of the crisis and support of prevention and control policies, and (3) propose policy recommendations on how to deal with psychological problems in the current COVID-19 crisis.
The remainder of this paper is organized as follows:
Section 2 reviews previous studies on the ways in which economic crises, natural disasters, and war and terrorist attacks affect mental health.
Section 3 presents a theoretical framework of risk perception and the mental health of people in a public health crisis.
Section 4 explains the research design.
Section 5 presents the results of structural equation modeling on risk perception and mental health based on online survey data.
Section 6 summarizes the main findings of this study and provides theoretical reflections and policy implications.
2. Literature Review
How crisis events may affect mental health has been widely examined by researchers globally. Previous studies have focused on the effects of three types of crisis events: economic crises, natural disasters, and war and terrorist attacks. Similar to the COVID-19 crisis, these three types of crisis usually cause huge economic losses or human casualties in a relatively short period of time. Thus, crises such as these usually have a negative impact on the psychological wellbeing of people. However, since the three types of crisis events are different in terms of degree of harm, scope of influence, and duration, the ways that different crisis events affect the mental health of people are also distinctive.
An economic crisis is a type of crisis that may typically be associated with mental health. Economic crises cause incomes to fall and unemployment, thus leading to a decline in living conditions. Researchers have shown that socioeconomic factors are related to happiness and the subjective wellbeing of people [
18,
19,
20]. If a person’s standard of living declines sharply in a short period during an economic crisis, their mental health could be worse than prior to the crisis. Studies show that the mental health of people suffers in economic crises [
8,
12]. However, this decline only lasts for a short period. After a stage of adaptation, people’s mental health during an economic crisis returns to the level that prevailed before the crisis [
21,
22].
Natural disasters are the second main type of crisis that may affect people’s mental health. Natural disasters such as tsunamis, earthquakes, floods, and volcanic eruptions threaten people’s lives and property safety. Moreover, disasters are usually difficult to predict. They often occur suddenly. Thus, the mental state of people is greatly stimulated in a short period of time. Some people may experience mental breakdown because of overstimulation. Studies of the 2004 tsunami in Southeast Asia, the 2008 Wenchuan earthquake, and the 2011 earthquake of the Pacific coast of Tōhoku all show that the mental health of people impacted by these natural disasters worsened significantly [
2,
3,
11,
17,
23,
24,
25,
26]. In addition, people’s mental health during these natural disasters may vary by gender, socioeconomic status, and age [
2,
3,
17]. Moreover, social support and policy support may alleviate the mental distress of people suffering from natural disasters [
2].
War and territorial attacks are the third type of crisis that is possibly associated with people’s mental health. In the present day, humans live in a world with uncertainties. War and terrorist attacks may put people at risk at any time. The September 11 attacks is a typical example. The incident resulted in a large number of casualties and caused great economic losses. Nearly 3000 people were killed and, in New York city after the attacks, more than 140,000 jobs were lost in the first month, and
$2.8 billion in wages in the first three months [
27]. A number of studies have shown that people who experienced the September 11 attacks have mental health problems [
15,
16,
28]. Other studies have also reached similar conclusions based on people who also experienced war or territorial attacks [
14]. Furthermore, the negative effect of war and territorial attacks on mental health could last for a long time. For instance, Wang and Yang showed that the mental health problems of people who experienced the September 11 attacks also resulted from the effect of an external traumatic event [
28].
Although previous studies have paid significant attention to the association between crisis events and mental health, minimal attention has been paid to the relationship between public health crises and mental health. Given the great influence of COVID-19 on people globally, investigating how COVID-19 may affect the mental health of people is an urgent issue. Precious studies have investigated how the COVID-19 crisis, particularly the lockdown and quarantine policies, affects people’s mental health [
1,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39]. However, few studies have shown how the risk perception of COVID-19 may affect people’s mental health.
Accordingly, this study sought to explore the effect of risk perception and its associated factors on depression in the COVID-19 crisis. This study is different from previous studies because it treated risk perception of public health crises as a potential factor of mental health problems. In addition, because risk perception is affected by distance perception of public health crises, this study included distance perception in its theoretical framework. Moreover, since prevention and control policies play a vital role in preventing the spread of COVID-19, we incorporated the support of prevention and control policies in the theoretical framework. Using online survey data, hypotheses developed by the theoretical framework were empirically tested. The research findings of this study may contribute to understanding the effect of the public health crisis on mental health in both theory and practice.
