Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Projects
2.2. Design, Measures and Data Processing
2.3. Categorising Wellbeing Scores
2.4. Creating a Single Variable for Analyses
2.5. Statistical Analysis
3. Results
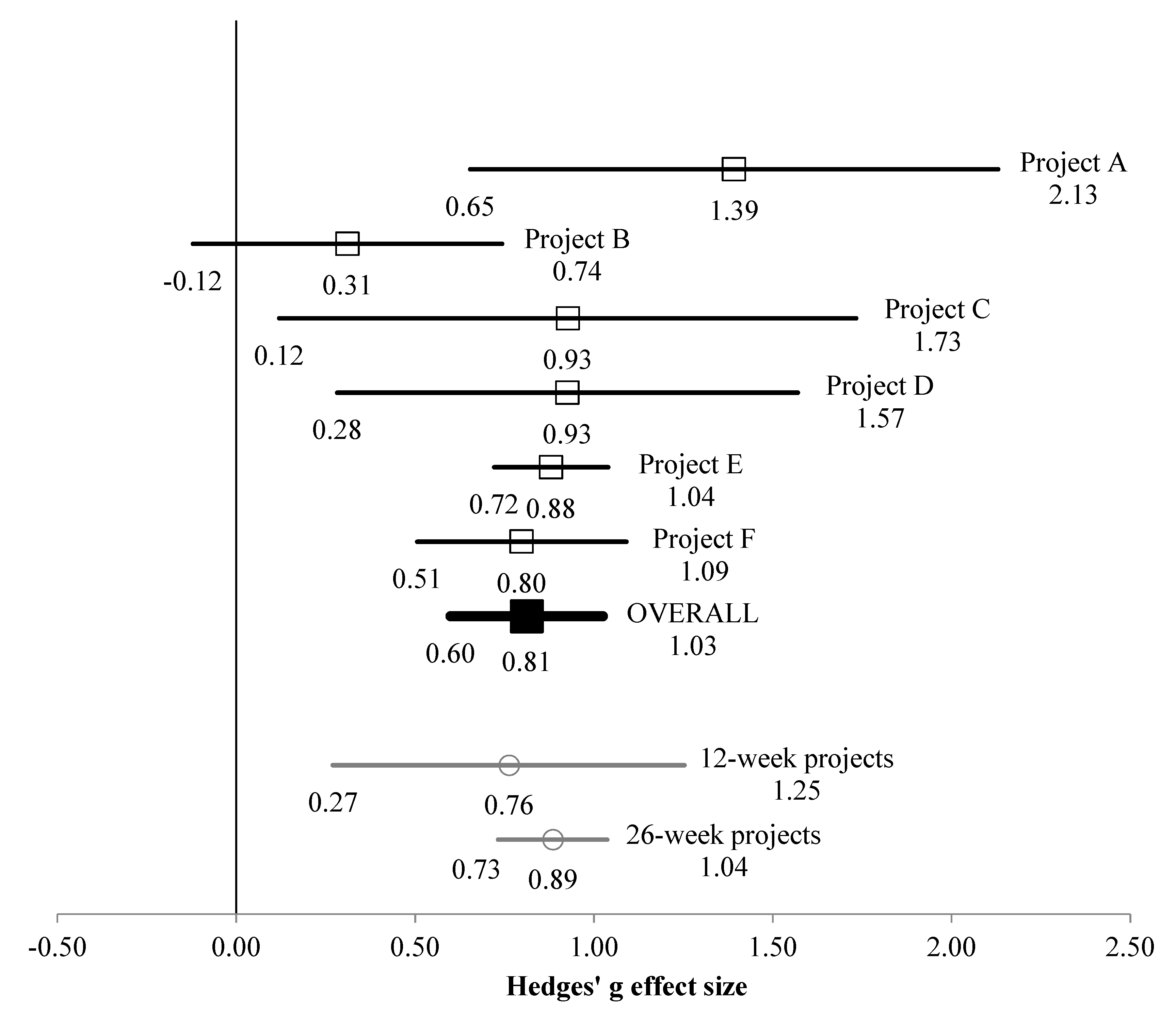
3.1. Whole Sample
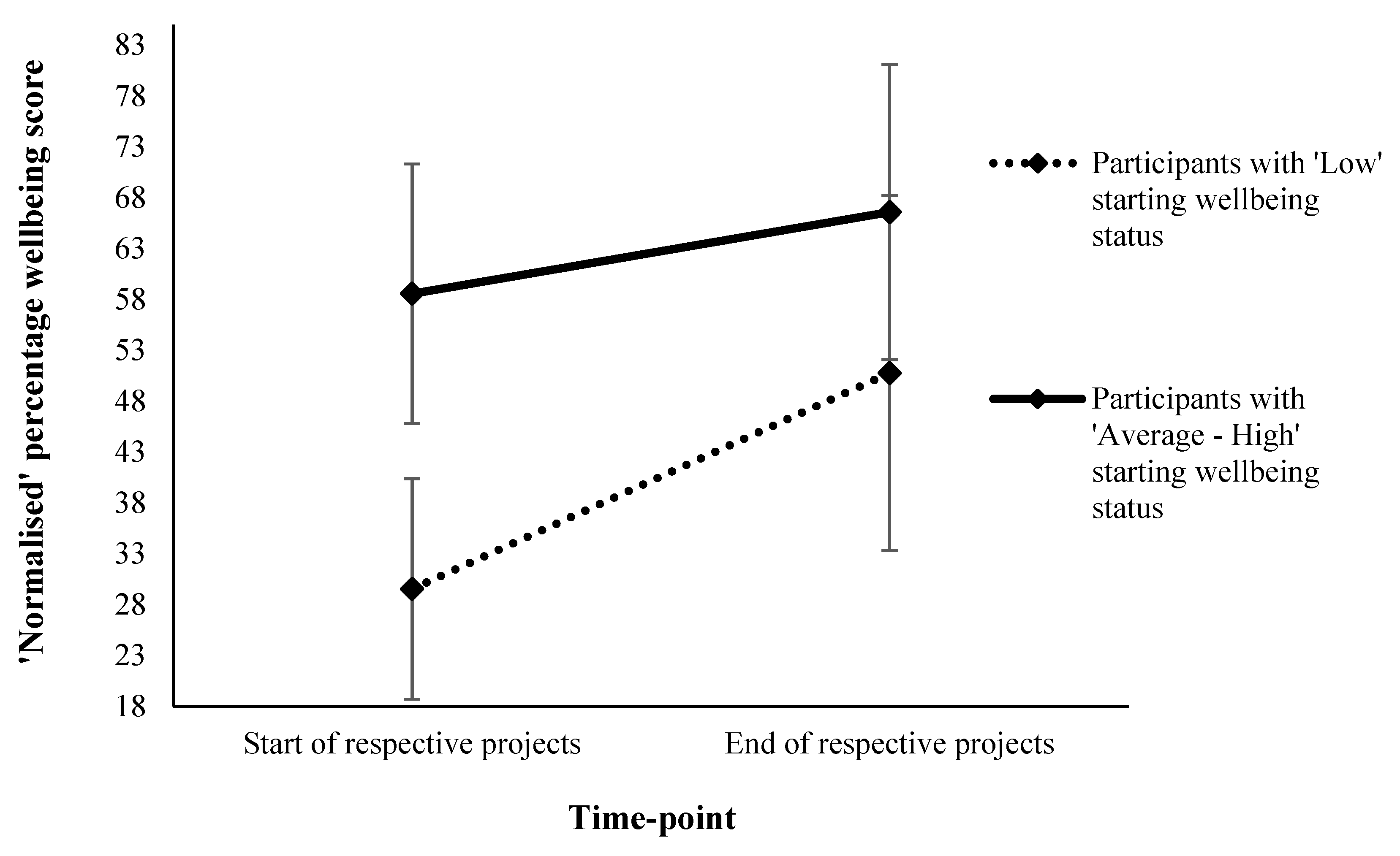
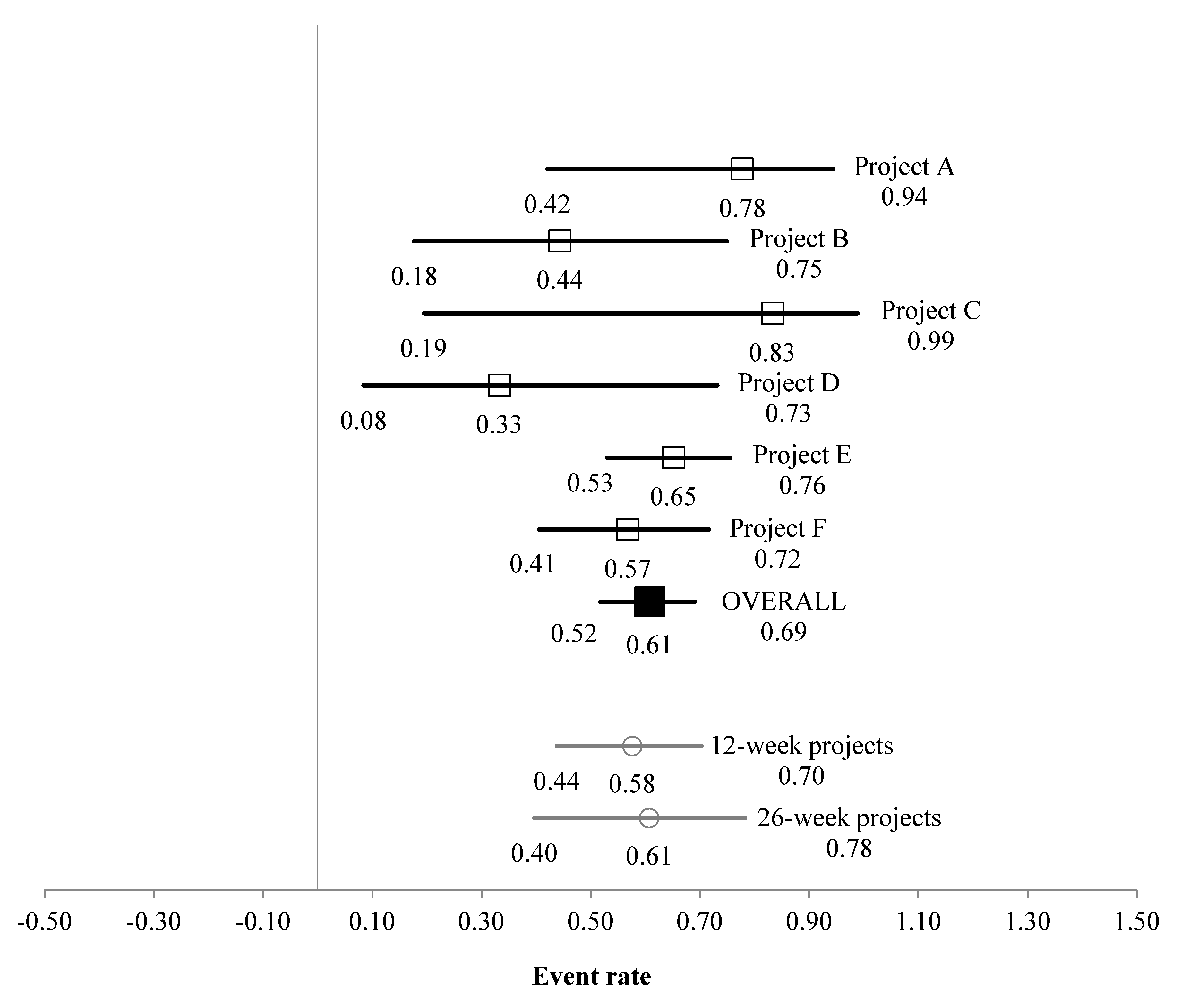
3.2. Low Wellbeing Subsample
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The mental and physical health outcomes of green exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Barton, J.; Bragg, R.; Wood, C.; Pretty, J. Green Exercise: Linking Nature, Health and Well-Being; Routledge: Abingdon, UK, 2016. [Google Scholar]
- Rogerson, M.; Brown, D.K.; Sandercock, G.; Wooller, J.J.; Barton, J. A comparison of four typical green exercise environments and prediction of psychological health outcomes. Perspect. Public Health 2015, 136, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [Green Version]
- Wood, C.J.; Pretty, J.; Griffin, M. A case–control study of the health and well-being benefits of allotment gardening. J. Public Health 2015, 38. [Google Scholar] [CrossRef]
- Brown, D.K.; Barton, J.L.; Gladwell, V.F. Viewing nature scenes positively affects recovery of autonomic function following acute-mental stress. Environ. Sci. Technol. 2013, 47, 5562–5569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, J.; Bragg, R.; Pretty, J.; Roberts, J.; Wood, C. The wilderness expedition an effective life course intervention to improve young people’s well-being and connectedness to nature. J. Exp. Educ. 2016. [Google Scholar] [CrossRef]
- Norton, C.L.; Tucker, A.; Russell, K.C.; Bettmann, J.E.; Gass, M.A.; Gillis, H.L.; Behrens, E. Adventure therapy with youth. J. Exp. Educ. 2014, 37, 46–59. [Google Scholar] [CrossRef]
- de Bruin, S.R.; Stoop, A.; Molema, C.C.; Vaandrager, L.; Hop, P.J.; Baan, C.A. Green care farms an innovative type of adult day service to stimulate social participation of people with dementia. Gerontol. Geriatr. Med. 2015, 1. [Google Scholar] [CrossRef] [Green Version]
