Satisfaction with Social Support Received from Social Relationships in Cases of Chronic Pain: The Influence of Personal Network Characteristics in Terms of Structure, Composition and Functional Content


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample Description
2.3. Variables
2.4. Data Collection Instruments
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Sociodemographic Variables
3.2. Bivariate Analysis
3.2.1. Ego Variables
- Participants aged between 30 and 51 years; mean satisfaction 2.01 (SD 0.19).
- Participants aged between 52 and 63 years; mean satisfaction 1.72 (SD 0.17).
- Participants aged between 65 and 73 years; mean satisfaction 1.51 (SD 0.18).
- Duration of pain between 1 and 8 years; mean satisfaction 2.04 (SD 0.18).
- Duration of pain between 9 and 19 years; mean satisfaction 1.67 (SD 0.18).
- Duration of pain between 20 and 39 years; mean satisfaction 1.5 (SD 0.18).
3.2.2. Composition Variables
3.2.3. Structural Variables
3.2.4. Functional Social Support
3.3. Multivariate Logistic Regression Model
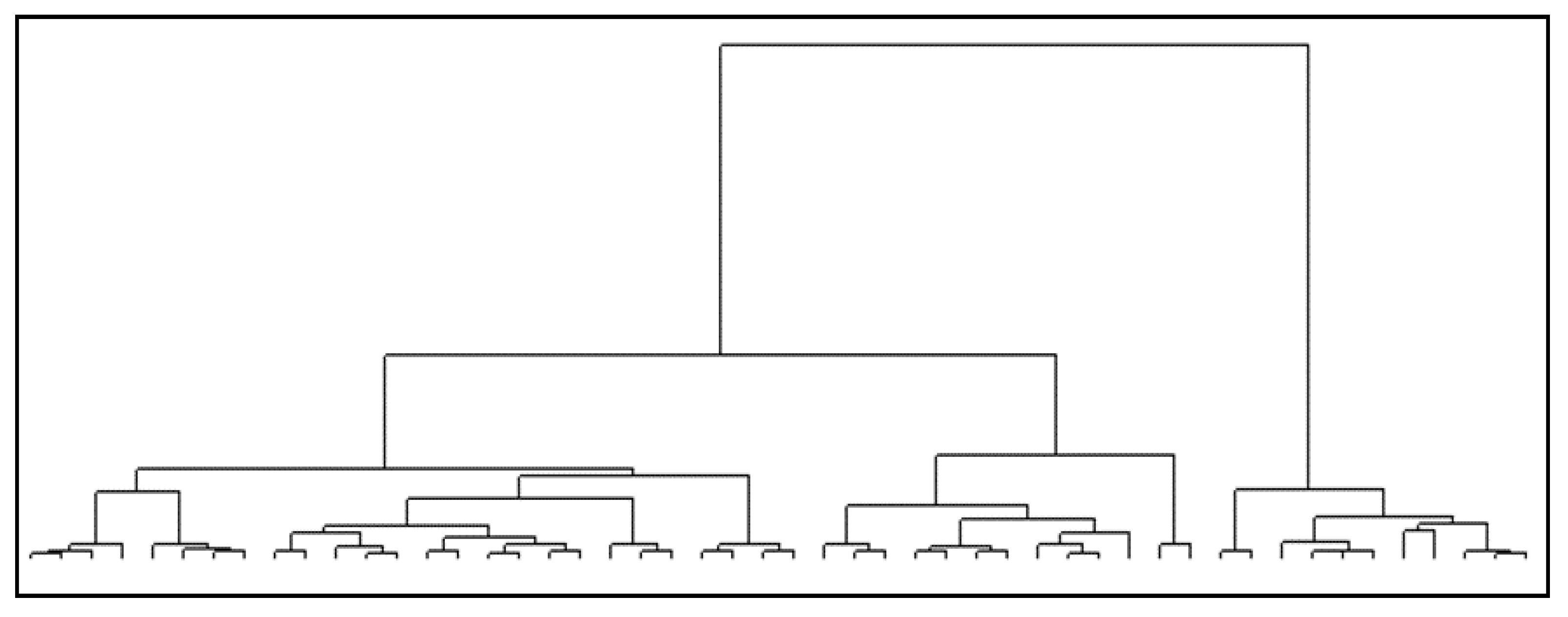
3.4. Cluster Analysis
3.4.1. Composition Variables
3.4.2. Structural Variables
3.4.3. Functional Social Support
4. Discussion
4.1. Composition Variables
4.2. Structural Variables
4.3. Functional Social Support
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 2 April 2020).
