Evaluation of a Cervical Stabilization Exercise Program for Pain, Disability, and Physical Impairments in University Violinists with Nonspecific Neck Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Outcome Measures
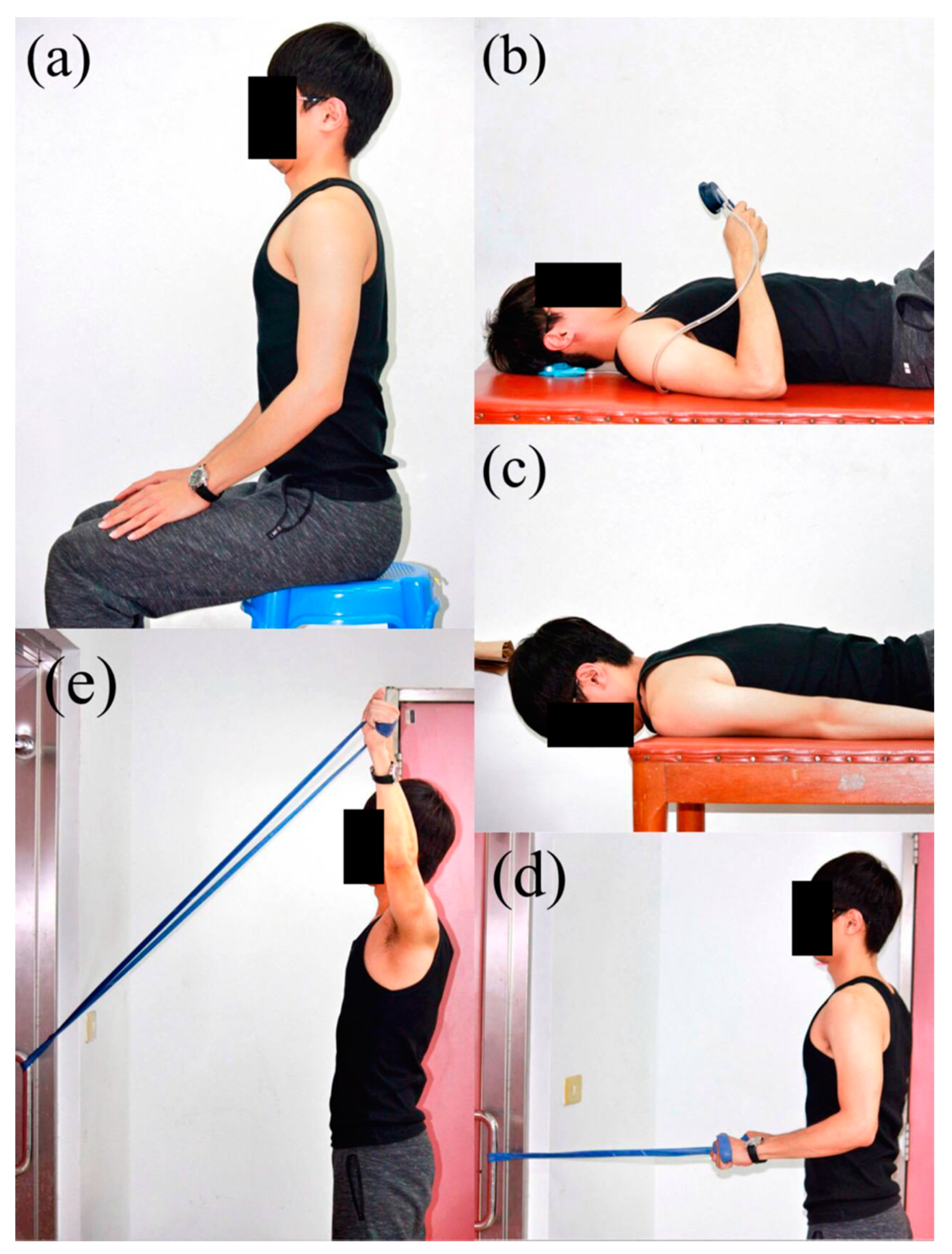
- Craniocervical flexion test: The craniocervical flexion test was used to assess the neuromuscular control of deep cervical flexors [18]. Participants performed a gentle head nodding action and increased the pressure reading of the pressure biofeedback unit (Stabilizer, Chattanooga Group, Dallas, TX) in 5 test increments (22, 24, 26, 28, and 30 mmHg) in a hook-lying position. Each test increment was held for 10 s with 10 s of rest between increments, and the highest achievable pressure was recorded. The craniocervical flexion test has been shown with good construct validity and moderate to good intra-rater reliability, and its MCID is 2 mmHg [18,19].
