The Impact of Business Cycle on Health Financing: Subsidized, Voluntary and Out-of-Pocket Health Spending



Abstract
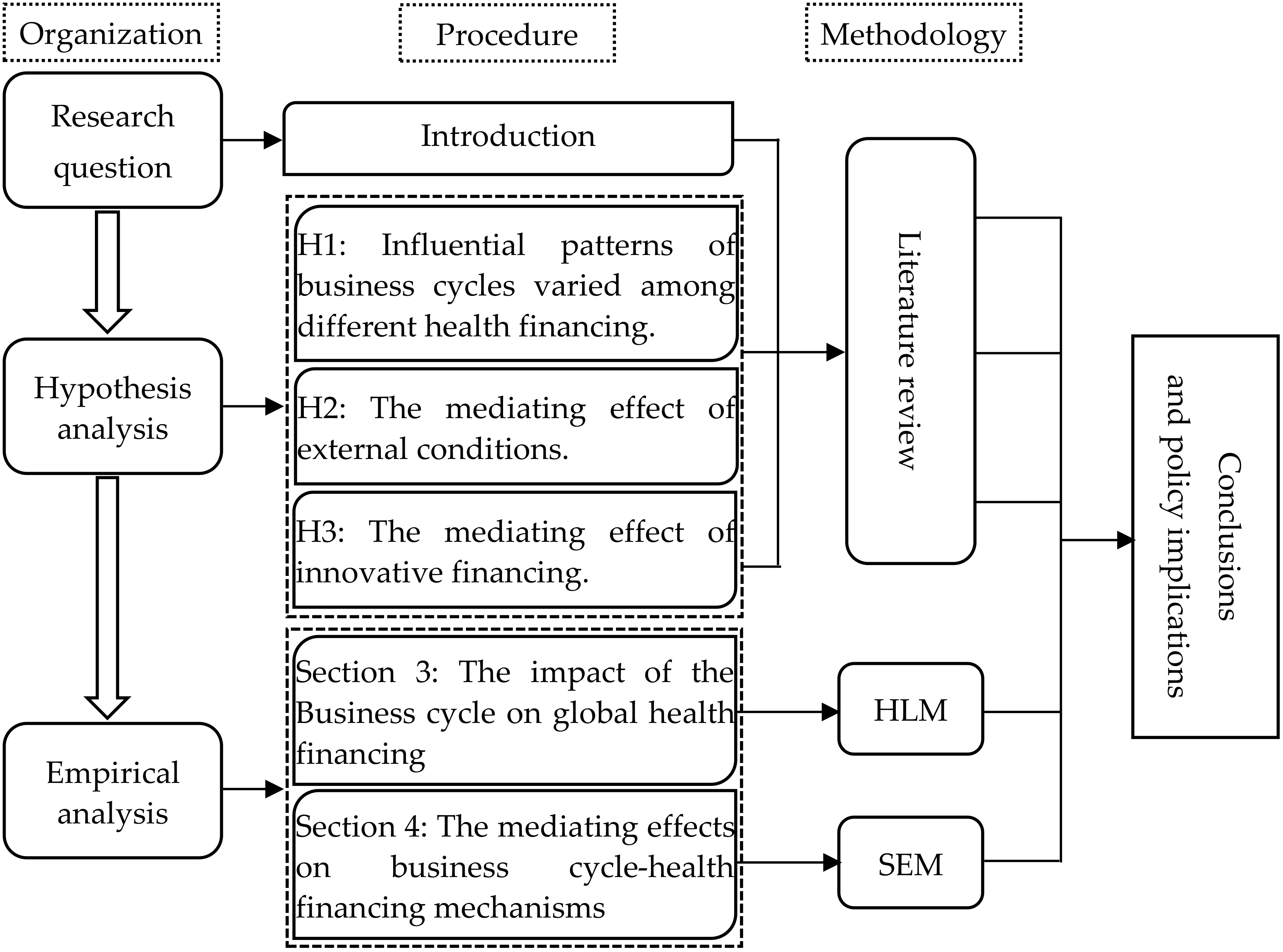
:1. Introduction
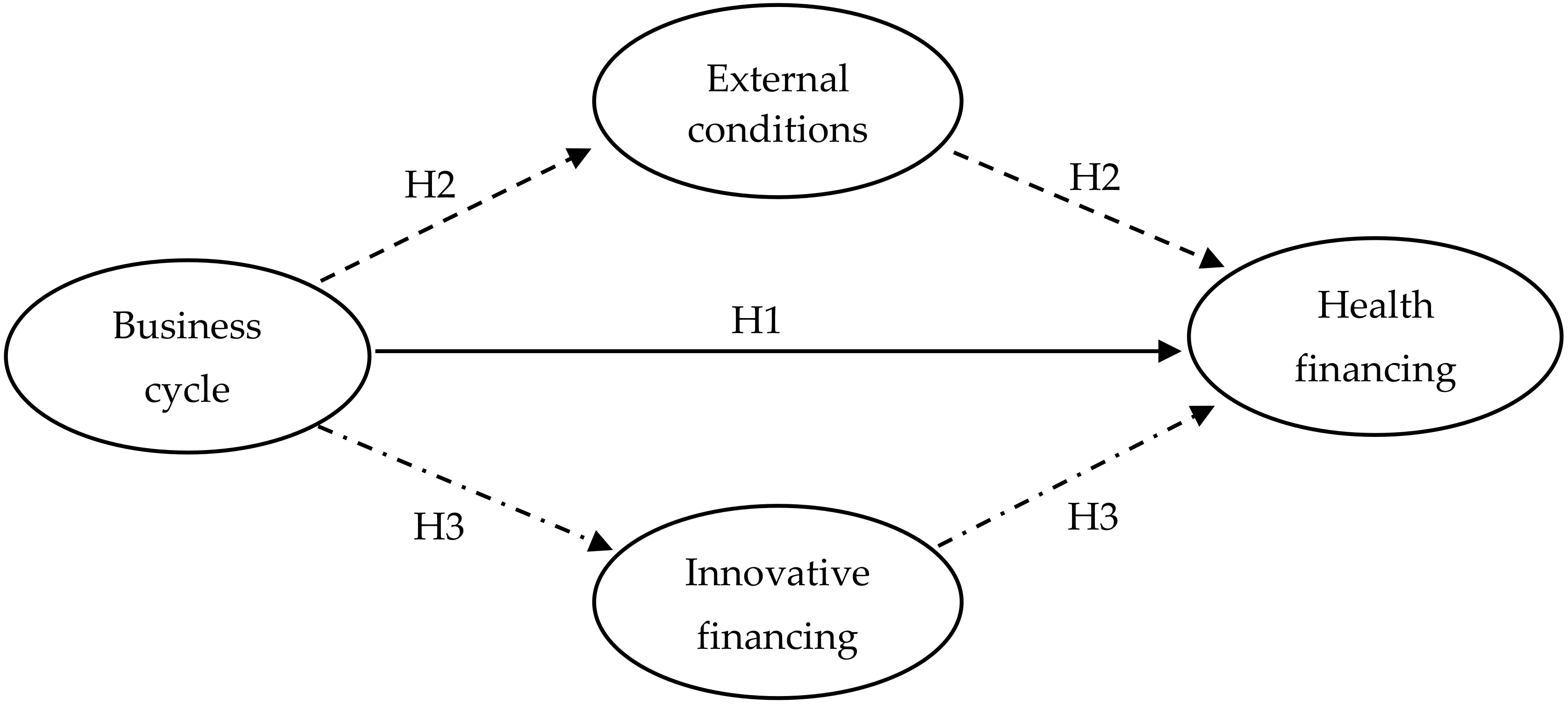
2. Research Hypothesis
3. The Impact of the Business Cycle on Global Health Financing
3.1. Hierarchical Linear Model
3.2. Data and Variables Selected
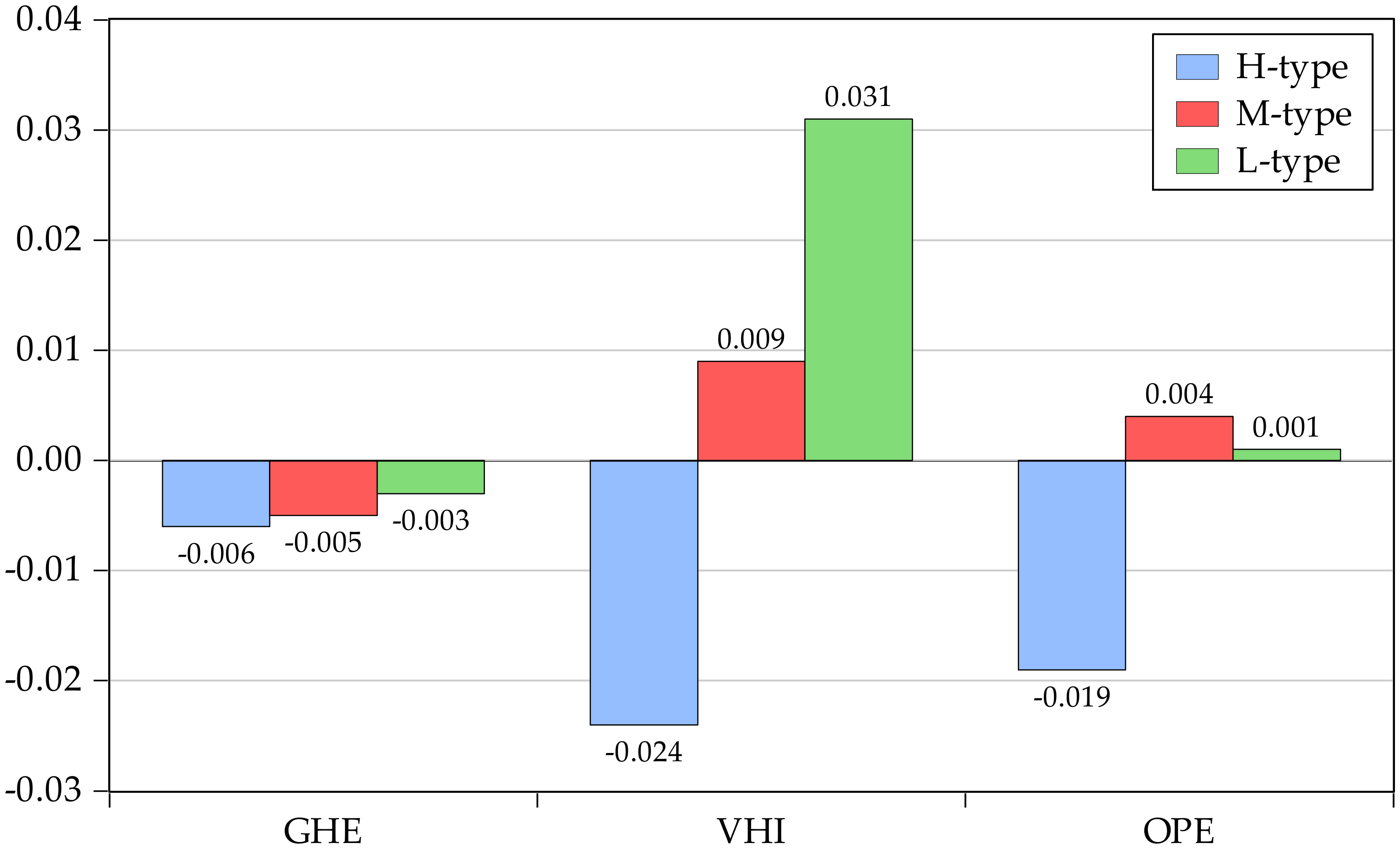
3.3. The Business Cycle Effects on Global Health Financing
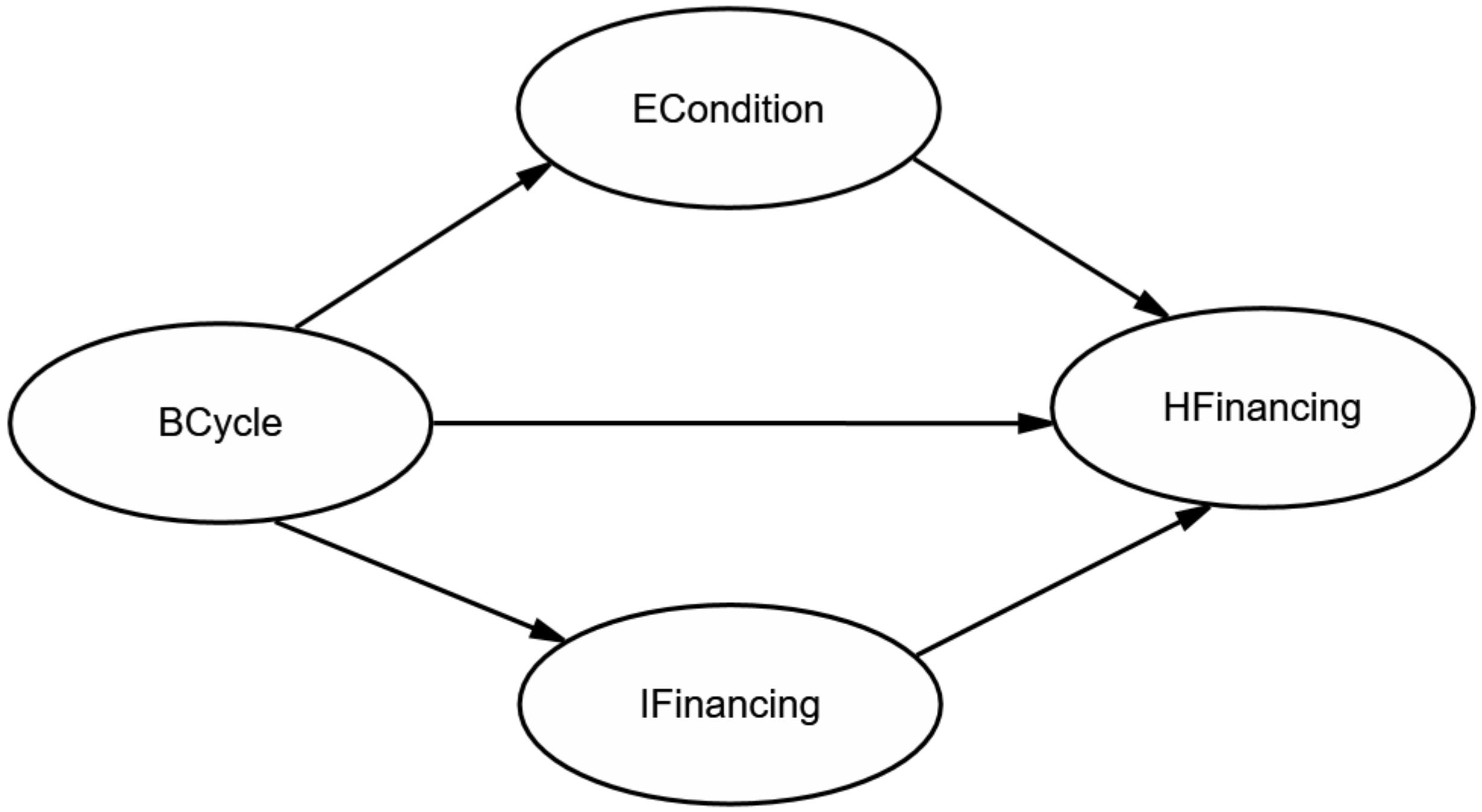
4. The Mediating Effects on Business Cycle-Health Financing Mechanisms
4.1. Research Design
4.1.1. Methods Selected
4.1.2. Model Conceptualization
4.1.3. Path Diagram Construction
4.1.4. Model Specification and Identification
4.1.5. Parameter Estimation
4.1.6. Assessment of Model Fit
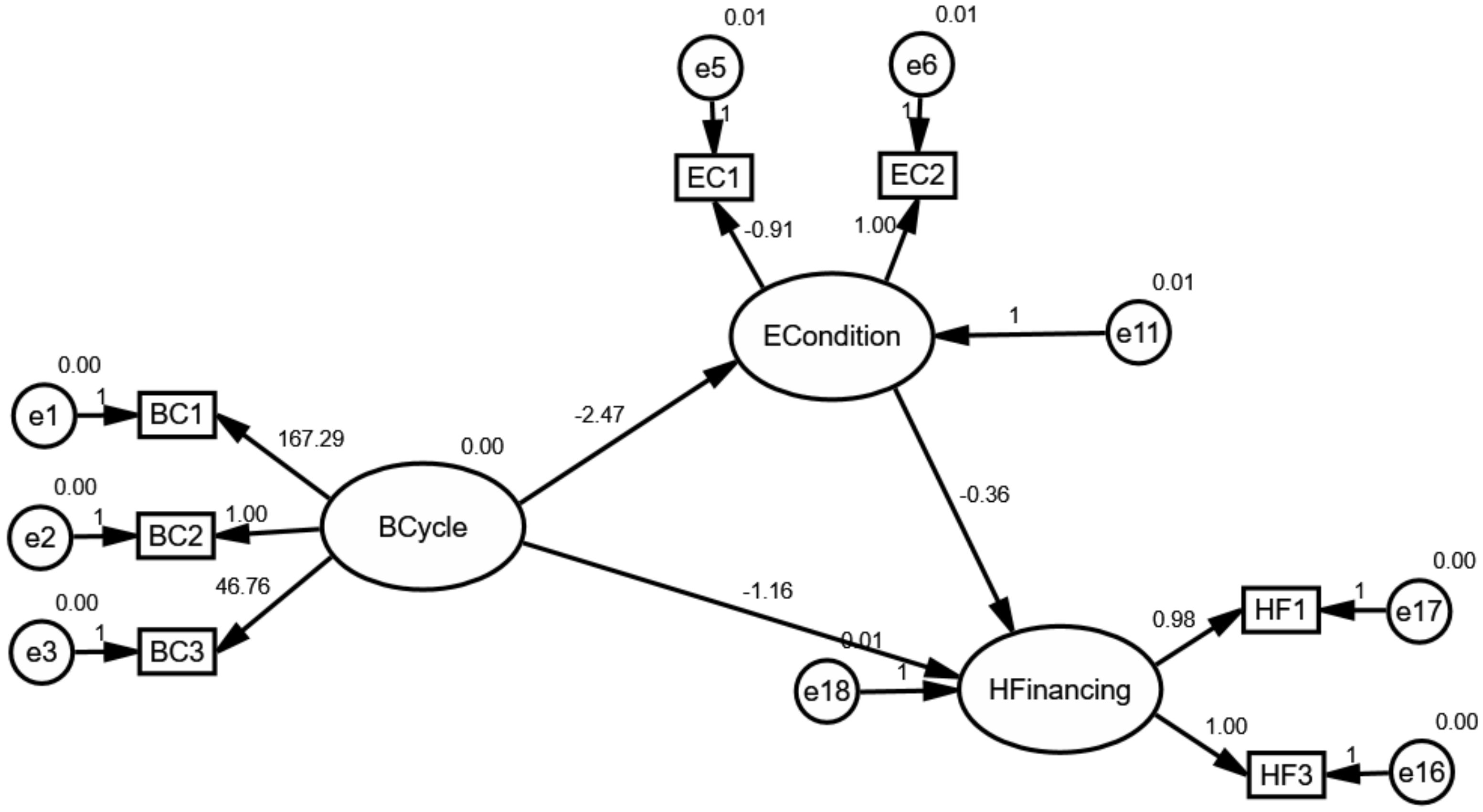
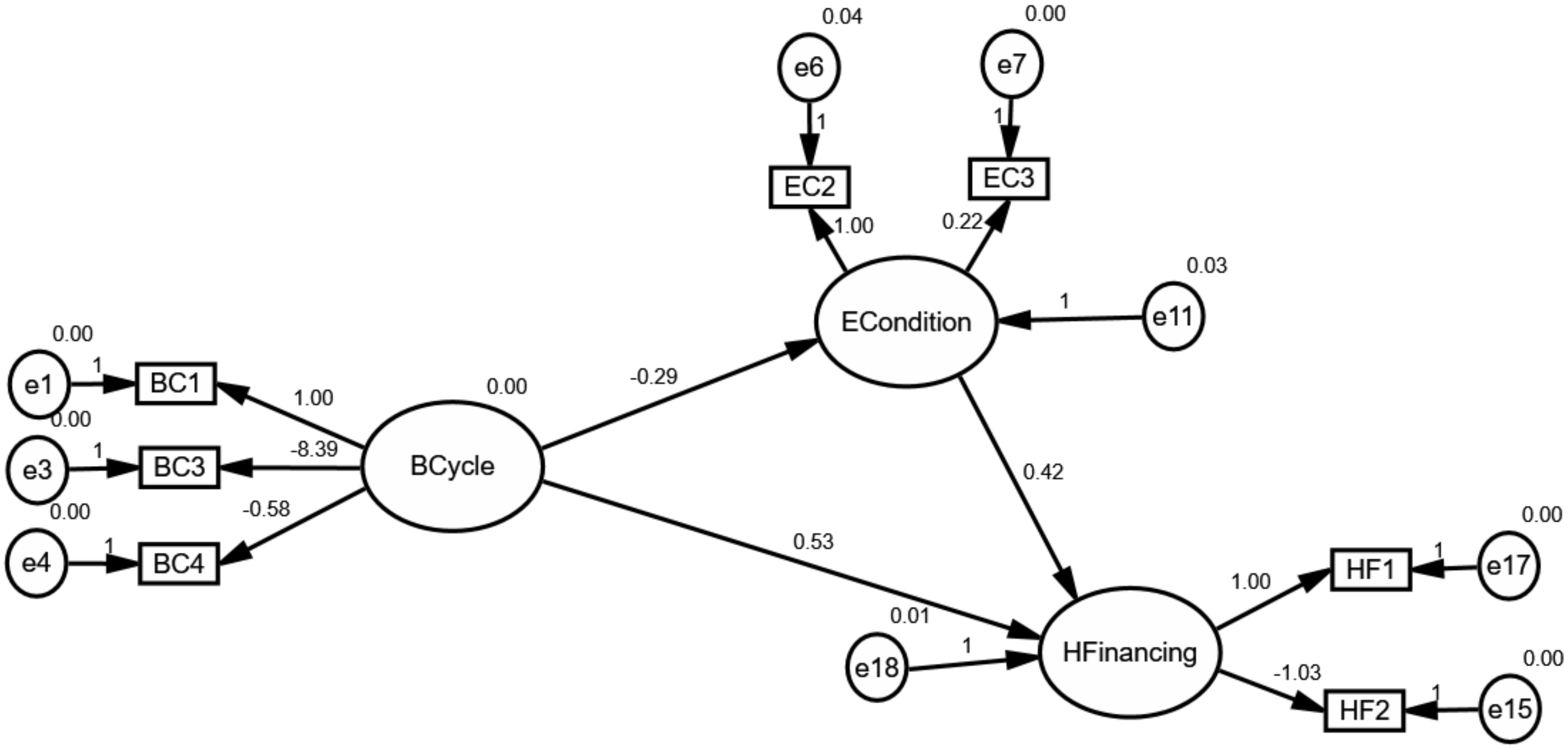
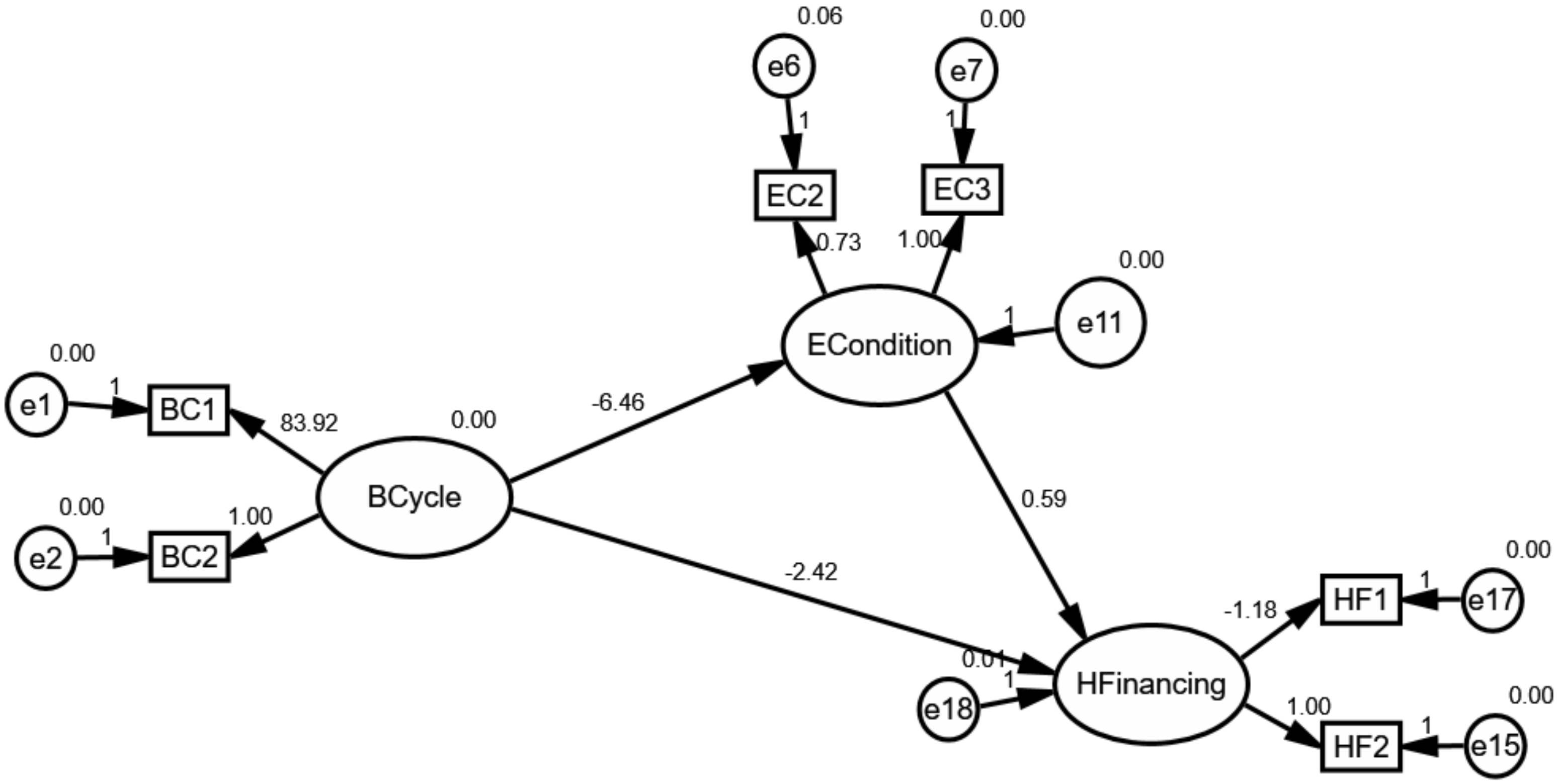
4.2. The Mediating Effect of External Conditions
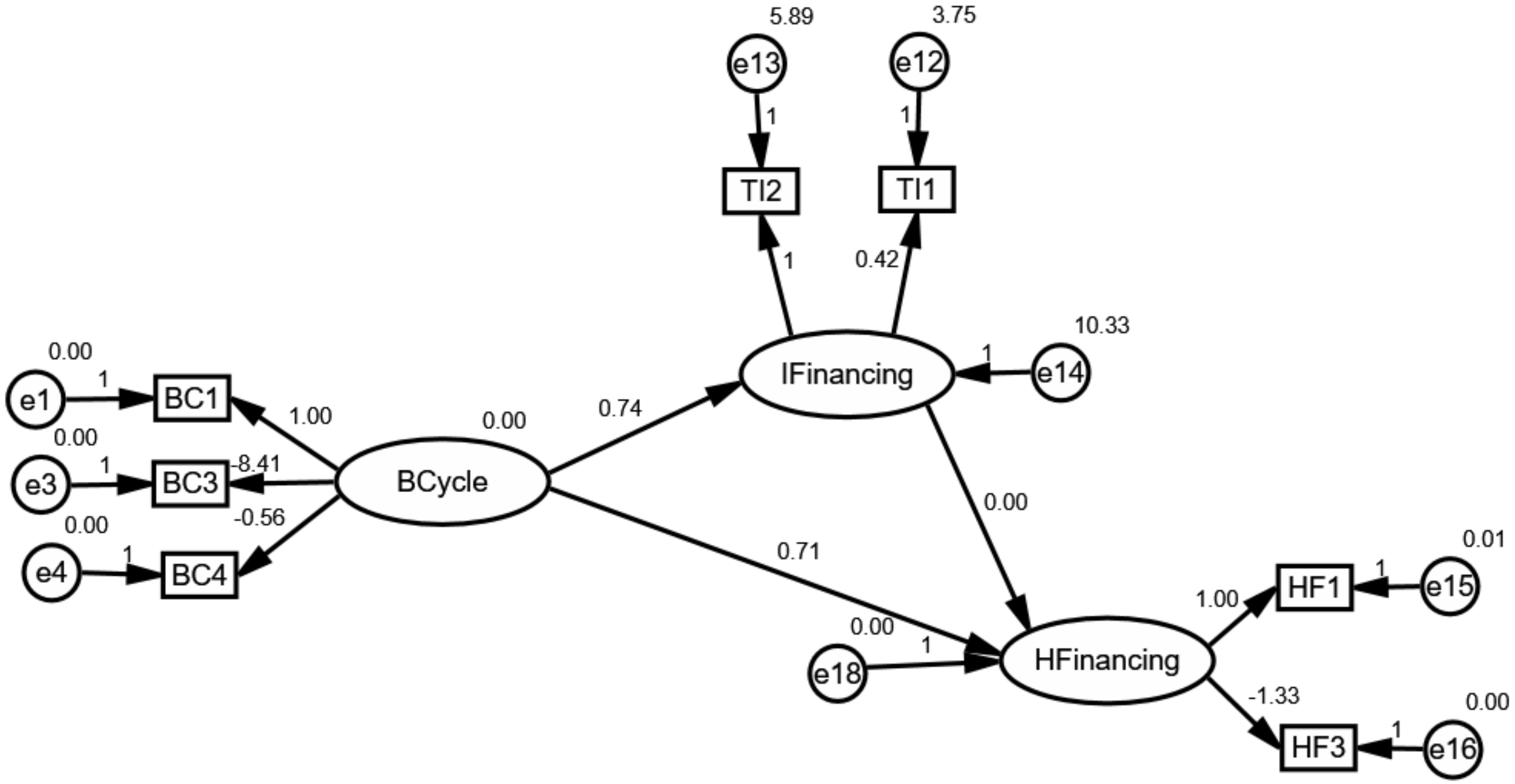
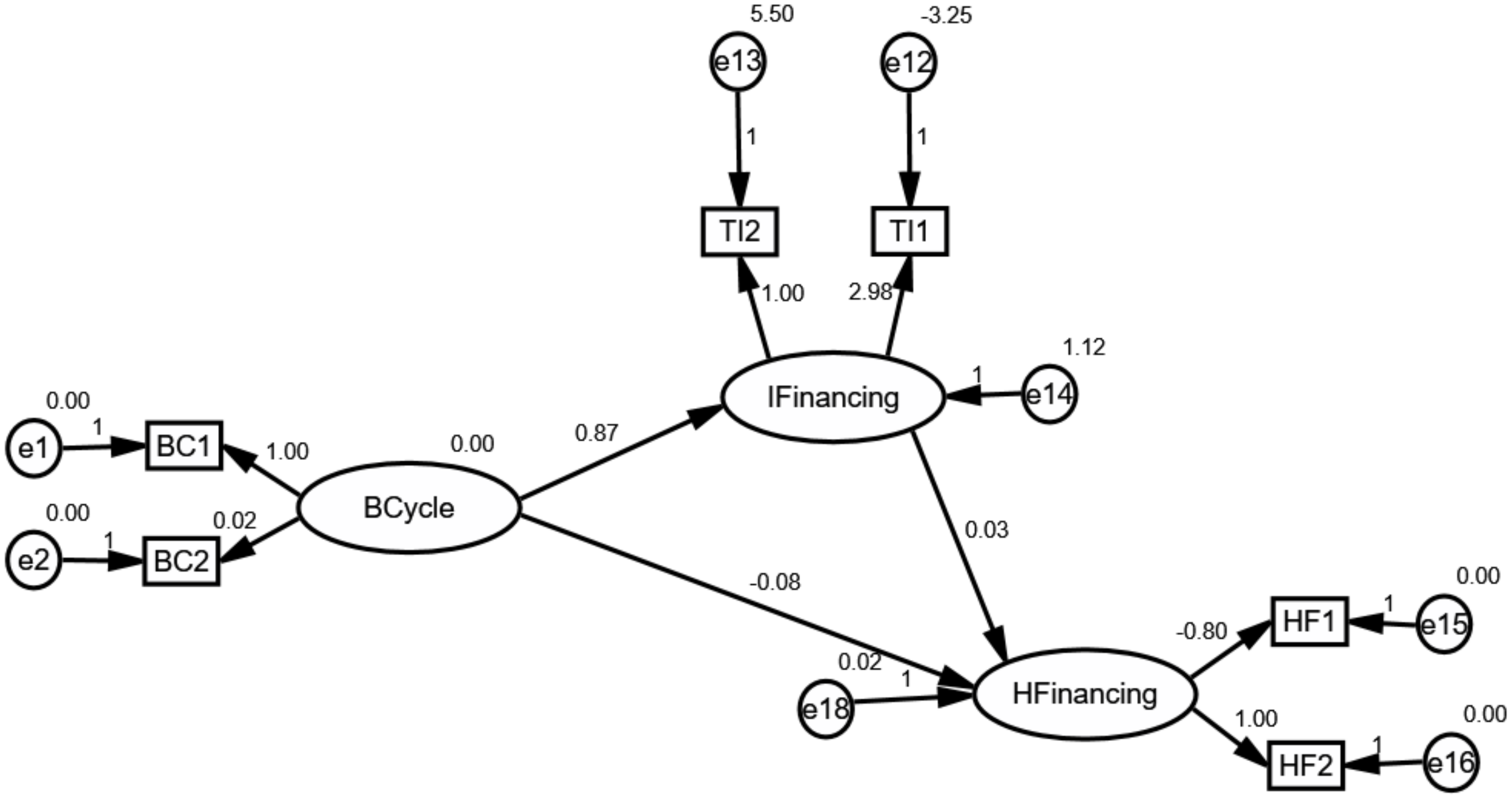
4.3. The Mediating Effect of Innovative Health Financing
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Full Results of the HLM

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Coef. | St. D | Statistic-Value | Prob. | |
|---|---|---|---|---|---|
| GHE | 0.661 | 0.029 | 23.14 | 0.000 | |
| −0.362 | 0.041 | −8.766 | 0.000 | ||
| −0.169 | 0.041 | −4.116 | 0.000 | ||
| 0.098 | 0.009 | 101,101.5 | 0.000 | ||
| −0.003 | 0.017 | −0.149 | 0.882 | ||
| −0.003 | 0.212 | −0.159 | 0.874 | ||
| −0.002 | 0.024 | −0.093 | 0.927 | ||
| 0.017 | 0.004 | 4.104 | 0.000 | ||
| 0.005 | 0.001 | 2.886 | 0.005 | ||
| 0.001 | 0.000 | 2.333 | 0.020 | ||
| 0.988 | 0.005 | 186.2 | 0.000 | ||
| VHI | 0.333 | 0.028 | 12.070 | 0.000 | |
| 0.351 | 0.039 | 8.811 | 0.000 | ||
| 0.175 | 0.039 | 4.391 | 0.000 | ||
| 0.095 | 0.009 | 71,782.03 | 0.000 | ||
| 0.031 | 0.020 | 1.504 | 0.133 | ||
| −0.055 | 0.024 | −2.246 | 0.025 | ||
| −0.022 | 0.027 | −0.804 | 0.422 | ||
| −0.034 | 0.005 | −6.162 | 0.000 | ||
| 0.021 | 0.007 | 3.042 | 0.003 | ||
| −0.004 | 0.002 | −2.036 | 0.042 | ||
| −0.001 | 0.001 | −1.850 | 0.064 | ||
| 0.066 | 0.019 | 3.489 | 0.001 | ||
| −1.021 | 0.006 | −165.1 | 0.000 | ||
| OPE | 0.237 | 0.023 | 10.353 | 0.000 | |
| 0.388 | 0.033 | 11.716 | 0.000 | ||
| 0.182 | 0.033 | 5.500 | 0.000 | ||
| 0.079 | 0.006 | 3306.75 | 0.000 | ||
| 0.001 | 0.077 | 0.016 | 0.987 | ||
| −0.020 | 0.094 | −0.211 | 0.833 | ||
| 0.003 | 0.105 | 0.028 | 0.978 | ||
| 0.049 | 0.023 | 2.119 | 0.034 | ||
| −0.020 | 0.007 | −2.597 | 0.010 | ||
| −0.744 | 0.024 | −31.481 | 0.000 |
