Social-Ecological Correlates of Regular Leisure-Time Physical Activity Practice among Adults

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
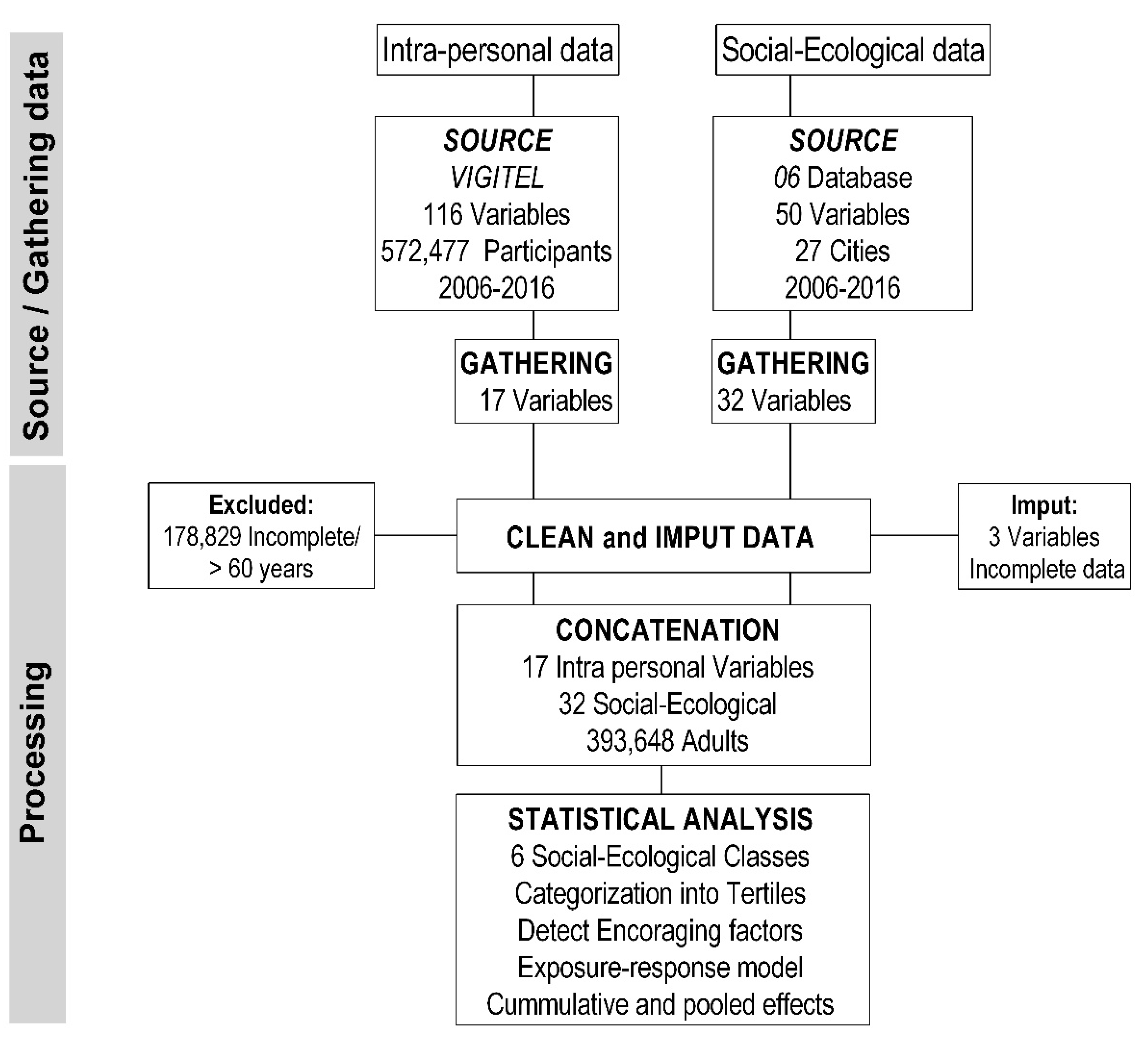
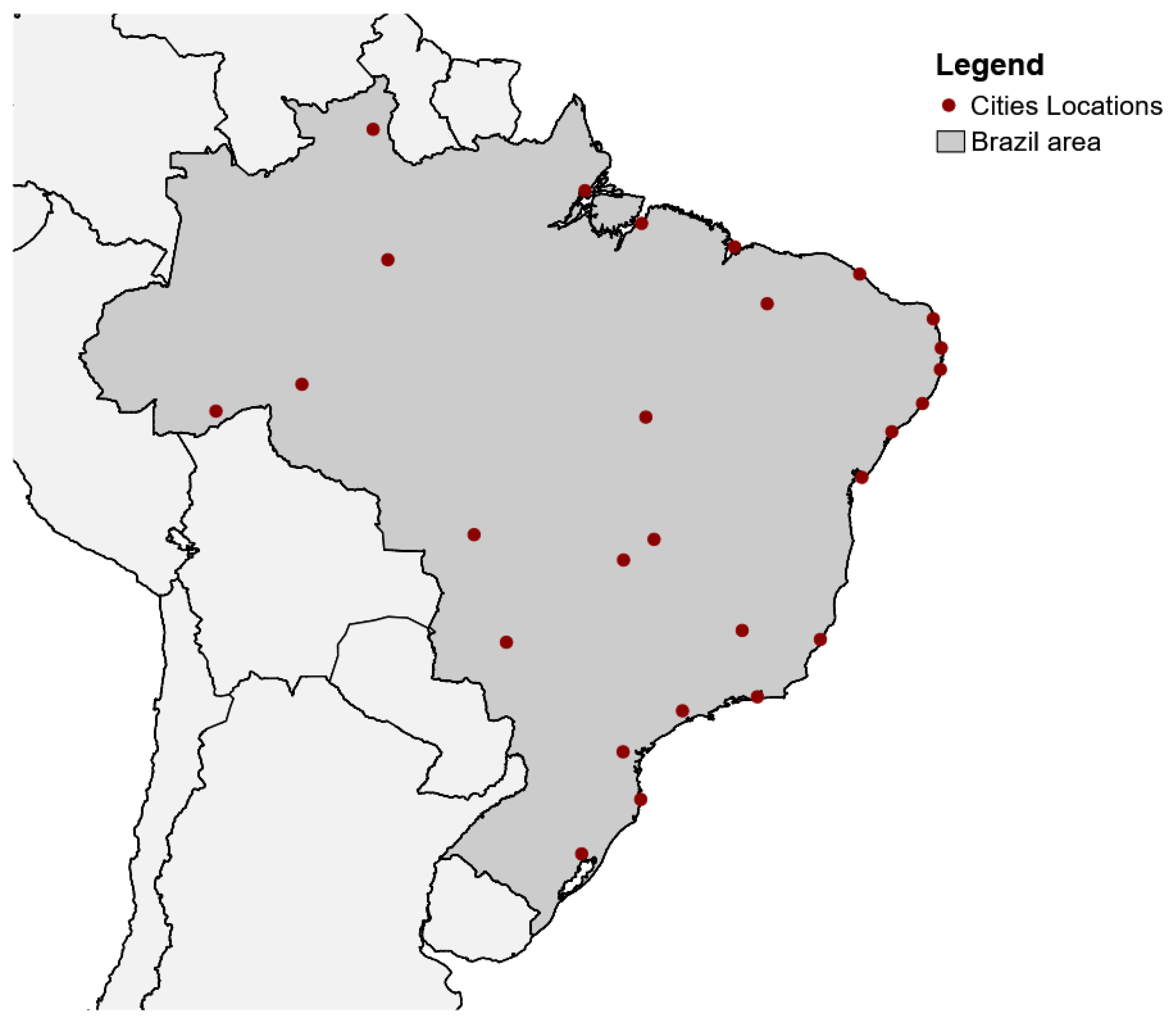
2.1. Design and Sample
2.2. Data Source, Gathering, and Procedures
2.3. Intra-Personal Data
- Demographics = age, marital status, and sex;
- Health = alcohol abuse, self-related heath, diabetes (medical diagnosis), hypertension (medical diagnosis), obesity (BMI > 30 m/kg2); TV time > 3 h/day; and current use of tobacco;
- Nutrition = regular consumption (≥5 days) in the previous seven days of fruits, meat, milk, soda, and vegetables; and consumption of the fat cap and skin when eating meat and chicken, respectively.