- Vella, E.J.; Milligan, B.; Bennett, J.L. Participation in outdoor recreation program predicts improved psychosocial well-being among veterans with post-traumatic stress disorder: A pilot study. Mil. Med. 2013, 178, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamers, S.M.; Bolier, L.; Westerhof, G.J.; Smit, F.; Bohlmeijer, E.T. The impact of emotional well-being on long-term recovery and survival in physical illness: A meta-analysis. J. Behav. Med. 2012, 35, 538–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Neve, J.E.; Diener, E.; Tay, L.; Xuereb, C. The objective benefits of subjective well-being (6 August 2013). In World Happiness Report 2013; Helliwell, J., Layard, R., Sachs, J., Eds.; UN Sustainable Development Solutions Network: New York, NY, USA, 2013. [Google Scholar]
- Eurofound. European Quality of Life Survey 2016: Quality of Life, Quality of Public Services, and Quality of Society; Publications Office of the European Union: Luxembourg, 2017. [Google Scholar]
- Rogerson, M.; Barton, J.; Pretty, J.; Gladwell, V. The green exercise concept: Two intertwining pathways to health and well-being. In Physical Activity in Natural Settings: Green Exercise and Blue Mind; MacIntyre, T.E., Donnelly, A.A., Eds.; Routledge: Abingdon upon Thames, UK, in press.
- Brymer, E.; Davids, K.; Mallabon, L. Understanding the psychological health and well-being benefits of physical activity in nature: An ecological dynamics analysis. Ecopsychology 2014, 6, 189–197. [Google Scholar]
- Flowers, E.P.; Freeman, P.; Gladwell, V.F. A cross-sectional study examining predictors of visit frequency to local green space and the impact this has on physical activity levels. BMC Public Health 2016, 16, 420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [Google Scholar] [CrossRef]