References
- McIntyre, D.; Kutzin, J.; Organization, W.H. Health Financing Country Diagnostic: A Foundation for National Strategy Development; 9241510110; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Liaropoulos, L.; Goranitis, I. Health care financing and the sustainability of health systems. Int. J. Equity Health 2015, 14, 80. [Google Scholar] [CrossRef] [Green Version]
- Frasquilho, D.; Matos, M.G.; Salonna, F.; Guerreiro, D.; Storti, C.C.; Gaspar, T.; Caldas-de-Almeida, J.M. Mental health outcomes in times of economic recession: A systematic literature review. BMC Public Health 2016, 16, 115. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, V.M.; Grassi, B. Large Firm Dynamics and the Business Cycle. Am. Econ. Rev. 2019, 109, 1375–1425. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Palacio, I.; Carrera-Lasfuentes, P.; Rabanaque, M.J. Youth unemployment and economic recession in Spain: Influence on health and lifestyles in young people (16–24 years old). Int. J. Public Health 2015, 60, 427–435. [Google Scholar] [CrossRef]
- Watson, P.; Deller, S. Economic diversity, unemployment and the Great Recession. Q. Rev. Econ. Financ. 2017, 64, 1–11. [Google Scholar] [CrossRef]
- Ronda, E.; Briones-Vozmediano, E.; Galon, T.; Garcia, A.M.; Benavides, F.G.; Agudelo-Suarez, A.A. A qualitative exploration of the impact of the economic recession in Spain on working, living and health conditions: Reflections based on immigrant workers’ experiences. Health Expect. 2016, 19, 416–426. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A. Reflections on and alternatives to WHO’s fairness of financial contribution index. Health Econ. 2002, 11, 103–115. [Google Scholar] [CrossRef]
- McIntyre, D.; Thiede, M.; Dahlgren, G.; Whitehead, M. What are the economic consequences for households of illness and of paying for health care in low-and middle-income country contexts? Soc. Sci. Med. 2006, 62, 858–865. [Google Scholar] [CrossRef]
- Reyes-Heroles, R.; Tenorio, G. Regime-switching in emerging market business cycles: Interest rate volatility and sudden stops. J. Int. Money Financ. 2019, 93, 81–100. [Google Scholar] [CrossRef]
- Bitler, M.; Hoynes, H. Heterogeneity in the Impact of Economic Cycles and the Great Recession: Effects within and across the Income Distribution. Am. Econ. Rev. 2015, 105, 154–160. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Templin, T.; Sadat, N.; Reidy, P.; Chapin, A.; Foreman, K.; Haakenstad, A.; Evans, T.; Murray, C.J.L.; Kurowski, C. National spending on health by source for 184 countries between 2013 and 2040. Lancet 2016, 387, 2521–2535. [Google Scholar] [CrossRef]