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving chronic illness care: Translating evidence into action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlow, J.; Wright, C.; Sheasby, J.; Turner, A.; Hainsworth, J. Self-management approaches for people with chronic conditions: A review. Patient Educ. Couns. 2002, 48, 177–187. [Google Scholar] [CrossRef]
- Van Houtum, L.; Rijken, M.; Heijmans, M.; Groenewegen, P. Self-management support needs of patients with chronic illness: Do needs for support differ according to the course of illness? Patient Educ. Couns. 2013, 93, 626–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, R.L.; Kennedy, A.; Sanders, C. Evolving ’self’-management: Exploring the role of social network typologies on individual long-term condition management. Heal. Expect. 2015, 19, 1044–1061. [Google Scholar] [CrossRef]
- Kendall, P.R.W. Investing in Prevention:Improving Health and Creating Sustainability; Bristish Columbia: Vancouver, Canada, 2010. [Google Scholar]
- World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Epping-Jordan, J.E. Integrated approaches to prevention and control of chronic conditions. Kidney Int. 2005, 68, 86–88. [Google Scholar] [CrossRef] [Green Version]
- Nuño, R.; Coleman, K.; Bengoa, R.; Sauto, R. Integrated care for chronic conditions: The contribution of the ICCC Framework. Health Policy 2012, 105, 55–64. [Google Scholar] [CrossRef]
- Barlow, J.H.; Brancroft, G.V.; Turner, A.P. Self-management training for people with chronic disease: A shared learning experience. J. Health Psychol. 2005, 10, 863–872. [Google Scholar] [CrossRef]
- Davies, F.; Wood, F.; Bullock, A.; Wallace, C.; Edwards, A. Interventions to improve the self-management support health professionals provide for people with progressive neurological conditions: Protocol for a realist synthesis. BMJ Open 2017, 7, e014575. [Google Scholar] [CrossRef]
- Nøst, T.H.; Steinsbekk, A.; Bratås, O.; Grønning, K. Expectations, effect and experiences of an easily accessible self-management intervention for people with chronic pain: Study protocol for a randomised controlled trial with embedded qualitative study. Trials 2016, 17, 325. [Google Scholar]
- Crotty, M.M.; Henderson, J.; Ward, P.R.; Fuller, J.; Rogers, A.; Kralik, D.; Gregory, S. Analysis of social networks supporting the self-management of type 2 diabetes for people with mental illness. BMC Health Serv. Res. 2015, 15, 257. [Google Scholar] [CrossRef] [Green Version]
- Gallant, M.P. The influence of social support on chronic illness self-management: A review and directions for research. Heal. Educ. Behav. 2003, 30, 170–195. [Google Scholar] [CrossRef] [PubMed]
- Vassilev, I.; Rogers, A.; Blickem, C.; Brooks, H.; Kapadia, D.; Kennedy, A.; Sanders, C.; Kirk, S.; Reeves, D. Social networks, the “Work” and work force of chronic illness self-management: A survey analysis of personal communities. PLoS ONE 2013, 8, e59723. [Google Scholar] [CrossRef] [PubMed]