- Roe, J.; Aspinall, P. The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place 2011, 17, 103–113. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Lachowycz, K.; Jones, A. Greenspace and obesity: A systematic review of the evidence. Obes. Rev. 2011, 12, e183–e189. [Google Scholar] [CrossRef]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- de Vries, S.; van Dillen, S.M.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef]
- van den Berg, M.M.; van Poppel, M.; van Kamp, I.; Ruijsbroek, A.; Triguero-Mas, M.; Gidlow, C.; Nieuwenhuijsen, M.J.; Gražulevičiene, R.; van Mechelen, W.; Kruize, H. Do physical activity, social cohesion, and loneliness mediate the association between time spent visiting green space and mental health? Environ. Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- McManus, S.; Bebbington, P.; Jenkins, R.; Brugha, T. Mental health and wellbeing in England: Adult psychiatric morbidity survey 2014; NHS Digital: Leeds, UK, 2016. [Google Scholar]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The warwick-edinburgh mental well-being scale (wemwbs): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fat, L.N.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and establishing national norms for mental wellbeing using the short warwick–edinburgh mental well-being scale (swemwbs): Findings from the health survey for england. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the warwick-edinburgh mental well-being scale (wemwbs): A rasch analysis using data from the scottish health education population survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.; Higgins, J.; Altman, D. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 [Updated March 2011]; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1988; Volume 13. [Google Scholar]
- Hedges, L.V. Distribution theory for glass’s estimator of effect size and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: San Diego, CA, USA, 1985. [Google Scholar]