- Uzochukwu, B.S.; Ughasoro, M.D.; Etiaba, E.; Okwuosa, C.; Envuladu, E.; Onwujekwe, O.E. Health care financing in Nigeria: Implications for achieving universal health coverage. Niger. J. Clin. Pract. 2015, 18, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Konstantinides, D.G. Ruin probabilities for a double renewal risk model with frequent premium arrivals. Quant. Financ. Econ. 2018, 2, 717–732. [Google Scholar] [CrossRef]
- Yamada, T.; Chen, C.C.; Murata, C.; Hirai, H.; Ojima, T.; Kondo, K.; Harris, J.R., III. Access disparity and health inequality of the elderly: Unmet needs and delayed healthcare. Int. J. Environ. Res. Public Health 2015, 12, 1745–1772. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.; Boerma, T.; Requejo, J.; Mesenburg, M.A.; Joseph, G.; Costa, J.C.; Vidaletti, L.P.; Ferreira, L.Z.; Hosseinpoor, A.R.; Barros, A.J. Analyses of inequalities in RMNCH: Rising to the challenge of the SDGs. BMJ Glob. Health 2019, 4, e001295. [Google Scholar] [CrossRef] [Green Version]
- Eslava-Schmalbach, J.; Garzón-Orjuela, N.; Elias, V.; Reveiz, L.; Tran, N.; Langlois, E. Conceptual framework of equity-focused implementation research for health programs (EquIR). Int. J. Equity Health 2019, 18, 80. [Google Scholar] [CrossRef]
- Spencer, N.; Raman, S.; O’Hare, B.; Tamburlini, G. Addressing inequities in child health and development: Towards social justice. BMJ Paediatr. Open 2019, 3, e000503. [Google Scholar] [CrossRef]
- Kankeu, H.T.; Boyer, S.; Fodjo Toukam, R.; Abu-Zaineh, M. How do supply-side factors influence informal payments for healthcare? The case of HIV patients in Cameroon. Int. J. Health Plan. Manag. 2016, 31, E41–E57. [Google Scholar] [CrossRef]
- Fujii, T. Sources of health financing and health outcomes: A panel data analysis. Health Econ. 2018, 27, 1996–2015. [Google Scholar] [CrossRef]
- Courtemanche, C.; Marton, J.; Ukert, B.; Yelowitz, A.; Zapata, D.; Fazlul, I. The three-year impact of the Affordable Care Act on disparities in insurance coverage. Health Serv. Res. 2019, 54, 307–316. [Google Scholar] [CrossRef]
- Cornell, P.Y.; Grabowski, D.C. The Impact of Policy Incentives on Long-Term Care Insurance and Medicaid Costs: Does Underwriting Matter? Health Serv. Res. 2018, 53, 3728–3749. [Google Scholar] [CrossRef]
- Cornell, P.Y.; Grabowski, D.C.; Cohen, M.; Shi, X.; Stevenson, D.G. Medical underwriting in long-term care insurance: Market conditions limit options for higher-risk consumers. Health Aff. 2016, 35, 1494–1503. [Google Scholar] [CrossRef] [Green Version]