- Cervical muscle endurance tests: Cervical muscle endurance tests were measured using a stopwatch for the successful time holding the tested position [19,20]. The cervical flexors endurance test was performed in a hook-lying position by lifting the head and neck approximately 2.5 cm off the plinth while maintaining the chin tucked. The cervical extensors endurance test was performed in a prone position with the head protruding from the plinth while retracting the chin and holding the head horizontally. The minimal detectable change (MDC) for the cervical flexors endurance test is 17.8 sec [20], and the MCID for the cervical extensors endurance test is 73 sec [19].
- Cervical range of motion: Cervical range of motion was examined using a validated cervical range-of-motion device (Performance Attainment Associates, Lindstrom, MN) [21]. Participants moved their heads from their own natural neutral position into maximal flexion, extension, left lateral flexion, right lateral flexion, left rotation, and right rotation positions. The MDC for cervical range of motion test is 9.6° for flexion, 7° for extension, 9.1° for left lateral flexion, 5.9° for right lateral flexion, 6.7° for left rotation, and 7.6° for right rotation [21].
- Cervicocephalic relocation test: The cervicocephalic relocation test was used to examine cervical joint position sense [22]. Participants were blindfolded and wore a laser pointer on their heads. Participants memorized the neutral head position, performed maximal cervical movements (flexion, extension, left rotation, and right rotation), and then relocated the head to the reference position. The cervical joint reposition error was measured as the distance between the final position of the light beam of the laser pointer and the initial reference position. The MDC for the cervicocephalic relocation test is 0.8–1.0 cm for cervical flexion, 0.8–0.9 cm for cervical extension, 0.6–0.8 cm for left rotation, and 0.6–1.0 cm for right rotation [23].
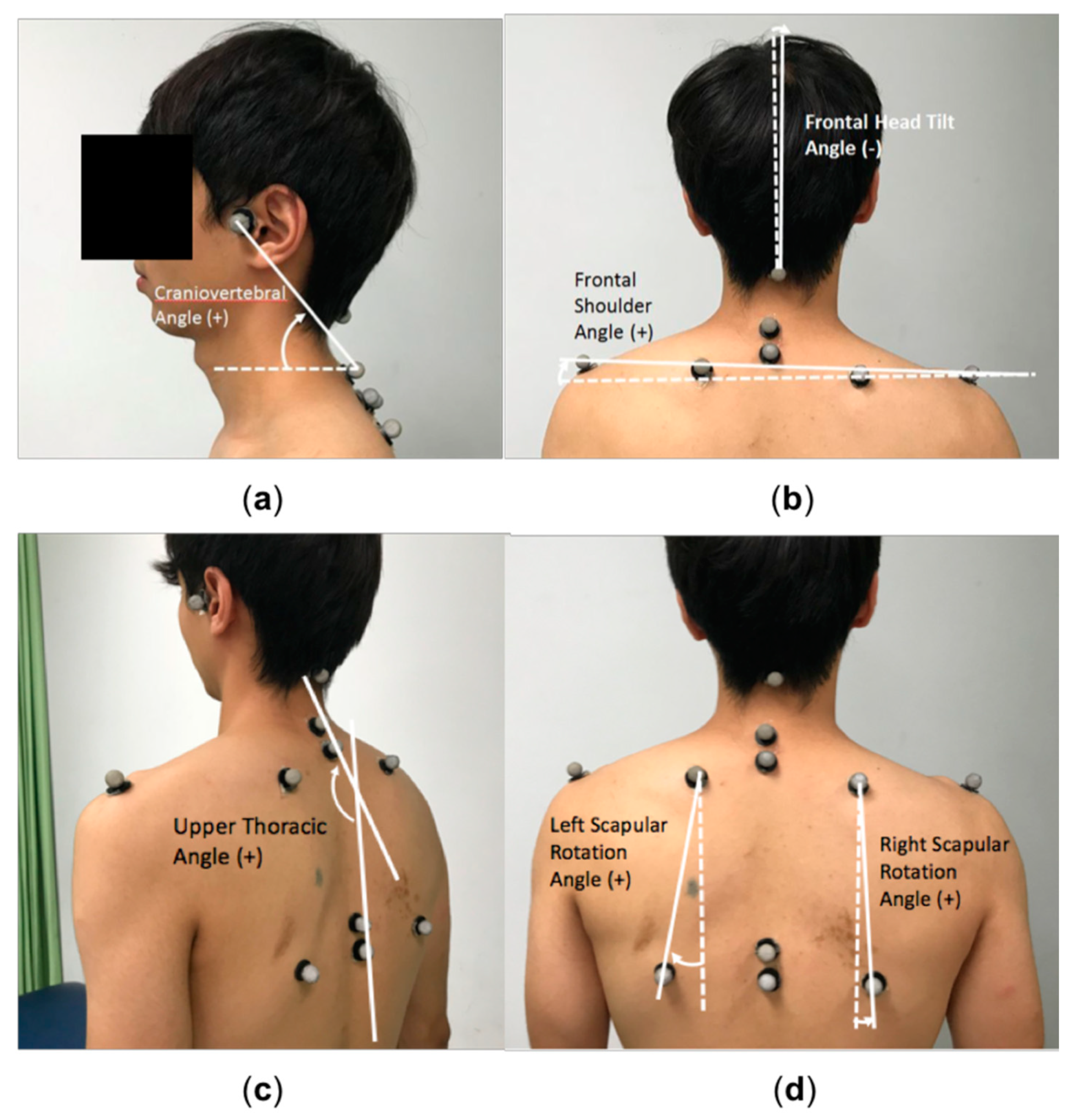
- Upper body posture: Upper body posture was measured using the photographic method [24,25]. A digital camera (Canon 450D) was set on a tripod, positioned 2.5 m from the participant and 1 m above the ground. Before photography, the researcher placed reflective markers on anatomic landmarks (Figure 1). One back- and 2 lateral-view photographs of the habitual standing posture were taken and analyzed using ImageJ software (National Institutes of Health, Bethesda, MD). Five postural angles were analyzed: frontal head tilt angle, frontal shoulder angle, right and left scapular rotation angles, craniovertebral angle, and upper thoracic angle (Figure 1).