- Funder, D.C.; Ozer, D.J. Evaluating effect size in psychological research: Sense and nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ Br. Med. J. 2003, 327, 557. [Google Scholar] [CrossRef] [Green Version]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening is beneficial for health: A meta-analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef]
- Clatworthy, J.; Hinds, J.; Camic, P.M. Gardening as a mental health intervention: A review. Ment. Health Rev. J. 2013. [Google Scholar] [CrossRef]
- Dodich, A.; Zollo, M.; Crespi, C.; Cappa, S.F.; Laureiro Martinez, D.; Falini, A.; Canessa, N. Short-term sahaja yoga meditation training modulates brain structure and spontaneous activity in the executive control network. Brain Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.; Romero, V.L.; Elkin-Frankston, S.; Bezdek, M.A.; Schumacher, E.H.; Lazar, S.W. Reduced interference in working memory following mindfulness training is associated with increases in hippocampal volume. Brain Imaging Behav. 2018, 13, 1–11. [Google Scholar]
- Christie, M.A.; Cole, F. The impact of green exercise on volunteer’s mental health and wellbeing-findings from a community project in a woodland setting. J. Ther. Hortic. 2017, 27, 16–32. [Google Scholar] [CrossRef]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C. Green spaces and general health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovell, R.; Husk, K.; Cooper, C.; Stahl-Timmins, W.; Garside, R. Understanding how environmental enhancement and conservation activities may benefit health and wellbeing: A systematic review. BMC Public Health 2015, 15, 864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, J.; Van Dillen, S.M.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Scale | Project | Sample Size | Mean Raw/Metric-Converted Scores for Respective Scale * | Normalised Percentage Scores | |||
|---|---|---|---|---|---|---|---|
