1. Introduction
Diarrhoeal disease continues to be a leading cause of mortality and morbidity in low and middle income countries, with 62.2% of diarrhoeal disease deaths in children under five attributed to poor water, sanitation and hygiene (WASH) and the associated consumption of contaminated foods in household settings [
1,
2,
3]. A range of recent studies have examined our current understanding and the efficacy of control measures taken to reduce exposure to enteric pathogens, including attempts to introduce multiple barriers to exposure pathways: enclosed sanitation, household water treatment, hand washing with soap, clean play spaces, domestic animal control and hygiene of complementary foods [
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18].
These multiple environmental pathways of transmission in low income countries make it difficult to attribute disease to a specific intervention, leading to calls for interventions that target the reduction of faecal contamination across the domestic environment, and develop a more appropriate package of effective WASH interventions [
8,
19,
20,
21,
22]. Despite the clear need for reducing faecal-oral contact, less than 5% of the population of Sub-Saharan Africa have access to improved water, sanitation and hygiene as described by the Sustainable Development Goal indicators [
23]. These complex and detrimental problems need a more integrated approach taking into consideration both widespread exposure to faecal contamination [
21,
24,
25], and the social, technological and economic influences that promote participation in and the uptake of sustained behavioural changes related to WASH at the household level [
8,
26,
27,
28,
29,
30]. The use of over-simplified interventions that have historically ignored these complexities is one potential reason why progress has been slow.
The Hygienic Family (
Banja la Ukhondo) intervention was based on formative research that found that children under the age of two were being exposed to multiple sources of faecal contamination within their domestic environments, particularly through complementary feeding at shared family meals, household drinking water, and exposure to environmental faeces [
31,
