Self-Control Moderates the Association Between Perceived Severity of Coronavirus Disease 2019 (COVID-19) and Mental Health Problems Among the Chinese Public


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Mean Levels of and the Bivariate Correlations Between Mental Health Problems, Perceived Severity, and Self-Control
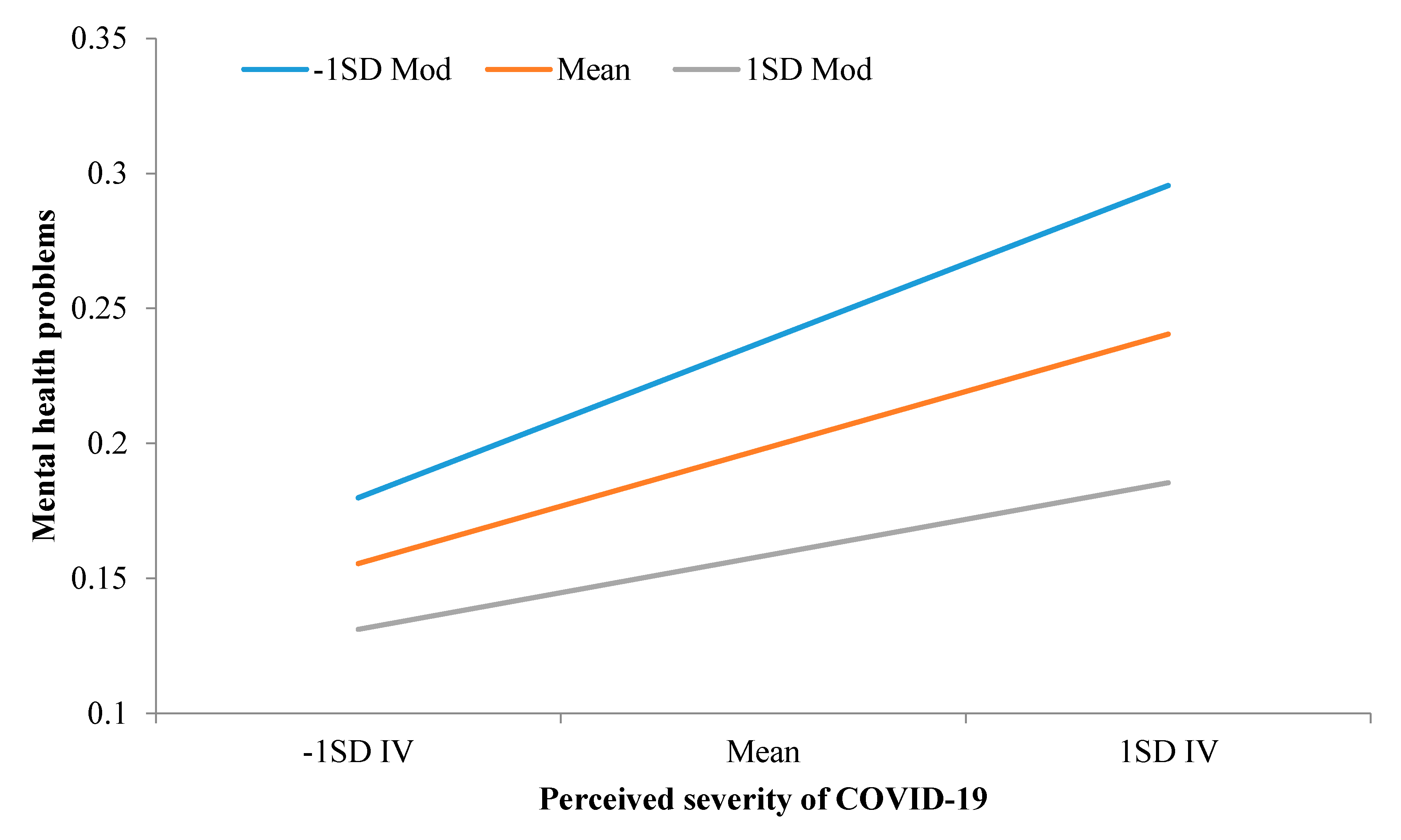
3.2. The Moderation of Self-Control in the Association Between Perceived Severity and Mental Health Problems
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Li, J.-B.; Yang, A.; Dou, K.; Wang, L.-X.; Zhang, M.-C.; Lin, X.-Q. Chinese public’s knowledge, perceived severity, and perceived controllability of the COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. 2020. (Manuscript under review). [Google Scholar]
- Masten, A.S. Ordinary magic. Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef]
- Tangney, J.P.; Baumeister, R.F.; Boone, A.L. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J. Personal. 2004, 72, 271–324. [Google Scholar] [CrossRef]
- Cheng, S.K.W.; Chong, G.H.C.; Chang, S.S.Y.; Wong, C.W.; Wong, C.S.Y.; Wong, M.T.P.; Wong, K.C. Adjustment to severe acute respiratory syndrome (SARS): Roles of appraisal and post-traumatic growth. Psychol. Health 2006, 21, 301–317. [Google Scholar] [CrossRef]
- Dorfan, N.M.; Woody, S.R. Danger appraisals as prospective predictors of disgust and avoidance of contaminants. J. Soc. Clin. Psychol. 2011, 30, 105–132. [Google Scholar] [CrossRef]
- Vartti, A.M.; Oenema, A.; Schreck, M.; Uutela, A.; de Zwart, O.; Brug, J.; Aro, A.R. SARS Knowledge, Perceptions, and Behaviors: A Comparison between Finns and the Dutch during the SARS Outbreak in 2003. Int. J. Behav. Med. 2009, 16, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.Z.; Chu, H.R. Who is afraid of the Ebola outbreak? The influence of discrete emotions on risk perception. J. Risk Res. 2018, 21, 834–853. [Google Scholar] [CrossRef]
- de Ridder, D.T.D.; de Boer, B.J.; Lugtig, P.; Bakker, A.B.; van Hooft, E.A.J. Not doing bad things is not equivalent to doing the right thing: Distinguishing between inhibitory and initiatory self-control. Personal. Individ. Differ. 2011, 50, 1006–1011. [Google Scholar] [CrossRef]
- Li, J.-B.; Delvecchio, E.; Lis, A.; Nie, Y.-G.; Di Riso, D. Positive coping as mediator between self-control and life satisfaction: Evidence from two Chinese samples. Personal. Individ. Differ. 2016, 97, 130–133. [Google Scholar] [CrossRef]
- Duckworth, A.L.; Seligman, M.E.P. Self-discipline outdoes IQ in predicting academic performance of adolescents. Psychol. Sci. 2005, 16, 939–944. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Houts, R.; Poulton, R.; Roberts, B.W.; Ross, S.; et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. USA 2011, 108, 2693–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, W.; Friese, M.; Strack, F. Impulse and self-control from a dual-systems perspective. Perspect. Psychol. Sci. 2009, 4, 162–176. [Google Scholar] [CrossRef] [PubMed]