3. Conceptual Framework and Hypotheses
Previous research has substantially explored how crisis events may affect mental health, particularly how demographic factors, income, employment, and social support affect mental health. However, in addition to the influence of these factors, the mental health of people involved in the public health crisis may be related to risk perception and the factors associated with it. For example, in the COVID-19 crisis, how the virus spreads may be not very clear, especially at the early stage of the crisis. People generally experience anxiety and restlessness in an uncertain environment. Thus, how people perceive the danger of a public health crisis could be significantly related to their mental health. Moreover, the distance that a public health crisis spreads is a significant factor that affects the relationship between risk perception and mental health [
40]. Therefore, people who are closer to the center of the crisis are more likely to be influenced by the crisis. Additionally, because of the significant role of social and policy support in alleviating the detrimental effect of the disaster on mental health [
2], measures taken by the government to respond to public health crises affect people’s sense of security. In a public health crisis, effective government policies that improve people’s sense of security are more likely to be supported by the public [
41]. In addition, an increase in the public’s sense of security can reduce depression. Therefore, support for prevention and control policies could be significantly associated with the mental health of the public.
The above analysis suggests that there are three core elements in a public health crisis that may affect people’s mental health: distance perception, risk perception, and policy support. Risk perception is defined as people’s subjective judgments of the possible negative consequences of an event [
42]. According to relevant research, risk perception can be divided into two categories: affective risk perception and cognitive risk perception [
43,
44,
45]. Affective risk perception is a type of heuristic information processing that is fast, intuitive, parallel, and spontaneous, and requires little use of cognitive resources. In contrast, cognitive risk perception represents analytical information processing that is slow, cautious, sequential, and controllable, and requires the use of more cognitive resources [
46]. Because of the large differences between affective risk perception and cognitive risk perception, we incorporated both in the analytical framework of this study. Distance perception can be defined as how far people think that they are from the center of the crisis. Since distance perception affects the risk perception of a crisis [
40], it is a significant factor that should be considered in analyzing the relationship between risk perception and people’s mental health. Policy support refers to the extent to which people support policies implemented by the government. Previous studies have shown that risk perception of a public health crisis is associated with policy support [
41]. Usually, when people believe that government responses can effectively cope with the public health crisis, they are more likely to support government policies. Moreover, theoretically, effective policies can strengthen people’s sense of security, thereby helping to reduce anxiety and restlessness. Thus, policy support should be considered in analyzing the relationship between risk perception and the mental health of people.
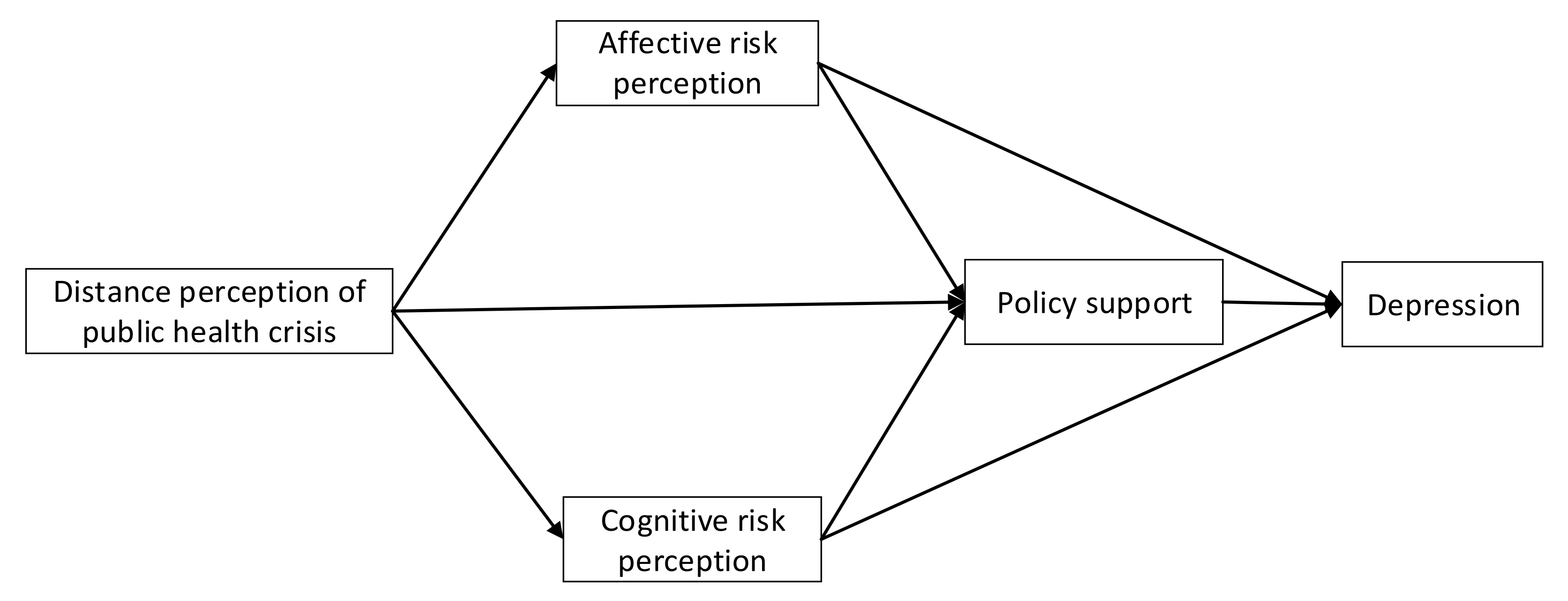
Figure 1 shows the conceptual framework of depression in a public health crisis. Because the links of the five variables are shaped like a diamond, we named this model the diamond model. According to this model, distance perception is the starting point of how a public health crisis may affect mental health. Since individuals who are closer to a crisis are more likely to be affected by it, the anxiety and restlessness of these people should be higher. Thus, we propose the first hypothesis of this study:
Hypothesis 1: The distance perception of a public health crisis is negatively associated with depression among people. The closer the perceived distance, the higher the depression of people.