32,
33]. However, as previous studies addressing food hygiene in low income settings measured success based on behavioural change, structural changes or the microbiological quality of food and water [
5,
9,
10], our study was designed to measure the relative impact of the hygiene of complementary foods on diarrhoeal disease as a primary outcome, and the impact of a food hygiene intervention (food hygiene + handwashing) relative to a food hygiene and WASH intervention (food hygiene + handwashing + faeces management + water management) [
31].
2. Materials and Methods
2.1. Background and Study Design
As described previously [
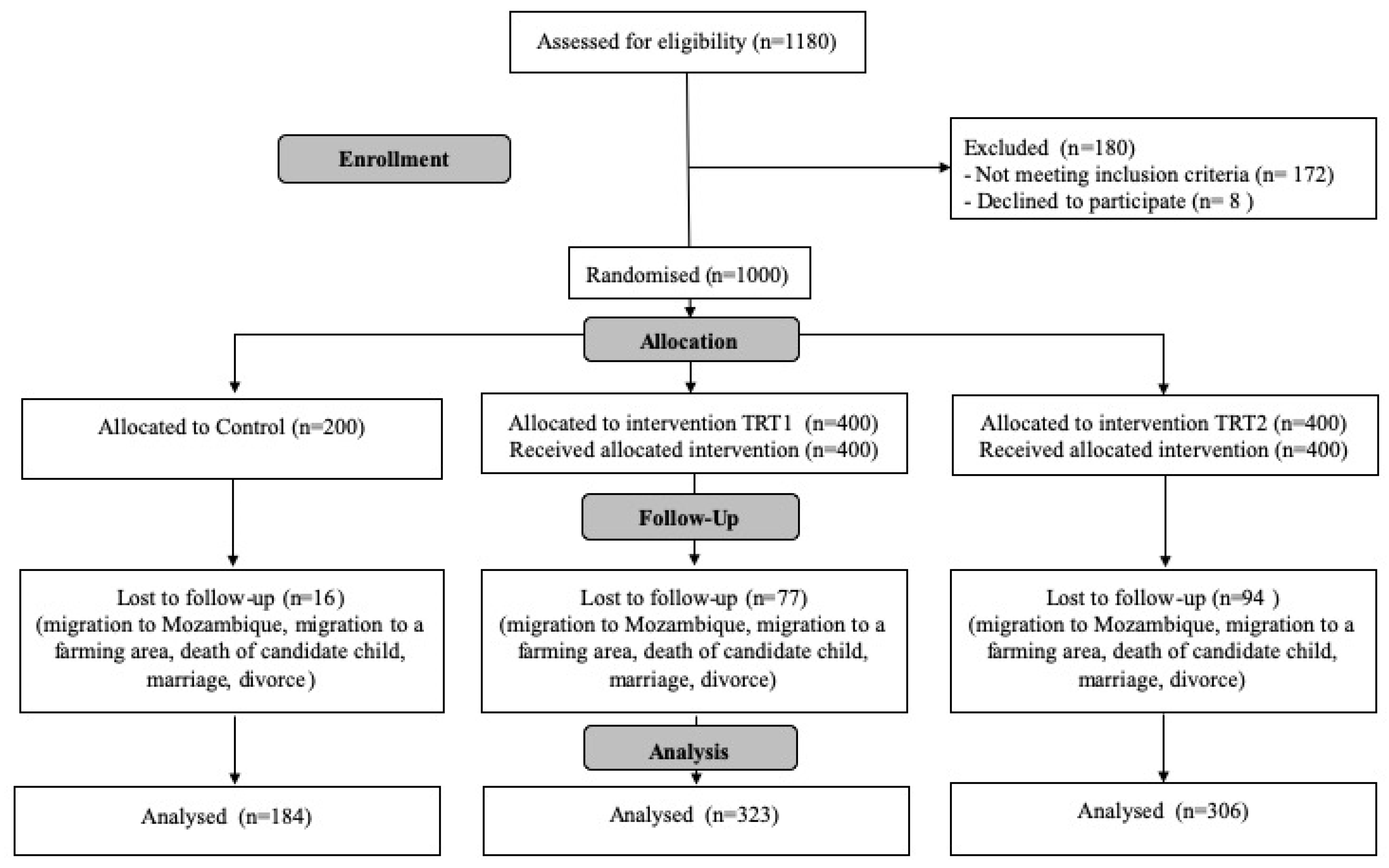
31], the study was a randomised before and after trial, with a control and two treatment arms, assessing the relative impact of the hygiene of complementary foods on the prevalence of diarrhoeal disease in children under five years old. For the programme, implemented from February–November 2018 in the rural District of Chikwawa in Southern Malawi, we recruited 1000 households in total. The two treatment arms were designed based on formative research: (1) a food hygiene intervention only (
n = 400), and (2) an integrated WASH and food hygiene intervention (
n = 400) [
31], with a control group in which no intervention took place (
n = 200). Although diarrhoeal disease was the primary outcome, respiratory infections were also monitored as indicators of improved WASH and food hygiene practices. End line data were collected in December 2018.
2.2. Study Area and Participant Selection
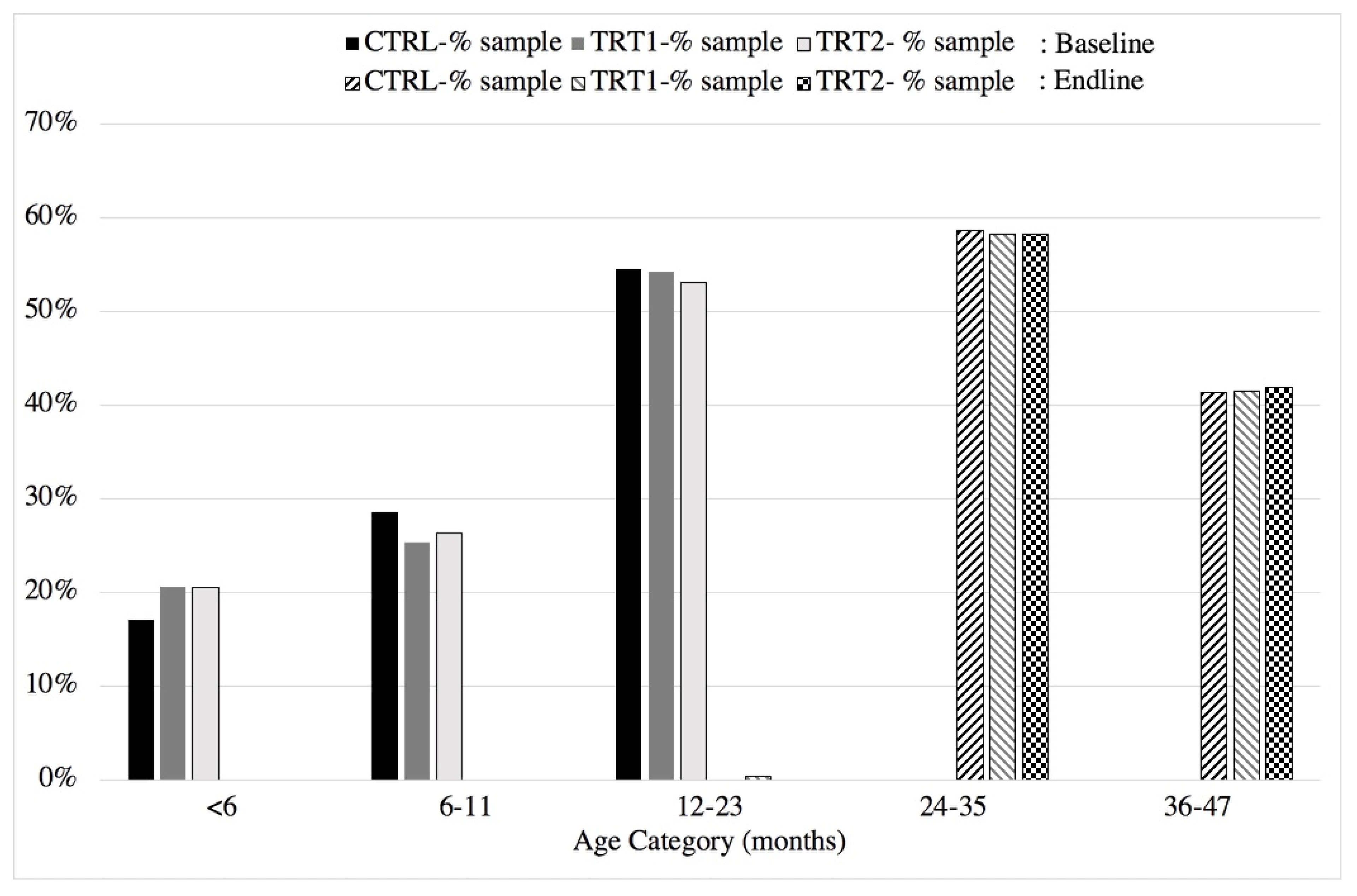
Malawi is divided into 28 Districts, which are subdivided into Traditional Authorities (TAs). Each TA contains villages, which are administered by chiefs and/or village heads. There are 12 Traditional Authorities (TAs) within Chikwawa district. This study was based in four different TAs: one in Treatment 1, two in Treatment 2, and one in the control. Treatment 2 included two TAs as there were insufficient eligible participants in the planned TA. Baseline data reported elsewhere showed homogeneity across all study groups in terms of household demographics, socio-economic status and hygiene related proxies [