2.4. Social-Ecological Data
- Social = crime mortality (1/100,000 inhabitants), number of employees of physical activity-related companies (inhab. rate), family income < 1/2 min wage (%), family income from 1/2 to 1 min wage (%), family income from 1 to 2 min wage (%), family income > 2 min wages (%), percentage of women (%), life expectancy for men, women and in general (years), population (millions), and traffic accident mortality (1/100,000 inhabitants);
- Political = basic grocery cost (cost of basic food items to feed a family of 4 for 1 month in BR$), availability of clean drinking water (%), family health care teams/primary care teams (n), GDP/capita (BR$), public primary care coverage (%), income inequalities—GINI index (ua), public investment in sports and leisure per capita (BR$), public investment in health care per capita (BR$), and private health insurance (1/100,000 inhabitants).
- Environment and Transport = bus fleet/100,000 inhabitants, car fleet/100,000 inhabitants, PA companies (e.g., sports and recreational clubs, gyms) (inhabitants’ rate), and vehicle fleet/100,000 inhabitants (all type);
- Climate = hours of sun/year, max temperature (°C), min temperature (°C), average humidity (%), max humidity (%), min humidity (%), and precipitation/year (mm3).
2.5. Concatenation and Analysis
2.6. Descriptive Analysis
2.7. Exposure-Response Model
2.8. Generalized and Pooled Effects
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pedersen, B.K.; Saltin, B. Exercise as medicine-evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashdown-Franks, G.; Firth, J.; Carney, R.; Carvalho, A.F.; Hallgren, M.; Koyanagi, A.; Rosenbaum, S.; Schuch, F.B.; Smith, L.; Solmi, M.; et al. Exercise as medicine for mental and substance use disorders: A meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med. 2019, 50, 151–170. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Shilton, T.; Westerman, L.; Varney, J.; Bull, F. World Health Organisation to develop global action plan to promote physical activity: Time for action. Br. J. Sports Med. 2018, 52, 484–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet. 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Lakerveld, J.; van der Ploeg, H.P.; Kroeze, W.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; Donnelly, A.E.; et al. Towards the integration and development of a cross-European research network and infrastructure: The DEterminants of DIet and Physical ACtivity (DEDIPAC) knowledge hub. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 143. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; De Bourdeaudhuij, I.; et al. Determinants of diet and physical activity (DEDIPAC): A summary of findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- Carlin, A.; Perchoux, C.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Coppinger, T. A life course examination of the physical environmental determinants of physical activity behavior: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182083. [Google Scholar] [CrossRef] [PubMed]