- Htet, S.; Alam, K.; Mahal, A. Economic burden of chronic conditions among households in Myanmar: The case of angina and asthma. Health Policy Plan. 2015, 30, 1173–1183. [Google Scholar] [CrossRef] [Green Version]
- Sangar, S.; Dutt, V.; Thakur, R. Distress financing of out-of-pocket health expenditure in India. Rev. Dev. Econ. 2019, 23, 314–330. [Google Scholar] [CrossRef]
- Sangar, S.; Dutt, V.; Thakur, R. Economic burden, impoverishment, and coping mechanisms associated with out-of-pocket health expenditure in India: A disaggregated analysis at the state level. Int. J. Health Plan. Manag. 2019, 34, e301–e313. [Google Scholar] [CrossRef] [Green Version]
- Atun, R.; Silva, S.; Knaul, F.M. Innovative financing instruments for global health 2002–15: A systematic analysis. Lancet Glob. Health 2017, 5, e720–e726. [Google Scholar] [CrossRef] [Green Version]
- Atun, R.; Silva, S.; Ncube, M.; Vassall, A. Innovative financing for HIV response in sub-Saharan Africa. J. Glob. Health 2016, 6, 010407. [Google Scholar] [CrossRef]
- Thomas, S.; Keegan, C.; Barry, S.; Layte, R.; Jowett, M.; Normand, C. A framework for assessing health system resilience in an economic crisis: Ireland as a test case. BMC Health Serv. Res 2013, 13, 450. [Google Scholar] [CrossRef] [Green Version]
- Garber, A.M.; Phelps, C.E. Economic foundations of cost-effectiveness analysis. J. Health Econ. 1997, 16, 1–31. [Google Scholar] [CrossRef]
- Zhang, H.; An, R.; Zhong, Q. Anti-corruption, government subsidies, and investment efficiency. China J. Account. Res. 2019, 12, 113–133. [Google Scholar] [CrossRef]
- Huang, Z.; Liao, G.; Li, Z. Loaning scale and government subsidy for promoting green innovation. Technol. Forecast. Soc. Chang. 2019, 144, 148–156. [Google Scholar] [CrossRef]
- Reeves, A.; McKee, M.; Basu, S.; Stuckler, D. The political economy of austerity and healthcare: Cross-national analysis of expenditure changes in 27 European nations 1995–2011. Health Policy 2014, 115, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Giannakopoulos, G.; Anagnostopoulos, D.C. Child health, the refugees crisis, and economic recession in Greece. Lancet 2016, 387, 1271. [Google Scholar] [CrossRef] [Green Version]
- Begenau, J.; Salomao, J. Firm Financing over the Business Cycle. Rev. Financ. Stud. 2019, 32, 1235–1274. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.; Jung, Y.; Islam, A.; Pande, B.; Yao, L. The impact of the global recession on the health of the people in Asia. In Poverty and Sustainable Development in Asia Impacts and Responses to the Global Economic Crisis; Bauer, A., Thant, M., Bauer, A., Eds.; Asian Development Bank: Mandaluyong, Philippines, 2010; pp. 405–424. [Google Scholar]