31]. All study sites were selected in collaboration with the District Coordinating Team (government intersectoral team) and had all been declared open defaecation free by the Government of Malawi.
All recruited households had a functioning latrine and resided within 500 m of a functioning borehole, to ensure that there were no significant variations in access to water or sanitation infrastructure. Eligible households had a child aged between 4 and 90 weeks at enrolment (March–April 2017) to ensure that children were not neonates and that all children were under 60 months old at the end of intervention period (November 2018). The age of children was verified through birth and/or immunisation records supplied by the caregiver. All children in the target age range from eligible households were recruited at baseline; however, only one child per household was recruited. Physical recruitment was conducted by trained research assistants with the approval and support of community health workers (Health Surveillance Assistants (HSAs), traditional leaders (village chiefs) and community coordinators (female community members employed by the study). Morse, et al. reported the sample size calculations for and population demographics of the study sample [
31].
Households were allocated to clusters (treatment areas n = 20; control area n = 10) of between 15 to 25 caregivers for the purpose of the intervention delivery. Due to the close proximity of these clusters to one another, and therefore the risk of spillover effects, the study was randomized by TA. Each TA was provided with a dedicated treatment arm coordinator to oversee the intervention delivery and data collection.
Participants were advised that they were taking part in a study focused on child caregiving practices during consent, to minimise the reflexivity and reporting bias of health outcomes.
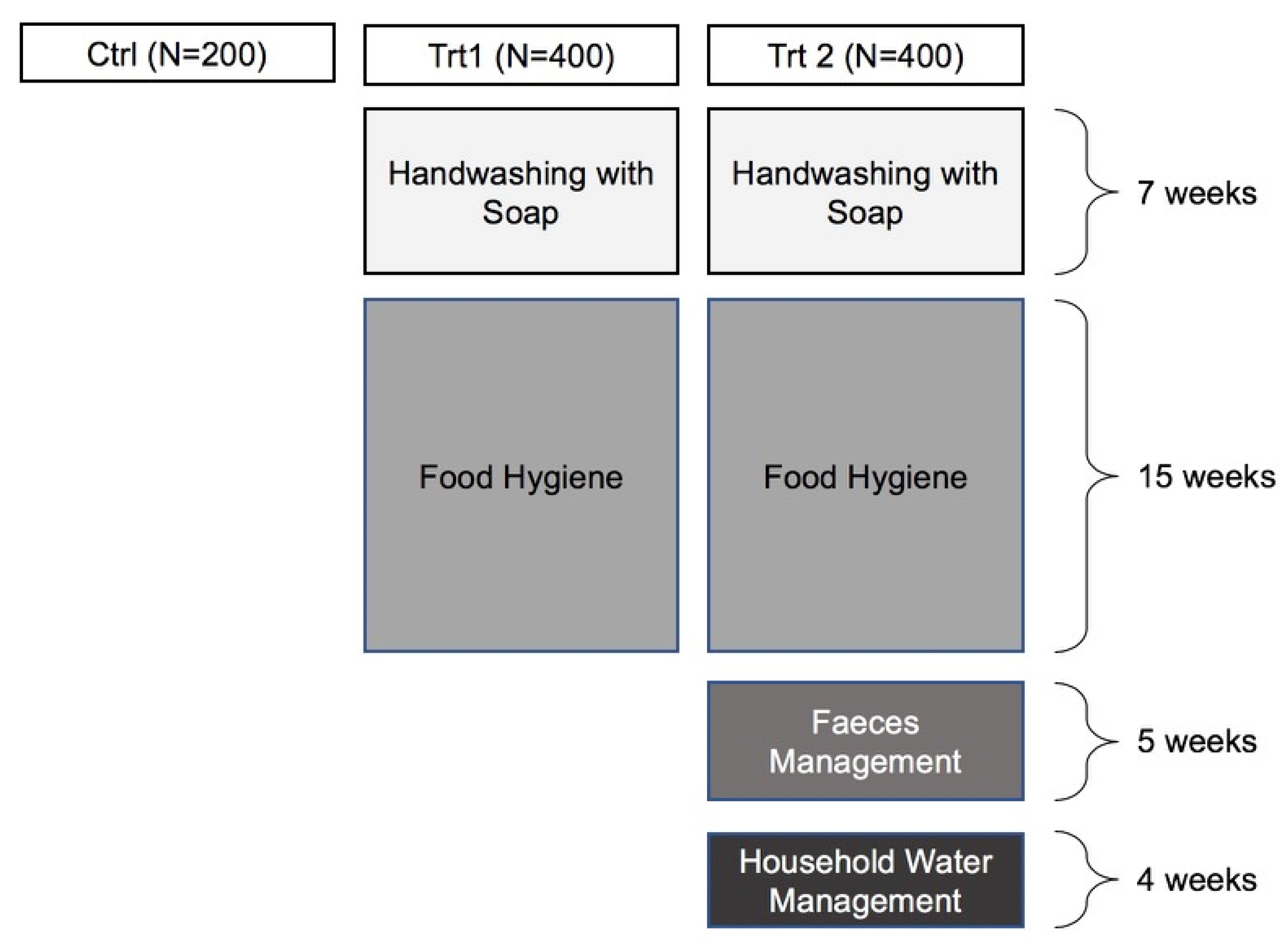
2.3. Intervention
Based on the findings of the formative and baseline data, and using a behaviour-centred approach, the 31-week intervention included four critical areas as outlined in
Figure 1 and described elsewhere [
31].
The intervention was designed in modules (