- Kärmeniemi, M.; Lankila, T.; Ikäheimo, T.M.; Koivumaa-Honkanen, H.; Korpelainen, R. The built environment as a determinant of physical activity: A systematic review of longitudinal studies and natural experiments. Ann. Behav. Med. 2018, 52, 239–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, R.E.; Saelens, B.E.; Sauvage-Mar, C. Understanding physical activity through interactions between the built environment and social cognition: A systematic review. Sports Med. 2018, 48, 1893–1912. [Google Scholar] [CrossRef] [PubMed]
- Rees-Punia, E.; Hathaway, E.D.; Gay, J.L. Crime, perceived safety, and physical activity: A meta-analysis. Prev. Med. 2018, 111, 307–313. [Google Scholar] [CrossRef]
- Cortis, C.; Puggina, A.; Pesce, C.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; et al. Psychological determinants of physical activity across the life course: A “DEterminants of DIet and Physical Activity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182709. [Google Scholar] [CrossRef]
- Condello, G.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Cortis, C. Behavioral determinants of physical activity across the life course: A “Determinants of Diet and physical Activity” (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 58–78. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Chan, K.H.K.; Huang, Y.-T.; Luo, X.; Liang, L.; Wilson, J.; Correa, A.; Levy, D.; Liu, S. Genetic determinants for leisure-time physical activity. Med. Sci. Sports Exerc. 2018, 50, 1620–1628. [Google Scholar] [CrossRef]
- Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Condello, G.; Coppinger, T.; et al. Policy determinants of physical activity across the life course: A ‘DEDIPAC’ umbrella systematic literature review. Eur. J. Public Health 2017, 28, 105–118. [Google Scholar] [CrossRef] [Green Version]
- Zenko, Z.; Ekkekakis, P.; Kavetsos, G. Changing minds: Bounded rationality and heuristic processes in exercise-related judgments and choices. Sport, Exerc. Perform. Psychol. 2016, 5, 337–351. [Google Scholar] [CrossRef]
- Evans, J.S.B.T. Dual-processing accounts of reasoning, judgment, and social cognition. Annu. Rev. Psychol. 2008, 59, 255–278. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, H.; Thomas, D. Principles of study design in environmental epidemiology. Environ. Health Perspect. 1993, 101, 23–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malta, D.C.; Da Silva, J.B. Policies to promote physical activity in Brazil. Lancet 2012, 380, 195–196. [Google Scholar] [CrossRef]
- Wilcox, S.; King, A.C.; Castro, C.; Bortz, W. Do changes in physical activity lead to dietary changes in middle and old age? Am. J. Prev. Med. 2000, 18, 276–283. [Google Scholar] [CrossRef] [Green Version]
