The Effects of Comprehensive Sexual and Reproductive Health/Family Planning Intervention Based on Knowledge, Attitudes, and Practices Among the Domestic Migrant Population of Reproductive Age in China: A Randomized Community Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
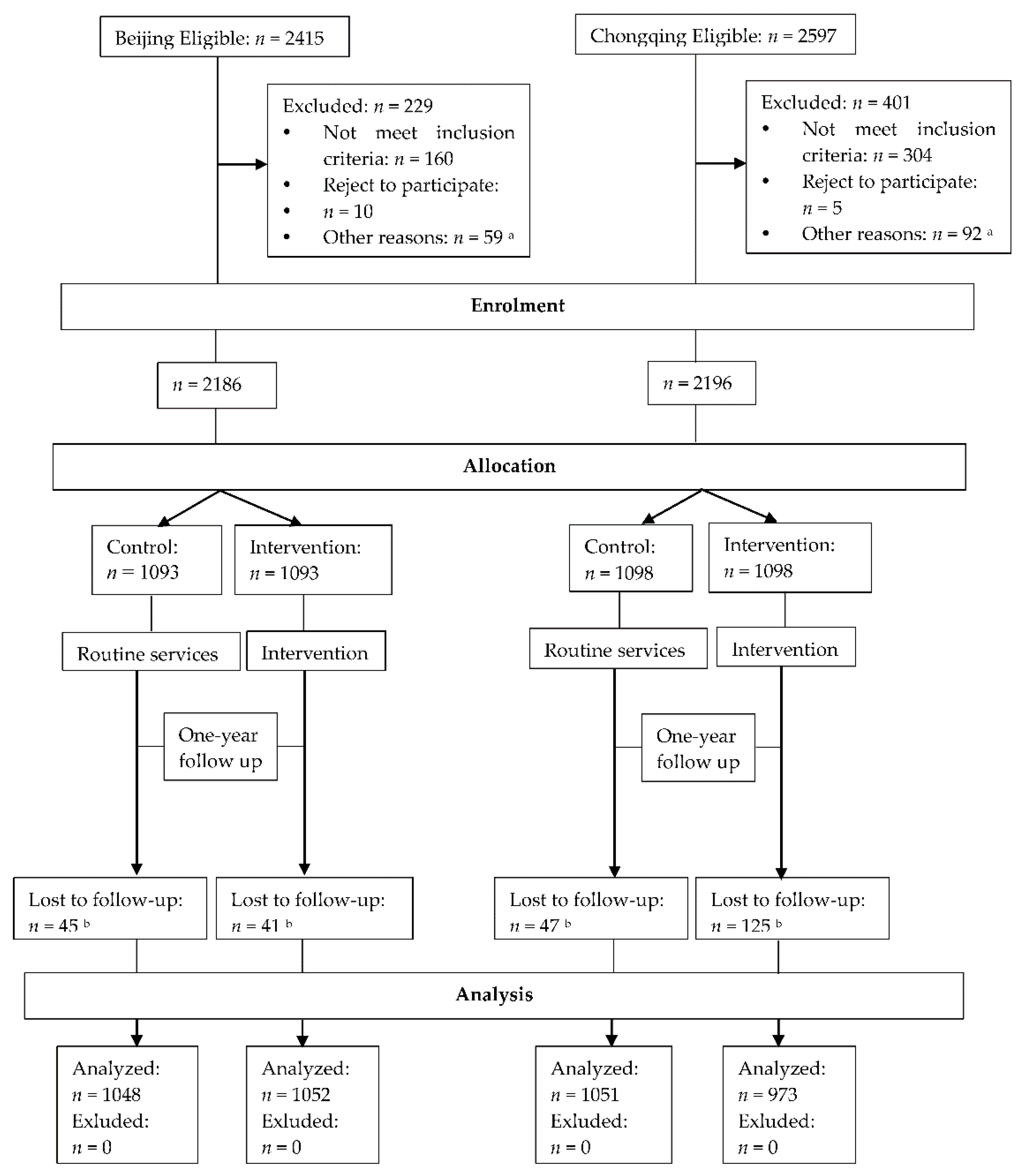
2.1. Sampling Methods
2.2. Sampling Size
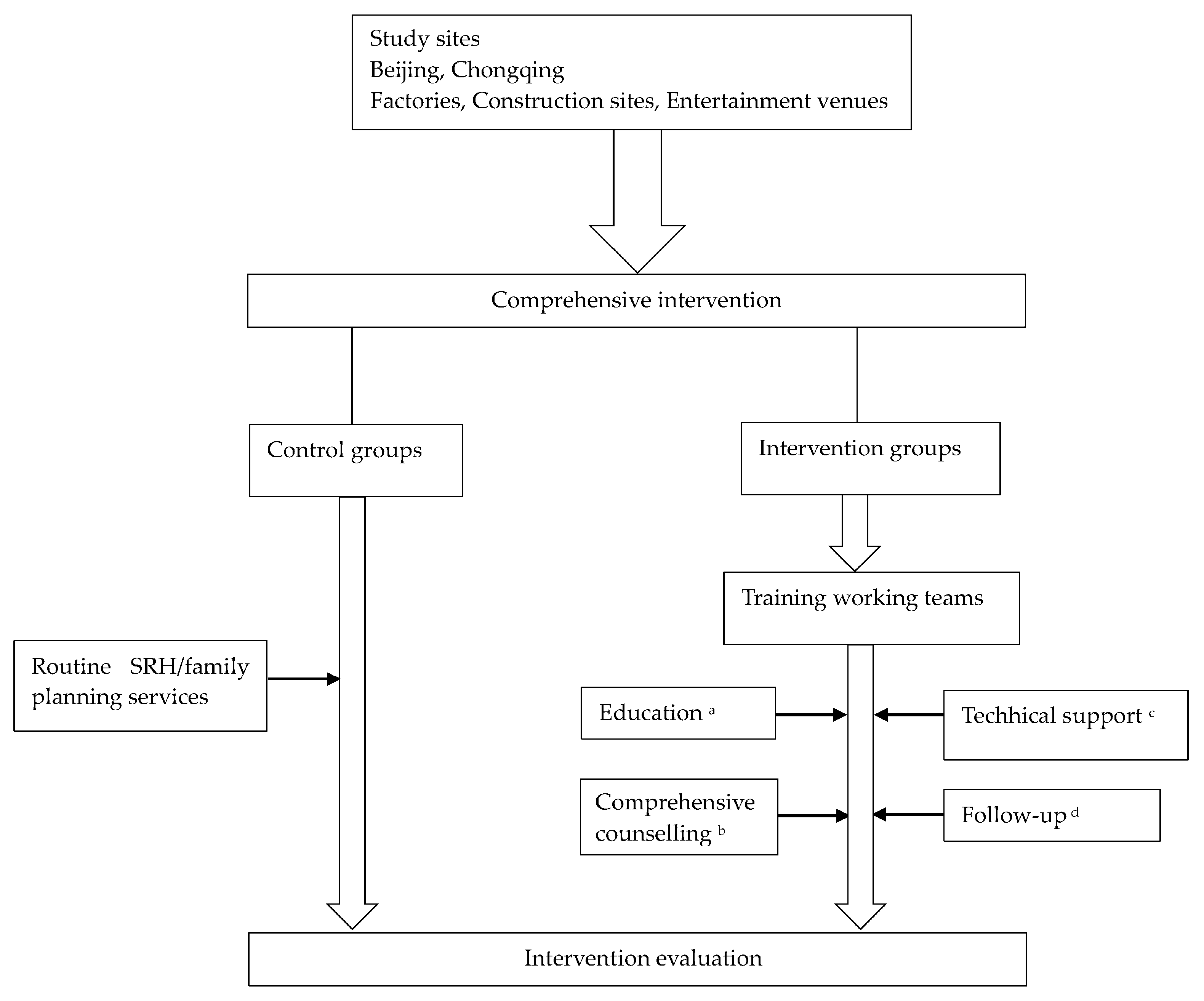
2.3. Study Design
2.4. Intervention Strategy
- (a)
- SRH/family planning education materials were developed to introduce the participants to the family planning regulations, as well as their rationales and applications, the pros and cons of contraceptive methods, knowledge about sexually transmitted diseases (STDs), and HIV/AIDS. The participants were given leaflets/brochures at least three times a month. The posters were put up in the specified areas and updated once a month. SRH lectures for the participants were held in the assigned places twice a month.
- (b)
- Counselling rooms were established to offer the participants counselling services for SRH/family planning at the study sites. SRH/family planning hot lines were also provided. Counselling files for in-depth analyses were generated to support the sustainable implementation of the intervention on the field. Expert counselling sessions were held once a quarter. The sessions could be held more frequently depending on the participants’ needs.
- (c)
- Technical services comprising maternal examinations, IUD examinations, and handling and checking certificates of marriage and childbirth for domestic migrant population (which are provided by the local department of family planning to prove the floating population’s identity, marital status, and birth status, and to facilitate the utilization of family planning services); were provided for free to the domestic migrant population. Contraceptives (pills and condoms) were also distributed. The participants were assisted by the working teams to select proper contraceptive methods in line with their own health conditions and encouraged the participants to take some novel contraceptives, including female condoms, IUDs and implants, etc. The teams encouraged the participants who were likely to engage in high-risk sexual behaviors to use condoms constantly. Actions were launched with several national welfare programs, such as the “cherishing girls action” (formulated by the State Council, which aims to protect the legitimate rights and interests of girls and to promote women’s development and gender equality) to facilitate the family planning benefit-oriented mechanism.
- (d)
- The follow-up was facilitated to be more pertinent, diverse, and standardized, and the follow-up quality and public service capacity were improved according to the requirements of “The Equalization of Family Planning Public Services for Migrant Populations”. A standardized and periodical follow-up was conducted by the working teams for the participants adopting contraceptive methods.
2.5. Quantitative Data Collected
2.6. Data Collection
2.7. Data Analysis
2.8. Ethics Approval and Consent to Participate
2.9. Patient and Public Involvement
3. Results
3.1. Comparison of the Characteristics between the Intervention and Control Groups in the Two Cities
3.2. Participation in the Comprehensive Intervention among the Participants in the Two Cities
3.3. Effects of Intervention on Knowledge among Participants
3.4. Effects of the Intervention on Attitude and Practice among Participants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIEI | adjusted intervention effect interval |
| HIV/AIDS | human immunodeficiency virus/ acquired immunodeficiency syndrome |
| ICPD | international conference on population and development |