Risk perception can be divided into affective and cognitive risk perceptions. Because affective risk perception is strongly subjective and often irrational, it will increase the anxiety and restlessness of people. On the contrary, cognitive risk perception is based on the rational judgment of the public health crisis. This rational judgment is based on the scientific basis that is conducive to promoting the correct understanding of public health crises. Therefore, cognitive risk perception should reduce the anxiety and restlessness of people. Based on the above analysis, this study proposes the following two hypotheses:
Hypothesis 2: Affective risk perception is positively associated with depression in public health crises. The higher the affective risk perception, the higher the depression.
Hypothesis 3: Cognitive risk perception is negatively associated with depression in public health crises. The higher the cognitive risk perception, the lower the depression.
In a public health crisis, prevention and control policies play a significant role in relieving anxiety among people. Prevention and control policies at the central, local, and community levels can serve as social-emotional stabilizers. Generally, the effectiveness of prevention and control policies is reflected by the high recognition and support of these policies by the public. In addition, effective prevention and control policies are more likely to reduce public anxiety. On the contrary, ineffective prevention and control policies may lead the public to greater levels of anxiety and restlessness. Therefore, we propose the fourth hypothesis of this study:
Hypothesis 4: Support for prevention and control policies is negatively associated with depression in public health crises. The stronger the support for prevention and control policies, the lower the depression.
6. Discussion
Although previous studies investigated how economic crises, natural disasters, and war and terrorist attacks affected mental health, the effect of public health crises on depression has yet to be explored. This study developed a “diamond model” that linked risk perception of a public health crisis to its associated factors, including distance perception of the crisis and support of prevention and control policies. Using online survey data on adults against the background of the COVID-19 crisis in China, this study empirically tested the hypotheses developed based on the diamond model.
First, this study finds that 25% of respondents reported moderate or severe depression symptoms. This figure is similar to the findings based on surveys in other countries such as Spain and Italy. This means that the psychological wellbeing of people globally is influenced by the COVID-19 crisis. Thus, the mental health problem of the public in the COVID-19 crisis is a global phenomenon and should be paid more attention.
Second, this study reveals that distance perception of the public health crisis is negatively associated with depression of people in public health crises. This finding is in line with the study of Lima, which reported a near-neighbor effect in which the mental health of people living closer to an incinerator is more likely to be affected by the incinerator [
40]. In addition, Wu and colleagues found that, during the 2005 SARS event, respondents who were closer to SARS-related risks were more likely to report mental health problems [
50]. Since epidemic diseases, such as COVID-19 and SARS, are highly contagious, people are very sensitive to highly infectious crowds and high-risk locations because living close to high-risk factors means that they are more likely to be infected. This may explain the negative association between DIP and depression. Results of SEM also suggest that DIP is significantly associated with ARP, CRP, and SPCP. Respondents who have a closer DIP tended to show higher risk perception, both affectively and cognitively. In addition, respondents who have a closer DIP tend to be more likely to support strict prevention and control policies. These two findings reflect that people are more sensitive to the public health crisis when they feel that they live close to high-risk places.
