Diarrhea in Under Five Year-old Children in Nepal: A Spatiotemporal Analysis Based on Demographic and Health Survey Data


Abstract
:1. Introduction
2. Materials and Methods
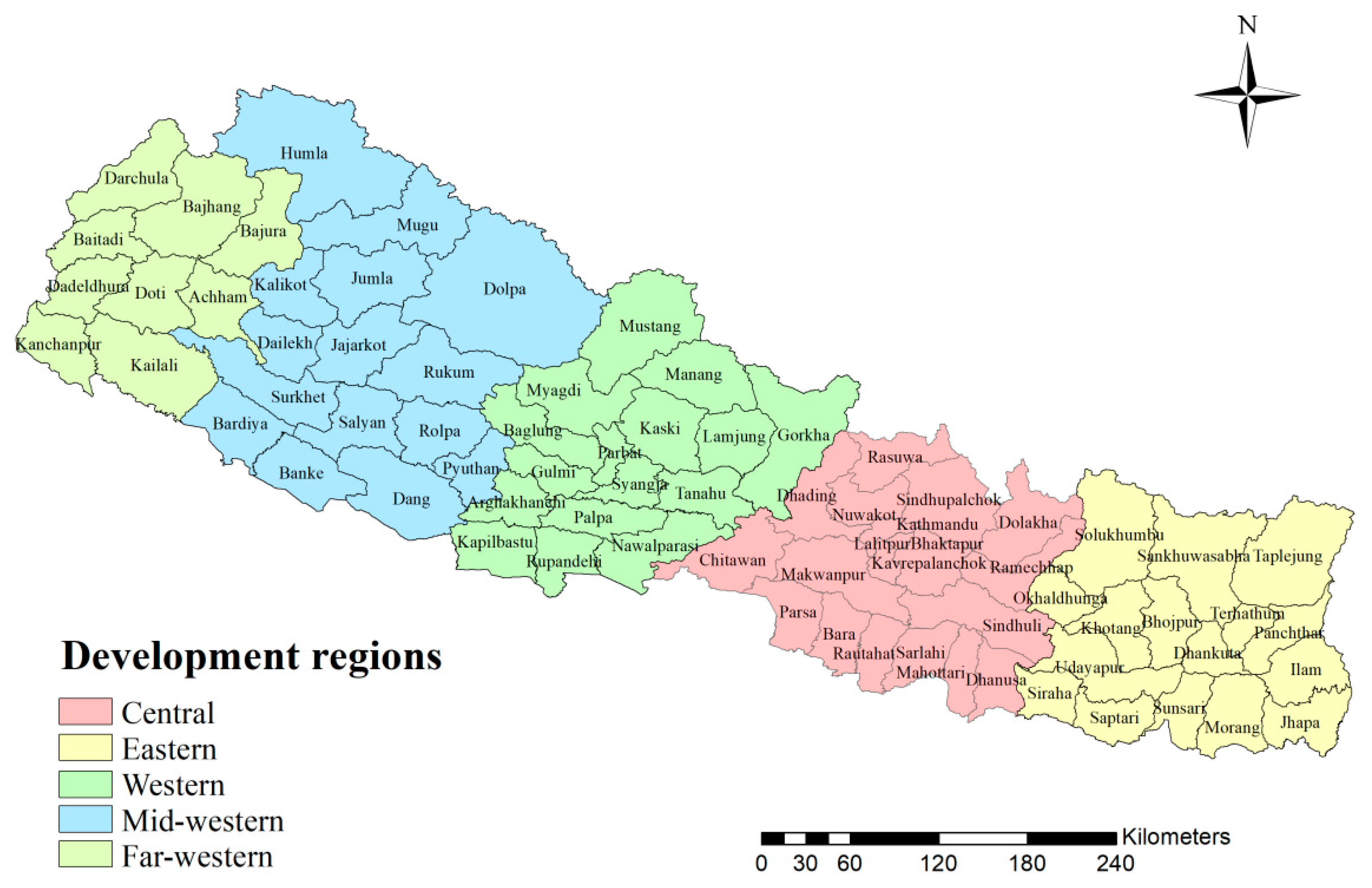
2.1. Study Area
2.2. The Data