2.4. Interventions
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lima, R.C.; Pinheiro, T.M.; Dias, E.C.; de Andrade, E.Q. Development, and prevention of work related Disord. In a sample of brazilian violinists. Work 2015, 51, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Rensing, N.; Schemmann, H.; Zalpour, C. Musculoskeletal demands in violin and viola playing: A literature review. Medic. Probl. Perf. Art. 2018, 33, 265–274. [Google Scholar] [CrossRef]
- Overton, M.; du Plessis, H.; Sole, G. Electromyography of neck and shoulder muscles in instrumental musicians with musculoskeletal pain compared to asymptomatic controls: A systematic review and meta-analysis. Musculoskelet Sci. Pract. 2018, 36, 32–42. [Google Scholar] [CrossRef]
- Mayoux-Benhamou, M.A.; Revel, M.; Vallee, C.; Roudier, R.; Barbet, J.P.; Bargy, F. Longus colli has a postural function on cervical curvature. Surg. Radiol. Anat. 1994, 16, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.A. Deep cervical flexor muscle dysfunction in whiplash. Jour. Musc. Pain. 2000, 8, 143–154. [Google Scholar] [CrossRef]
- Falla, D.L.; Jull, G.A.; Hodges, P.W. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine 2004, 29, 2108–2114. [Google Scholar] [CrossRef]
- Jull, G.; Kristjansson, E.; Dall’Alba, P. Impairment in the cervical flexors: A comparison of whiplash and insidious onset neck pain patients. Man Ther. 2004, 9, 89–94. [Google Scholar] [CrossRef]
- Steinmetz, A.; Claus, A.; Hodges, P.W.; Jull, G.A. Neck muscle function in violinists/violists with and without neck pain. Clin. Rheumatol. 2016, 35, 1045–1051. [Google Scholar] [CrossRef]
- Kisner, C.; Colby, L.A. Therapeutic Exercise: Foundations and Techniques, 6th ed.; Davis Company: Philadelphia, PA, USA, 2013. [Google Scholar]
- Dusunceli, Y.; Ozturk, C.; Atamaz, F.; Hepguler, S.; Durmaz, B. Efficacy of neck stabilization exercises for neck pain: A randomized controlled study. J. Rehabil. Med. 2009, 41, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, C.; Dziedzic, K.; Waterfield, J.; Sim, J. Effectiveness of specific neck stabilization exercises or a general neck exercise program for chronic neck disorders: A randomized controlled trial. J. Rheumatol. 2009, 36, 390–397. [Google Scholar] [CrossRef]
- Kaka, B.; Ogwumike, O.O.; Ogunlade, S.O.; Adeniyi, A.F. Effect of neck stabilization and dynamic exercises on pain, disability, and fear avoidance beliefs in patients with non-specific neck pain. Arch. Physiother. Glob. Res. 2015, 19, 17–29. [Google Scholar] [CrossRef]