- James, E.L.; Freund, M.; Booth, A.; Duncan, M.J.; Johnson, N.; Short, C.E.; Wolfenden, L.; Stacey, F.G.; Kay-Lambkin, F.; Vandelanotte, C. Comparative efficacy of simultaneous versus sequential multiple health behavior change interventions among adults: A systematic review of randomised trials. Prev. Med. 2016, 89, 211–223. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Nigg, C.R.; Spring, B.; Velicer, W.F.; Prochaska, J.O. The benefits and challenges of multiple health behaviour change in research and in practice. Prev. Med. 2010, 50, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Levin, L. How may public transport influence the practice of everyday life among younger and older people and how may their practices influence public transport? Soc. Sci. 2019, 8, 96. [Google Scholar] [CrossRef] [Green Version]
- Van Dyck, D.; Cerin, E.; Conway, T.L.; De Bourdeaudhuij, I.; Owen, N.; Kerr, J.; Cardon, G.; Frank, L.D.; Saelens, B.E.; Sallis, J.F. Associations between perceived neighborhood environmental attributes and adults’ sedentary behavior: Findings from the USA, Australia and Belgium. Soc. Sci. Med. 2012, 74, 1375–1384. [Google Scholar] [CrossRef] [Green Version]
- Wallmann, B.; Bucksch, J.; Hansen, S.; Schantz, P.; Froböse, I. Sitting time in Germany: An analysis of socio-demographic and environmental correlates. BMC Public Health 2013, 13, 196. [Google Scholar] [CrossRef] [Green Version]
- Fields, R.; Kaczynski, A.T.; Bopp, M.; Fallon, E. Built environment associations with health behaviors among hispanics. J. Phys. Act. Health 2013, 10, 335–342. [Google Scholar] [CrossRef]
- Zolnik, E.J. The effects of sprawl on private-vehicle commuting distances and times. Environ. Plan. B Plan. Des. 2011, 38, 1071–1084. [Google Scholar] [CrossRef]
- Sugiyama, T.; Merom, D.; van der Ploeg, H.P.; Corpuz, G.; Bauman, A.; Owen, N. Prolonged sitting in cars: Prevalence, socio-demographic variations, and trends. Prev. Med. 2012, 55, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, C.M.; Limb, E.S.; Ram, B.; Shankar, A.; Clary, C.; Lewis, D.; Cummins, S.; Procter, D.; Cooper, A.R.; Page, A.S.; et al. The effect of moving to East Village, the former London 2012 Olympic and Paralympic Games Athletes’ Village, on physical activity and adiposity (ENABLE London): A cohort study. Lancet Public Health 2019, 4, e421–e430. [Google Scholar] [CrossRef]
- Knell, G.; Brown, H.S.; Gabriel, K.P.; Durand, C.P.; Shuval, K.; Salvo, D.; Kohl, H.W. Cost-effectiveness of improvements to the built environment intended to increase physical activity. J. Phys. Act. Health 2019, 16, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P.; Gilliland, J. The effect of season and weather on physical activity: A systematic review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef]
- Wagner, A.L.; Keusch, F.; Yan, T.; Clarke, P.J. The impact of weather on summer and winter exercise behaviors. J. Sport Health Sci. 2016, 8, 39–45. [Google Scholar] [CrossRef]