Third, this study shows that while ARP is positively related to depression among respondents, CRP is negatively related to depression among respondents. This finding confirms a conclusion of previous studies, namely, that it is highly important to categorize different types of risk perception [
43,
44,
45]. Furthermore, this finding means that ARP and CRP affect respondents’ mental health in totally different ways. Because ARP is a type of heuristic information processing that is fast, intuitive, parallel, and spontaneous, it is a very subjective and irrational type of judgment. Thus, the psychological wellbeing of people in a public health crisis is negatively affected by ARP. In contrast, CRP is a type of information processing that is slow, cautious, sequential, and controllable. Rational cognition is able to help people calm their emotions in public health crises. In addition, this finding means that it is very important to promote the CRP and reduce the ARP of citizens through various interventions in a public health crisis.
Fourth, this study suggests that SPCP is negatively associated with depression among respondents. A recent study showed that quarantine policies have a negative impact on the mental health of university students [
1]. However, the present study shows that if prevention and control policies are effective and supported by people, they can effectively reduce the psychological distress experienced during a public health crisis. A possible explanation for these differences is that quarantine measures usually cause not only physical distancing but also social distancing. While physical distancing may help reduce the spread of the COVID-19 virus, social distancing is detrimental to psychological wellbeing. If prevention and control policies can enforce physical distancing without causing serious social distancing, people will generally regard these policies as a type of social support rather than a social control. Previous studies have shown the importance of social and policy support in alleviating the depression of people who suffer crisis events [
2,
6]. The negative association between SPCP and depression may hint that if people in public health crises support prevention and control policies, they will regard these policies as a sort of social support.
The theoretical implication of this study is that when analyzing how a public health crisis affects the mental health of people, it is important to consider the role of risk perceptions. In particular, risk perceptions should be divided into ARP and CRP because these two types of risk perceptions have distinctive effects on the mental health of people during public health crises. In addition, associated factors of risk perception, including DIP and SPCP, also play a significant role in determining the mental health of people during a public health crisis. DIP significantly affects ARP, CRP, and SPCP, and ARP and CRP significantly influence SPCP. Moreover, DIP, ARP, CRP, and SPCP all significantly affect the mental health of people in a public health crisis. This justifies the diamond model of this study, which links the risk perception of the public health crisis to DIP and SPCP. Therefore, health policies aiming to improve the psychological wellbeing of people in a public health crisis should take risk perception into consideration. Moreover, this model may be extended to predict the mental health of people in other types of public health crises.
This study also has policy implications. First, the negative association between DIP and depression means that, in a public health crisis, people generally require a safe sense of distance. Thus, it is important to enforce physical (but not social) distancing measures in the COVID-19 crisis. Physical isolation measures are useful for blocking the spread of the virus and reducing the possibility of citizens being affected [
51]. Measures such as these may increase the sense of security of the public. As a result, they are less likely to be depressed by the COVID-19 crisis. Second, the distinctive effects of ARP and CRP on depression mean that when a public health crisis happens, it is vital to promote health education among the public. Health education can increase the scientific recognition of the public health crisis among the public. This strategy may effectively reduce ARP and increase CRP of the public, which could help to reduce their anxiety and restlessness. Third, the negative association between SPCP and depression means that it is necessary to conduct policy promotion when implementing the prevention and control policies. When an epidemic prevention policy is well understood by the public, they will tend to support the policies, which is beneficial to their psychological wellbeing.
This study has some limitations. First, data were taken from an online survey that was not based on representative sampling. This issue may cause the empirical analysis to be biased. In addition, this study only collected one wave of survey data. In a public health crisis, people may gradually adapt to the crisis over time; that is, people’s depression may gradually decrease with time. Therefore, a longitudinal research design may better reveal the psychological condition of people during a public health crisis. Moreover, other important issues, such as social capital, community support, and medical resources, are significant factors that may influence the mental health of people during a public health crisis. However, these factors were not included in the empirical analysis of our study. Our future study will be dedicated to revealing the mental health of people in a public health crisis using a more elaborate research design.


{kind=link}
{kind=link}
{kind=link}