n = 4) to be delivered through community coordinators with the support of government HSAs, and oversight from study coordinators, to determine if the content and approach were appropriate for scaling up within existing structures. The content was conveyed through community-level open days at the beginning and end of the trial (
n = 2). Additional content was delivered through cluster meetings (up to 25 caregivers per group) (
n = 17) and household visits (one-to-one meetings) (
n = 14), which took place on alternating weeks. Cluster meetings included community coordinator-led discussions, practical exercises, demonstrations, games and celebrations of success to promote behavioural change and build supportive networks and social capital within the group [
31]. Household visits allowed community coordinators to assess progress, helped to put lessons into action, and provided support for any challenges that the households might have been facing. The number of cluster meetings and household visits varied depending on the material included in each topic.
Both community coordinators and health workers were supported and supervised by treatment arm coordinators to ensure the integrity and fidelity of the content delivered. Each module of the intervention was preceded by a one-week course of training for the community coordinators and HSAs. Completion of the module was also followed up with a review exercise to evaluate the successes and challenges encountered, and outline proposed changes in the content or delivery mechanisms.
2.4. Data Collection
Two health outcomes were measured in target children:
Primary health outcome—diarrhoeal disease, defined by WHO as the passage of three or more loose or liquid stools per day [
34].
Secondary health outcome—acute respiratory infections, defined as children having a fever plus either a cough or nasal congestion, or a fever plus breathing difficulty [
35].
All health outcomes were measured in two ways:
2.5. Data Analysis
The use of two treatment arms allowed us to measure:
The impact of each intervention on the incidence of diarrhoeal disease.
The impact of each intervention relative to the control group.
The impact of the food hygiene intervention relative to the WASH + food hygiene intervention.