- Madden, K.M.; Allem, J.-P.; Ayers, J. The seasonal periodicity of healthy contemplations about exercise and weight loss: Ecological correlational study. JMIR Public Health Surveill. 2017, 3, e92. [Google Scholar] [CrossRef]
- Obradovich, N.; Fowler, J.H. Climate change may alter human physical activity patterns. Nat. Hum. Behav. 2017, 1, 97. [Google Scholar] [CrossRef] [Green Version]
- Badland, H.; Christian, H.; Giles-Corti, B.; Knuiman, M. Seasonality in physical activity: Should this be a concern in all settings? Health Place 2011, 17, 1084–1089. [Google Scholar] [CrossRef]
- Zhao, J.; Lorenzo, S.; An, N.; Feng, W.; Lai, L.; Cui, S. Effects of heat and different humidity levels on aerobic and anaerobic exercise performance in athletes. J. Exerc. Sci. Fit. 2013, 11, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Moyen, N.E.; Mündel, T.; Du Bois, A.M.; Ciccone, A.B.; Morton, R.H.; Judelson, D.A. Increasing humidity affects thermoregulation during low-intensity exercise in women. Aviat. Space Environ. Med. 2014, 85, 905–911. [Google Scholar] [CrossRef]
- Mekjavic, I.B.; Ciuha, U.; Grönkvist, M.; Eiken, O. The effect of low ambient relative humidity on physical performance and perceptual responses during load carriage. Front. Physiol. 2017, 8, 451. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Classes | Social-Ecological Correlate | All | Male | Female |
|---|---|---|---|---|
| Outcome | PA > 150 min/week | 21.9 (21.6; 22.3) | 25.3 (24.8; 25.9) * | 19.5 (19.1; 19.9) |
| Demographic | Age (18–32 y) | 31.2 (30.8; 31.5) | 34.7 (34.2; 35.3) * | 28.6 (28.1; 29.1) |
| Age (33–45 y) | 31.5 (31.2; 31.9) | 31.1 (30.5; 31.6) | 31.9 (31.4; 32.4) | |
| Age (46–60 y) | 37.3 (36.9; 37.7) | 34.2 (33.6; 34.8) | 39.5 (39.0; 40.0) * | |
| Marital status (Single) | 38.8 (38.5; 39.2) | 40.4 (39.8; 41.0) * | 37.7 (37.2; 38.2) | |
| Marital status (Married) | 40.1 (39.8; 40.5) | 41.8 (41.2; 42.4) * | 39.0 (38.5; 39.5) | |
| Marital status (Divorced) | 11.6 (11.3; 11.8) | 12.7 (12.3; 13.1) * | 10.8 (10.5; 11.1) | |
| Marital status (Widowed) | 2.3 (2.2; 2.4) | 0.5 (0.4; 0.6) | 3.6 (3.4; 3.8) * | |
| Marital status (Other) | 7.2 (7.0; 7.4) | 4.7 (4.4; 4.9) | 8.9 (8.7; 9.2) * | |
| Nutrition | Vegetables (yes) | 53.9 (53.5; 54.3) | 48.2 (47.6; 48.9) | 58.0 (57.5; 58.5) * |
| Fruits (yes) | 64.2 (63.8; 64.6) | 56.6 (56.0; 57.2) | 69.7 (69.2; 70.2) * | |
| Fruits and vegetables (yes) | 39.6 (39.2; 40.0) | 32.1 (31.6; 32.7) | 45.0 (44.5; 45.5) * | |
| Meat (yes) | 22.2 (21.9; 22.5) | 30.6 (30.1; 31.2) * | 16.2 (15.8; 16.5) | |
| Chicken skin (yes) | 16.3 (16.0; 16.5) | 24.3 (23.8; 24.9) * | 10.5 (10.1; 10.8) | |
| Meat fat (yes) | 30.4 (30.0; 30.8) | 41.9 (41.3; 42.5) * | 22.2 (21.8; 22.6) | |
| Milk (yes) | 53.9 (53.6; 54.3) | 57.3 (56.7; 57.9) * | 51.5 (51.0; 52.1) | |
| Soda (yes) | 16.7 (16.4; 17.0) | 20.3 (19.8; 20.8)* | 14.1 (13.8; 14.5) | |
| Health | Weight (kg) # | 70.3 (69.7; 70.3) | 77.6 (77.5; 77;8) * | 65.0 (64.5; 65.3) |