2.3. Statistical Analysis
3. Results
3.1. Summary of NDHS on Children Diarrhea
3.2. Single-Factor Analysis
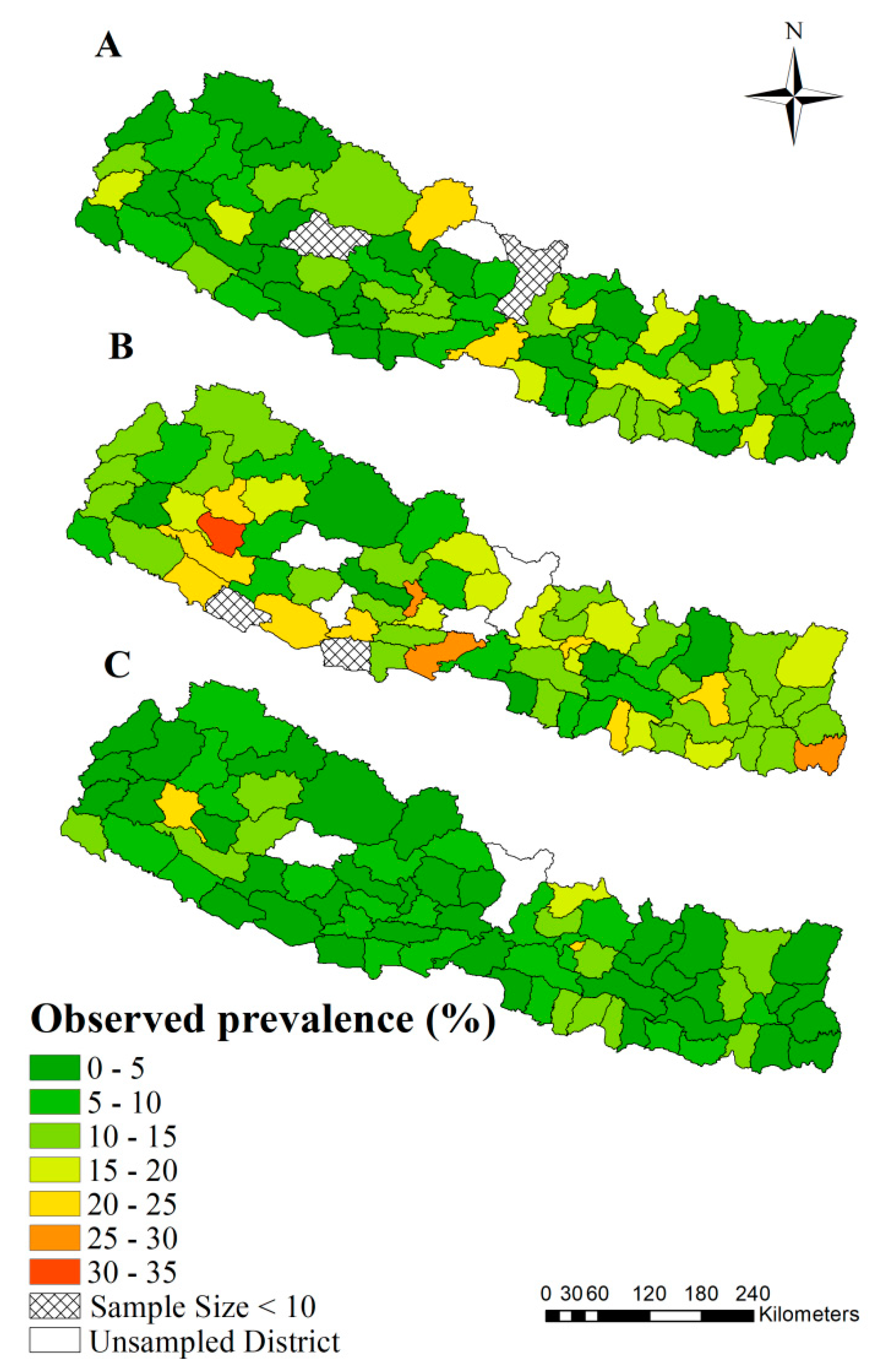
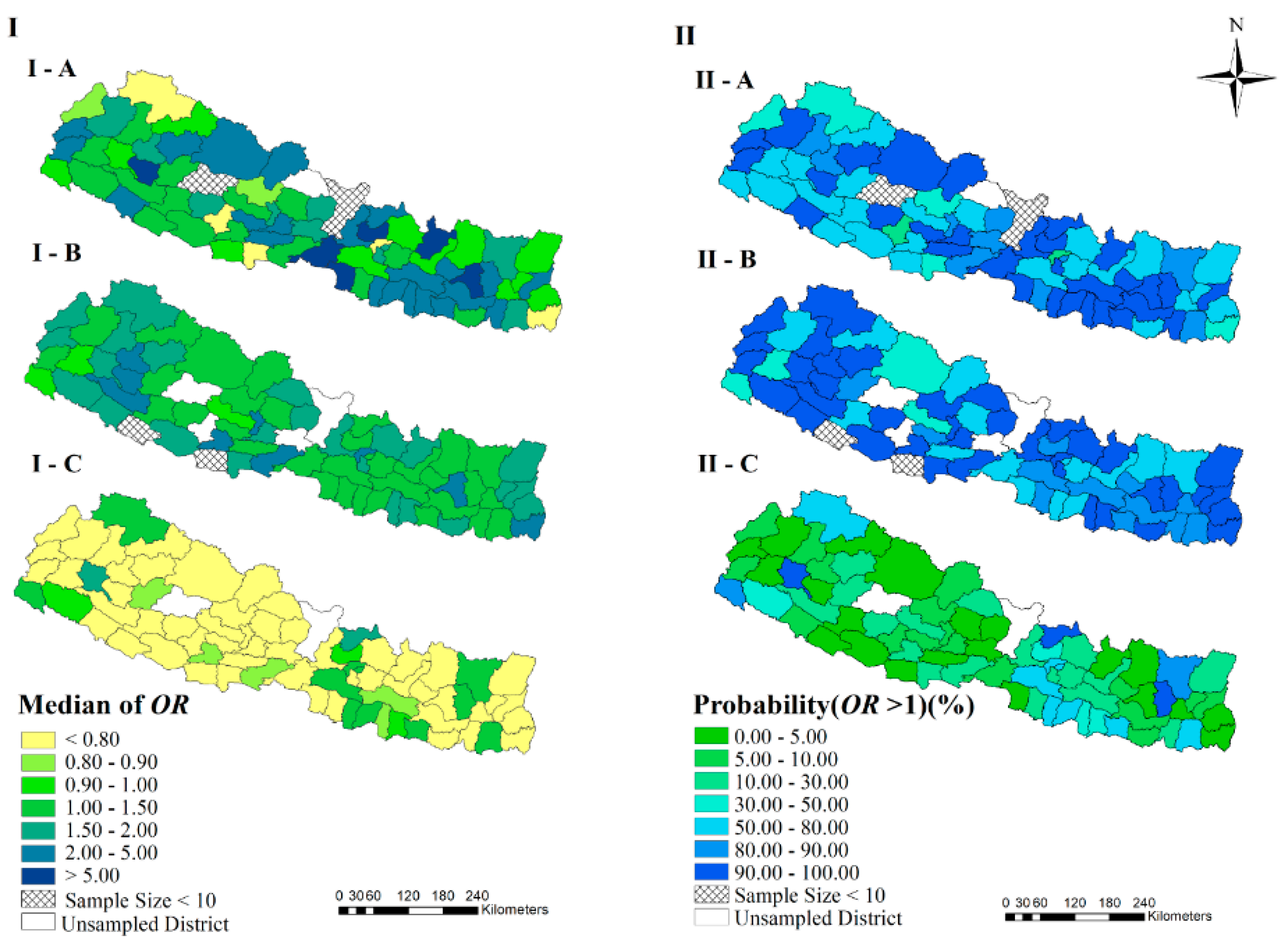
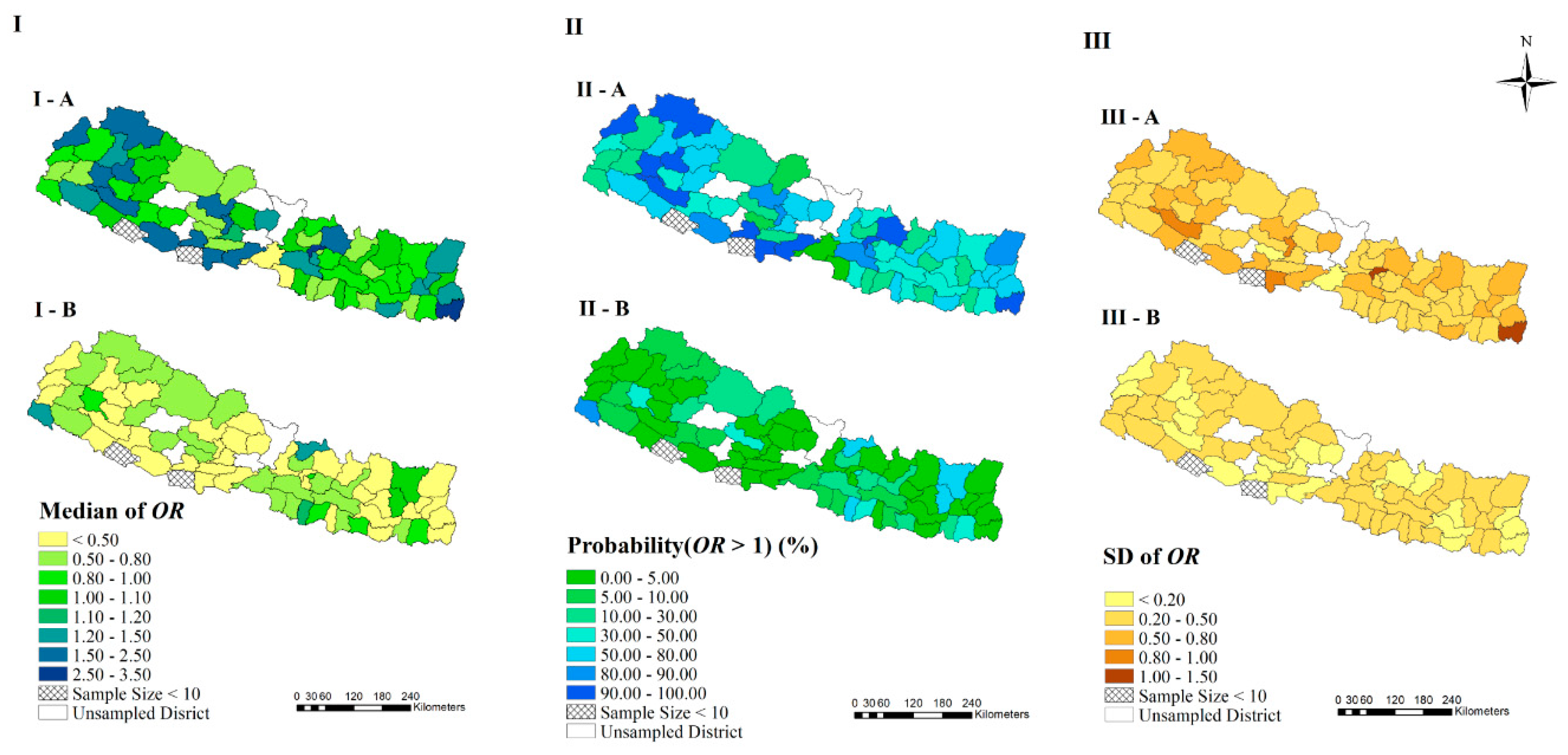
3.3. Spatial-Temporal Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- UNICEF; WWBU. Levels and Trends in Child Mortality Report 2019. Available online: https://www.unicef.org/reports/levels-and-trends-child-mortality-report-2019 (accessed on 15 October 2019).
