Decrease in Serum HDL-C Level Is Associated with Elevation of Blood Pressure: Correlation Analysis from the Korean National Health and Nutrition Examination Survey 2017



Abstract
:1. Introduction
2. Methods
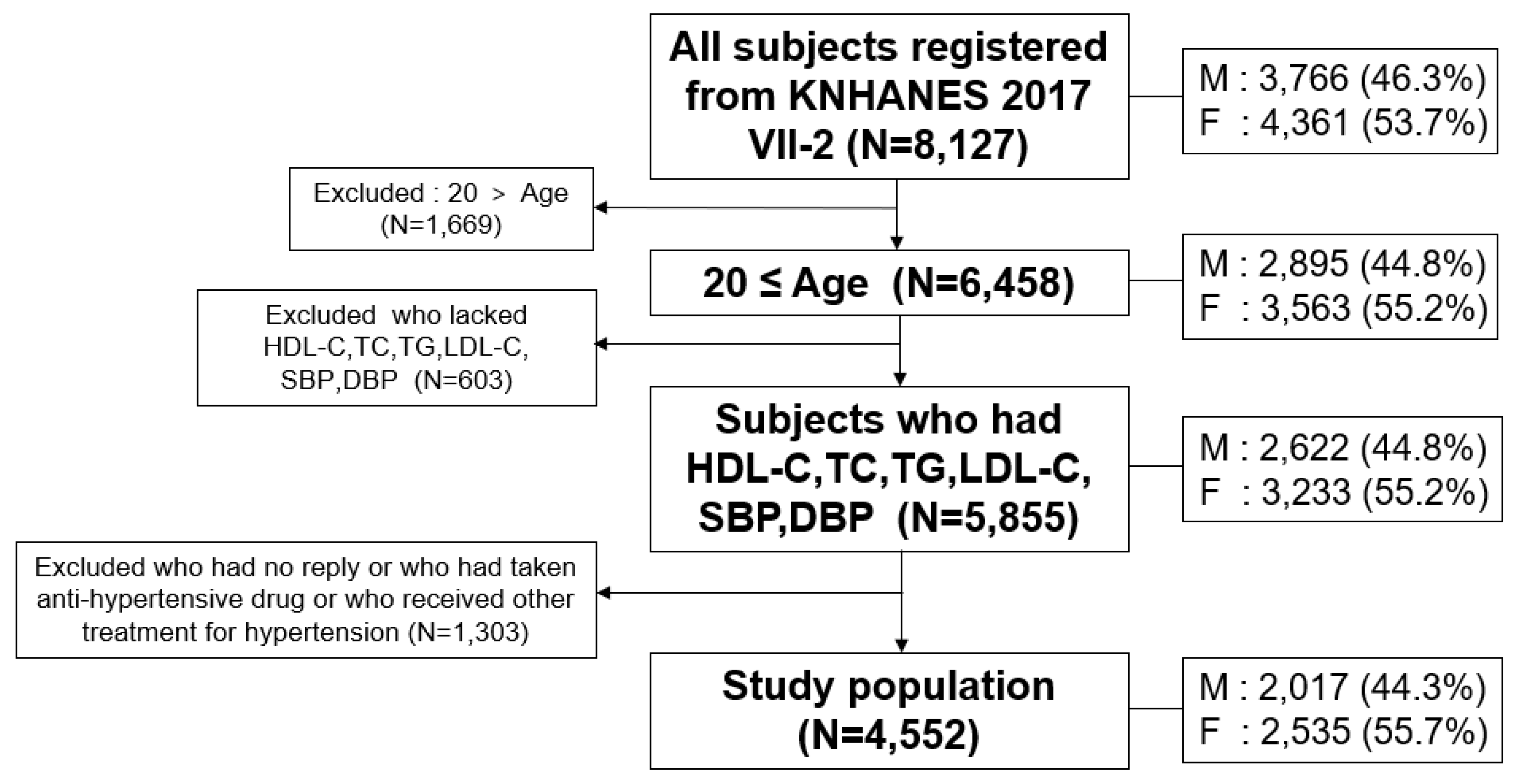
2.1. Study Population