- Rechel, B.; Suhrcke, M.; Tsolova, S.; Suk, J.E.; Desai, M.; McKee, M.; Stuckler, D.; Abubakar, I.; Hunter, P.; Senek, M. Economic crisis and communicable disease control in Europe: A scoping study among national experts. Health Policy 2011, 103, 168–175. [Google Scholar] [CrossRef]
- Arroyo, E.; Renart, G.; Saez, M. How the economic recession has changed the likelihood of reporting poor self-rated health in Spain. Int. J. Equity Health 2015, 14, 149. [Google Scholar] [CrossRef] [Green Version]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Bova, E.; Ruiz-Arranz, M.; Toscani, F.G.; Ture, H.E. The impact of contingent liability realizations on public finances. Int. Tax Public Financ. 2018, 26, 381–417. [Google Scholar] [CrossRef]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Stanaway, J.D. The global economic burden of dengue: A systematic analysis. Lancet Infect. Dis. 2016, 16, 935–941. [Google Scholar] [CrossRef]
- Li, Z.; Dong, H.; Huang, Z.; Failler, P. Asymmetric Effects on Risks of Virtual Financial Assets (VFAs) in different regimes: A Case of Bitcoin. Quant. Financ. Econ. 2018, 2, 860–883. [Google Scholar] [CrossRef]
- Massuda, A.; Hone, T.; Leles, F.A.G.; de Castro, M.C.; Atun, R. The Brazilian health system at crossroads: Progress, crisis and resilience. BMJ Glob. Health 2018, 3, e000829. [Google Scholar] [CrossRef] [Green Version]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Lakdawalla, D.N.; Doshi, J.A.; Garrison, L.P., Jr.; Phelps, C.E.; Basu, A.; Danzon, P.M. Defining elements of value in health care—A health economics approach: An ISPOR Special Task Force report [3]. Value Health 2018, 21, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Deller, S.; Watson, P. Did regional economic diversity influence the effects of the great recession? Econ. Inq. 2016, 54, 1824–1838. [Google Scholar] [CrossRef]
- McCoy, D.; Brikci, N. Taskforce on innovative international financing for health systems: What next? Bull. World Health Organ. 2010, 88, 478–480. [Google Scholar] [CrossRef]
- Albuquerque, M.V.d.; Viana, A.L.d.Á.; Lima, L.D.d.; Ferreira, M.P.; Fusaro, E.R.; Iozzi, F.L. Regional health inequalities: Changes observed in Brazil from 2000–2016. Cienc. Saude Coletiva 2017, 22, 1055–1064. [Google Scholar] [CrossRef] [Green Version]
- Chansa, C.; Sundewall, J.; Ostlund, N. Effect of currency exchange rate fluctuations on Aid Effectiveness in the Health Sector in Zambia. Health Policy Plan. 2018, 33, 811–820. [Google Scholar] [CrossRef]