| IE | intervention effects |
| SRH | sex and reproductive health |
| STD | sexual transmitted diseases |
Appendix A

{kind=link}
{kind=link}
| Type of Data | Variable | Assignment and Coding | Quantitative Indicator |
|---|---|---|---|
| Knowledge | knowledge of SRH and contraceptive methods▲ | N/A | Scores of knowledge on SRH and contraceptive methods |
| Attitude | What types of contraceptive methods do you expect to use? | Reversible = 1 Irreversible = 2 | % of “Reversible” |
| Do you think about whether the knowledge/information for SRH/family planning is enough? | Yes = 1 No = 1 | % of “Yes” | |
| Do you think about whether a man should be involved in SRH/family planning education? | Yes = 1 No = 1 | % of “Yes” | |
| Practice | What contraceptive methods are you using at present? | Reversible = 1◆ Irreversible = 2★ | % of “Reversible” |
| Who determines your use of contraceptive methods? | Couples/sexual partners = 1 Family planning service providers (FPSPs) /physicians/community health workers = 2 | % of “Couples/sexual partners” | |
| Have you received IUD assessment services? | Yes = 1 No = 1 | % of “Yes” | |
| Have you used condoms in your last three sexual encounters? | Yes = 1 No = 1 | % of “Yes” | |
| Have you received a “certificate of marriage and childbirth for domestic migrant population”? | Yes = 1 No = 1 | % of “Yes” | |
| Have you participated in family planning services? * | Yes = 1 No = 1 | % of “Yes” |
| Type of Variable | Variable | Assignment and Coding |
|---|---|---|
| Group | Group | Control = 1 Intervention = 2 |
| Demographic characteristics | Age | <20 = 1 20–29 = 2 30–39 = 3 40–49 = 4 |
| Gender | Male = 1 Female = 2 | |
| Occupation | Laborer = 1 White-collar worker = 2 Service worker = 3 Other (unemployed or self-employed) = 4 | |
| Educational attainment | Elementary school or lower = 1 Junior high school = 2 High school = 3 Junior college = 4 Undergraduate or higher = 5 | |
| Family per capita monthly income (yuan) | <1000 = 1 1000–2999 = 2 3000–4999 = 3 ≧5000 = 4 | |
| Registered residence status | Rural = 1 Urban = 2 | |
| Migration characteristics | Length of the first immigration up to now (year) | <3 = 1 3–6 = 2 7–10 = 3 ≧11 = 4 |
| Length of stay in city per year (month) | <7 = 1 7–9 = 2 ≧10 = 3 | |
| Purpose for migration | Work = 1 Marriage = 2 Giving birth = 3 Other (business/learning skills) = 4 | |
| Whether having medical insurance or not in city | Yes = 1 No = 2 | |
| Current living conditions | Dormitory = 1 Renting = 2 Renting with families = 3 Own house = 4 Renting with others = 5 Other = 6 | |
| Status of medical payment | Full self-paying = 1 Most self-paying = 2 Less self-paying = 3 Payed by the employer = 4 Other = 5 | |
| Sexual and marital characteristics | Age of the first intercourse | <20 = 1 20–25 = 2 26–30 = 3 ≧30 = 4 |
| Partner of the first intercourse | Boyfriend/girlfriend = 1 Spouse = 2 Other = 3 | |
| Marital status | Married = 1 Unmarried, but has had sexual partners = 2, divorced/bereaved, no sexual partners = 3, single = 4 | |
| Months with spouse/partner per year | <1 = 1 1–6 = 2 7–12 = 3 | |
| Frequency of communication with spouse/partner | Rarely = 1 Sometimes = 2 Frequently = 3 | |
| Having sex depression | Yes = 1 No = 2 | |
| Engaging in masturbation | Yes = 1 No = 2 |
| Variable | Control (n = 1048) | Intervention (n = 1052) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Age | 1.98 | ||||||
| <20 | 7 | 0.67 | 7 | 0.67 | 0 | 0 | |
| 20–29 | 235 | 22.42 | 218 | 20.72 | 0 | 0.041 | |
| 30–39 | 464 | 44.27 | 455 | 43.25 | 0.005 | 0.021 | |
| 40–49 | 342 | 32.63 | 372 | 35.36 | 0.005 | 0.058 | |
| Gender | 0.62 | ||||||
| Male | 321 | 30.63 | 339 | 32.22 | 0.043 | 0.034 | |
