Cross-Sectional Analysis of University Students’ Health Using a Digitised Health Survey

 and
and
Abstract
:1. Introduction
1.1. Student Health Screening
1.2. Singapore Healthy Campus Initiative
2. Materials and Methods
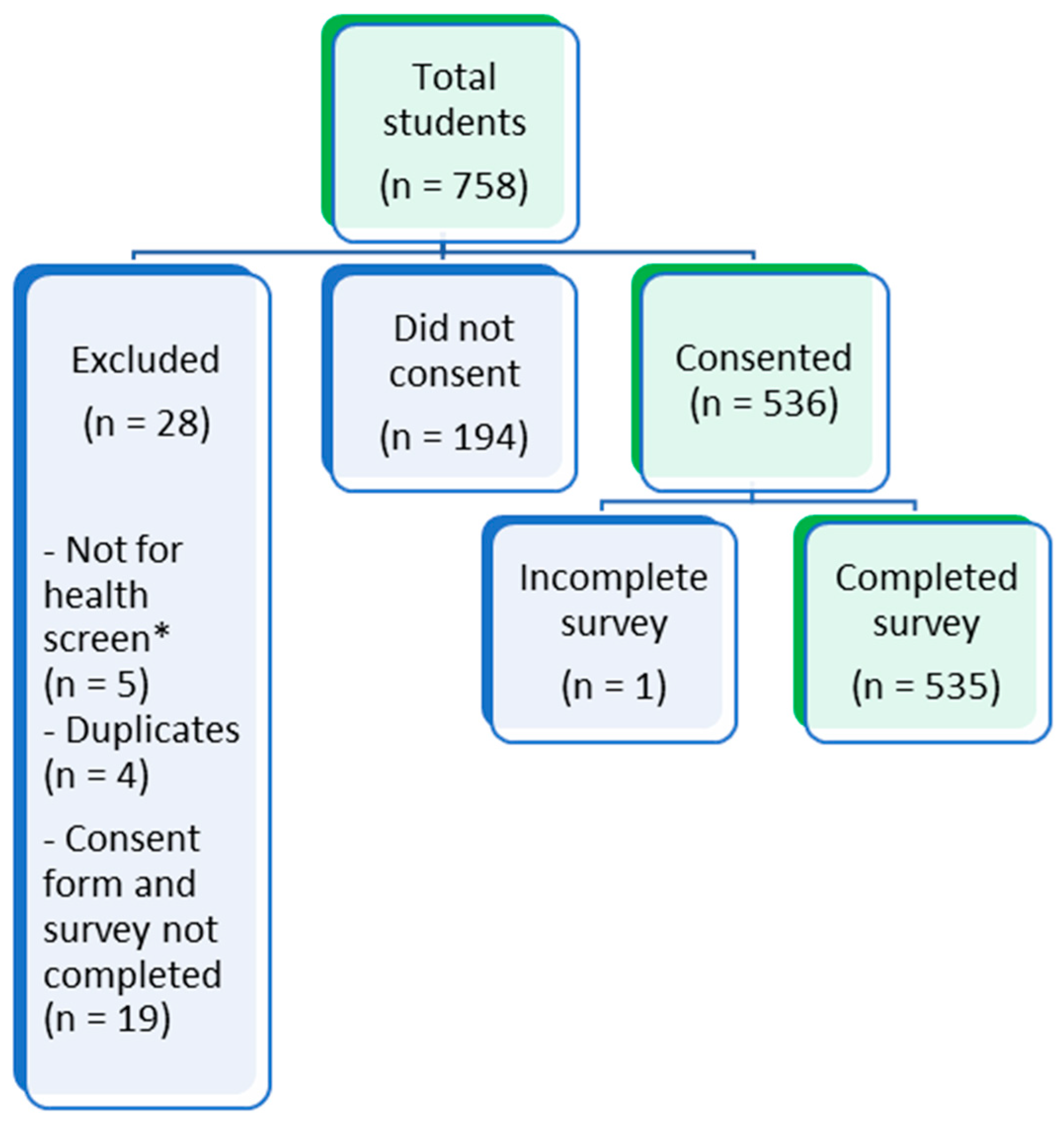
2.1. Study Population
2.2. Digital Health Survey
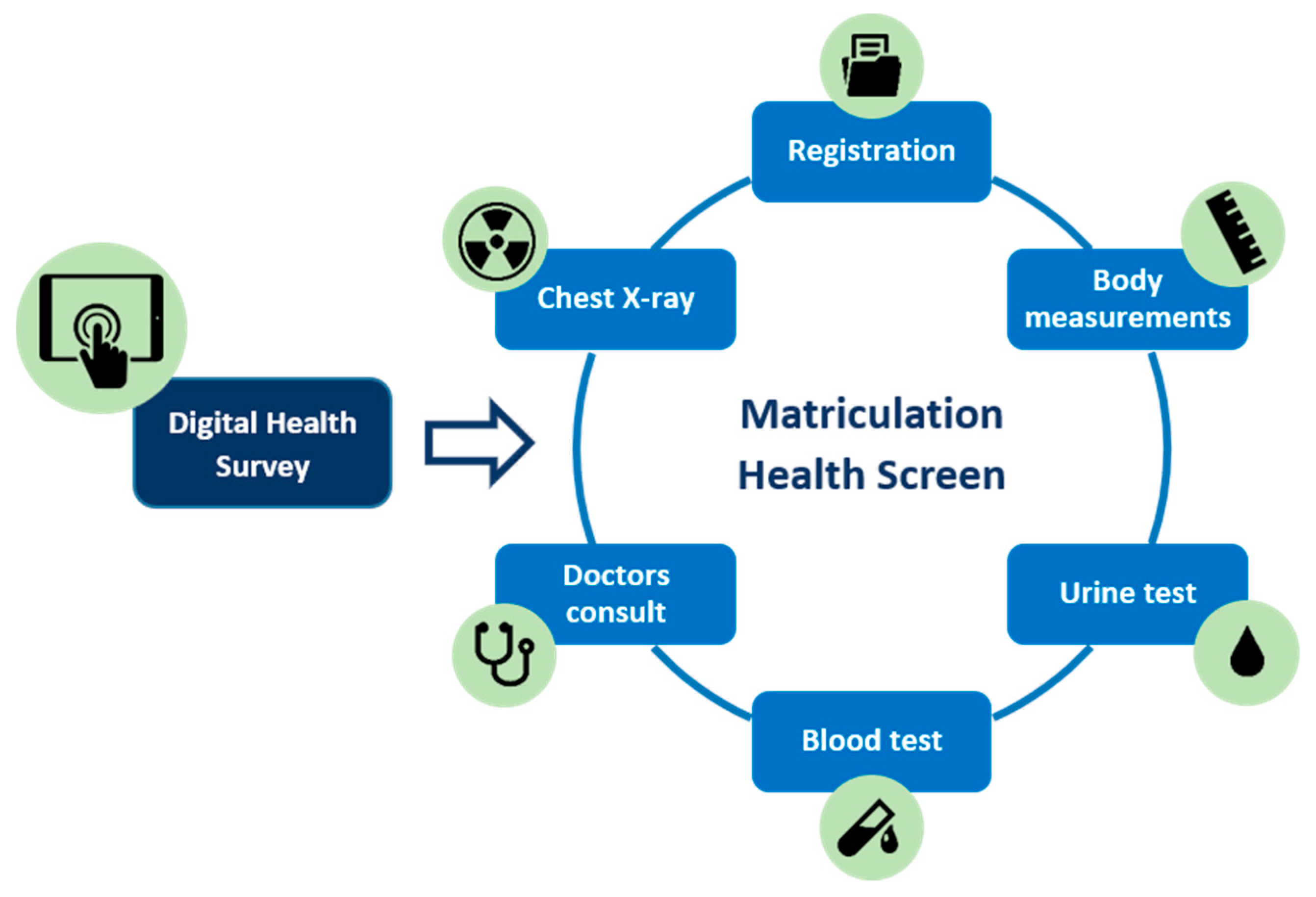
2.3. Study Procedure
- 1.