- de Ridder, D.T.D.; Lensvelt-Mulders, G.; Finkenauer, C.; Stok, F.M.; Baumeister, R.F. Taking stock of self-control: A meta-analysis of how trait self-control relates to a wide range of behaviors. Personal. Soc. Psychol. Rev. 2012, 16, 76–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wills, T.A.; Ainette, M.G.; Stoolmiller, M.; Gibbons, F.X.; Shinar, O. Good Self-Control as a Buffering Agent for Adolescent Substance Use: An Investigation in Early Adolescence With Time-Varying Covariates. Psychol. Addict. Behav. 2008, 22, 459–471. [Google Scholar] [CrossRef] [Green Version]
- Dishion, T.J.; Connell, A. Adolescents‘ resilience as a self-regulatory process: Promising themes for linking intervention with developmental science. Ann. N. Y. Acad. Sci. 2006, 1094, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, J. The introduction of the Common Mental Health Screening Scales and the comparison of their reliablity and validity. Chin. J. Soc. Med. 2014, 31, 86–88. [Google Scholar]
- Li, J.-B.; Vazsonyi, A.T.; Dou, K. Is individualism-collectivism associated with self-control? Evidence from Chinese and U.S. samples. PLoS ONE 2018, 13, e0208541. [Google Scholar] [CrossRef]
- Enders, C.K.; Tofighi, D. Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychol. Methods 2007, 12, 121–138. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- American, S. WHO Declares Coronavirus Outbreak a Global Health Emergency. Available online: https://www.scientificamerican.com/article/who-declares-coronavirus-outbreak-a-global-health-emergency/ (accessed on 1 March 2020).
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.R.; Faria, S.; Lopes, H. Stress and Psychological Health: Testing the Mediating Role of Cognitive Appraisal. West. J. Nurs. Res. 2016, 38, 1448–1468. [Google Scholar] [CrossRef] [Green Version]
- Germani, A.; Buratta, L.; Delvecchio, E.; Mazzeschi, C. Emerging Adults and COVID-19: The Role of Individualism-Collectivism on Perceived Risks and Psychological Maladjustment. Int. J. Environ. Res. Public Health 2020, 17, 3497. [Google Scholar] [CrossRef]
- Barkur, G.; Vibha; Kamath, G.B. Sentiment analysis of nationwide lockdown due to COVID 19 outbreak: Evidence from India. Asian J. Psychiatry 2020, 51, 102089. [Google Scholar] [CrossRef]
- Willems, Y.E.; Boesen, N.; Li, J.; Finkenauer, C.; Bartels, M. The heritability of self-control: A meta-analysis. Neurosci. Biobehav. Rev. 2019, 100, 324–334. [Google Scholar] [CrossRef]
- Hay, C.; Meldrum, R. Self-control and Crime over the Life Course; Sage Publications: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Tang, Y.-Y.; Ma, Y.; Wang, J.; Fan, Y.; Feng, S.; Lu, Q.; Yu, Q.; Sui, D.; Rothbart, M.K.; Fan, M.; et al. Short-term meditation training improves attention and self-regulation. Proc. Natl. Acad. Sci. USA 2007, 104, 17152–17156. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Zhao, J.; Chen, Y.; Zu, S.; Zhao, J. Comprehensive self-control training benefits depressed college students: A six-month randomized controlled intervention trial. J. Affect. Disord. 2018, 226, 251–260. [Google Scholar] [CrossRef]
- Forum, W.E. The COVID-19 Pandemic Could Last for 2 Years, According to US Experts. Available online: https://www.weforum.org/agenda/2020/05/coronavirus-pandemic-last-2-years/ (accessed on 6 May 2020).