| Female | 727 | 69.37 | 713 | 67.78 | 0.043 | 0.034 | |
| Occupation | 13.12 ** | ||||||
| Laborer | 69 | 6.58 | 104 | 9.89 | 0.019 | 0.120 | |
| White-collar worker | 142 | 13.55 | 132 | 12.55 | 0.018 | 0.030 | |
| Service worker | 748 | 71.37 | 756 | 71.86 | 0.022 | 0.011 | |
| Other (unemployed or self-employed) | 89 | 8.49 | 60 | 5.70 | 0.005 | 0.109 | |
| Educational attainment | 4.41 | ||||||
| Elementary school or lower | 78 | 7.44 | 67 | 6.37 | 0.029 | 0.042 | |
| Junior high school | 349 | 33.30 | 374 | 35.55 | 0.013 | 0.047 | |
| High school | 315 | 30.06 | 311 | 29.56 | 0.041 | 0.011 | |
| Junior college | 164 | 15.65 | 141 | 13.40 | 0.003 | 0.064 | |
| Undergraduate or higher | 142 | 13.55 | 159 | 15.11 | 0.010 | 0.045 | |
| Family per capita monthly income (yuan) | 5.32 | ||||||
| <1000 | 19 | 1.81 | 27 | 2.57 | 0.045 | 0.052 | |
| 1000–2999 | 151 | 14.41 | 177 | 16.83 | 0.007 | 0.067 | |
| 3000–4999 | 422 | 40.27 | 420 | 39.93 | 0.027 | 0.007 | |
| 5000–6999 | 288 | 27.48 | 284 | 27.00 | 0.039 | 0.011 | |
| 7000 | 168 | 16.03 | 144 | 13.69 | 0.014 | 0.066 | |
| Registered residence status | 1.05 | ||||||
| Rural | 675 | 64.41 | 700 | 66.54 | 0.010 | 0.045 | |
| Urban | 373 | 35.59 | 352 | 33.46 | 0.010 | 0.045 | |
| Variable | Control (n = 1048) | Intervention (n = 1052) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Length of the first immigration up to now (year) | 3.35 | ||||||
| <3 | 148 | 14.12 | 146 | 13.88 | 0.011 | 0.007 | |
| 3–6 | 233 | 22.23 | 204 | 19.39 | 0.003 | 0.007 | |
| 6–10 | 276 | 26.34 | 277 | 26.33 | 0.011 | 0 | |
| ≥10 | 391 | 37.31 | 425 | 40.40 | 0.005 | 0.063 | |
| Length of stay in city per year (month) | 5.31 | ||||||
| <7 | 29 | 2.77 | 29 | 2.76 | 0.015 | 0.001 | |
| 7–9 | 36 | 3.44 | 58 | 5.51 | 0.019 | 0.101 | |
| ≥10 | 983 | 93.80 | 965 | 91.73 | 0.005 | 0.080 | |
| Purpose for migration | 5.23 | ||||||
| Work | 843 | 80.44 | 881 | 83.75 | 0.016 | 0.086 | |
| Marriage | 150 | 14.31 | 116 | 11.03 | 0.008 | 0.099 | |
| Giving birth | 13 | 1.24 | 12 | 1.14 | 0 | 0.009 | |
| Other (business/learning skills) | 42 | 4.01 | 43 | 4.09 | 0.018 | 0.004 | |
| Whether having medical insurance or not in city | 9.97 ** | ||||||
| Yes | 557 | 53.15 | 631 | 59.98 | 0.010 | 0.028 | |
| No | 491 | 46.85 | 421 | 40.02 | 0.010 | 0.019 | |
| Current living conditions | 8.47 | ||||||
| Dormitory | 220 | 20.99 | 263 | 25.00 | 0.012 | 0.095 | |
| Renting | 301 | 28.72 | 287 | 27.28 | 0.008 | 0.032 | |
| Renting with families | 374 | 35.69 | 345 | 32.79 | 0.013 | 0.061 | |
| Own house | 97 | 9.26 | 98 | 9.32 | 0.025 | 0.002 | |
| Renting with others | 27 | 2.58 | 38 | 3.61 | 0.030 | 0.060 | |
| Other | 29 | 2.77 | 21 | 2.00 | 0 | 0.051 | |
| Medical payment | 6.08 | ||||||
| Full self-paying | 429 | 40.94 | 425 | 40.40 | 0.002 | 0.011 | |
| Most self-paying | 307 | 29.29 | 320 | 30.42 | 0.011 | 0.025 | |
| Less self-paying | 249 | 23.76 | 266 | 25.29 | 0.023 | 0.035 | |
| paying by the employer | 53 | 5.06 | 32 | 3.04 | 0.038 | 0.102 | |
| Other | 10 | 0.95 | 9 | 0.86 | 0.013 | 0.010 | |
| Variable | Control (n = 1048) | Intervention (n = 1052) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Age of the first intercourse | 3.18 | ||||||
| <20 | 119 | 11.35 | 101 | 9.60 | 0.034 | 0.057 | |
| 20–25 | 753 | 71.85 | 771 | 73.29 | 0.006 | 0.032 | |
| 26–30 | 158 | 15.08 | 154 | 14.64 | 0.007 | 0.012 | |
| ≥30 | 18 | 1.72 | 26 | 2.47 | 0.035 | 0.053 | |
| Partner of the first intercourse | 14.03 *** | ||||||
| Boy/girl friend | 246 | 23.54 | 212 | 20.54 | 0 | 0.064 | |
| Spouse | 770 | 73.68 | 811 | 78.59 | 0.006 | 0.107 | |
| Other | 29 | 2.78 | 9 | 0.87 | 0.025 | 0.144 | |
| Marital status | 7.27 * | ||||||