- Registration: students register at the clinic’s reception desk with their valid identification and matriculation health check forms. The staff enter the students’ details into the system and print the patient stickers. These are attached to the forms as well as a blood lab form. The forms are stamped with the date and clinic details and stapled together. A slip with the student’s queue number is printed and attached to the forms with a paper clip. This process takes 1–2 min—however, with only 1–2 staff completing this, students are required to wait during peak times.
- 2.
- Measurements: height, weight, body mass index (BMI), and visual acuity are assessed at a single station. Height and weight are assessed using an automatic standing scale, from which BMI is calculated. The eye test is done using a Rosenbaum chart (numbers chart) at 6 m distance, noting whether the participant is using corrective lenses or not. The results are hand-recorded on the student forms, and no further action is taken. There is one healthcare worker at this station, and the station takes 2–3 min to complete. Total time at the station, including waiting time, can range from between 2 (with no queue) to 10 min during busy times.
- 3.
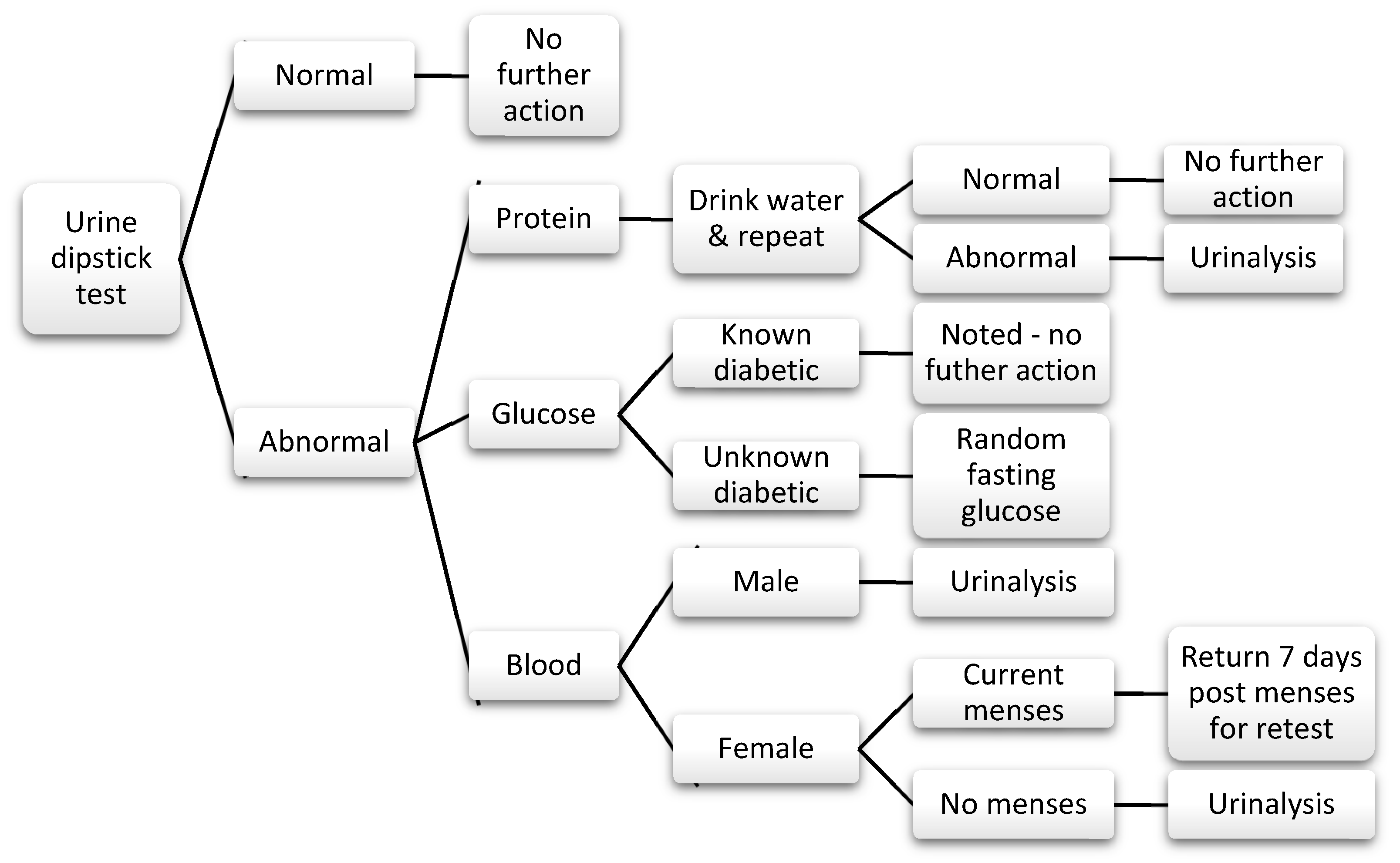
- Urine test: students are given a bag/cup with a urine dipstick, sent to the bathroom to cover the stick in urine, and asked to return to show the results to the nurse. The test is assessed by a nurse. Abnormal results, including any trace elements of glucose, blood, or protein are generally managed following a protocol (see Figure 2). There is one healthcare worker at this station. On average students, spend 10 min at this station from the time of collection of dipsticks to completion. The staff confirm students’ queue numbers or names, and manually write the results into their form. Female students who are currently having their menstrual period need to return 7 days after the end of their period to complete the urine test.
- 4.
- Blood tests: specific blood tests are required for international students and for students entering specific courses:
- Hepatitis B—medicine and biomedical science (traditional Chinese medicine), as well as international students;
- Hepatitis C—medicine;
- HIV (human immunodeficiency virus)—medicine and international students.
- 5.
- Chest X-ray (CXR): all students require a CXR to assess for evidence of pulmonary tuberculosis, as well as other chest pathologies, including current chest infections or structural abnormalities. There are two to three staff members at this station, one registering, one coordinating, and the other one conducting the X-rays. On average, students spend around 4–25 min at this station. The X-ray itself only takes 2–3 min; however, the preparation and waiting time is required, as female students are requested to remove their bra and tops and wear a gown, as well as put their hair in a bun to avoid artefacts on the X-ray.
- 6.
- Doctor consultation: students are required to complete a doctor’s consultation, where their blood pressure (BP), pulse, colour vision, and a physical examination are completed. There are generally four doctors on duty, with one designated to normal health consultations and the rest focused on matriculation health screening. After 5:30 pm, there is only one doctor to attend to the remaining students still to be seen. The consultation times range from 2–10 min, with an average of 3–4 min per student which varies from doctor to doctor.