- Howitt, P.; Darzi, A.; Yang, G.Z.; Ashrafian, H.; Atun, R.; Barlow, J.; Blakemore, A.; Bull, A.M.; Car, J.; Conteh, L. Technologies for global health. Lancet 2012, 380, 507–535. [Google Scholar] [CrossRef]
- Van Dusen, B.; Nissen, J. Modernizing use of regression models in physics education research: A review of hierarchical linear modeling. Phys. Rev. Phys. Educ. Res. 2019, 15, 020108. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.J.; Jin, Y.L.; Zhu, T.T. The health effects of individual characteristics and environmental factors in China: Evidence from the hierarchical linear model. J. Clean. Prod. 2018, 194, 554–563. [Google Scholar] [CrossRef]
- Dang, V.T.; Lin, C.S. Using hierarchical linear modeling to test the effect of overall strategic fit on firm performance in different industry. Chin. Manag. Stud. 2017, 11, 637–657. [Google Scholar] [CrossRef]
- Xiong, B.; Skitmore, M.; Xia, B. A critical review of structural equation modeling applications in construction research. Autom. Constr. 2015, 49, 59–70. [Google Scholar] [CrossRef] [Green Version]
- Bentler, P.M. Multivariate analysis with latent variables: Causal modeling. Annu. Rev. Psychol. 1980, 31, 419–456. [Google Scholar] [CrossRef]
- Qureshi, S.M.; Kang, C. Analysing the organizational factors of project complexity using structural equation modelling. Int. J. Proj. Manag. 2015, 33, 165–176. [Google Scholar] [CrossRef]
- Li, Z.; Liao, G.; Albitar, K. Does corporate environmental responsibility engagement affect firm value? The mediating role of corporate innovation. Bus. Strategy Environ. 2019. [Google Scholar] [CrossRef]
- Lopez-Valcarcel, B.G.; Barber, P. Economic Crisis, Austerity Policies, Health and Fairness: Lessons Learned in Spain. Appl. Health Econ. Health Policy 2017, 15, 13–21. [Google Scholar] [CrossRef] [Green Version]










| Nature of Variables | Variables | Abbr. | Measurement | Description | Source |
|---|---|---|---|---|---|
| Dependent variables | Government Health Expenditure | GHE | Domestic General Government Health Expenditure as % Current Health Expenditure | This indicator depicts that governments give subsidy to healthcare systems. | GHE database |
| private prepaid plans | VHI | Voluntary Financing Arrangements as % of Current Health Expenditure | This shows the voluntary prepayment schemes to healthcare systems. | GHE database | |
| Out-of-Pocket Expenditure | OPE | Out-of-pocket as % of Current Health Expenditure | This highlights the importance of assessing the extent of financial protection in healthcare systems. | GHE database | |