| Married | 973 | 92.84 | 943 | 89.64 | 0 | 0.114 | |
| unmarried, but had sex partners | 64 | 6.11 | 97 | 9.22 | 0.015 | 0.117 | |
| Divorced/bereaved, no sex partners | 11 | 1.05 | 12 | 1.14 | 0.036 | 0.009 | |
| Months with spouse/partner per year | |||||||
| <1 | 76 | 7.25 | 53 | 5.04 | 18.08 *** | 0.006 | 0.092 |
| 1–6 | 162 | 15.46 | 233 | 22.15 | 0.023 | 0.172 | |
| 7–12 | 810 | 77.29 | 766 | 72.81 | 0.024 | 0.104 | |
| Frequency of communication with spouse/partner | 0.52 | ||||||
| Rarely | 264 | 25.19 | 279 | 26.52 | 0.008 | 0.030 | |
| Sometimes | 644 | 61.45 | 632 | 60.08 | 0.005 | 0.028 | |
| Frequently | 140 | 13.36 | 141 | 13.40 | 0.004 | 0.001 | |
| Whether having sex depression | 1.55 | ||||||
| Yes | 58 | 5.53 | 72 | 6.84 | 0.010 | 0.054 | |
| No | 990 | 94.47 | 980 | 93.16 | 0.010 | 0.054 | |
| Whether having masturbation | 0.15 | ||||||
| Yes | 113 | 10.78 | 108 | 10.27 | 0.020 | 0.017 | |
| No | 935 | 89.22 | 944 | 89.73 | 0.020 | 0.017 | |
| Variable | Control (n = 1051) | Intervention (n = 973) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Age | 31.47 *** | ||||||
| <20 | 63 | 5.99 | 110 | 11.31 | 0.006 | 0.190 | |
| 20–29 | 362 | 34.44 | 365 | 37.51 | 0.059 | 0.064 | |
| 30–39 | 264 | 25.12 | 171 | 17.57 | 0.004 | 0.185 | |
| 40–49 | 362 | 34.44 | 327 | 33.61 | 0.061 | 0.018 | |
| Gender | 40.49 *** | ||||||
| Male | 626 | 59.56 | 442 | 45.43 | 0.016 | 0.286 | |
| Female | 425 | 40.44 | 531 | 54.57 | 0.016 | 0.286 | |
| Occupation | 10.01 * | ||||||
| Laborer | 553 | 52.62 | 576 | 59.20 | 0.003 | 0.133 | |
| White-collar worker | 277 | 26.36 | 232 | 23.84 | 0.026 | 0.058 | |
| Service worker | 205 | 19.51 | 150 | 15.42 | 0.021 | 0.108 | |
| Other (unemployed or self-employed) | 16 | 1.52 | 15 | 1.54 | 0.011 | 0.002 | |
| Educational attainment | 34.61 *** | ||||||
| Elementary school or lower | 73 | 6.95 | 115 | 11.82 | 0 | 0.168 | |
| Junior high school | 365 | 33.87 | 330 | 33.92 | 0.003 | 0.001 | |
| High school | 325 | 30.92 | 332 | 34.12 | 0.024 | 0.068 | |
| Junior college | 159 | 15.13 | 128 | 13.16 | 0.056 | 0.057 | |
| Undergraduate or higher | 138 | 13.13 | 68 | 6.99 | 0.022 | 0.205 | |
| Family per capita monthly income (yuan) | 19.71 ** | ||||||
| <1000 | 39 | 3.71 | 36 | 3.70 | 0.033 | 0.001 | |
| 1000–2999 | 264 | 25.12 | 183 | 18.81 | 0.011 | 0.153 | |
| 3000–4999 | 366 | 34.82 | 405 | 41.62 | 0.003 | 0.140 | |
| 5000–6999 | 273 | 26.98 | 224 | 23.02 | 0.015 | 0.069 | |
| 7000 | 109 | 10.37 | 125 | 12.85 | 0.010 | 0.077 | |
| Registered residence status | 53.09 *** | ||||||
| Rural | 626 | 59.56 | 728 | 74.82 | 0.003 | 0.329 | |
| Urban | 425 | 40.44 | 245 | 25.18 | 0.003 | 0.329 | |
| Variable | Control (n = 1051) | Intervention (n = 973) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Length of the first immigration up to now (year) | 72.75 *** | ||||||
| <3 | 218 | 20.74 | 344 | 35.35 | 0.004 | 0.330 | |
| 3–6 | 186 | 17.70 | 197 | 20.25 | 0.012 | 0.065 | |
| 6–10 | 214 | 20.36 | 170 | 17.47 | 0.008 | 0.074 | |
| ≥10 | 433 | 41.20 | 262 | 26.93 | 0.020 | 0.305 | |
| Length of stay in city per year (month) | 12.54 ** | ||||||
| <7 | 168 | 15.98 | 209 | 21.48 | 0 | 0.141 | |
| 7–9 | 40 | 3.81 | 48 | 4.93 | 0.016 | 0.055 | |
| ≥10 | 843 | 80.21 | 716 | 73.59 | 0.008 | 0.158 | |
| Purpose for migration | 2.09 | ||||||
| Work | 921 | 87.63 | 848 | 87.15 | 0.009 | 0.014 | |
| Marriage | 74 | 7.04 | 62 | 6.37 | 0.006 | 0.027 | |
| Giving birth | 12 | 1.14 | 10 | 1.03 | 0.017 | 0.011 | |
| Other (business/learning skills) | 44 | 4.19 | 53 | 5.45 | 0.031 | 0.059 | |
| Whether having medical insurance or not in city | 13.88 ** | ||||||
| Yes | 743 | 70.69 | 612 | 62.90 | 0.020 | 0.166 | |