| Height (cm) # | 165.4 (164.8; 166.0) | 172.2 (171.7; 172.5) * | 160.6 (159.9; 161.1) | |
| TV > 3 h/day (yes) | 22.3 (21.9; 22.6) | 23.3 (22.8; 23.8) * | 21.6 (21.1; 22.0) | |
| Tabaco use (yes) | 8.6 (8.4; 8.9) | 11.2 (10.9; 11.6) * | 6.8 (6.5; 7.0) | |
| Obesity (yes) | 17.6 (17.3; 17.9) | 19.2 (18.7; 19.7) * | 16.4 (16.1; 16.8) | |
| Alcohol abuse (yes) | 19.4 (19.1; 19.8) | 30.1 (29.6; 30.7) * | 11.8 (11.5; 12.2) | |
| Poor self-related health (yes) | 3.8 (3.7; 4.0) | 2.7 (2.6; 3.0) | 4.6 (4.4; 4.8) * | |
| Hypertension (yes) | 20.7 (20.4; 21.0) | 19.9 (19.5; 20.4) | 21.3 (20.8; 21.7) * | |
| Diabetes (yes) | 5.4 (5.2; 5.6) | 5.2 (5.0; 5.5) | 5.5 (5.3; 5.8) |
| Classes | Social-Ecological Correlate | Mean ± SD | Min–Max |
|---|---|---|---|
| Political | Basic grocery package (BR$) | 259.1 ± 74.3 | 132.1–459.0 |
| Availability of clean drinking water (%) | 88.5 ± 12.8 | 49.2–99.3 | |
| Primary care coverage (%) | 63.2 ± 20.3 | 20.88–100 | |
| Income inequalities—Gini Index (a.u.) | 0.5 ± 0.1 | 0.42–0.60 | |
| Family health care—public health policy (n) | 234.1 ± 269.1 | 41–1531 | |
| Public investment * in sports and leisure per capita (BR$) | 10.5 ± 13.26 | 0–117.6 | |
| Public investment * in health care per capita (BR$) | 497.8 ± 227.3 | 118.2–1260.6 | |
| GDP per capita (BR$) | 25,336 ± 13,881 | 7682–79,099 | |
| Private health insurance (1/100,000 inhabit.) | 32,358 ± 14,717 | 5992–77,525 | |
| Social | Life expectancy (years) | 72. ± 2.6 | 67.3–79.1 |
| Male life Expectancy (years) | 69.39 ± 2.6 | 63.0–75.8 | |
| Female life Expectancy (years) | 76.6 ± 2.5 | 71.2–82.4 | |
| Family income < 1/2 min wage (%) | 24.1 ± 10.7 | 5.2–47.1 | |
| Family income 1 to 2 min wage (%) | 18.9 ± 7.9 | 7.9–43.9 | |
| Family income 1/2 to 1 min wage (%) | 24.1 ± 6.0 | 13.2–38.6 | |
| Family income > 2 min wage (%) | 29.3 ± 3.9 | 18–36.4 | |
| Population (millions) | 1721.0 ± 2279.0 | 0.184–12,038.0 | |
| Traffic accident mortality (1/100,000 inhabit.) | 45.3 ± 60.9 | 0.62–482.3 | |
| Crime mortality (1/100,000 inhabit.) | 105.4 ± 163.2 | 1.05–1098.0 | |
| Number of employees in PA companies (inhabit. rate) | 825.2 ± 536.2 | 194.53–2906.4 | |
| Female proportion (%) | 0.5 ± 0.01 | 0.47–0.54 | |
| Environment Transport | PA companies (inhabit. rate) | 2888 ± 1561 | 648–7796 |
| Car fleet (1/100,000 inhabit.) | 386.1 ± 144.6 | 125.3–740.7 | |
| Bus fleet (1/100,000 inhabit.) | 4.3 ± 1.42 | 1.4–7.9 | |
| Vehicle fleet (1/100,000 inhabit.) | 416.2 ± 157.3 | 135.4–806.5 | |
| Climate | Precipitation (mm3) | 1771.61 ± 591.41 | 104–3775.6 |
| Hours of sun/year (hours) | 2327 ± 392 | 475.3–3250 | |
| Max temperature (°C) | 30.2 ± 2.7 | 23.0–35.5 | |
| Min temperature (°C) | 21.3 ± 2.9 | 13.4–25.7 | |
| Average humidity (%) | 75.5 ± 6.7 | 56.2–98.0 | |
| Max humidity (%) | 82.8 ± 5.1 | 62.6–98.0 | |
| Min humidity (%) | 66.5 ± 12.6 | 31.0–98.0 |