- Koetsenruijter, J.; Van Lieshout, J.; Vassilev, I.; Portillo, M.C.; Serrano, M.; Knutsen, I.; Roukova, P.; Lionis, C.; Todorova, E.; Foss, C.; et al. Social support systems as determinants of self-management and quality of life of people with diabetes across Europe: Study protocol for an observational study. Health Qual. Life Outcomes 2014, 12, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeves, D.; Blickem, C.; Vassilev, I.; Brooks, H.; Kennedy, A.; Richardson, G.; Rogers, A. The contribution of social networks to the health and self-management of patients with long-term conditions: A longitudinal study. PLoS ONE 2014, 9, e98340. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.; Ensel, W.; Simeone, R.; Kuo, W. Social support, stressful life events, and illness: A model and an empirical test. J. Heal. Soc. Behav. 1979, 20, 108–119. [Google Scholar] [CrossRef]
- Lin, N.; Dean, A.; Ensel, W.M. Social support scales: A methodological note. Schizophr. Bull. 1981, 7, 73–89. [Google Scholar] [CrossRef] [Green Version]
- House, J.S. Social support and social structure. Sociol. Forum 1987, 2, 135–146. [Google Scholar] [CrossRef] [Green Version]
- House, J.S.; Landis, K.R.; Umberson, D. Social relationships and health. Science 1988, 241, 540–545. [Google Scholar] [CrossRef]
- Rn, D.C.B.; Rn, F.P.; Benton, D.C.; Pérez-Raya, F.; Fernández-Fernández, M.P.; González-Jurado, M.A. A systematic review of nurse-related social network analysis studies. Int. Nurs. Rev. 2014, 62, 321–339. [Google Scholar]
- Bae, S.H.; Nikolaev, A.N.; Seo, J.; Castner, J. Health care provider social network analysis: A systematic review. Nurs. Outlook 2015, 63, 566–584. [Google Scholar] [CrossRef]
- Scherlowski, H.; Guimaraes de Araújo, M.; Andrade, J.; Feijó, T.; Souza, V.; dos Santos, R. Social network analysis in primary health care: An integrative review. Integr. Rev. 2018, 31, 108–115. [Google Scholar]
- Hawe, P.; Webster, C.; Shiell, A. A glossary of terms for navigating the field of social network analysis. J. Epidemiol. Community Health 2004, 58, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.M.; Robinson, J.C. Social network analysis: Presenting an underutilised method for nursing research. J. Adv. Nurs. 2018, 74, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Del-Pino-Casado, R.; Frías-Osuna, A.; Palomino-Moral, P.; Ruzafa-Martínez, M.; Ramos-Morcillo, A. Social support and subjective burden in caregivers of adults and older adults: A meta-analysis. PLoS ONE 2018, 13, e0189874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Madrid, M.N.; del Río-Lozano, M.; Fernandez-Peña, R.; Jiménez-Pernett, J.; García-Mochón, L.; Lupiañez-Castillo, A.; García-Calvente, M.M. Gender differences in social support received by informal caregivers: A personal network analysis approach. Int. J. Environ. Res. Public Health 2019, 16, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, B.; Pescosolido, B.; Borgatti, S. Egocentric Network Analysis: Foundations, Methods, and Models; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- McCarty, C. Structure in personal networks. J. Soc. Struct. 2002, 3, 20. [Google Scholar]
- Hâncean, M.; Molina, J.L.; Lubbers, M.J. Recent advancements, developments and applications of personal network analysis. Int. Rev. Soc. Res. 2016, 6, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Molina, J.L. El estudio de las redes personales: Contribuciones, métodos y perspectiva. Empiria Rev. Metodol. Cienc. Soc. 2005, 10, 71–105. [Google Scholar]
- McCarty, C.; Lubbers, M.J.; Vacca, R.; Molina, J.L. How personal networks have been used so far. In Conducting Personal Network Research. A Practical Guide; The Guilford Press: New York, NY, USA, 2019; p. 270. [Google Scholar]
- Smith, K.; Christakis, N. Social networks and health. Annu. Rev. Sociol. 2008, 34, 405–418. [Google Scholar] [CrossRef] [Green Version]