| No | 308 | 29.31 | 361 | 37.10 | 0.020 | 0.166 | |
| Current living conditions | 66.11 *** | ||||||
| Dormitory | 381 | 36.25 | 467 | 48.00 | 0.039 | 0.240 | |
| Renting | 241 | 22.93 | 241 | 24.77 | 0.007 | 0.043 | |
| Renting with families | 128 | 12.18 | 114 | 11.72 | 0.033 | 0.014 | |
| Own house | 261 | 24.83 | 113 | 11.61 | 0.031 | 0.348 | |
| Renting with others | 20 | 1.90 | 23 | 2.36 | 0.042 | 0.032 | |
| Other | 20 | 1.90 | 15 | 1.54 | 0 | 0.028 | |
| Status of medical payment | 56.56 *** | ||||||
| Full self-paying | 295 | 28.07 | 349 | 35.87 | 0.007 | 0.168 | |
| Most self-paying | 327 | 31.11 | 367 | 37.72 | 0.003 | 0.139 | |
| Less self-paying | 379 | 36.06 | 209 | 21.48 | 0.018 | 0.326 | |
| paying by the employer | 26 | 2.47 | 16 | 1.64 | 0.022 | 0.058 | |
| Other | 24 | 2.28 | 32 | 3.29 | 0.040 | 0.061 | |
| Variable | Control (n = 1051) | Intervention (n = 973) | χ2 | Standardized Difference | Standardized Difference | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | (Matched Sample) | (Unmatched Sample) | ||
| Age of the first intercourse | 12.87 ** | ||||||
| <20 | 315 | 29.97 | 314 | 32.27 | 0.041 | 0.050 | |
| 20–25 | 663 | 63.08 | 625 | 64.23 | 0.046 | 0.024 | |
| 26–30 | 66 | 6.28 | 29 | 2.98 | 0.008 | 0.157 | |
| ≥30 | 7 | 0.67 | 5 | 0.51 | 0.021 | 0.020 | |
| Partner of the first intercourse | 1.57 | ||||||
| Boy/girl friend | 517 | 49.19 | 469 | 48.20 | 0.076 | 0.020 | |
| Spouse | 496 | 47.19 | 477 | 49.02 | 0.073 | 0.037 | |
| Other | 38 | 3.62 | 27 | 2.77 | 0.010 | 0.048 | |
| Marital status | 7.98 * | ||||||
| Married | 713 | 67.84 | 626 | 64.34 | 0.064 | 0.074 | |
| unmarried, but had sex partners | 133 | 12.65 | 165 | 16.96 | 0.022 | 0.121 | |
| Divorced/breaved, no sex partners | 192 | 18.27 | 167 | 17.16 | 0.059 | 0.029 | |
| Single | 13 | 1.24 | 15 | 1.54 | 0 | 0.026 | |
| Months with spouse/partner per year | 5.42 | ||||||
| <1 | 241 | 22.93 | 213 | 21.89 | 0.077 | 0.025 | |
| 1–6 | 222 | 21.12 | 248 | 25.49 | 0.060 | 0.103 | |
| 7–12 | 588 | 55.95 | 512 | 52.62 | 0.013 | 0.067 | |
| Frequency of communication with spouse/partner | 1.19 | ||||||
| Rarely | 219 | 20.84 | 222 | 22.82 | 0.008 | 0.048 | |
| Sometimes | 589 | 56.04 | 529 | 54.37 | 0.006 | 0.034 | |
| Frequently | 243 | 23.12 | 222 | 22.82 | 0 | 0.007 | |
| Whether having sex depression | 0.30 | ||||||
| Yes | 157 | 14.94 | 137 | 14.08 | 0.023 | 0.024 | |
| No | 894 | 85.06 | 836 | 85.92 | 0.023 | 0.024 | |
| Whether having masturbation | 3.53 | ||||||
| Yes | 214 | 20.46 | 167 | 17.18 | 0.016 | 0.082 | |
| No | 832 | 79.54 | 805 | 82.82 | 0.016 | 0.091 | |
References
- The National Health and Family Planning Commission. The 2016 Report on China’s Migrant Population Development; China Population Publishing House: Beijing, China, 2016. [Google Scholar]
- Liu, Y.; Feng, J. Characteristics and Impact Factors of Migration in China: Based on the Analysis of The Sixth Census Data. Hum. Geogr. 2014, 29, 129–137. [Google Scholar]
- Tang, J.; Gao, X.; Yu, Y.; Ahmed, N.I.; Zhu, H.; Wang, J.; Du, Y. Sexual knowledge, attitudes and behaviors among unmarried migrant female workers in China: A comparative analysis. BMC Public Health 2011, 11, 917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.Y.; Li, N.; Zhou, Y.; Liu, B.Y.; Yu, S.; Zhang, H.; Zhao, H.X.; Wu, J.Q. Study of HIV/AIDS-related sexual behaviors and influencing factors among migrants in Shenzhen, China. Fudan Univ. J. Med. Sci. 2010, 37, 304–309. [Google Scholar]
- Cai, B.; Shang, M.; Cai, Y. Study of HIV/AIDS related knowledge, attitude, and premarital sexual intercourse among unmarried female migrant workers in Shanghai. J. Shanghai Jiaotong Univ. (Med Sci.) 2013, 33, 1643–1647. [Google Scholar]