- UN. News on Millennium Development Goals. Available online: https://www.un.org/millenniumgoals (accessed on 8 August 2019).
- UN. About the Sustainable Development Goals. Available online: https://www.un.org/ sustainabledevelopment/sustainable-development-goals/ (accessed on 8 August 2019).
- Kotloff, K.L.; Platts-Mills, J.A.; Nasrin, D.; Roose, A.; Blackwelder, W.C.; Levine, M.M. Global burden of diarrheal diseases among children in developing countries: Incidence, etiology, and insights from new molecular diagnostic techniques. Vaccine 2017, 35, 6783–6789. [Google Scholar] [CrossRef] [PubMed]
- Alebel, A.; Tesema, C.; Temesgen, B.; Gebrie, A.; Petrucka, P.; Kibret, G.D. Prevalence and determinants of diarrhea among under-five children in Ethiopia: A systematic review and meta-analysis. PLoS ONE 2018, 13, e199684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Causes of Child Mortality. Available online: https://www.who.int/gho/child_health/mortality/ causes/en/ (accessed on 9 August 2019).
- Walker, C.L.F.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, K.L.; Campbell, H.; Black, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef]
- Victora, C.G.P.D.; Requejo, J.H.P.; Barros, A.J.D.P.; Berman, P.P.; Bhutta, Z.P.; Boerma, T.M.; Chopra, M.M.; de Francisco, A.M.; Daelmans, B.M.; Hazel, E.M.; et al. Countdown to 2015: A decade of tracking progress for maternal, newborn, and child survival. Lancet 2015, 387, 2049–2059. [Google Scholar] [CrossRef] [Green Version]
- Nepal Statistics. Available online: https://www.who.int/countries/npl/en/ (accessed on 15 August 2019).
- United States of America Statistics Not the Publisher. Available online: https://www.who.int/countries/usa/en/ (accessed on 15 August 2019).
- WHO. Proportion of Deaths by Country. Diarrhoeal Diseases. Available online: http://apps.who.int/ gho/data/view.main.ghe3002015-CH3?lang=en (accessed on 15 August 2019).
- Akram, R.; Sultana, M.; Ali, N.; Sheikh, N.; Sarker, A.R. Prevalence and Determinants of Stunting Among Preschool Children and Its Urban-Rural Disparities in Bangladesh. Food Nutr. Bull. 2018, 39, 521–535. [Google Scholar] [CrossRef]
- Guerrant, R.L.; Schorling, J.B.; McAuliffe, J.F.; de Souza, M.A. Diarrhea as a cause and an effect of malnutrition: Diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration. Am. J. Trop. Med. Hyg. 1992, 47, 28–35. [Google Scholar] [CrossRef]
- Ministry of Health and Population Nepal, NEII. Nepal Demographic Health Survey 2016; Ministry of Health and Population Nepal: Kathmandu, Nepal, 2016.
- Publisher. Number of Deaths by Country Diarrhoeal Diseases. Available online: http://apps.who.int/gho/data/view.main.ghe1002015-CH3?lang=en (accessed on 10 February 2020).
- Acharya, D.; Singh, J.K.; Adhikari, M.; Gautam, S.; Pandey, P.; Dayal, V. Association of water handling and child feeding practice with childhood diarrhoea in rural community of Southern Nepal. J. Infect Public Health 2018, 11, 69–74. [Google Scholar] [CrossRef]
- Hasan, M.M.; Richardson, A. How sustainable household environment and knowledge of healthy practices relate to childhood morbidity in South Asia: Analysis of survey data from Bangladesh, Nepal and Pakistan. BMJ Open 2017, 7, e15019. [Google Scholar] [CrossRef] [Green Version]
- Pruss-Ustun, A.; Bartram, J.; Clasen, T.; Colford, J.J.; Cumming, O.; Curtis, V.; Bonjour, S.; Dangour, A.D.; De France, J.; Fewtrell, L.; et al. Burden of disease from inadequate water, sanitation and hygiene in low- and middle-income settings: A retrospective analysis of data from 145 countries. Trop. Med. Int. Health 2014, 19, 894–905. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Riumallo-Herl, C.; Salomon, J.A.; Resch, S.C.; Brenzel, L.; Verguet, S. Estimating the distribution of morbidity and mortality of childhood diarrhea, measles, and pneumonia by wealth group in low- and middle-income countries. BMC Med. 2018, 16, 102. [Google Scholar] [CrossRef]