| Explanatory variable | Business Cycle | BC | Real GDP | This variable reflects the economic operation within a country. | IFS database |
| Control variables | Under Five Mortality rate | UNF | Mortality rate, under-5 (per 1,000 live births) | This indicator concerns about the global monitoring of child mortality. | WDI database |
| People using safely managed sanitation services | SER | People using safely managed sanitation services (% of population) | This indicator indicates the percentage of people using improved sanitation facilities that are not shared with other households and where excreta are safely disposed of in situation or transported and treated offsite. | WDI database | |
| Government Effectiveness | GOV | Government Effectiveness | This indicator represents a proxy for the quality of government. | WGI database | |
| Unemployment | UEM | Unemployment, total (% of total labor force) | This indicator is of critical importance in measuring the (in)ability of workers to readily obtain gainful work within a country. | WDI database | |
| Patent applications | TEC | Patent applications, residents | Patent applications are worldwide patent applications filed through the Patent Cooperation Treaty procedure or with a national patent office for exclusive rights for an invention-a product or process that provides a new way of doing something or offers a new technical solution to a problem. | WDI database | |
| Compulsory Financing Arrangements | SW | Compulsory Financing Arrangements as % of Current Health Expenditure | This reflects inadequate financing and resource misallocation in healthcare systems. | GHE database 1 |
| Categories | Rank | Abbr. | Country Lists |
|---|---|---|---|
| High OPE | 1–11 | H | Armenia, Azerbaijan, Bangladesh, Ecuador, Egypt, Georgia, Guatemala, Morocco, Iran, Pakistan, Philippines |
| Middle OPE | 12–22 | M | Bosnia and Herzegovina, China, Korea, Malaysia, Mexico, Paraguay, Peru, Singapore, Tunisia, Uzbekistan, Venezuela |
| Low OPE | 23–34 | L | Algeria, Belarus, Brazil, Jordan, Kazakhstan, Mongolia, New Zealand, Norway, Russian Federation, Saudi Arabia, United Kingdom, United States 2 |
| Parameters | Coef. | St. D | t-Value | Prob. | |
|---|---|---|---|---|---|
| GHE | 0.661 | 0.029 | 23.14 | 0.000 | |
| −0.362 | 0.041 | −8.766 | 0.000 | ||
| −0.169 | 0.041 | −4.116 | 0.000 | ||
| −0.003 | 0.017 | −0.149 | 0.882 | ||
| −0.003 | 0.212 | −0.159 | 0.874 | ||
| −0.002 | 0.024 | −0.093 | 0.927 | ||
| C.V. | YES | ||||
| Sum. | H | −0.006 | |||
| M | −0.005 | ||||
| L | −0.003 | ||||
| VHI | 0.333 | 0.028 | 12.070 | 0.000 | |