- Doeglas, D.; Suurmeijer, T.; Briançon, S.; Moum, T.; Krol, B.; Bjelle, A.; Sanderman, R.; Van der Heuvel, W. An international study on measuring social support: Interactions and satisfaction. Soc. Sci. Med. 1996, 43, 1389–1397. [Google Scholar] [CrossRef] [Green Version]
- Franks, H.M.; Cronan, T.A.; Oliver, K. Social support in women with fibromyalgia: Is quality more important than quantity? J. Community Psychol. 2004, 32, 425–438. [Google Scholar] [CrossRef]
- Tardy, C. Social support measurement. Am. J. Community Psychol. 1985, 13, 187–202. [Google Scholar] [CrossRef]
- Bernardes, S.F.; Forgeron, P.; Fournier, K.; Reszel, J. Beyond solicitousness: A comprehensive review on informal pain-related social support. Pain 2017, 158, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Fernández Peña, R. El Estudio del Apoyo Social y la Calidad de Vida Desde las Redes Personales: El Caso del Dolor Crónico. Ph.D. Thesis, Universidad Autónoma de Barcelona, Barcelona, Spain, 2015. [Google Scholar]
- Fernández-Peña, R.; Molina, J.L.; Valero, O. Personal network analysis in the study of social support: The case of chronic pain. Int. J. Environ. Res. Public Health 2018, 15, 2695. [Google Scholar]
- Borgatti, S.P.; Everett, M.G. Analyzing Social Networks; Sage Publications: London, UK, 2013. [Google Scholar]
- Greenacre, M. Correspondence Analysis in Practice, 2nd ed.; Chapman & Hall: London, UK, 2007. [Google Scholar]
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Hartigan, J.A. Clustering Algorithms; Wiley & Sons: New York, NY, USA, 1975. [Google Scholar]
- Weiner, A.S.B.; Hannum, J.W. Differences in the quantity of social support between geographically close and long-distance friendships. J. Soc. Pers. Relat. 2012, 30, 662–672. [Google Scholar] [CrossRef]
- Fernández, M. Social support networks in Spain: The factors that determine models of choice. Int. Sociol. 2012, 27, 384–402. [Google Scholar]
- Mok, D.; Wellman, B. Did distance matter before the Internet? Interpersonal contact and support in the 1970s. Soc. Netw. 2007, 29, 430–461. [Google Scholar] [CrossRef]
- Tomini, F.; Tomini, S.M.; Groot, W. Understanding the value of social networks in life satisfaction of elderly people: A comparative study of 16 European countries using SHARE data. BMC Geriatr. 2016, 16, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonucci, T.C.; Akiyama, H.; Lansford, J.E. Negative effects of close social relations. Fam. Relat. 1998, 47, 379–384. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D. Can we improve our physical health by altering our social networks? Perspect. Psychol. Sci. 2009, 4, 375–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rook, K.S. The negative side of social interaction: Impact on psychological well-being. J. Pers. Soc. Psychol. 1984, 46, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Rook, K.S. Exposure and reactivity to negative social exchanges: A preliminary investigation using daily diary data. J. Gerontol. 2003, 58, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newsom, J.T.; Rook, K.S.; Nishishiba, M.; Sorkin, D.H.; Mahan, T.L. Understanding the relative importance of positive and negative social exchanges: Examining specific domains and appraisals. J. Gerontol. 2005, 60, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Català, E.; Reig, E.; Artés, M.; Aliaga, L.; López, J.S.; Segú, J.L. Prevalence of pain in the Spanish population: Telephone survey in 5000 homes. Eur. J. Pain 2002, 6, 133–140. [Google Scholar] [CrossRef]