| Start of Intervention | End of Intervention | Start of Intervention | End of Intervention | ||||
| Whole sample | WEMWBS (14–70) | A | 13 | 33.3 ± 12.2 | 46.2 ± 9.0 | 34.5 ± 21.7 | 57.4 ± 16.2 |
| C | 7 | 39.6 ± 12.8 | 57.9 ± 10.1 | 45.7 ± 22.9 | 78.3 ± 18.1 | ||
| D | 12 | 36.0 ± 5.7 | 43.4 ± 6.2 | 39.3 ± 10.2 | 52.5 ± 11.1 | ||
| F | 58 | 35.5 ± 13.1 | 45.6 ± 10.6 | 38.3 ± 23.4 | 56.4 ± 18.8 | ||
| SWEMWBS (7–35) | B | 20 | 19.4 ± 2.7 | 20.5 ± 3.5 | 44.3 ± 9.6 | 48.3 ± 12.6 | |
| E | 208 | 21.2 ± 4.7 | 24.5 ± 4.8 | 50.6 ± 16.6 | 62.4 ± 17.0 | ||
| Low wellbeing subsample | WEMWBS (14–70) | A | 9 | 27.0 ± 6.0 | 43.9 ± 6.6 | 23.2 ± 10.6 | 53.4 ± 11.8 |
| C | 2 | 23.0 ± 1.4 | 61.5 ± 12.0 | 16.1 ± 2.5 | 84.8 ± 21.5 | ||
| D | 6 | 30.8 ± 2.1 | 40.7 ± 7.2 | 30.1 ± 3.8 | 47.6 ± 12.9 | ||
| F | 37 | 27.2 ± 7.1 | 42.2 ± 10.3 | 23.6 ± 12.7 | 50.3 ± 18.3 | ||
| SWEMWBS (7–35) | B | 9 | 16.9 ± 1.3 | 19.1 ± 4.3 | 35.4 ± 4.5 | 43.3 ± 15.3 | |
| E | 66 | 16.3 ± 2.4 | 21.3 ± 4.9 | 33.3 ± 8.6 | 50.9 ± 17.4 | ||
| Test of Null (2-Tailed) | Heterogeneity between Projects/for Respective Moderator | Tau2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Z | P | Q | df (Q) | P | I2 | Tau2 | SE | Variance | ||
| Whole sample | Overall (in relation to Hedges g effect size) | 7.463 | <0.001 | 8.343 | 5 | 0.138 | 40.07 | 0.025 | 0.043 | 0.002 |
| Moderator effect for project duration | - | - | 0.215 | 1 | 0.643 | - | - | - | - | |
| 12 weeks | 3.053 | 0.002 | - | - | - | - | - | - | - | |
| 26 weeks | 11.393 | <0.001 | - | - | - | - | - | - | - | |
| Including moderator of wellbeing scale version | - | - | 1.086 | 1 | 0.297 | - | - | - | - | |
| WEMWBS | 7.287 | <0.001 | - | - | - | - | - | - | - | |
| SWEMWBS | 2.240 | 0.025 | - | - | - | - | - | - | - | |
| Low wellbeing subsample | Overall (in relation to Event Rate) | 2.345 | 0.019 | 5.060 | 5 | 0.409 | 1.19 | 0.003 | 0.169 | 0.029 |
| Including moderator of project duration | - | - | 0.061 | 1 | 0.805 | - | - | - | - | |