- Ghaderi, F.; Jafarabadi, M.A.; Javanshir, K. The clinical and EMG assessment of the effects of stabilization exercise on nonspecific chronic neck pain: A randomized controlled trial. J. Back Musculoskelet Rehabil. 2017, 30, 211–219. [Google Scholar] [CrossRef]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G.; Rodgers, M.; Romani, W. Muscles, Testing and Function, 5th ed.; Wolters Kluwer Health: Baltimore, MD, USA, 2014. [Google Scholar]
- Misailidou, V.; Malliou, P.; Beneka, A.; Karagiannidis, A.; Godolias, G. Assessment of patients with neck pain: A review of definitions, selection criteria, and measurement tools. J. Chiropr. Med. 2010, 9, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleland, J.A.; Childs, J.D.; Whitman, J.M. Psychometric properties of the neck disability index and numeric pain rating scale in patients with mechanical neck pain. Arch. Phys. Med. Rehabil. 2008, 89, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using g*power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Jull, G.A.; O’Leary, S.P.; Falla, D.L. Clinical assessment of the deep cervical flexor muscles: The craniocervical flexion test. J. Manipulative Physiol. Ther. 2008, 31, 525–533. [Google Scholar] [CrossRef]
- Jorgensen, R.; Ris, I.; Juhl, C.; Falla, D.; Juul-Kristensen, B. Responsiveness of clinical tests for people with neck pain. BMC Musculoskelet Disord. 2017, 18, 548. [Google Scholar] [CrossRef]
- Edmondston, S.J.; Wallumrod, M.E.; Macleid, F.; Kvamme, L.S.; Joebges, S.; Brabham, G.C. Reliability of isometric muscle endurance tests in subjects with postural neck pain. J. Manipulative Physiol. Ther. 2008, 31, 348–354. [Google Scholar] [CrossRef]
- Fletcher, J.P.; Bandy, W.D. Intrarater reliability of crom measurement of cervical spine active range of motion in persons with and without neck pain. J. Orthop. Sports Phys. Ther. 2008, 38, 640–650. [Google Scholar] [CrossRef]
- Pinsault, N.; Fleury, A.; Virone, G.; Bouvier, B.; Vaillant, J.; Vuillerme, N. Test-retest reliability of cervicocephalic relocation test to neutral head position. Physiother. Theory Pract. 2008, 24, 380–391. [Google Scholar] [CrossRef]
- Jorgensen, R.; Ris, I.; Falla, D.; Juul-Kristensen, B. Reliability, construct and discriminative validity of clinical testing in subjects with and without chronic neck pain. BMC Musculoskelet Disord. 2014, 15, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Ferreira, A.; Fernandes, J.; Kuo, Y.L.; Bernardo, L.M.; Fernandes, O.; Laranjo, L.; Silva, A. Does pilates-based exercise improve postural alignment in adult women? Women Health 2013, 53, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.H.; Chiu, T.T.; Poon, A.T. The relationship between head posture and severity and disability of patients with neck pain. Man Ther. 2008, 13, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using Ibm Spss Statistics; SAGE: London, UK, 2013. [Google Scholar]