- Geisser, M.E.; Cano, A.; Leonard, M. Factors associated with marital satisfaction and mood among spouses of persons with chronic back pain. J. Pain 2005, 6, 518–525. [Google Scholar] [CrossRef]
- Leonard, M.T.; Cano, A.; Johansen, A.B. Chronic pain in a couples context: A review and integration of theoretical models and empirical evidence. J. Pain 2006, 7, 377–390. [Google Scholar] [CrossRef]
- Cano, A.; Leonard, M. Integrative behavioral couple therapy for chronic pain: Promoting behavior change and emotional acceptance. J. Clin. Psychol. 2006, 62, 1409–1418. [Google Scholar] [CrossRef]
- Roy, R. What happens to spouses? In Social Relations and Chronic Pain; Kluwer Academic Publishers: New York, NY, USA, 2002; pp. 57–70. ISBN 0306471973. [Google Scholar]
- Entwisle, B.; Faust, K.; Rindfuss, R.R.R.; Kaneda, T. Networks and contexts: Variation in the structure of social ties. Am. J. Sociol. 2007, 112, 1495–1533. [Google Scholar] [CrossRef] [Green Version]
- Jolly, A.; Muth, S.; Wylie, J.; Potterat, J. Sexual networks and sexually transmitted infections: A tale of two cities. J. Urban Heal. 2001, 78, 433–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.M.A.; Grierson, J.; Wain, D.; Pitts, M.; Pattison, P. Associations between the sexual behaviour of men who have sex with men and the structure and composition of their social networks. Sex. Transm. Infect. 2004, 80, 455–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birkett, M.; Kuhns, L.; Latkin, C.; Muth, S.; Mustanski, B. The sexual networks of racially diverse young men who have sex with men. Arch. Sex. Behav. 2015, 44, 1787–1797. [Google Scholar] [CrossRef] [PubMed]
- Morris, M. Sexual networks and HIV in four african populations: The use of standardized behavioral surveys with biological markers. In Network Epidemiology: A Handbook for Survey Design and Data Collection; Oxford University Press on Demand: Oxford, UK, 2004; pp. 58–84. ISBN 9780199269013. [Google Scholar]
- Bearman, P.S.; Moody, J.; Stovel, K. Chains of affection: The structure of adolescent romantic and sexual networks. Am. J. Sociol. 2004, 110, 44–91. [Google Scholar] [CrossRef] [Green Version]
- Hansen, L.R.; Pedersen, S.B.; Overgaard, C.; Torp-Pedersen, C.; Ullits, L.R. Associations between the structural and functional aspects of social relations and poor mental health: A cross-sectional register study. BMC Public Health 2017, 17, 860. [Google Scholar] [CrossRef] [Green Version]
- Haas, S.A.; Schaefer, D.R.; Kornienko, O. Health and the structure of adolescent social networks. J. Health Soc. Behav. 2010, 51, 424–439. [Google Scholar] [CrossRef]
- Agneessens, F.; Waege, H.; Lievens, J. Diversity in social support by role relations: A typology. Soc. Netw. 2006, 28, 427–441. [Google Scholar] [CrossRef]
- Platt, J.; Keyes, K.M.; Koenen, K.C. Size of the social network versus quality of social support: Which is more protective against PTSD? Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1279–1286. [Google Scholar] [CrossRef]
- Stokes, J.P. Predicting satisfaction with social support form social network structure. Am. J. Community Psychol. 1983, 11, 141–152. [Google Scholar] [CrossRef]