| 12 weeks | 1.081 | 0.280 | - | - | - | - | - | - | - | |
| 26 weeks | 1.000 | 0.317 | - | - | - | - | - | - | - | |
| Including moderator of wellbeing scale version | - | - | 0.017 | 1 | 0.895 | - | - | - | ||
| WEMWBS | 1.036 | 0.300 | - | - | - | - | - | - | - | |
| SWEMWBS | 1.188 | 0.235 | - | - | - | - | - | - | - | |
| Sex | Age Category (years) | Starting Wellbeing Status | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 18–30 | 31–50 | 51–70 | >70 | Low | Average–High | ||
| Whole sample | Starting | 47.2 ± 18.4 | 46.8 ± 17.5 | 48.6 ± 20.5 | 45.3 ± 16.2 | 49.8 ± 19.5 | 46.9 ± 12.4 | 29.5 ± 10.8 | 58.6 ± 12.8 |
| Δ | 15.0 ± 16.5 n = 125 | 13.4 ± 15.8 n = 177 | 13.9 ± 16.9 n = 67 | 14.6 ± 17.1 n = 122 | 12.2 ± 15.3 n = 77 | 19.0 ± 14.1 n = 15 | 21.2 ± 18.7 n = 129 | 8.0 ± 12.1 n = 189 | |
| Low wellbeing | Starting | 29.7 ± 11.0 | 30.7 ± 10.3 | 27.9 ± 11.0 | 30.4 ± 11.2 | 28.4 ± 11.0 | 36.5 ± 6.0 | - | - |
| Δ | 22.6 ± 18.9 n = 49 | 21.3 ± 19.4 n = 71 | 23.9 ± 20.0 n = 25 | 21.9 ± 21.8 n= 49 | 21.9 ± 17.7 n = 25 | 23.2 ± 12.0 n = 7 | - | - | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogerson, M.; Wood, C.; Pretty, J.; Schoenmakers, P.; Bloomfield, D.; Barton, J. Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing. Int. J. Environ. Res. Public Health 2020, 17, 1526. https://doi.org/10.3390/ijerph17051526
Rogerson M, Wood C, Pretty J, Schoenmakers P, Bloomfield D, Barton J. Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing. International Journal of Environmental Research and Public Health. 2020; 17(5):1526. https://doi.org/10.3390/ijerph17051526
Chicago/Turabian StyleRogerson, Mike, Carly Wood, Jules Pretty, Patrick Schoenmakers, Dan Bloomfield, and Jo Barton. 2020. "Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing" International Journal of Environmental Research and Public Health 17, no. 5: 1526. https://doi.org/10.3390/ijerph17051526