- Kim, H.-Y. Statistical notes for clinical researchers: Effect size. Rest. Dent. Endod. 2015, 40, 328–331. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Hodges, P.; Vicenzino, B. An endurance-strength training regime is effective in reducing myoelectric manifestations of cervical flexor muscle fatigue in females with chronic neck pain. Clin. Neurophysiol. 2006, 117, 828–837. [Google Scholar] [CrossRef]
- Jull, G.; Trott, P.; Potter, H.; Zito, G.; Niere, K.; Shirley, D.; Emberson, J.; Marschner, I.; Richardson, C. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine 2002, 27, 1835–1843. [Google Scholar] [CrossRef]
- Kingston, G.; Williams, G.; Gray, M.; Judd, J. Does a dvd improve compliance with home exercise programs for people who have sustained a traumatic hand injury? Results of a feasibility study. Disabil. Reh. Assist. Technol. 2013, 9, 188–194. [Google Scholar] [CrossRef]
- Emmerson, K.B.; Harding, K.E.; Taylor, N.F. Providing exercise instructions using multimedia may improve adherence but not patient outcomes: A systematic review and meta-analysis. Clin. Rehabil. 2018, 33, 607–618. [Google Scholar] [CrossRef]
- Szeto, G.P.; Straker, L.; Raine, S. A field comparison of neck and shoulder postures in symptomatic and asymptomatic office workers. Appl. Ergon. 2002, 33, 75–84. [Google Scholar] [CrossRef]
- Lee, S.; Lee, Y.; Chung, Y. Effect of changes in head postures during use of laptops on muscle activity of the neck and trunk. Phys. Ther. Rehabil. Sci. 2017, 6, 33–38. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Pre-Test 1 | Pre-Test 2 | Post-Test | Baseline Period | Intervention Period | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| ICC | Δ | p | r | Δ | p | r | ||||
| Numeric rating scale (point) | 4 (0) | 4 (1) | 0 (2) | 0.953 | 0 | 0.08 | −0.39 1 | 4 | < 0.01 | −0.89 1 |
| Neck disability index (%) | 8 (6) | 8 (7.5) | 4 (6) | 0.958 | 0 | 0.32 | −0.22 1 | 4 | < 0.01 | −0.88 1 |
| Craniocervical flexion test (mmHg) | 20 (2) | 20 (2) | 24 (4) | 0.674 | 0 | > 0.99 | 0 1 | −4 | < 0.01 | −0.77 1 |
| Cervical muscles endurance (sec) | ||||||||||
| Flexors | 9.2 ± 3.4 | 9.1 ± 3.0 | 14.5 ± 4.8 | 0.919 | 0.1 | 0.80 | 0.06 | −5.4 | < 0.01 | 0.83 |
| Extensors | 72.0 ± 63.6 | 76.9 ± 58.6 | 155.2 ± 75.3 | 0.979 | −4.9 | 0.22 | 0.28 | −78.3 | < 0.01 | 0.70 |
| Cervical range of motion (degree) | ||||||||||
| Flexion | 42.7 ± 15.9 | 44.0 ± 14.8 | 48.4 ± 12.0 | 0.777 | −1.4 | 0.65 | 0.10 | −4.4 | 0.08 | 0.40 |
| Extension | 52.7 ± 12.0 | 50.7 ± 17.3 | 59.6 ± 14.3 | 0.822 | 1.9 | 0.47 | 0.17 | −8.9 | 0.01 | 0.57 |