- Ashida, S.; Heaney, C.A. Differential associations of social support and social connectedness with structural features of social networks and the health status of older adults. J. Aging Health 2008, 20, 872–893. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, B.J. Natural support systems and coping with major life changes. Am. J. Community Psychol. 1980, 8, 159–172. [Google Scholar] [CrossRef]
- Burt, R.S. Structural holes and good ideas. Am. J. Sociol. 2004, 110, 349–399. [Google Scholar] [CrossRef]
- Wellman, B.; Wortley, S. Different strokes from different folks: Community ties and social support. Am. J. Sociol. 1990, 96, 558–588. [Google Scholar] [CrossRef] [Green Version]
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling alone: America’s declining social capital. In Culture and Politics; Palgrave Macmillan: New York, NY, USA, 2000; pp. 223–234. [Google Scholar]
- Chandola, T.; Marmot, M.; Siegrist, J. Failed reciprocity in close social relationships and health: Findings from the Whitehall II study. J. Psychosom. Res. 2007, 63, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Knowlton, A.R.; Yang, C.; Bohnert, A.; Wissow, L.; Chander, G.; Arnsten, J.A. Informal care and reciprocity of support are associated with HAART adherence among men in baltimore. AIDS Behav. 2011, 15, 1429–1436. [Google Scholar] [CrossRef] [Green Version]
- Mercken, L.; Candel, M.; Willems, P.; De Vries, H. Disentangling social selection and social influence effects on adolescent smoking: The importance of reciprocity in friendships. Addiction 2007, 102, 1483–1492. [Google Scholar] [CrossRef]
- Adelman, R.D.; Tmanova, L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. J. Am. Med. Assoc. 2014, 311, 1052–1059. [Google Scholar] [CrossRef]
- Jones, S.L.; Hadjistavropoulos, H.D.; Janzen, J.A.; Hadjistavropoulos, T. The relation of pain and caregiver burden in informal order adult caregivers. Pain Med. 2011, 12, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Rodakowski, J.; Skidmore, E.R.; Rogers, J.C.; Schulz, R. Role of social support in predicting caregiver burden. Arch. Phys. Med. Rehabil. 2012, 93, 2229–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, B.A.; Krause, N.; Liang, J.; Bennett, J. Tracking changes in social relations throughout late life. J. Gerontol. 2007, 62, 90–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feld, S.L.L.; Suitor, J.J.J.; Gartner, J.G.; Hoegh, J.G.; Gartner, J.G. Describing changes in personal networks over time. Field Methods 2007, 19, 218–236. [Google Scholar] [CrossRef]
- Mollenhorst, G.; Volker, B.; Flap, H. Changes in personal relationships: How social contexts affect the emergence and discontinuation of relationships. Soc. Netw. 2014, 37, 65–80. [Google Scholar] [CrossRef]
- Fischer, C.S.; Beresford, L. Changes in support networks in late middle age: The extension of gender and educational differences. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 70, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Mean (SD) |
|---|---|---|
| Age of the alter * | ≤30 years | 1.36 (0.17) |
| 31–50 years | 1.95 (0.13) | |
| 51–60 years | 1.67 (0.16) | |
| >60 years | 1.69 (0.14) | |
| Sex of the alter * | Women | 1.91 (0.12) |
| Men | 1.56 (0.12) | |
| Tie with the ego * | Partner | 3.22 (0.26) |
| Parents | 3.03 (0.33) | |
| Brothers | 1.75 (0.18) | |
| Children | 2.77 (0.19) | |
| Other family members | 1.32 (0.13) | |
| Friends | 1.61 (0.14) | |