| 0.351 | 0.039 | 8.811 | 0.000 | ||
| 0.175 | 0.039 | 4.391 | 0.000 | ||
| 0.031 | 0.020 | 1.504 | 0.133 | ||
| −0.055 | 0.024 | −2.246 | 0.025 | ||
| −0.022 | 0.027 | −0.804 | 0.422 | ||
| C.V | YES | ||||
| Sum. | H | −0.024 | |||
| M | 0.009 | ||||
| L | 0.031 | ||||
| OPE | 0.237 | 0.023 | 10.353 | 0.000 | |
| 0.388 | 0.033 | 11.716 | 0.000 | ||
| 0.182 | 0.033 | 5.500 | 0.000 | ||
| 0.001 | 0.077 | 0.016 | 0.987 | ||
| −0.020 | 0.094 | −0.211 | 0.833 | ||
| 0.003 | 0.105 | 0.028 | 0.978 | ||
| C.V. | YES | ||||
| Sum. | H | −0.019 | |||
| M | 0.004 | ||||
| L | 0.001 3 | ||||
| Latent Variables | Observed Variables | Abbr. | Source |
|---|---|---|---|
| Business cycle (BCycle) |
| BC1 | IFS database |
| BC2 | IFS database | |
| BC3 | IFS database | |
| BC4 | IFS database | |
| External conditions (ECondition) |
| EC1 | WDI database |
| EC2 | WDI database | |
| EC3 | WDI database | |
| EC4 | GHE database | |
| Innovative financing (IFinancing) |
| IF1 | WDI database |
| IF2 | UNESCO database | |
| Health financing (HFinancing) |
| HF1 | GHE database |
| HF2 | GHE database | |
| HF3 | GHE database |
| Model | Prob. | RMSEA (0 to 0.1) | ECVI | NCP | PGFI (>0.5) | CFI (>0.9) | |
|---|---|---|---|---|---|---|---|
| H1 | 2.781 | 0.993 | 0.000 | 0.198 [0.242, 0.242] | 0.000 [0, 0.000] | 0.391 | 1.000 |
| H2 | 5.643 | 0.896 | 0.000 | 0.213 [0.242, 0.255] | 0.000 [0, 2.405] | 0.390 | 1.000 |
| M1 | 2.702 | 0.994 | 0.000 | 0.197 [0.242, 0.242] | 0.000 [0, 0.000] | 0.391 | 1.000 |
| M2 | 0.911 | 1.000 | 0.026 | 0.188 [0.242, 0.242] | 0.000 [0, 0.000] | 0.392 | 1.000 |
| L1 | 0.795 | 0.992 | 0.000 | 0.167 [0.177, 0.177] | 0.000 [0, 0.000] | 0.284 | 1.000 |
| L2 | 0.842 | 0.991 | 0.000 | 0.152 [0.177, 0.177] | 0.000 [0, 0.000] | 0.285 | 1.000 5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, H.; Li, Z.; Failler, P. The Impact of Business Cycle on Health Financing: Subsidized, Voluntary and Out-of-Pocket Health Spending. Int. J. Environ. Res. Public Health 2020, 17, 1928. https://doi.org/10.3390/ijerph17061928
Dong H, Li Z, Failler P. The Impact of Business Cycle on Health Financing: Subsidized, Voluntary and Out-of-Pocket Health Spending. International Journal of Environmental Research and Public Health. 2020; 17(6):1928. https://doi.org/10.3390/ijerph17061928
Chicago/Turabian StyleDong, Hao, Zhenghui Li, and Pierre Failler. 2020. "The Impact of Business Cycle on Health Financing: Subsidized, Voluntary and Out-of-Pocket Health Spending" International Journal of Environmental Research and Public Health 17, no. 6: 1928. https://doi.org/10.3390/ijerph17061928