2.4. Data Management
2.5. Equipment and Manpower
2.6. Ethical Considerations
3. Results
3.1. Demographics
3.2. Physical Measures
3.3. Medical History
3.4. Allergies and Medications
3.5. Family History
3.6. Smoking
3.7. Alcohol
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Health Screening Questionnaire
Appendix A.1. Introduction
Appendix A.2. Personal Details
Appendix A.3. Medical History
Appendix A.4. Medications and Allergies
Appendix A.5. Family History
Appendix A.6. Substance Use
Appendix A.6.1. Smoking
Appendix A.6.2. Alcohol Consumption (AUDIT-C Score)
Appendix B. Personal Data Protection Notice and Consent
References
- Jewett, A.; Bell, T.; Cohen, N.J.; Buckley, K.; Leino, E.V.; Even, S.; Beavers, S.; Brown, C.; Marano, N. US college and university student health screening requirements for tuberculosis and vaccine-preventable diseases, 2012. J. Am. Coll. Health 2016, 64, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.Y.; Arbour-Nicitopoulos, K.P.; Duku, E.; Faulkner, G. Patterns of multiple health risk-behaviours in university students and their association with mental health: Application of latent class analysis. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2016, 36, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, M.Y.; Cairney, J.; Faulkner, G.E.; Pullenayegum, E.E. Physical activity and other health-risk behaviors during the transition into early adulthood: A longitudinal cohort study. Am. J. Prev. Med. 2012, 42, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.Y.; Faulkner, G.E.; Arbour-Nicitopoulos, K.P.; Cairney, J. Prevalence of health-risk behaviours among Canadian post-secondary students: Descriptive results from the National College Health Assessment. BMC Public Health 2013, 13, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, D.; Gollust, S.E.; Golberstein, E.; Hefner, J.L. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am. J. Orthopsychiatry 2007, 77, 534–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskin, M.; Sun, J.-M.; Abuidhail, J.; Yoshimasu, K.; Kujan, O.; Janghorbani, M.; Flood, C.; Carta, M.G.; Tran, U.S.; Mechri, A.; et al. Suicidal Behavior and Psychological Distress in University Students: A 12-nation Study. Arch. Suicide Res. 2016, 20, 369–388. [Google Scholar] [CrossRef]
- Said, D.; Kypri, K.; Bowman, J. Risk factors for mental disorder among university students in Australia: Findings from a web-based cross-sectional survey. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 935–944. [Google Scholar] [CrossRef]
- Subramaniam, M.; Abdin, E.; Vaingankar, J.A.; Shafie, S.; Chua, B.Y.; Sambasivam, R.; Zhang, Y.J.; Shahwan, S.; Chang, S.; Chua, H.C.; et al. Tracking the mental health of a nation: Prevalence and correlates of mental disorders in the second Singapore mental health study. Epidemiol. Psychiatr. Sci. 2020, 29. [Google Scholar] [CrossRef] [Green Version]
- News, U.W. Worldwide Student Numbers Forecast to Double by 2025. 2012 [cited 2019 21/08/19]. Available online: https://www.universityworldnews.com/post.php?story=20120216105739999 (accessed on 21 August 2019).
- Knopf, J.A.; Finnie, R.K.; Peng, Y.; Hahn, R.A.; Truman, B.I.; Vernon-Smiley, M.; Johnson, V.C.; Johnson, R.L.; Fielding, J.E.; Muntaner, C. School-based health centers to advance health equity: A Community Guide systematic review. Am. J. Prev. Med. 2016, 51, 114–126. [Google Scholar] [CrossRef] [Green Version]
- Programs, S.U.S.L. Resilience Resources. Available online: https://learningconnection.stanford.edu/resilience-project (accessed on 25 April 2020).
- University, V. REDCap. Available online: https://www.project-redcap.org/ (accessed on 25 April 2020).
- World Health Organization, Body mass index - BMI. [cited 2020]. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 25 April 2020).
- Department of Statistics, M.O.T.I. Republic of Singapore. POPULATION TRENDS, 2018. Available online: https://www.singstat.gov.sg/-/media/files/publications/population/population2018.pdf (accessed on 25 April 2020).
- Schreiner, P.J.; Terry, J.G.; Evans, G.W.; Hinson, W.H.; Crouse, J.R.; Heiss, G. Sex-specific associations of magnetic resonance imaging-derived intra-abdominal and subcutaneous fat areas with conventional anthropometric indices. The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 1996, 144, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Pischon, T.; Boeing, H.; Hoffmann, K.; Bergmann, M.; Schulze, M.B.; Overvad, K.; Van der Schouw, Y.T.; Spencer, E.; Moons, K.G.; Tjonneland, A.; et al. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2008, 359, 2105–2120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.; Willett, W.C.; Colditz, G.A.; Hunter, D.J.; Manson, J.E.; Rosner, B.; Speizer, F.E.; Hankinson, S.E. Waist circumference, waist:hip ratio, and risk of breast cancer in the Nurses’ Health Study. Am. J. Epidemiol. 1999, 150, 1316–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, S.; Wang, Z.; Heshka, S.; Heo, M.; Faith, M.S.; Heymsfield, S.B. Waist circumference and obesity-associated risk factors among whites in the third National Health and Nutrition Examination Survey: Clinical action thresholds. Am. J. Clin. Nutr. 2002, 76, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Allison, D.B.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, R. Waist circumference and cardiometabolic risk: A consensus statement from shaping America’s health: Association for Weight Management and Obesity Prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Diabetes Care 2007, 30, 1647–1652. [Google Scholar]
- Health, M.O. National Population Health Survey 2016/17; Ministry of Health: Singapore, 2017.