| Other ties | 1.41 (0.18) | |
| Strength of the tie * | Very close | 2.83 (0.13) |
| Quite close | 2.19 (0.12) | |
| Close | 1.50 (0.12) | |
| Not very close | 0.74 (0.13) | |
| Not at all close | 0.21 (0.20) | |
| Place of residence of the alter compared to the ego | Same locality | 1.89 (0.13) |
| Same province | 1.66 (0.13) | |
| Other province/country | 1.53 (0.18) |
| Variable | Range/Category | Mean (SD) |
|---|---|---|
| Density * | <40% | 1.57 (0.15) |
| 41–60% | 1.64 (0.16) | |
| >60% | 2.28 (0.22) | |
| Degree centrality (alter) * | 0–5 | 1.35 (0.14) |
| 6–11 | 1.60 (0.13) | |
| 12–19 | 2.35 (0.15) | |
| Betweeness Centrality (alter) * | 0 | 1.44 (0.13) |
| 0.1–1.2 | 1.69 (0.15) | |
| 1.2–114.3 | 2.12 (0.14) | |
| Components | 1 | 2 (0.16) |
| 2 | 1.54 (0.20) | |
| 3–11 | 1.58 (0.18) | |
| Isolates | 0 | 1.89 (0.14) |
| 1 | 1.63 (0.23) | |
| 2–9 | 1.46 (0.22) |
| Variable | Category | Mean (SE) |
|---|---|---|
| Social support variables in provider relationships (n = 401) | ||
| Type * | Emotional | 2.37 (0.07) |
| Emotional and instrumental | 3.18 (0.10) | |
| Emotional, instrumental and informational | 3.62 (0.18) | |
| Other types of support | 2.55 (0.14) | |
| Frequency * | Daily | 3.26 (0.09) |
| Weekly | 2.57 (0.08) | |
| Biweekly | 2.42 (0.12) | |
| Monthly | 1.94 (0.11) | |
| >2 months | 1.83 (0.15) | |
| Transmission channel * | Face-to-face | 2.70 (0.09) |
| By telephone | 2.22 (0.13) | |
| Face-to-face and by telephone | 2.74 (0.10) | |
| Internet/Telephone + internet | 2.16 (0.28) | |
| Variation of support * | Increases | 3.22 (0.18) |
| No variation | 1.47 (0.12) | |
| Decreases | 1.73 (0.19) | |
| Reciprocity * | Yes | 1.97 (0.10) |
| No | 0.99 (0.14) | |
| Category | Profile 1 | Profile 2 | Profile 3 |
|---|---|---|---|
| 30–49 years | 38.4 | 31.1 | 19.1 |
| 50–64 years | 35.9 | 37.2 | 37.2 |
| 65 and over | 25.7 | 31.7 | 43.7 |
| Total | 100 | 100 | 100 |
| Variable | Category | Profile 1 | Profile 2 | Profile 3 |
|---|---|---|---|---|
| Age of the alter * | <20 | 2.1 | 7.3 | 15.1 |
| 20–39 | 21.5 | 24.4 | 19.6 | |
| 40–59 | 45.6 | 45.2 | 32.7 | |
| >60 | 30.8 | 23.1 | 32.6 | |
| Sex of the alter * | Male | 45.1 | 41.5 | 57.8 |
| Female | 54.9 | 58.5 | 42.2 | |
| Relationship with ego * | Close family members | 17.3 | 59.8 | 14.1 |
| Family members | 24.9 | 7.9 | 24.1 | |
| Other family member | 4.2 | 9.1 | 17.6 | |
| Friends | 35.9 | 17.1 | 32.2 | |
| Neighbors | 8.4 | 3 | 6.5 | |
| Work and professional colleagues | 9.3 | 3 | 5.5 | |
| Strength of the tie * | Strong tie | 77.2 | 100 | 49.2 |
| Weak tie | 22.8 | 0 | 50.8 | |
| Place of residence of the alter compared to the ego * | Same location | 35 | 58 | 43.2 |
| Same province | 43 | 32.9 | 40.2 | |
| Other province | 17.4 | 8.5 | 12.6 | |
| Other province/country | 4.6 | 0.6 | 4 |
| Variable | Profile 1 | Profile 2 | Profile 3 | Global Mean |
|---|---|---|---|---|
| Density | 0.44 | 0.53 | 0.41 | 0.45 |
| Degree Centrality (a) | 7.08 | 12.44 | 7.25 | 8.60 |
| Betweeness Centrality (a) | 2.41 | 8.53 | 2.10 | 3.98 |
| Components | 2.41 | 2.11 | 3.03 | 2.53 |
| Isolates | 0.91 | 0.74 | 1.62 | 1.10 |
| Variable | Category | Profile 1 | Profile 2 | Profile 3 |
|---|---|---|---|---|
| Type * | Emotional | 83.5 | 34.8 | 0 |
| Instrumental | 5.1 | 2.4 | 0 | |
| Informative | 2.1 | 0 | 0 | |
| All three types of support | 0.4 | 12.8 | 0 | |