- Strand, T.A.; Sharma, P.R.; Gjessing, H.K.; Ulak, M.; Chandyo, R.K.; Adhikari, R.K.; Sommerfelt, H. Risk factors for extended duration of acute diarrhea in young children. PLoS ONE 2012, 7, e36436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budhathoki, S.S.; Bhattachan, M.; Yadav, A.K.; Upadhyaya, P.; Pokharel, P.K. Eco-social and behavioural determinants of diarrhoea in under-five children of Nepal: A framework analysis of the existing literature. Trop. Med. Int. Health 2016, 44, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, D.L.; Roose, A.; Roh, M.; Kotloff, K.L.; Proctor, J.L. The seasonality of diarrheal pathogens: A retrospective study of seven sites over three years. PLoS Negl. Trop. Dis. 2019, 13, e7211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, T.; Kapwata, T.; Behera, S.K.; Minakawa, N.; Hashizume, M.; Sweijd, N.; Mathee, A.; Wright, C.Y. Climatic Factors in Relation to Diarrhoea Hospital Admissions in Rural Limpopo, South Africa. Atmosphere 2019, 10, 522. [Google Scholar] [CrossRef] [Green Version]
- Azage, M.; Kumie, A.; Worku, A.C.; Bagtzoglou, A.; Anagnostou, E. Effect of climatic variability on childhood diarrhea and its high-risk periods in northwestern parts of Ethiopia. PLoS ONE 2017, 12, e186933. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Carlin, B.P.; Gelfand, A.E. Hierarchical Modeling and Analysis for Spatial Data, 2nd ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2014. [Google Scholar]
- Lawson, A.B. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology; Chapman & Hall/CRC: London, UK, 2013. [Google Scholar]
- Osei, F.B.; Stein, A. Bayesian Random Effect Modeling for analyzing spatial clustering of differential time trends of diarrhea incidences. Sci. Rep. 2019, 9, 13217. [Google Scholar] [CrossRef]
- Osei, F.B.; Stein, A. Diarrhea Morbidities in Small Areas: Accounting for Non-Stationarity in Sociodemographic Impacts using Bayesian Spatially Varying Coefficient Modelling. Sci. Rep. 2017, 7, 9908–9915. [Google Scholar] [CrossRef]
- Anwar, M.Y.; Warren, J.L.; Pitzer, V.E. Diarrhea Patterns and Climate: A Spatiotemporal Bayesian Hierarchical Analysis of Diarrheal Disease in Afghanistan. Am. J. Trop. Med. Hyg. 2019, 101, 525–533. [Google Scholar] [CrossRef]
- WBG Nepal Income Level. Available online: https://data.worldbank.org/country/nepal?view=chart (accessed on 10 August 2019).
- Spatial Data Download Country: Nepal. Available online: https://www.diva-gis.org/gdata (accessed on 10 March 2019).
- DHS. The Demographic and Health Surveys (DHS) Program. Available online: https://dhsprogram.com/ (accessed on 18 August 2019).
- Ministry of Health and Population Nepal, NEII. Nepal Demographic Health Survey, 2006; Ministry of Health and Population Nepal: Kathmandu, Nepal, 2006.
- Ministry of Health and Population Nepal, NEII. Nepal Demographic Health Survey, 2011; Ministry of Health and Population Nepal: Kathmandu, Nepal, 2011.
- Shrestha, S.; Haramoto, E.; Malla, R.; Nishida, K. Risk of diarrhoea from shallow groundwater contaminated with enteropathogens in the Kathmandu Valley, Nepal. J. Water Health 2015, 13, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Climate of Nepal. Available online: http://www.anatravels.com/nepal-climate.php (accessed on 3 February 2020).
- Pfeiffer, D.; Robinson, T.P.; Stevenson, M.; Stevens, K.B.; Rogers, D.J.; Clements, A.C. Spatial Analysis in Epidemiology; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Moran, P.A.P. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Knorr-Held, L. Bayesian modelling of inseparable space-time variation in disease risk. Stat. Med. 2000, 19, 2555–2567. [Google Scholar] [CrossRef] [Green Version]
- Blangiardo, M.; Cameletti, M. Spatial and Spatio-Temporal Bayesian Models with R-INLA; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2015. [Google Scholar]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B-Stat. Methodol. 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Guide to DHS Statistics. Available online: https://www.dhsprogram.com/pubs/pdf/DHSG1/ Guide_to_DHS_Statistics_29Oct2012_DHSG1.pdf (accessed on 6 September 2019).