- Health Promotion Board. National Nutrition Survey 2010; Health Promotion Board: Singapore, 2010.
- Singapore Ministry of Health. National Health Survey 2010; Singapore Ministry of Health: Singapore, 2011.
- Brener, N.D.; Eaton, D.K.; Lowry, R.; McManus, T. The association between weight perception and BMI among high school students. Obes. Res. 2004, 12, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Cilliers, J.; Senekal, M.; Kunneke, E. The association between the body mass index of first-year female university students and their weight-related perceptions and practices, psychological health, physical activity and other physical health indicators. Public Health Nutr. 2006, 9, 234–243. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, E.-L.; Pathy, P.; Chan, Y.H. Anorexia nervosa in Singapore: An eight-year retrospective study. Singap. Med J. 2005, 46, 275. [Google Scholar]
- Pike, K.M.; Dunne, P.E. The rise of eating disorders in Asia: A review. J. Eat. Disord. 2015, 3, 33. [Google Scholar] [CrossRef] [Green Version]
- Robin, G.K.H.; Ee Lian, L.; Lim, P.; Si, L.S. Anorexia nervosa and eating disorder not otherwise specified (NOS) in Singapore: A seven-year retrospective study. ASEAN J. Psychiatr. 2016, 17, 21. [Google Scholar]
- Seidenfeld, M.E.; Rickert, V.I. Impact of anorexia, bulimia, and obesity on the gynecologic health of adolescents. Am. Fam. Physician 2001, 64, 445. [Google Scholar]
- Sirang, Z.; Bashir, H.H.; Jalil, B.; Khan, S.H.; Hussain, S.A.; Baig, A.; Taufeeq, M.; Samad, K.; Kadir, M.M. Weight patterns and perceptions among female university students of Karachi: A cross sectional study. BMC Public Health 2013, 13, 230. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.J.; Jiang, Y. Epidemiology of myopia. Eye (Lond. Engl.) 2014, 28, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saw, S.-M.; Carkeet, A.; Chia, K.-S.; Stone, R.A.; Tan, D.T.H. Component dependent risk factors for ocular parameters in Singapore Chinese children. Ophthalmology 2002, 109, 2065–2071. [Google Scholar] [CrossRef]
- Seet, B.; Wong, T.Y.; Tan, D.T.H.; Saw, S.M.; Balakrishnan, V.; Lee, L.K.H.; Lim, A.S.M. Myopia in Singapore: Taking a public health approach. Br. J. Ophthalmol. 2001, 85, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lougheed, T. Myopia: The evidence for environmental factors. Environ. Health Perspect. 2014, 122, A12–A19. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Foster, P.J.; Johnson, G.J.; Seah, S.K. Refractive errors, axial ocular dimensions, and age-related cataracts: The Tanjong Pagar survey. Investig. Ophthalmol. Vis. Sci. 2003, 44, 1479–1485. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.L.; Shih, Y.F.; Tsai, C.B.; Chen, C.J.; Lee, L.A.; Hung, P.T.; Hou, P.K. Epidemiologic study of ocular refraction among schoolchildren in Taiwan in 1995. Optom. Vis. Sci. 1999, 76, 275–281. [Google Scholar] [CrossRef]