- Greenfield, P.M. Linking social change and developmental change: Shifting pathways of human development. Dev. Psychol. 2009, 45, 401–418. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Sex | ||||||||||
| 2. Age | −0.08 *** | |||||||||
| 3. Phy. history | 0.06 *** | −0.10 *** | ||||||||
| 4. Psy. history | −0.01 | 0.01 | 0.08 *** | |||||||
| 5. Health con. | −0.04 ** | −0.03 | 0.18 *** | 0.08 *** | ||||||
| 6. Education | −0.00 | −0.13 ** | −0.03 * | 0.03 * | 0.02 | |||||
| 7. Rel. w. COVID-19 | 0.01 | 0.09 ** | −0.02 | −0.03 * | −0.03 * | −0.01 | ||||
| 8. Mental health problems | 0.07 *** | 0.04 * | −0.08 *** | −0.09 *** | −0.19 *** | 0.02 | 0.03 * | |||
| 9. Perceived severity | 0.11 *** | 0.09 *** | 0.00 | −0.00 | −0.04 ** | −0.03 * | −0.00 | 0.19 *** | ||
| 10. Self-control | −0.01 | 0.21 *** | 0.05 ** | 0.06 *** | 0.21 *** | −0.06 *** | 0.03 | −0.21 *** | −0.10 *** | |
| Cronbach’s α | - | - | - | - | - | - | - | 0.86 | 0.84 | 0.84 |
| Min. | 1.00 | 17 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 0.00 | 1.00 | 1.31 |
| Max. | 2.00 | 90 | 2.00 | 2.00 | 5.00 | 6.00 | 2.00 | 2.00 | 5.00 | 5.00 |
| M | - | 23.71 | - | - | - | - | - | 0.19 | 4.09 | 3.03 |
| SD | - | 7.29 | - | - | - | - | - | 0.27 | 0.59 | 0.50 |
| Predictors | B | SE | p |
|---|---|---|---|
| Sex | 0.04 | 0.01 | <0.001 |
| Age | 0.00 | 0.00 | 0.048 |
| Phy. history | −0.04 | 0.02 | 0.025 |
| Psy. history | −0.17 | 0.07 | 0.013 |
| Health con. | −0.04 | 0.01 | <0.001 |
| Education | 0.01 | 0.01 | 0.062 |
| Rel. w. COVID-19 | 0.08 | 0.03 | 0.013 |
| Perceived severity | 0.07 | 0.01 | <0.001 |
| Self-control | −0.08 | 0.01 | <0.001 |
| Perceived severity × self-control | −0.05 | 0.01 | <0.001 |
| Simple Slope Tests and Comparison | B | SE | p | 95% Bootstrapping CI (N = 20,000) b |
|---|---|---|---|---|
| Simple slopes | ||||
| Low self-control (−1SD) | 0.10 | 0.01 | <0.001 | [0.080, 0.116] |
| Medium self-control (mean) a | 0.07 | 0.01 | <0.001 | [0.058, 0.086] |
| High self-control (1SD) | 0.05 | 0.01 | <0.001 | [0.028, 0.064] |
| Comparison between simple slopes | ||||
| Difference between low and medium self-control | 0.03 | 0.01 | <0.001 | [0.015, 0.037] |
| Difference between low and high self-control | 0.05 | 0.01 | <0.001 | [0.029, 0.075] |
| Difference between medium and high self-control | 0.04 | 0.01 | <0.001 | [0.015, 0.037] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.-B.; Yang, A.; Dou, K.; Cheung, R.Y.M. Self-Control Moderates the Association Between Perceived Severity of Coronavirus Disease 2019 (COVID-19) and Mental Health Problems Among the Chinese Public. Int. J. Environ. Res. Public Health 2020, 17, 4820. https://doi.org/10.3390/ijerph17134820
Li J-B, Yang A, Dou K, Cheung RYM. Self-Control Moderates the Association Between Perceived Severity of Coronavirus Disease 2019 (COVID-19) and Mental Health Problems Among the Chinese Public. International Journal of Environmental Research and Public Health. 2020; 17(13):4820. https://doi.org/10.3390/ijerph17134820
Chicago/Turabian StyleLi, Jian-Bin, An Yang, Kai Dou, and Rebecca Y. M. Cheung. 2020. "Self-Control Moderates the Association Between Perceived Severity of Coronavirus Disease 2019 (COVID-19) and Mental Health Problems Among the Chinese Public" International Journal of Environmental Research and Public Health 17, no. 13: 4820. https://doi.org/10.3390/ijerph17134820