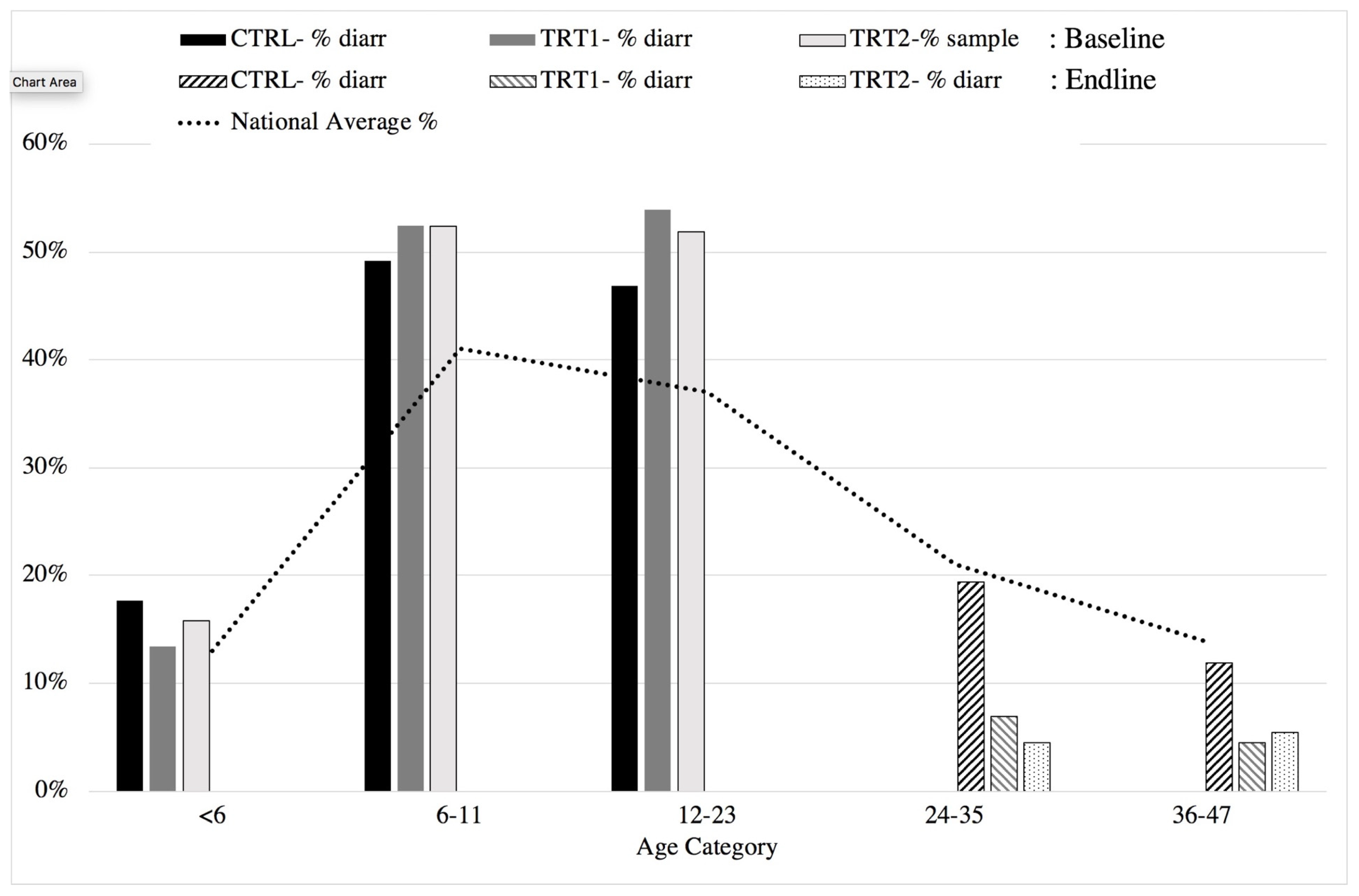
The primary variable of interest was the occurrence of diarrhoea within the past 2 weeks as reported by the primary caregiver, measured as a binary outcome. The impact of the interventions was analysed using a difference-in-differences approach, i.e., the prevalence of diarrhoea in the treatment areas was measured between baseline and the follow-up surveys and compared to that at the same time points in the control areas (n = 1000). Attendance at cluster meetings (individual level), cluster attendance score (cluster level), socio-economic characteristics (individual level), and household hygiene improvements (e.g., installation of a dish rack) (individual level), were included as covariates in the model. The incidence of secondary outcomes of acute respiratory infection was likewise analysed.