- Saw, S.-M.; Tong, L.; Chua, W.-H.; Chia, K.-S.; Koh, D.; Tan, D.T.H.; Katz, J. Incidence and Progression of Myopia in Singaporean School Children. Investig. Ophthalmol. Vis. Sci. 2005, 46, 51–57. [Google Scholar] [CrossRef]
- Xiong, S.; Sankaridurg, P.; Naduvilath, T.; Zang, J.; Zou, H.; Zhu, J.; Lv, M.; He, X.; Xu, X. Time spent in outdoor activities in relation to myopia prevention and control: A meta-analysis and systematic review. Acta Ophthalmol. 2017, 95, 551–566. [Google Scholar] [CrossRef] [Green Version]
- The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998, 351, 1225–1232. [Google Scholar] [CrossRef]
- Wang, X.S.; Shek, L.P.; Ma, S.; Soh, S.E.; Lee, B.W.; Goh, D.Y.T. Time trends of co-existing atopic conditions in Singapore school children: Prevalence and related factors. Pediatric Allergy Immunol. 2010, 21, e137–e141. [Google Scholar] [CrossRef] [PubMed]
- Cheok, S.; Yee, F.; Song, M.J.Y.; Leow, R.; Ho, M.S.L.; Yew, Y.W.; Tay, Y.K.; Rebello, S.A.; Luo, N.; Koh, M.J.A. Prevalence and descriptive epidemiology of atopic dermatitis and its impact on quality of life in Singapore. Br. J. Dermatol. 2018, 178, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Gelfand, J.M.; Margolis, D.J.; Boguniewicz, M.; Fonacier, L.; Grayson, M.H.; Simpson, E.L.; Ong, P.Y.; Chiesa Fuxench, Z.C. Patient burden and quality of life in atopic dermatitis in US adults: A population-based cross-sectional study. Ann. Allergy Asthma Immunol. 2018, 121, 340–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazarika, N.; Archana, M. Hazarika, N.; Archana, M. The Psychosocial Impact of Acne Vulgaris. Indian J. Dermatol. 2016, 61, 515–520. [Google Scholar] [CrossRef]
- Tan, J.H.; Shahwan, S.; Satghare, P.; Cetty, L.; Verma, S.; Sendren, J.R.; Chong, S.A.; Subramaniam, M. Binge drinking: Prevalence, correlates, and expectancies of alcohol use among individuals with first-episode psychosis. Early Interv. Psychiatry 2019, 13, 1136–1145. [Google Scholar] [CrossRef]
- Biolcati, R.; Passini, S.; Mancini, G. “I cannot stand the boredom.” Binge drinking expectancies in adolescence. Addict. Behav. Rep. 2016, 3, 70–76. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Ethnicity | Local Students | International Students | Total n (%) | ||
|---|---|---|---|---|---|
| Female | Male | Female | Male | ||
| Chinese | 32 | 21 | 153 | 193 | 399 (75%) |
| Malay | 3 | 2 | 0 | 0 | 5 (1%) |
| Indian | 1 | 4 | 29 | 29 | 59 (11%) |
| White European | 0 | 0 | 2 | 1 | 3 (1%) |
| Other | 1 | 0 | 29 | 43 | 73 (14%) |
| Total | 37 | 27 | 213 | 266 | 543 * |
| Classification (WHO) | BMI | Female | Male | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Severely underweight | <16 | 3 | 1.3% | 4 | 1.4% |
| Mildly underweight | 16–16.9 | 13 | 5.5% | 4 | 1.4% |
| Moderately underweight | 17–18.49 | 29 | 12.2% | 22 | 7.8% |
| Normal range | 18.5–24.9 | 162 | 68.4% | 162 | 57.4% |