| Emotional and instrumental | 3.4 | 46.3 | 0 | |
| Emotional and informative | 3.4 | 3.7 | 0 | |
| Instrumental and informative | 0.4 | 0 | 0 | |
| Professional | 1.7 | 0 | 0 | |
| None | 0 | 0 | 100 | |
| Frequency * | Daily | 7.6 | 63.4 | 0.5 |
| Weekly | 39.2 | 31.7 | 0.5 | |
| Biweekly | 17.3 | 3.7 | 0 | |
| Monthly | 23.6 | 0.6 | 0 | |
| Every 2 or 3 months | 6.3 | 0.6 | 0 | |
| Every 3 months or more | 5.9 | 0 | 99 | |
| Channel of transmission * | Face-to-face | 43.5 | 54.3 | 0 |
| By telephone | 24.1 | 3.7 | 0 | |
| Internet | 3 | 0.6 | 0 | |
| Face-to-face and by telephone | 27.8 | 41.5 | 0 | |
| Telephone and internet | 1.7 | 0 | 0 | |
| No support | 0 | 0 | 100 | |
| Variation * | Has not varied | 70.5 | 61 | 92 |
| More support | 13.1 | 31.1 | 0 | |
| Less support | 16.5 | 7.9 | 8 | |
| Reciprocity * | Yes | 78.9 | 93.3 | 59.3 |
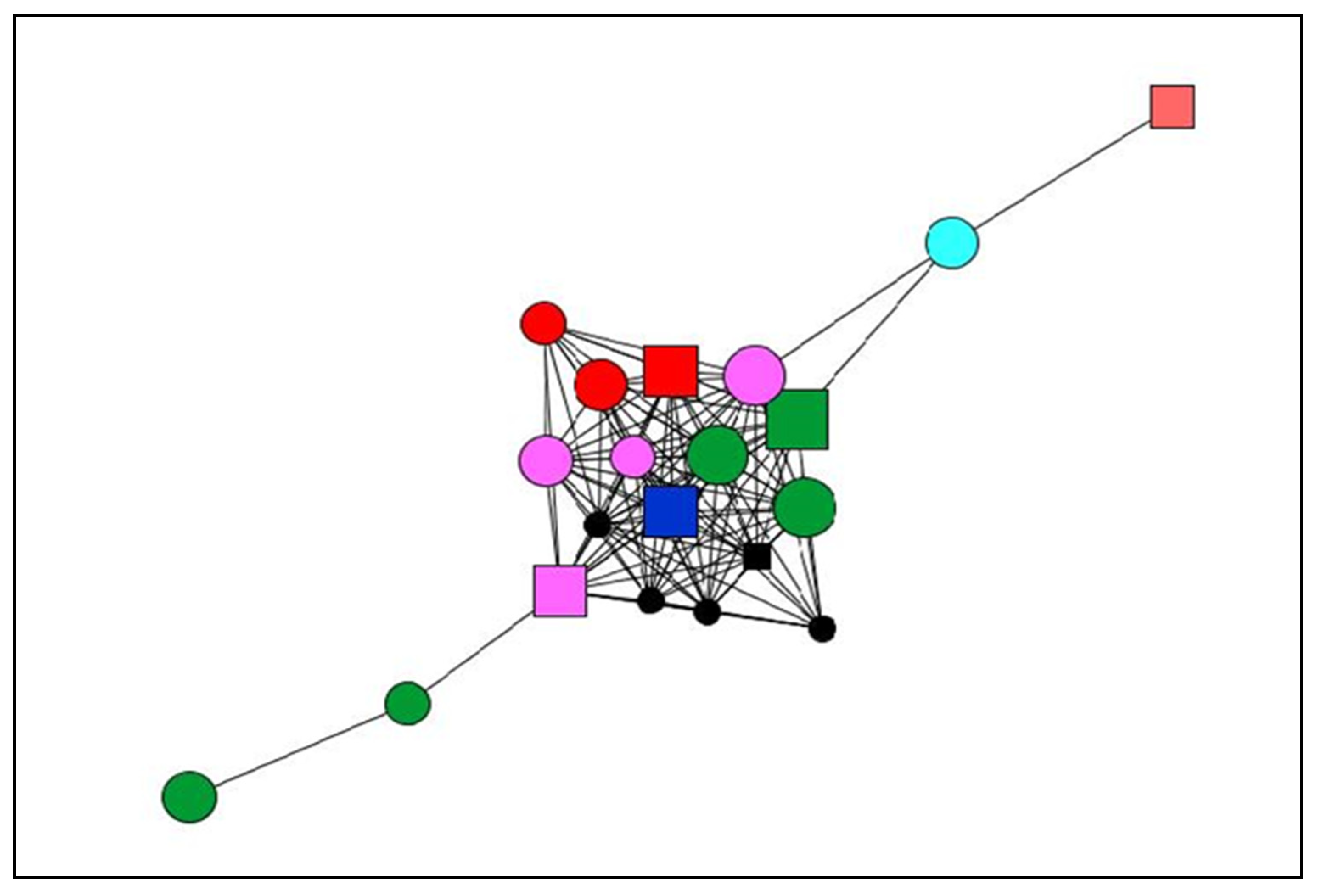
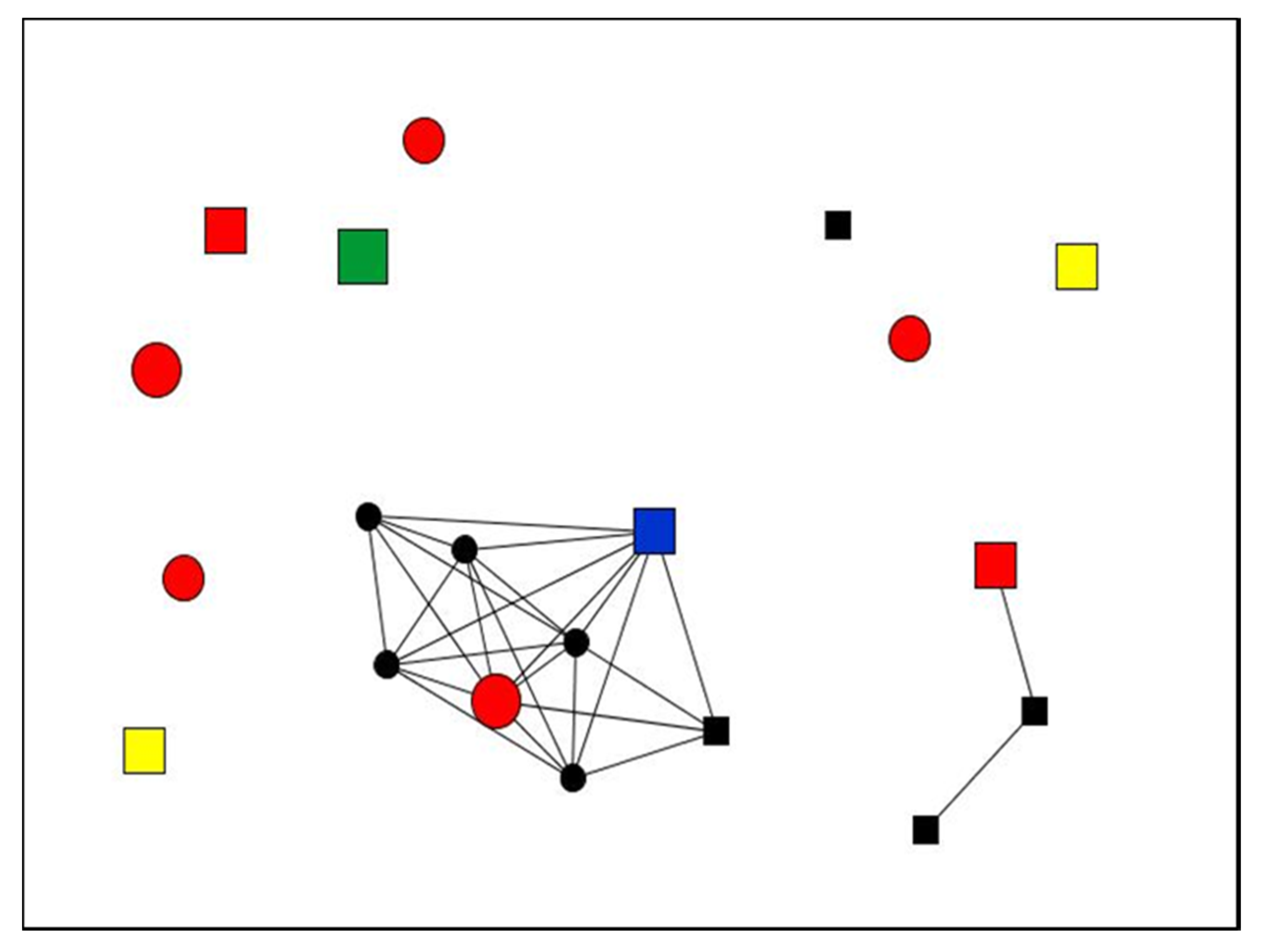
| Node Shape: Sex | Node Size: Satisfaction | Node Colour: Type of Social Support |
|---|---|---|
| Circle: Women Square: Men | Large: More satisfaction Small: Less satisfaction | Red: Emotional Dark blue: Instrumental Pink: Emotional and instrumental Yellow: Informational Green: All types Black: Non-providers Light blue: Emotional and informational Orange: Professional |
| Case 01 | Case 28 | ||
|---|---|---|---|
| Satisfaction (%) | Very satisfactory | 20 | 0 |
| Quite satisfactory | 35 | 15 | |
| Satisfactory | 20 | 40 | |
| Quite unsatisfactory | 0 | 0 | |
| Very unsatisfactory | 25 | 45 | |
| Structure | Density | 0.605 | 0.137 |
| Degree Centrality (mean) | 11.5 | 2.6 | |
| Betweenness Centrality (mean) | 5.7 | 0.25 | |
| Components | 1 | 11 | |
| Isolates | 0 | 9 | |
| Composition (%) | Sex of the alters Women (vs. men) | 70 | 50 |
| Strength of the tie Strong tie (vs. weak) | 80 | 90 | |
| Place of residence of alters Same locality as ego | 80 | 15 | |
| Reciprocity Yes | 45 | 90 | |
| Social support (%) | Type of support All three types Emotional and instrumental Non-providers | 25 20 25 | 5 0 45 |
| Variation of support Increases | 55 | 15 | |
| Frequency of support Daily 2 or 3 times per week | 25 10 | 5 0 | |
| Transmission channel Face-to-face Face-to-face and telephone | 65 10 | 45 10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Peña, R.; Molina, J.L.; Valero, O. Satisfaction with Social Support Received from Social Relationships in Cases of Chronic Pain: The Influence of Personal Network Characteristics in Terms of Structure, Composition and Functional Content. Int. J. Environ. Res. Public Health 2020, 17, 2706. https://doi.org/10.3390/ijerph17082706
Fernández-Peña R, Molina JL, Valero O. Satisfaction with Social Support Received from Social Relationships in Cases of Chronic Pain: The Influence of Personal Network Characteristics in Terms of Structure, Composition and Functional Content. International Journal of Environmental Research and Public Health. 2020; 17(8):2706. https://doi.org/10.3390/ijerph17082706
Chicago/Turabian StyleFernández-Peña, Rosario, José Luis Molina, and Oliver Valero. 2020. "Satisfaction with Social Support Received from Social Relationships in Cases of Chronic Pain: The Influence of Personal Network Characteristics in Terms of Structure, Composition and Functional Content" International Journal of Environmental Research and Public Health 17, no. 8: 2706. https://doi.org/10.3390/ijerph17082706