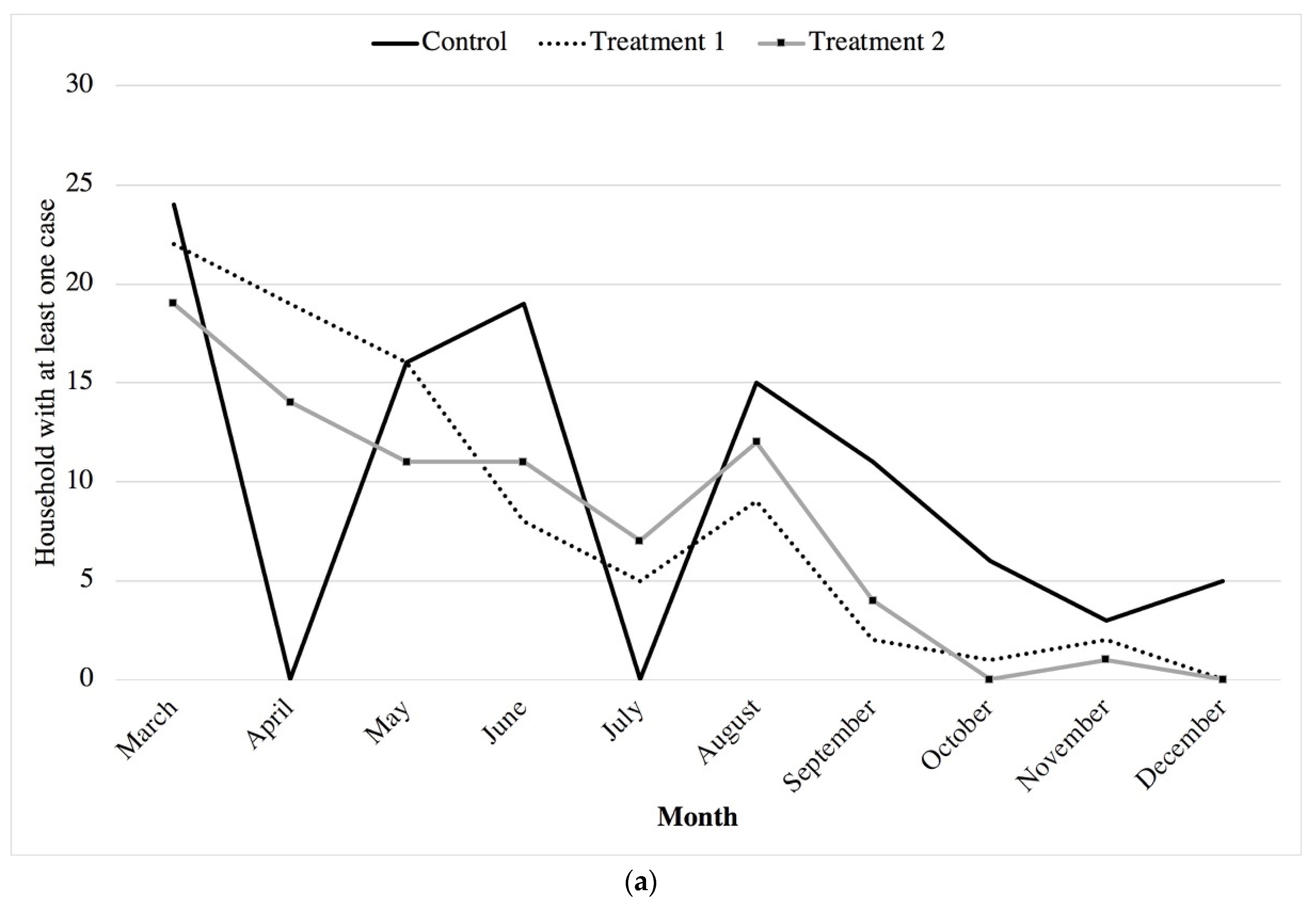
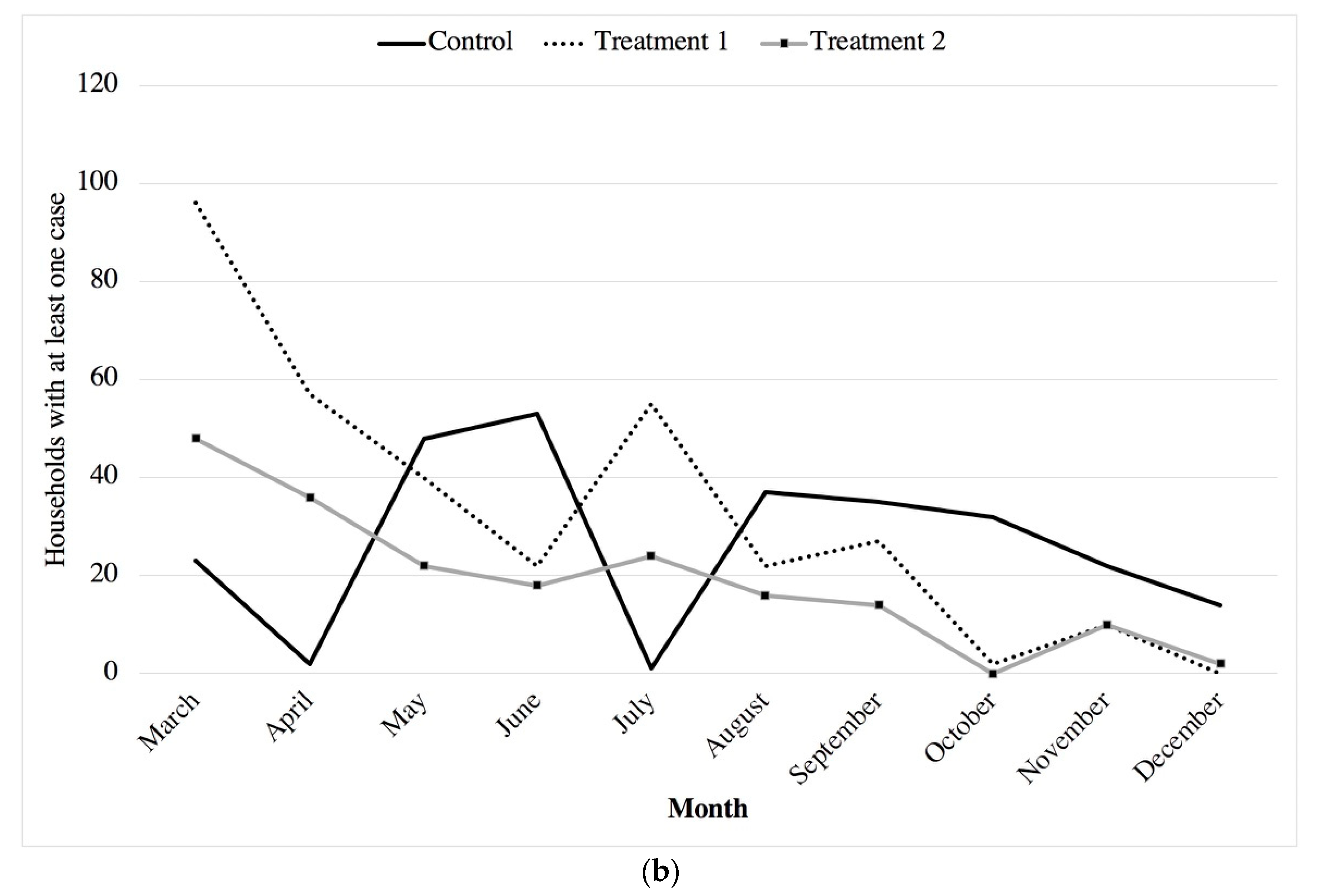
Daily diarrhoea and respiratory infection values (continuous data) were collected as a way of monitoring temporal changes that may have resulted due to other interventions, environmental changes, seasonality, or other unknown factors.
In the treatment areas, the attendance of caregivers at cluster meetings was measured using a register maintained by the community coordinators and checked by the treatment arm coordinators. Household visits were measured through the submission of completed household checklists completed by the community coordinators at each household visit and checked by the treatment arm coordinators. All attendance and visit records were consolidated by the treatment arm coordinators and submitted as weekly reports.
Data were cleaned and analysed using Stata version 13.1 (College Station, TX, USA).
2.6. Ethics
The study protocol was approved by the University of Malawi’s College of Medicine Research Ethics Committee. Permission was obtained from the local authorities, those are, the Chikwawa District Council, the Chikwawa District Health Office, and the traditional chiefs. The participants were advised that they had the freedom to refuse participation or withdraw from the study at any time. Participants’ written informed consent was obtained before inclusion in the study. Participants were provided with a unique identifying number, and data were anonymized during data analysis. Data were accessed only by the authors. The study was registered with the Pan African Clinical Trials Registry (PACTR201703002084166).
4. Discussion
This before and after trial with a control in rural Malawi measured the relative impact of a multi-faceted hygiene intervention on the reduction of diarrhoeal disease in an under five population. Self-reported results indicated a significant reduction in diarrhoeal disease associated with improved hand washing with soap at critical times and food hygiene practices. Those households that also improved faeces and water management additionally showed a significant reduction in acute respiratory infections. We did not find any significant explanatory variables for the reduction in illness in the treatment arms, indicating that the gains were likely to be from marginal effects across multiple sources rather than from one over-riding single behaviour. This finding is in line with the outcomes in the recent body of evidence from a range of WASH trials, which have highlighted the need to tackle multiple routes of pathogen exposure and take a new approach to how these are addressed [
8,
19]. Although there may be concerns related to self-reporting illness, our study relied on both daily diaries and two week recall at baseline and end line. The data sources show similar reductions in disease prevalence across the study period, thereby supporting our reported findings.