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. General Profiles of BP and Lipid
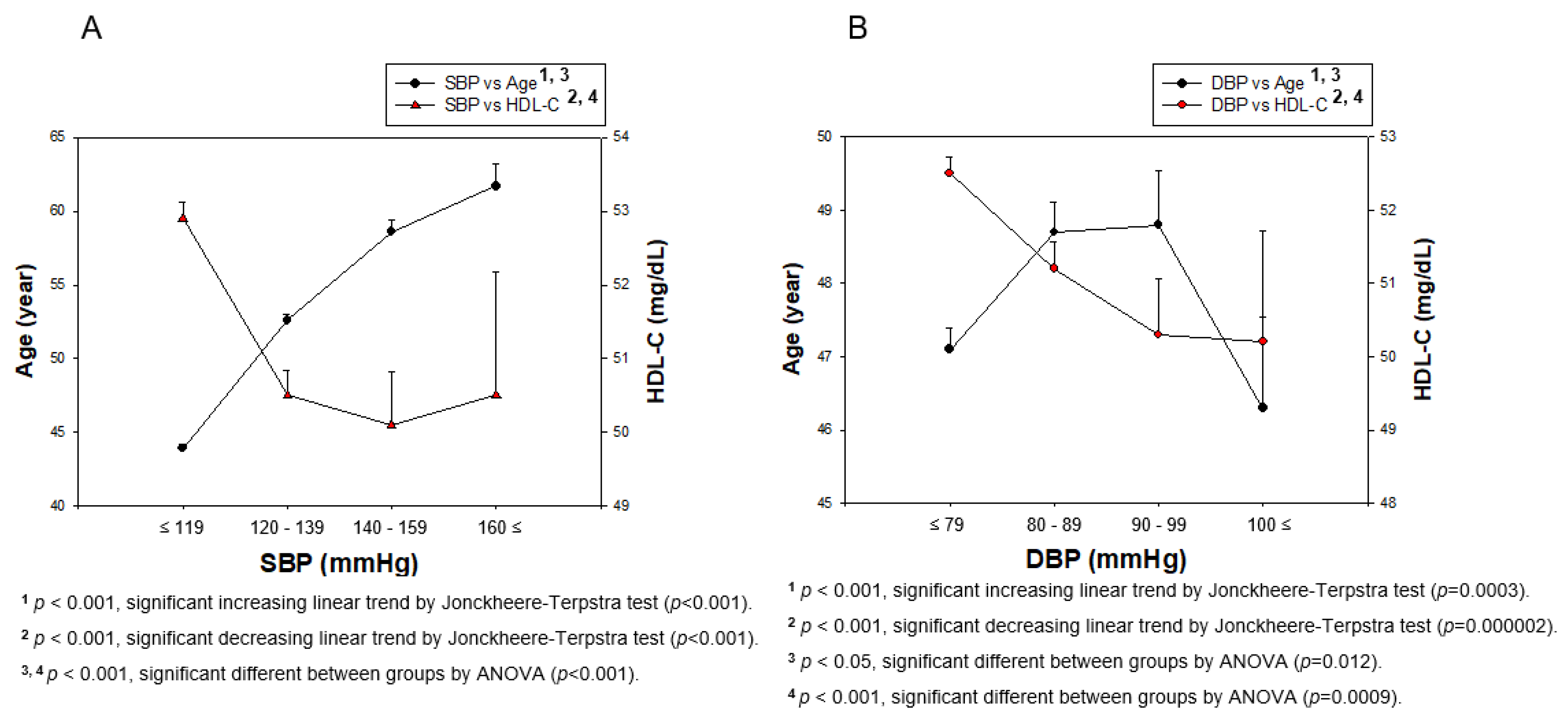