- Hongxin, Z. Family Planning/Reproductive Health and the Assessment of Qualified Service among Migrant Population in Three Cities China. Ph.D. Thesis, Fudan University, Shanghai, China, 2011. [Google Scholar]
- Yu, C.; Wu, J.; Li, Y.; Zhou, Y.; Zhao, R.; Ji, H.; Li, Y.-R.; Han, Y.; Tong, Q. The Other Side: How does Informed Choice Affect Induced Abortions among Reproductive-Age Immigrant Women in China—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2016, 13, 1038. [Google Scholar] [CrossRef] [PubMed]
- Junqing, W.; Shikun, Z. Management and Service of Sexual and Reproductive Health for Migrants in China; Shanghai Scientific and Technical Publishers: Shanghai, China, 2015. [Google Scholar]
- Kewei, W. An Intervention Study of Informed Choice on Contraceptives among Female Migrants of Reproductive Age in Shanghai. Ph.D. Thesis, Fudan University, Shanghai, China, 2014. [Google Scholar]
- Liu, P.; Wu, J.; Du, G. Awareness of AIDS knowledge among permanent population and floating population in Zhangjiagang City. Occup. Health 2014, 30, 798–801. [Google Scholar]
- World Health Organization. International Classification of Health Interventions (ICHI)—Alpha Version; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Lin, D.; Li, X.; Stanton, B.; Fang, X.; Lin, X.; Xu, X.; Ma, L.; Xia, C. Theory-based HIV-related sexual risk reduction prevention for Chinese female rural-to-urban migrants. AIDS Educ. Prev. 2010, 22, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Shuangfei, X.; Yuyan, L.; Junqing, W. Prevalence, risk factors and control strategies of reproductive tract infection, sex transmitted disease and acquired immune deficiency syndrome among floating people. Chin. J. Reprod. Contracept. 2017, 37, 250–254. [Google Scholar]
- He, D.; Cheng, Y.-M.; Wu, S.-Z.; Decat, P.; Wang, Z.-J.; Minkauskiene, M.; Moyer, E. Promoting contraceptive use more effectively among unmarried male migrants in construction sites in China: A pilot intervention trial. Asia Pac. J. Public Health 2012, 24, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Vu, L.T.H.; Nguyen, N.T.K.; Tran, H.T.D.; Muhajarine, N. mHealth information for migrants: An e-health intervention for internal migrants in Vietnam. Reprod. Health 2016, 13, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendelsohn, J.B.; Calzavara, L.; Light, L.; Burchell, A.N.; Ren, J.; Kang, L. Design and implementation of a sexual health intervention for migrant construction workers situated in Shanghai, China. Emerg. Themes Epidemiol. 2015, 12, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichun, X.; Meihua, S.; Xuchun, Z.; Shu, L. Performance appraisal of reproductive health service for floating populationin, Shenzhen. Chin. J. Fam. Plan. 2010, 2, 73–77. [Google Scholar]
- Kaliyaperumal, K. Guideline for Conducting a Knowledge, Attitude and Practice (KAP) Study. AECS Illum. 2004, 4, 7–9. [Google Scholar]
- Thoemmes, F.J.; Kim, E.S. A systematic review of propensity score methods in the social sciences. Multivar. Behav. Res. 2011, 46, 90–118. [Google Scholar] [CrossRef]
- World Health Organization. Health Education: Theoretical Concepts, Effective Strategies and Core Competencies: A Foundation Document to Guide Capacity Development of Health Educators; World Health Organization: Atlanta, GA, USA, 2012. [Google Scholar]
- Li, Y. HNA and Socio-Psycho-Behavioral Factors Associated to Male Reproductive Health in Chongqing. Ph.D. Thesis, Third Minitary Medical University of Chinese, P.L.A., Chongqing, China, 2011. [Google Scholar]
- Arlen. What is Certificate of Marriage and Childbirth for Internal Migrant Population? Available online: http://www.chashebao.com/shengyubaoxian/15487.html (accessed on 1 December 2017).