| Left SB | 36.0 ± 9.8 | 34.1 ± 8.8 | 40.2 ± 8.6 | 0.874 | 1.9 | 0.18 | 0.31 | −6.1 | < 0.01 | 0.72 |
| Right SB | 36.5 ± 8.1 | 34.8 ± 10.7 | 40.2 ± 9.6 | 0.887 | 1.7 | 0.22 | 0.28 | −5.4 | < 0.01 | 0.60 |
| Left rotation | 57.1 ± 10.0 | 54.1 ± 12.5 | 66.9 ± 10.7 | 0.705 | 3.0 | 0.23 | 0.27 | −12.8 | < 0.01 | 0.77 |
| Right rotation | 56.5 ± 14.5 | 55.1 ± 12.4 | 65.8 ± 14.0 | 0.853 | 1.4 | 0.55 | 0.14 | −10.6 | < 0.01 | 0.71 |
| Cervical joint position sense (cm) | ||||||||||
| Flexion | 6.3 ± 2.3 | 6.7 ± 3.1 | 4.1 ± 1.8 | 0.818 | −0.5 | 0.35 | 0.22 | 2.6 | < 0.01 | 0.61 |
| Extension | 5.7 ± 2.7 | 5.8 ± 3.7 | 4.6 ± 1.6 | 0.873 | −0.1 | 0.84 | 0.05 | 1.3 | 0.09 | 0.38 |
| Left rotation | 5.3 ± 1.9 | 6.1 ± 2.7 | 4.5 ± 2.1 | 0.381 | −0.8 | 0.22 | 0.28 | 1.6 | < 0.01 | 0.57 |
| Right rotation | 8.0 ± 3.3 | 7.4 ± 3.3 | 5.7 ± 3.0 | 0.842 | 0.6 | 0.26 | 0.26 | 1.6 | 0.05 | 0.43 |
| Upper body posture (degree) | ||||||||||
| Frontal head tilt angle 2 | −1.2 ± 8.1 | −1.2 ± 8.1 | −0.6 ± 2.5 | 1.000 | 0.002 | 0.52 | 0.15 | −0.6 | 0.72 | 0.08 |
| Frontal shoulder angle | 0.4 ± 1.7 | 0.4 ± 1.7 | 0.02 ± 1.3 | 1.000 | −0.006 | 0.02 | 0.51 | 0.3 | 0.11 | 0.36 |
| Scapular rotation angle 3 (right) | 2.1 ± 9.5 | 2.1 ± 9.6 | −0.1 ± 3.9 | 1.000 | −0.003 | 0.61 | 0.12 | 2.2 | 0.18 | 0.31 |
| Scapular rotation angle 3 (left) | 3.7 ± 8.7 | 3.7 ± 8.7 | 0.3 ± 3.5 | 1.000 | 0.004 | 0.31 | 0.23 | 3.4 | 0.06 | 0.42 |
| Craniovertebral angle | 51.4 ± 5.4 | 51.4 ± 5.4 | 53.2 ± 5.0 | 1.000 | 0.002 | 0.76 | 0.07 | −1.8 | < 0.01 | 0.64 |
| Upper thoracic angle | 149.9 ± 13.4 | 149.5 ± 13.4 | 149.6 ± 10.1 | 1.000 | −0.04 | 0.37 | 0.21 | −0.08 | 0.96 | 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-L.; Lee, T.-H.; Tsai, Y.-J. Evaluation of a Cervical Stabilization Exercise Program for Pain, Disability, and Physical Impairments in University Violinists with Nonspecific Neck Pain. Int. J. Environ. Res. Public Health 2020, 17, 5430. https://doi.org/10.3390/ijerph17155430
Kuo Y-L, Lee T-H, Tsai Y-J. Evaluation of a Cervical Stabilization Exercise Program for Pain, Disability, and Physical Impairments in University Violinists with Nonspecific Neck Pain. International Journal of Environmental Research and Public Health. 2020; 17(15):5430. https://doi.org/10.3390/ijerph17155430
Chicago/Turabian StyleKuo, Yi-Liang, Tsung-Han Lee, and Yi-Ju Tsai. 2020. "Evaluation of a Cervical Stabilization Exercise Program for Pain, Disability, and Physical Impairments in University Violinists with Nonspecific Neck Pain" International Journal of Environmental Research and Public Health 17, no. 15: 5430. https://doi.org/10.3390/ijerph17155430