3.2. Distribution of BP, Age, and HDL-C in Total Population
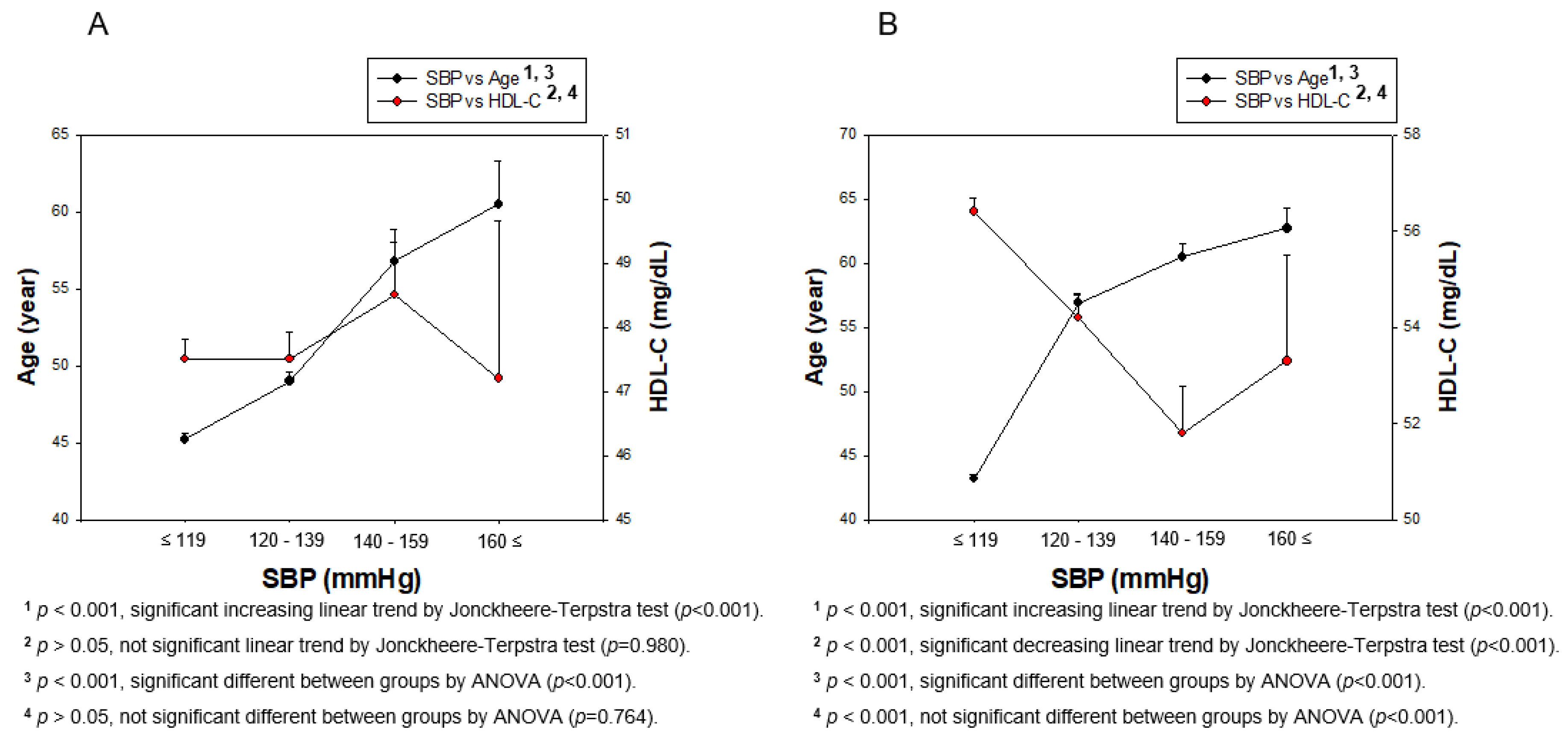
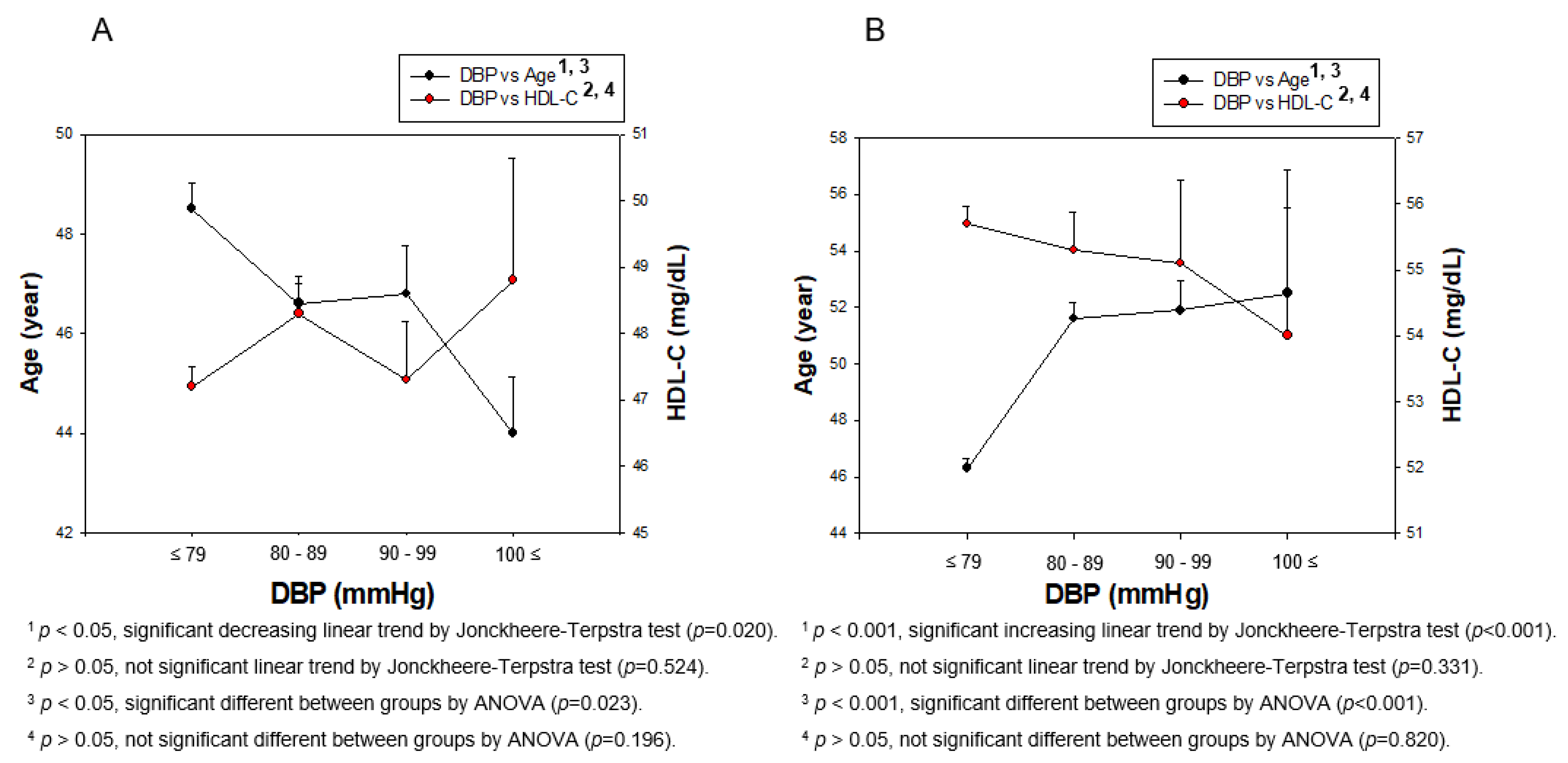