| Variable | Beijing (n = 1052) | Chongqing (n = 973) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Frequency of receiving leaflets/brochures | ||||
| 0 | 77 | 7.30 | 594 | 61.05 |
| 1~2 | 198 | 18.82 | 315 | 32.37 |
| 3~4 | 666 | 63.33 | 54 | 5.55 |
| 5~6 | 61 | 5.80 | 7 | 0.72 |
| >6 | 50 | 4.75 | 3 | 0.31 |
| Interest in reading leaflets/brochures | ||||
| Not interested | 24 | 2.46 | 25 | 6.60 |
| Interested in some of them | 327 | 33.54 | 136 | 35.88 |
| Interested in most of them | 613 | 62.87 | 196 | 51.72 |
| Interested in all | 11 | 1.13 | 22 | 5.80 |
| Gains from leaflets/brochures | ||||
| No gains | 30 | 3.08 | 17 | 4.49 |
| Having some gains | 569 | 58.36 | 191 | 50.40 |
| Having great gains | 376 | 38.56 | 171 | 45.12 |
| Content assessment of leaflets/brochures | ||||
| Too shallow | 19 | 1.95 | 21 | 5.54 |
| Too difficult | 53 | 5.44 | 42 | 11.08 |
| Moderately difficult | 417 | 42.77 | 195 | 51.45 |
| Very helpful | 483 | 49.54 | 119 | 31.40 |
| Other | 3 | 0.31 | 2 | 0.53 |
| Frequency of participating in SRH/family planning lectures | ||||
| 0 | 574 | 54.56 | 617 | 63.41 |
| 1~2 | 280 | 26.62 | 321 | 32.99 |
| 3~4 | 140 | 13.31 | 28 | 2.88 |
| 5~6 | 40 | 3.80 | 6 | 0.62 |
| >6 | 18 | 1.71 | 1 | 0.10 |
| Gains from SRH/family planning lectures a | ||||
| No gains | 4 | 0.84 | 12 | 3.37 |
| Having some gains | 213 | 44.56 | 135 | 37.92 |
| Having great gains | 261 | 54.60 | 205 | 57.58 |
| Frequency of watching SRH/family planning VCDs | ||||
| 0 | 810 | 77.00 | 829 | 85.20 |
| 1~2 | 154 | 14.64 | 116 | 11.92 |
| 3~4 | 66 | 6.27 | 21 | 2.16 |
| 5~6 | 14 | 1.33 | 6 | 0.62 |
| >6 | 8 | 0.76 | 1 | 0.10 |
| Gains from SRH/family planning VCDs | ||||
| No gains | 3 | 1.24 | 17 | 11.81 |
| Having some gains | 119 | 49.17 | 63 | 43.75 |
| Having great gains | 120 | 49.59 | 64 | 44.44 |
| Frequency of browsing posters | ||||
| 0 | 506 | 48.10 | 616 | 63.31 |
| 1~2 | 274 | 26.05 | 297 | 30.52 |
| 3~4 | 199 | 18.92 | 49 | 5.04 |
| 5~6 | 52 | 4.94 | 9 | 0.92 |
| >6 | 21 | 2.00 | 2 | 0.21 |
| Interested in posters | ||||
| Not interested | 15 | 2.75 | 20 | 5.60 |
| Interested in some of posters | 290 | 53.11 | 153 | 42.86 |
| Interested in most of posters | 237 | 43.41 | 165 | 46.22 |
| Interested in all | 4 | 0.73 | 19 | 5.32 |
| Gains from posters | ||||
| No gains | 21 | 3.85 | 23 | 6.44 |
| Having some gains | 315 | 57.69 | 172 | 48.18 |
| Having great gains | 210 | 38.46 | 162 | 45.38 |
| Frequency of face-to-face counselling for SRH/family planning | ||||
| 0 | 740 | 70.34 | 717 | 73.69 |
| 1~2 | 229 | 21.77 | 227 | 23.33 |
| 3~4 | 65 | 6.18 | 18 | 1.85 |
| 5~6 | 18 | 1.71 | 10 | 1.03 |
| >6 | 0 | 0 | 1 | 0.10 |
| Content assessment of face-to-face counselling | ||||
| Too shallow | 3 | 0.96 | 4 | 1.56 |
| Too difficult | 34 | 10.90 | 42 | 16.41 |
| Moderately difficult | 106 | 33.97 | 83 | 32.42 |
| Very helpful | 168 | 53.85 | 123 | 48.05 |
| Other | 1 | 0.32 | 4 | 1.56 |
| Frequency of counselling by phone | ||||
| 0 | 774 | 73.57 | 824 | 84.69 |
| 1~2 | 177 | 16.83 | 124 | 12.74 |
| 3~4 | 81 | 7.70 | 17 | 1.75 |
| 5~6 | 20 | 1.90 | 6 | 0.62 |
| >6 | 0 | 0 | 2 | 0.21 |
| Content assessment of counselling by phone | ||||
| Too shallow | 3 | 1.08 | 5 | 3.36 |
| Too difficult | 29 | 10.43 | 24 | 16.11 |
| Moderately difficult | 103 | 37.05 | 52 | 34.90 |
| Very helpful | 141 | 50.72 | 66 | 44.30 |
| Other | 2 | 0.72 | 2 | 1.34 |
| Variable | Beijing (815 pairs) | Chongqing (629 pairs) | ||||
|---|---|---|---|---|---|---|
| Control (Mean ± Std) | Intervention (Mean ± Std) | Sensitivity Analysis | Control (Mean ± Std) | Intervention (Mean ± Std) | Sensitivity Analysis | |
| Knowledge on contraception | −0.61 ± 0.76 | 0.61 ± 0.77 | t = 32.46, p < 0.0001; AIEI: (1.22, 1.23), IE = 1.23, adjusted 95%CI: (1.16, 1.31) | −0.37 ± 0.73 | 0.37 ± 0.99 | t = 15.86, p < 0.001; AIEI: (0.74, 0.76), IE = 0.75, adjusted 95% CI: (0.65, 0.84) |
| Knowledge on SRH | −0.49 ± 0.87 | 0.49 ± 0.86 | t = 22.78, p < 0.0001; AIEI: (0.98, 0.99), E = 0.99, adjusted 95%CI: (0.90, 1.07) | −0.37 ± 0.89 | 0.37 ± 0.95 | t = 14.00, p < 0.0001; AIEI: (0.74, 0.76), IE = 0.75, adjusted 95% CI: (0.63, 0.85) |
| Variate (Quantitative Indicator) | Beijing | Chongqing | ||||
|---|---|---|---|---|---|---|
| Intervention (%) | Control (%) | Sensitivity Analysis | Intervention (%) | Control (%) | Sensitivity Analysis | |
| Attitudes | ||||||
| 713 pairs | 410 pairs | |||||
| What type of contraceptive methods do you expect to use? ** (% of “Reversible”) | 94.25 | 89.48 | S = 10.51, p = 0.0012, p-value interval: (0.0008, 0.0019) * | 95.12 | 91.46 | S = 4.59, p = 0.0321, p-value interval: (0.0213, 0.0329) * |