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.H.; Schmidt, W. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39 (Suppl. 1), i193–i205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takele, K.; Zewotir, T.; Ndanguza, D. Risk factors of morbidity among children under age five in Ethiopia. BMC Public Health 2019, 19, 942–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asfaha, K.F.; Tesfamichael, F.A.; Fisseha, G.K.; Misgina, K.H.; Weldu, M.G.; Welehaweria, N.B.; Gebregiorgis, Y.S. Determinants of childhood diarrhea in Medebay Zana District, Northwest Tigray, Ethiopia: A community based unmatched case-control study. BMC Pediatr. 2018, 18, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, D.; Dabas, A.; Anand, T.; Pinnamaneni, R. Maternal knowledge, attitude and practices during childhood diarrhoea. Trop. Doct. 2018, 48, 298–300. [Google Scholar] [CrossRef]
- Melo, M.C.; Taddei, J.A.; Diniz-Santos, D.R.; Vieira, C.; Carneiro, N.B.; Melo, R.F.; Silva, L.R. Incidence of diarrhea in children living in urban slums in Salvador, Brazil. Braz. J. Infect. Dis. 2008, 12, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Siziya, S.; Muula, A.S.; Rudatsikira, E. Correlates of diarrhoea among children below the age of 5 years in Sudan. Afr. Health Sci. 2013, 13, 376–383. [Google Scholar] [CrossRef] [Green Version]
- Ansari, S.; Sherchand, J.B.; Parajuli, K.; Mishra, S.K.; Dahal, R.K.; Shrestha, S.; Tandukar, S.; Pokhrel, B.M. Bacterial etiology of acute diarrhea in children under five years of age. J. Nepal Health Res. Counc. 2012, 10, 218–223. [Google Scholar]
- Anand, A.; Roy, N. Transitioning toward Sustainable Development Goals: The Role of Household Environment in Influencing Child Health in Sub-Saharan Africa and South Asia Using Recent Demographic Health Surveys. Front. Public Health 2016, 4, 87. [Google Scholar] [CrossRef] [Green Version]
- Melese, B.; Paulos, W.; Astawesegn, F.H.; Gelgelu, T.B. Prevalence of diarrheal diseases and associated factors among under-five children in Dale District, Sidama zone, Southern Ethiopia: A cross-sectional study. BMC Public Health 2019, 19, 1235. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.; Lee, J.; Seo, D.; Park, B.M.; Mansiangi, P.; Bernard, K.; Mulakub-Yazho, G.J.N.; Famasulu, H.M. Effects of improved sanitation on diarrheal reduction for children under five in Idiofa, DR Congo: A cluster randomized trial. Infect. Dis. Poverty 2017, 6, 112–137. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y.; Agestika, L.; Sintawardani, N.; Yamauchi, T. Risk Factors for Undernutrition and Diarrhea Prevalence in an Urban Slum in Indonesia: Focus on Water, Sanitation, and Hygiene. Am. J. Trop. Med. Hyg. 2019, 100, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aihara, Y.; Shrestha, S.; Kazama, F.; Nishida, K. Validation of household water insecurity scale in urban Nepal. Water Policy 2015, 17, 2015116. [Google Scholar] [CrossRef]
- Chou, W.; Wu, J.; Wang, Y.; Huang, H.; Sung, F.; Chuang, C. Modeling the impact of climate variability on diarrhea-associated diseases in Taiwan (1996–2007). Sci. Total Environ. 2010, 409, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Wangdi, K.; Clements, A.C. Spatial and temporal patterns of diarrhoea in Bhutan 2003–2013. BMC Infect. Dis. 2017, 17, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Hu, W.; Zhang, Y.; Wang, X.; Zhou, M.; Su, H.; Huang, C.; Tong, S.; Guo, Q. Exploration of diarrhoea seasonality and its drivers in China. Sci. Rep. 2015, 5, 8241. [Google Scholar] [CrossRef] [Green Version]
- UNDP. Nepal Human Development Report 2014. Available online: http://www.hdr.undp.org/ sites/default/files/nepal_nhdr_2014-final.pdf (accessed on 9 November 2019).
- WHO. Nepal—WHO Country Cooperation Strategy: 2018–2022. Available online: https://apps.who.int/ iris/handle/10665/272476 (accessed on 10 November 2019).
- MoHP. Nepal Health Sector Strategy. Available online: https://nepal.unfpa.org/en/publications/nepal-health-sector-strategy-2015-2020 (accessed on 10 November 2019).
- DoHS; MoHP. Annual Report of Department of Health Services 2072/73 (2015/2016). Available online: https://phpnepal.org.np/publication/current-issue/recently-released/136-annual-report-of-department-of-health-services-2072-73-2015-2016 (accessed on 13 November 2019).
- Ministry of Health and Population Nepal, NEII. Key Indicators of Nepal Demographic and Health Survey 2016. Available online: https://phpnepal.org.np/publication/current-issue/recently-released/120-key-indicators-of-nepal-demographic-and-health-survey-2016 (accessed on 9 September 2019).
- Aryal, K.K.; Joshi, H.D.; Dhimal, M.; Singh, S.P.; Dhakal, P.; Dhimal, B.; Bhusal, C.L. Environmental burden of diarrhoeal diseases due to unsafe water supply and poor sanitation coverage in Nepal. J. Nepal Health Res. Counc. 2012, 10, 125. [Google Scholar]
- Kafle, S.; Pradhan, B. Situation of Water, Sanitation and Hygiene and Diarrhoeal Diseases After Open Defecation Free Declaration. J. Nepal Health Res. Counc. 2018, 16, 160. [Google Scholar] [CrossRef]
- Ahs, J.W.; Tao, W.; Löfgren, J.; Forsberg, B.C. Diarrheal Diseases in Low-and Middle-Income Countries: Incidence, Prevention and Management. Open Infect. Dis. J. 2010, 4, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Clasen, T.; Schmidt, W.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. BMJ 2007, 334, 782–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of Nepal. Country Programme Action Plan 2018–2022. Available online: https://www.unicef.org/nepal/media/191/file/CPAP%202018-2022.pdf (accessed on 15 November 2019).
- Ministry of Education, Nepal. Nepal School Sector Development Plan 2016–2023. Available online: https://www.globalpartnership.org/content/nepal-school-sector-development-plan-2016-2023 (accessed on 16 November 2019).