Minimal relative reductions in diarrhoeal disease between Treatments 1 and 2 infer a significant role played by food hygiene practices and associated hand washing with soap at critical times. The role of food in diarrhoeal disease transmission has been long recognised [
37,
38,
39,
40,
41], and a recent WHO report attributed 70% of the burden of foodborne disease to low and middle income countries, with 40% of this burden affecting children under the age of five [
2]. Our findings support the growing body of evidence that improving food hygiene practices can play a significant role in reducing diarrhoeal disease in under five populations. We also recognise the role that effective hand washing with soap may be playing in this reported reduction in diarrhoea, and acknowledge that even increased hand washing with water alone may be contributing to these improved health outcomes [
18,
42,
43,
44].
Similar reductions in diarrhoeal disease between Treatments 1 and 2 may also have been affected by the content of the WASH based modules: our study did not promote or subsidise point of use water treatment, which may have limited the impact of the water management improvements due to the continued post collection contamination of drinking water with
E. coli. In addition, it may be indicative of the wide level of faecal contamination already present in the environment [
13,
14], which existed before the intervention supported the management of animal and child faeces from the household yard.
In terms of reductions in respiratory infections, results infer the need for a wider approach to reducing environmental exposure to faecal matter. Our observed reduction associated with improved WASH practices is in agreement with previous reports of improved hygiene having a secondary impact on acute respiratory infections [
35,
45].
Our behaviour-centred intervention used the Risks, Attitudes, Norms, Abilities and Self Regulation (RANAS) approach, [
46] and the embedded recommended behavioural change techniques [
31], within existing community structures to provide both familiarity and innovation in how messages were delivered. Although the contact time was intensive, the mode of delivery used reflected that of existing community-based women’s and caregiver groups [
47]. Our formative research outlined the challenges this approach may have regarding caregiver availability, given that the majority of households were subsistence farmers and, therefore, self-employed [
31]. As such, the intervention content was designed in such a way as to provide repetition and ensure that missed cluster meetings or household visits would not impede long-term progress. The achievement of health outcome improvements in this study appears to show that this intensive and repetitive approach warrants further use, as attendance at neither cluster meetings nor household visits ever reached 100%. However, despite this, hygiene proxies and behaviours [
48] were seen to significantly improve in the treatment versus control arms. Any intervention must cognisant of the context in which it is set and the other household commitments of caregivers and targeted populations, which may impact their ability to participate in community or household meetings. Therefore, by using group and one-to-one household meetings to provide the same message through a range of behavioural change techniques and concurrently build trust and social capital [
49], such an approach could have effective implications for wider community hygiene improvements. This finding agrees with recent reviews which reported the benefits of a high degree of contact time to achieve the anticipated behavioural change, particularly at the household level [
8,
30].
The use of community-based coordinators and community health workers (HSAs) was tested in this intervention to determine if the low education level of coordinators could be overcome with effective training and supervision. Although we do acknowledge a degree of heterogeneity in the delivery and participation with the intervention content, the successful health outcomes of the intervention infer that the use of community-based coordinators, similar to that of care group coordinators (Scaling Up Nutrition) or maternal health women’s group coordinators [
47] could be an effective route for implementation. The use of local and familiar facilitators can ensure an ongoing empathy with caregivers, as they have a working knowledge and personal experience of caregiver capabilities, pressures and stressors, all of which can affect a caregiver’s ability to make sustained structural and behavioural changes [
50]. This is particularly important when considering the poorest populations and lowest levels of caregiver education in high risk populations in low income settings, where access to health care providers is limited, and exposure to faecal pathogens is high [
1,
51,
52].
The modules developed through the Hygienic Family intervention have been designed in such a way as to support the integration of the content with other programmes, and to take into consideration the limitations of facilitators and irregular attendance from caregivers. There may be concerns that the integration of too many health and hygiene messages within specific caregiver groups could be overwhelming for both facilitators and participants. However, the call for an improved integration of services, as well as evidence from recent studies [
53], demonstrates that such integration is an effective route for improving hygiene practices in the lowest quintile of caregivers by education.
The study limitations must be taken into consideration in the interpretation of these results. The intervention was limited to a nine-month period but likely would have been more effective over a full twelve months. Despite this, the results reflect a range of seasons within Malawi, including the initiation of the rainy season (November 2018), which sees the peak prevalence of diarrhoeal disease in the under-five population. End line data were also collected soon after (December 2018) the completion of the intervention (November 2018), which may have led to reflexivity in the responses. As outlined above, we believe that we have compensated for this with the use of two methods for reporting illness. We also acknowledge that our study did not measure all variables that may affect the prevalence of diarrhoea or respiratory infections, such as low birth weight status, malnutrition, HIV status, or the presence of other diseases such as measles, malaria, etc.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