| 815 pairs | 629 pairs | |||||
| Do you think about whether the knowledge/information for SRH/family planning is enough? (% of “Yes”) | 60.12 | 47.36 | S = 9.42, p = 0.0021, p-value interval: (0.0018, 0.0083) * | 52.31 | 35.45 | S = 39.01, p < 0.0001#* |
| Do you think about whether a man should be involved in SRH/family planning education? (% of “Yes”) | 79.51 | 72.27 | S = 11.72, p = 0.0006, p-value interval: (0.0005, 0.0021) * | 73.29 | 59.30 | S = 26.89, p < 0.0001#* |
| Practices | ||||||
| 713 pairs | 410 pairs | |||||
| What contraceptive methods are you using currently? ** (% of “Couples/sexual partners”) | 95.23 | 92.14 | S = 5.38, p = 0.0204, p-value interval: (0.0149, 0.0275) * | 95.61 | 90.73 | S = 7.41, p = 0.0065, p-value interval: (0.0038, 0.0067) * |
| Who determines the utilization of contraceptive methods? ** (% of “Reversible”) | 94.59 | 89.74 | S = 11.67, p = 0.0006, p-value interval: (0.0004, 0.0097) * | 94.39 | 82.93 | S = 25.39, p < 0.0001 ** |
| 114 pairs | 115 pairs | |||||
| Have you received an IUD assessment service? ** (% of “Yes”) | 76.32 | 56.14 | S = 9.61, p = 0.0019, p-value interval: (0.0005, 0.0010) * | 74.78 | 57.39 | S = 6.90, p = 0.0086, p-value interval: (0.0054, 0.0093) * |
| 837 pairs | 520 pairs | |||||
| Have you used condoms in the last three sexual encounters? ** (% of “Yes”) | 65.23 | 57.96 | S = 9.37, p = 0.0022, p-value interval: (0.0018, 0.0085) * | 52.31 | 39.81 | S = 16.44, p < 0.0001 * |
| 815 pairs | 629 pairs | |||||
| Have you gotten the “certificate of marriage and childbirth for domestic migrant populations”? (% of “Yes”) | 78.40 | 73.25 | S = 5.92, p = 0.0150, p-value interval: (0.0126, 0.0331) * | 42.77 | 31.00 | S = 18.88, p < 0.0001 * |
| Have you participated in for family planning services? (% of “Yes”) | 31.53 | 22.94 | S = 15.12, p = 0.0001, p-value interval: (0.0001, 0.0004) * | 10.49 | 3.66 | S = 22.83, p < 0.0001 ** |
| Variable | Beijing | Chongqing |
|---|---|---|
| Models | Models | |
| Attitude | ||
| n = 1864 | n = 1476 | |
| What type of contraceptive methods do you expect to use? △ | Trivariate probit model▲★: intervention: (β = 0.24, p = 0.0129), 95%CI: (0.05, 0.43) | Trivariate probit model▲★: intervention: (β = 0.27, p = 0.0116), 95%CI: (0.06, 0.48) |
| Practice | ||
| n = 1864 | n = 1476 | |
| What contraceptive methods are you adopting currently? △ | Trivarate probit model▼★: Intervention: (β = 0.25, p = 0.0159), 95%CI: (0.05, 0.46) | Trivariate probit model▼★: Intervention: (β = 0.47, p < 0.0001), 95%CI: (0.25, 0.69) |
| Who determines the utilization of contraceptive methods? △ | Trivarate probit model▲★: Intervention: (β = 0.37, p < 0.0001), 95%CI: (0.19, 0.54) | Trivarate probit model▲★: Intervention: (β = 0.53, p < 0.0001), 95%CI: (0.32, 0.75) |
| n = 401 | n = 480 | |
| Have you received an IUD assessment service? ▽ | Quavarate probit model▲★: Intervention: (β = 0.51, p < 0.0001), 95%CI: (0.26, 0.75) | Quavariate probit model▼★: Intervention: (β = 0.46, p < 0.0001), 95%CI: (0.21, 0.71) |
| n = 2077 | n = 1631 | |
| Have you used condoms in the last three sexual encounters? ☆ | Heckprobit mode▲★: Intervention: (β = 0.16, p = 0.0052), 95%CI: (0.05, 0.27) | Heckprobit mode▲★: Intervention: (β = 0.37, p < 0.0001), 95%CI: (0.22, 0.51) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, S.-F.; Wu, J.-Q.; Yu, C.-N.; Li, Y.-Y.; Zhao, R.; Li, Y.-R.; Zhou, Y. The Effects of Comprehensive Sexual and Reproductive Health/Family Planning Intervention Based on Knowledge, Attitudes, and Practices Among the Domestic Migrant Population of Reproductive Age in China: A Randomized Community Study. Int. J. Environ. Res. Public Health 2020, 17, 2093. https://doi.org/10.3390/ijerph17062093
Xu S-F, Wu J-Q, Yu C-N, Li Y-Y, Zhao R, Li Y-R, Zhou Y. The Effects of Comprehensive Sexual and Reproductive Health/Family Planning Intervention Based on Knowledge, Attitudes, and Practices Among the Domestic Migrant Population of Reproductive Age in China: A Randomized Community Study. International Journal of Environmental Research and Public Health. 2020; 17(6):2093. https://doi.org/10.3390/ijerph17062093
Chicago/Turabian StyleXu, Shuang-Fei, Jun-Qing Wu, Chuan-Ning Yu, Yu-Yan Li, Rui Zhao, Yi-Ran Li, and Ying Zhou. 2020. "The Effects of Comprehensive Sexual and Reproductive Health/Family Planning Intervention Based on Knowledge, Attitudes, and Practices Among the Domestic Migrant Population of Reproductive Age in China: A Randomized Community Study" International Journal of Environmental Research and Public Health 17, no. 6: 2093. https://doi.org/10.3390/ijerph17062093