- Målqvist, M.; Singh, C.; Kc, A.; Medicinska, F.; Medicinska, O.F.V.; Institutionen, F.K.O.B.; Internationell, M.O.B.I.; Uppsala, U. Care seeking for children with fever/cough or diarrhoea in Nepal: Equity trends over the last 15 years. Scand. J. Public Health 2017, 45, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gizaw, Z.; Woldu, W.; Bitew, B.D. Child feeding practices and diarrheal disease among children less than two years of age of the nomadic people in Hadaleala District, Afar Region, Northeast Ethiopia. Int. Breastfeed J. 2017, 12, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Ogbo, F.A.; Agho, K.; Ogeleka, P.; Woolfenden, S.; Page, A.; Eastwood, J.; Global Child Health Research Interest Group. Infant feeding practices and diarrhoea in sub-Saharan African countries with high diarrhoea mortality. PLoS ONE 2017, 12, e171792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, B.; Saha, D.; Sanogo, D.; Das, S.K.; Omore, R.; Farag, T.H.; Nasrin, D.; Li, S.; Panchalingam, S.; Levine, M.M.; et al. Association Between Shigella Infection and Diarrhea Varies Based on Location and Age of Children. Am. J. Trop. Med. Hyg. 2015, 93, 918–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombara, D.V.; Faruque, A.S.G.; Cowgill, K.D.; Mayer, J.D. Risk factors for diarrhea hospitalization in Bangladesh, 2000–2008: A case-case study of cholera and shigellosis. BMC Infect. Dis. 2014, 14, 440. [Google Scholar] [CrossRef] [Green Version]
- Njuguna, C.; Njeru, I.; Mgamb, E.; Langat, D.; Makokha, A.; Ongore, D.; Mathenge, E.; Kariuki, S. Enteric pathogens and factors associated with acute bloody diarrhoea, Kenya. BMC Infect. Dis. 2016, 16, 477. [Google Scholar] [CrossRef] [Green Version]
- Berendes, D.; Leon, J.; Kirby, A.; Clennon, J.; Raj, S.; Yakubu, H.; Robb, K.; Kartikeyan, A.; Hemavathy, P.; Gunasekaran, A.; et al. Household sanitation is associated with lower risk of bacterial and protozoal enteric infections, but not viral infections and diarrhoea, in a cohort study in a low-income urban neighbourhood in Vellore, India. Trop. Med. Int. Health 2017, 22, 1119–1129. [Google Scholar] [CrossRef] [Green Version]
- MICS6 TOOLS Study Design. Available online: http://mics.unicef.org/tools (accessed on 20 February 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Type | Source | Period | Temporal Resolution | Spatial Resolution |
|---|---|---|---|---|
| NDVI a | MODIS/Terra b | 2006, 2011 and 2016 | 16 days | 1 km |
| LST c in the daytime and at night | MODIS/Terra b | 2006, 2011 and 2016 | 8 days | 1 km |
| Elevation | WorldClim d | 2000 | - | 1 km |
| Moisture | Atlas of the Biosphere e | 1950–2000 | - | 50 km |
| Water bodies | SWBD f | 2000 | - | 30 m |
| Development Regions | 2006 | 2011 | 2016 | |||
|---|---|---|---|---|---|---|
| No. Respondents | Prevalence (%) | No. Respondents | Prevalence (%) | No. Respondents | Prevalence (%) | |
| Eastern | 1217 | 11.83 | 1148 | 11.66 | 902 | 6.33 |
| Central | 1342 | 12.30 | 1066 | 15.02 | 1264 | 9.67 |
| Western | 1281 | 12.87 | 1159 | 15.63 | 923 | 5.39 |
| Mid-western | 778 | 9.32 | 914 | 14.37 | 1078 | 8.49 |
| Far-western | 798 | 12.07 | 741 | 10.94 | 660 | 6.22 |
| Total | 5416 | 11.99 | 5028 | 13.92 | 4827 | 7.67 |
| Factors | with Diarrhea | without Diarrhea | p-Value | |
|---|---|---|---|---|
| Age c | Age (<12 month) | 457 (27.30%) | 2496 (18.36%) | <0.001 d,* |
| Age (12–24 month) | 538 (32.14%) | 2493 (18.33%) | ||
| Age (24–59 month) | 679 (40.56%) | 8608 (63.31%) | ||
| Gender c | Boy | 943 (56.33%) | 6960 (51.18%) | 0.053 c |
| Girl | 731 (43.67%) | 6637 (48.82%) | ||
| Live with mother c | Yes | 1672 (99.88%) | 13,521 (99.44%) | 0.028 c,* |
| No | 2 (0.12%) | 76 (0.56%) | ||
| Mother’s education year b | 0 (7) | 2 (8) | 0.001 d,* | |
| Mother’s age when gave birth b | 25 (7) | 26 (7) | 0.032 d,* | |