| Social-Ecological Class | AGE 18–32 y | AGE 33–45 y | AGE 46–60 y | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | ΔPR | GRPR | GROR | OR (CI95%) | ΔPR | GRPR | GROR | OR (CI95%) | ΔPR | GRPR | GROR | OR (CI95%) | |
| Health | M | 35.1 | 15.1 | 0.40 | 1.53 (1.28–1.84) | 16.0 | 5.8 | 0.10 | 1.22 (1.06–1.41) | 9.8 | 7.8 | 0.23 | 1.39 (1.23–1.57) |
| F | 19.8 | 12.6 | 0.41 | 2.06 (1.50–2.83) | 19.9 | 8.8 | 0.50 | 1.37 (1.11–1.70) | 11.0 | 7.1 | 0.51 | 1.44 (1.22–1.71) | |
| Nutrition | M | 18.6 | 17.9 | 0.91 | 1.67 (1.25–2.24) | 13.1 | 12.7 | 0.90 | 2.01 (1.48–2.75) | 11.2 | 12.2 | 0.92 | 2.00 (1.49–2.69) |
| F | 11.8 | 10.4 | 0.69 | 1.79 (1.28–2.50) | 15.7 | 13.3 | 1.01 | 2.03 (1.56–2.66) | 13.1 | 11.5 | 0.82 | 2.05 (1.52–2.78) | |
| Social | M | 2.2 | 0.4 | 0.26 | 1.22 (1.09–1.38) | 2.9 | −1.8 | 0.27 | 1.40 (1.19–1.64) | 5.2 | −0.7 | 0.12 | 1.29 (1.09–1.51) |
| F | 1.0 | −0.8 | −0.05 | 1.18 (1.03–1.34) | 0.0 | −4.3 | 0.08 | 1.23 (1.07–1.40) | −2.7 | −2.3 | −0.02 | 0.83 (0.74–0.94) | |
| Environment Transport | M | 5.4 | 3.6 | 0.31 | 1.24 (1.09–1.40) | −2.6 | −1.6 | −0.11 | 0.99 (0.87–1.12) | −2.2 | −0.7 | 0.12 | 0.96 (0.84–1.09) |
| F | −3.7 | −3.2 | −0.25 | 0.93 (0.82–1.06) | 3.6 | 2.7 | 0.08 | 1.14 (1.02–1.28) | −1.5 | −2.1 | 0.14 | 1.15 (1.02–1.31) | |
| Political | M | 5.6 | 5.0 | 0.04 | 0.97 (0.89–1.07) | −3.5 | −4.4 | −0.20 | 0.79 (0.71–0.89) | 1.6 | 0.1 | 0.02 | 0.91 (0.81–1.02) |
| F | 5.7 | 3.8 | 0.15 | 1.14 (1.03–1.26) | 0.3 | −0.6 | −0.15 | 0.80 (0.71–0.90) | −3.3 | −2.5 | −0.20 | 0.82 (0.75–0.91) | |
| Climate | M | 7.9 | 3.1 | 0.45 | 1.33 (1.21–1.46) | 6.9 | 3.7 | 0.46 | 1.49 (1.33–1.66) | 7.9 | 4.9 | 0.50 | 1.49 (1.34–1.66) |
| F | 6.0 | 3.3 | 0.21 | 1.18 (1.07–1.31) | 1.0 | −2.3 | 0.00 | 1.22 (1.10–1.34) | 1.4 | −1.2 | 0.08 | 1.33 (1.22–1.47) | |
| Pooled Effect | M | 12.5 | 7.5 | 0.40 | 1.29 (1.27–1.37) | 5.5 | 2.4 | 0.24 | 1.27 (1.11–1.40) | 5.6 | 3.9 | 0.32 | 1.31 (1.15–1.44) |
| F | 6.8 | 4.4 | 0.19 | 1.26 (1.12–1.41) | 6.8 | 2.9 | 0.25 | 1.22 (1.07–1.39) | 3.0 | 1.8 | 0.18 | 1.16 (1.01–1.32) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavazzotto, T.G.; Ronque, E.R.V.; Vieira, E.R.; Queiroga, M.R.; Serassuelo Junior, H. Social-Ecological Correlates of Regular Leisure-Time Physical Activity Practice among Adults. Int. J. Environ. Res. Public Health 2020, 17, 3619. https://doi.org/10.3390/ijerph17103619
Cavazzotto TG, Ronque ERV, Vieira ER, Queiroga MR, Serassuelo Junior H. Social-Ecological Correlates of Regular Leisure-Time Physical Activity Practice among Adults. International Journal of Environmental Research and Public Health. 2020; 17(10):3619. https://doi.org/10.3390/ijerph17103619
Chicago/Turabian StyleCavazzotto, Timothy Gustavo, Enio Ricardo Vaz Ronque, Edgar Ramos Vieira, Marcos Roberto Queiroga, and Helio Serassuelo Junior. 2020. "Social-Ecological Correlates of Regular Leisure-Time Physical Activity Practice among Adults" International Journal of Environmental Research and Public Health 17, no. 10: 3619. https://doi.org/10.3390/ijerph17103619