| Overweight | 25–29.9 | 22 | 9.3% | 69 | 24.5% |
| Obese | 30–39.9 | 8 | 3.4% | 20 | 7.1% |
| Severely obese | >40 | 0 | 0.0% | 1 | 0.4% |
| Total students | 237 | 282 | |||
| Common Medical Conditions | No. of Students | % of Total |
|---|---|---|
| Myopia | 79 | 10.8% |
| Asthma | 13 | 1.8% |
| Eczema | 14 | 1.9% |
| Acne | 9 | 1.2% |
| Allergic rhinitis | 6 | 0.8% |
| Urticaria | 5 | 0.7% |
| Hepatitis B | 3 | 0.4% |
| Colour blindness | 3 | 0.4% |
| Hypertension | 1 | 0.1% |
| Irregular menses (females) | 20 | 8.0 * |
| Severe menstrual pain (females) | 15 | 6.0 * |
| Allergies | ||
| Drug Allergies | 38 | 7.1% |
| Non-drug allergies | 58 | 10.8% |
| Alcohol | 2 | 3.4% ** |
| Nuts | 8 | 13.8% ** |
| Dust | 12 | 20.7% ** |
| Shellfish | 12 | 20.7% ** |
| Seafood | 10 | 17.2% ** |
| Cosmetics | 4 | 6.9% ** |
| Family History | ||
| Hypertension | 178 | 33.3% |
| Diabetes | 158 | 29.5% |
| Heart Disease | 76 | 14.2% |
| Cancer | 66 | 12.3% |
| Hypercholesterolaemia | 51 | 9.5% |
| Asthma | 25 | 4.7% |
| Obesity | 15 | 2.8% |
| Eczema | 5 | 0.9% |
| Kidney disease | 5 | 0.9% |
| Depression | 5 | 0.9% |
| Anxiety | 5 | 0.9% |
| Tuberculosis | 3 | 0.6% |
| Dementia | 3 | 0.6% |
| Schizophrenia | 3 | 0.6% |
| Bipolar disorder | 1 | 0.2% |
| Alcohol or substance abuse | 1 | 0.2% |
| Chronic Obstructive Lung Disease | 0 | 0.0% |
| Gender | Age Started Smoking | No. of Cigarettes Per Day | Attempted to Stop | Method of Cessation |
|---|---|---|---|---|
| Male | 21 | 10 | Yes | Nicotine replacement |
| Male | 22 | 5 | No | n/a |
| Male | 15 | 6 | Yes | Abrupt cessation |
| Male | 19 | 4 | No | n/a |
| Male | 20 | 2 | No | n/a |
| Male | 14 | 3 | No | n/a |
| Male | 20 | 2 | No | n/a |
| Female | 19 | 5 | Yes | Smokeless tobacco |
| AUDIT C | Male | Female | Total |
|---|---|---|---|
| 1 | 73 | 59 | 132 |
| 2 | 19 | 8 | 27 |
| 3 | 16 | 7 | 23 |
| 4 | 6 | 3 | 9 |
| 5 | 1 | 0 | 1 |
| 6 | 2 | 0 | 2 |
| 7 | 0 | 0 | 0 |
| 8 | 1 | 0 | 1 |
| Total | 118 | 77 | 195 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinazze, P.A.; Kasteleyn, M.J.; Aardoom, J.J.; Car, J.; Chavannes, N.H. Cross-Sectional Analysis of University Students’ Health Using a Digitised Health Survey. Int. J. Environ. Res. Public Health 2020, 17, 3009. https://doi.org/10.3390/ijerph17093009
Spinazze PA, Kasteleyn MJ, Aardoom JJ, Car J, Chavannes NH. Cross-Sectional Analysis of University Students’ Health Using a Digitised Health Survey. International Journal of Environmental Research and Public Health. 2020; 17(9):3009. https://doi.org/10.3390/ijerph17093009
Chicago/Turabian StyleSpinazze, Pier A., Marise J. Kasteleyn, Jiska J. Aardoom, Josip Car, and Niels H. Chavannes. 2020. "Cross-Sectional Analysis of University Students’ Health Using a Digitised Health Survey" International Journal of Environmental Research and Public Health 17, no. 9: 3009. https://doi.org/10.3390/ijerph17093009