| Number of children under five years old b | 2 (1) | 2 (1) | 0.695 d | |
| Type of place of residence c | Urban | 460 (27.5%) | 4577 (33.7%) | 0.004 c,* |
| Rural | 1214 (72.5%) | 9020 (66.3%) | ||
| Residing status c | legal | 1569 (93.73) | 12,789 (94.06) | 0.629 c |
| Illegal | 105 (6.27) | 808 (5.94) | ||
| Wealth index a,b | −52,160 (96,609) | −47,194 (106,529) | 0.078 d | |
| Water source c | Improved | 1334 (79.69%) | 11,109 (81.70%) | 0.047 c,* |
| Unimproved | 235 (14.04%) | 1680 (12.36%) | ||
| Sanitation c | Improved | 676 (40.38%) | 6693 (49.22%) | <0.001 c,* |
| Unimproved | 893 (53.35%) | 6095 (44.83%) | ||
| Fuel c | Solid | 1362 (81.36%) | 10,756 (79.11%) | 0.006 c,* |
| Nonsolid | 207 (12.37%) | 2032 (14.94%) | ||
| Season c | Spring (Feb–Apr) | 739 (44.15%) | 4792 (35.24%) | <0.001 c,* |
| Summer (Mar–Jul) | 683 (40.80%) | 5086 (37.41%) | ||
| Autumn (Aug–Oct) | 108 (6.45%) | 1745 (12.83%) | ||
| Winter (Nov–Jan) | 144 (8.60%) | 1974 (14.52%) | ||
| Elevation b | 694.52 (1283.44) | 665.68 (1230.64) | 0.439 d | |
| NDVI b | 0.56 (0.11) | 0.56 (0.11) | 0.394 d | |
| Moisture b | 76.47 (39.30) | 81.66 (39.30) | 1.000 d | |
| LST_day (°C) b | 25.35 (4.83) | 25.49 (4.55) | 0.534 d | |
| LST_night (°C) b | 16.17 (5.97) | 16.36 (5.77) | 0.194 d | |
| Distance to the nearest water bodies b | 0.02 (0.02) | 0.02 (0.02) | 0.288 d | |
| Year | Moran’s I | Expected Index | Variance | z-Score | p-Value |
|---|---|---|---|---|---|
| 2006 | 0.03 | −0.01 | <0.01 | 0.64 | 0.53 |
| 2011 | 0.02 | −0.01 | <0.01 | 0.56 | 0.58 |
| 2016 | 0.04 | −0.01 | <0.01 | 1.01 | 0.31 |
| Covariates | Median (95% BCI) | OR (95% BCI) | Prob (%) $ |
|---|---|---|---|
| Gender (Girl) # | 0.22 (0.12, 0.33) * | 1.24 (1.13, 1.39) | >99.99 |
| Age of child (<12 month) # | |||
| 12–24 month | 0.18 (0.04, 0.32) * | 1.20 (1.04, 1.38) | 99.80 |
| >24 month | −0.86 (−0.99, −0.73) * | 0.42 (0.37, 0.48) | <0.01 |
| Mother’ education year | −0.07 (−0.14, −0.0003) * | 0.93 (0.87,0.997) | 2.80 |
| Mother’s age when gave birth | −0.03 (−0.09, 0.03) | 0.97 (0.91, 1.03) | 15.00 |
| Live with mother | 1.07 (−0.11, 2.72) | 2.91 (0.90, 15.18) | 93.6 |
| Type of place of residence (Rural) # | −0.04 (−0.18, 0.10) | 0.999 (0.84, 1.15) | 32.60 |
| Wealth index | −0.01 (−0.10, 0.08) | 0.99 (0.90, 1.08) | 40.20 |
| Water source (Unimproved) # | −0.0001 (−0.14, 0.14) | 1.0001 (0.81, 1.13) | 50.80 |
| Sanitation (Unimproved) # | −0.10 (−0.24, 0.04) | 0.79 (0.70, 0.91) | 6.80 |
| Fuel (Nonsolid) # | −0.04 (−0.26, 0.18) | 0.90 (0.79, 1.04) | 36.80 |
| Season (Spring) # | |||
| Summer | −0.14 (−0.29, 0.006) | 0.87 (0.75, 1.006) | 3.00 |
| Autumn | −0.85 (−1.12, −0.59) * | 0.43 (0.33, 0.55) | <0.01 |
| Winter | −0.68 (−0.92, −0.45) * | 0.51 (0.40, 0.64) | <0.01 |
| Spatial-temporal variance () | 7.36 (4.91, 11.70) | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, R.; Lai, Y.; Feng, C.; Dev, R.; Wang, Y.; Hao, Y. Diarrhea in Under Five Year-old Children in Nepal: A Spatiotemporal Analysis Based on Demographic and Health Survey Data. Int. J. Environ. Res. Public Health 2020, 17, 2140. https://doi.org/10.3390/ijerph17062140
Li R, Lai Y, Feng C, Dev R, Wang Y, Hao Y. Diarrhea in Under Five Year-old Children in Nepal: A Spatiotemporal Analysis Based on Demographic and Health Survey Data. International Journal of Environmental Research and Public Health. 2020; 17(6):2140. https://doi.org/10.3390/ijerph17062140
Chicago/Turabian StyleLi, Ruixue, Yingsi Lai, Chenyang Feng, Rubee Dev, Yijing Wang, and Yuantao Hao. 2020. "Diarrhea in Under Five Year-old Children in Nepal: A Spatiotemporal Analysis Based on Demographic and Health Survey Data" International Journal of Environmental Research and Public Health 17, no. 6: 2140. https://doi.org/10.3390/ijerph17062140