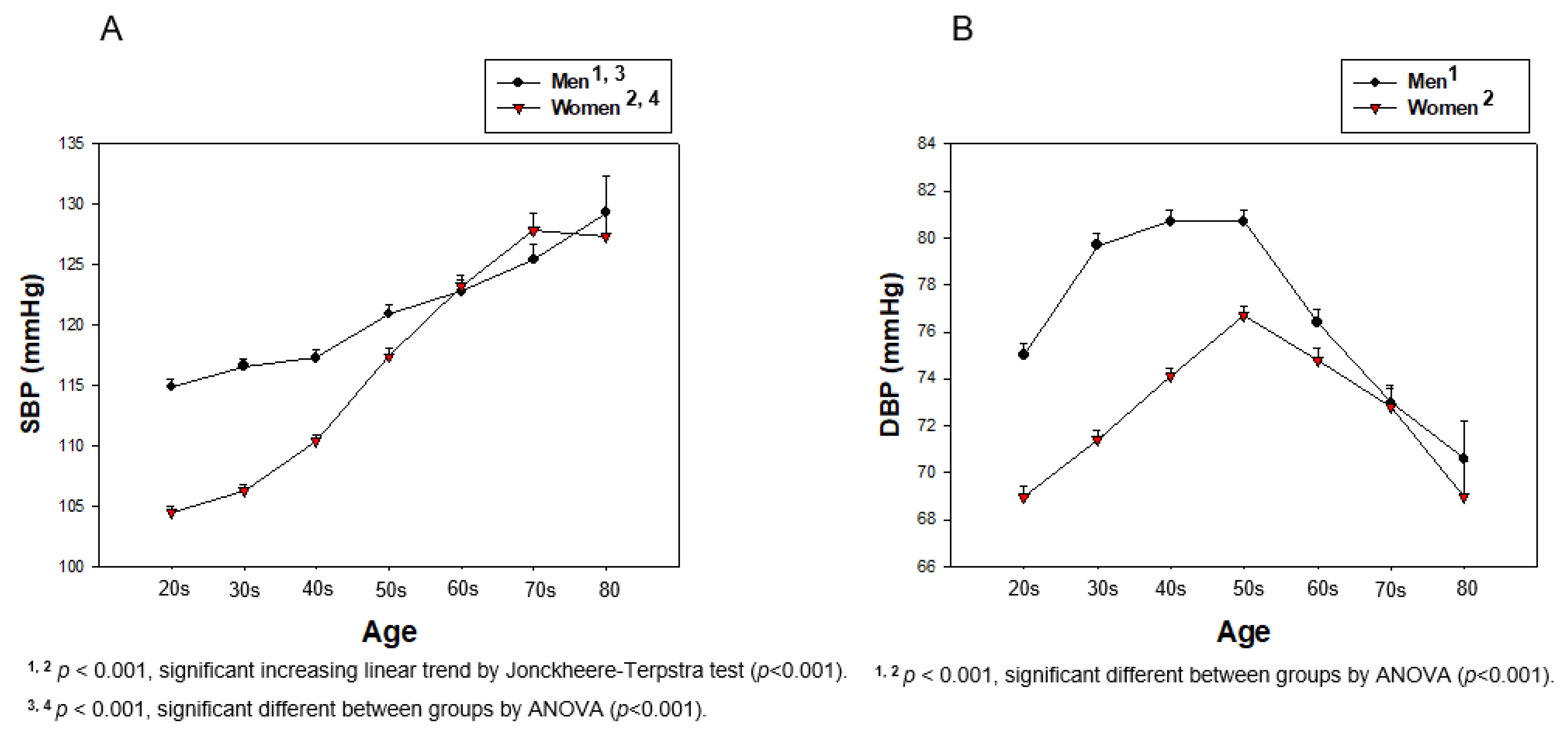
3.3. Distribution of BP and HDL-C Depends on Gender
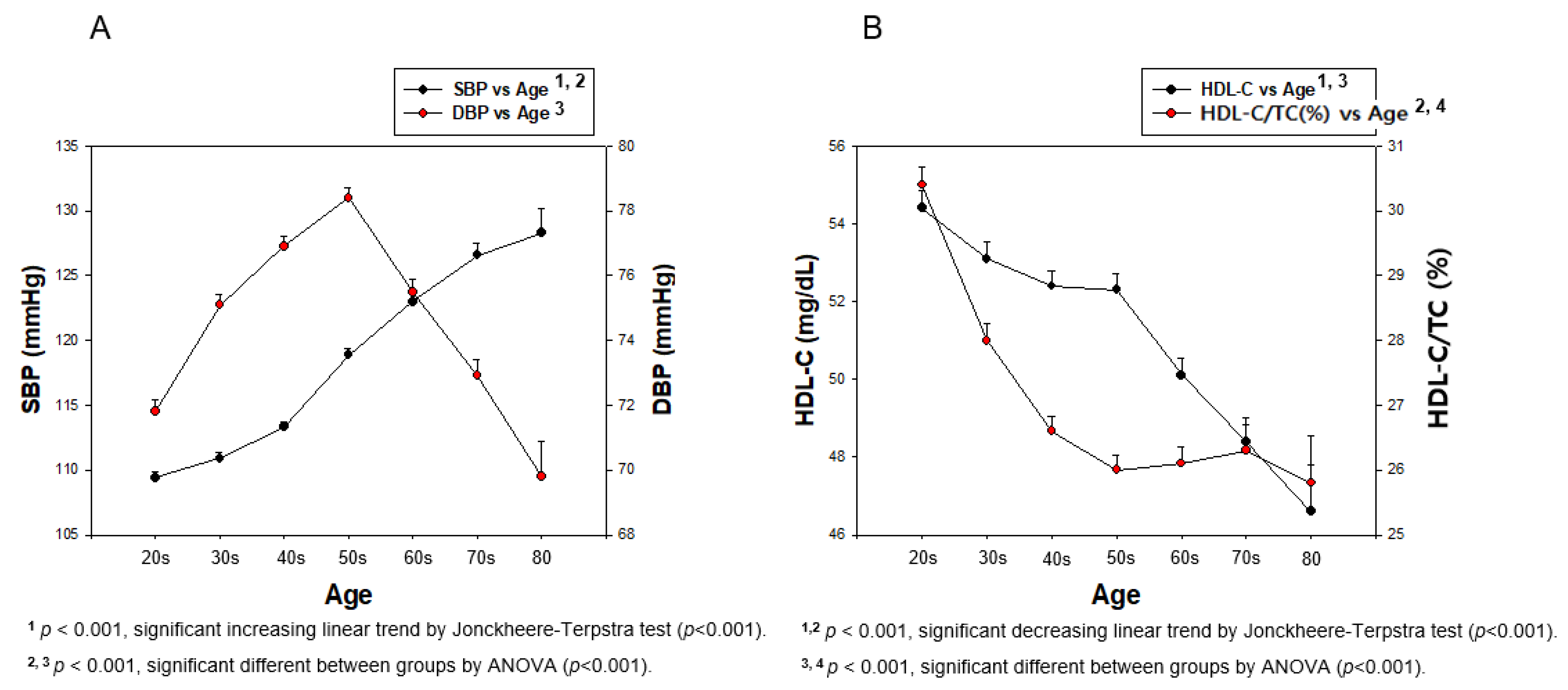
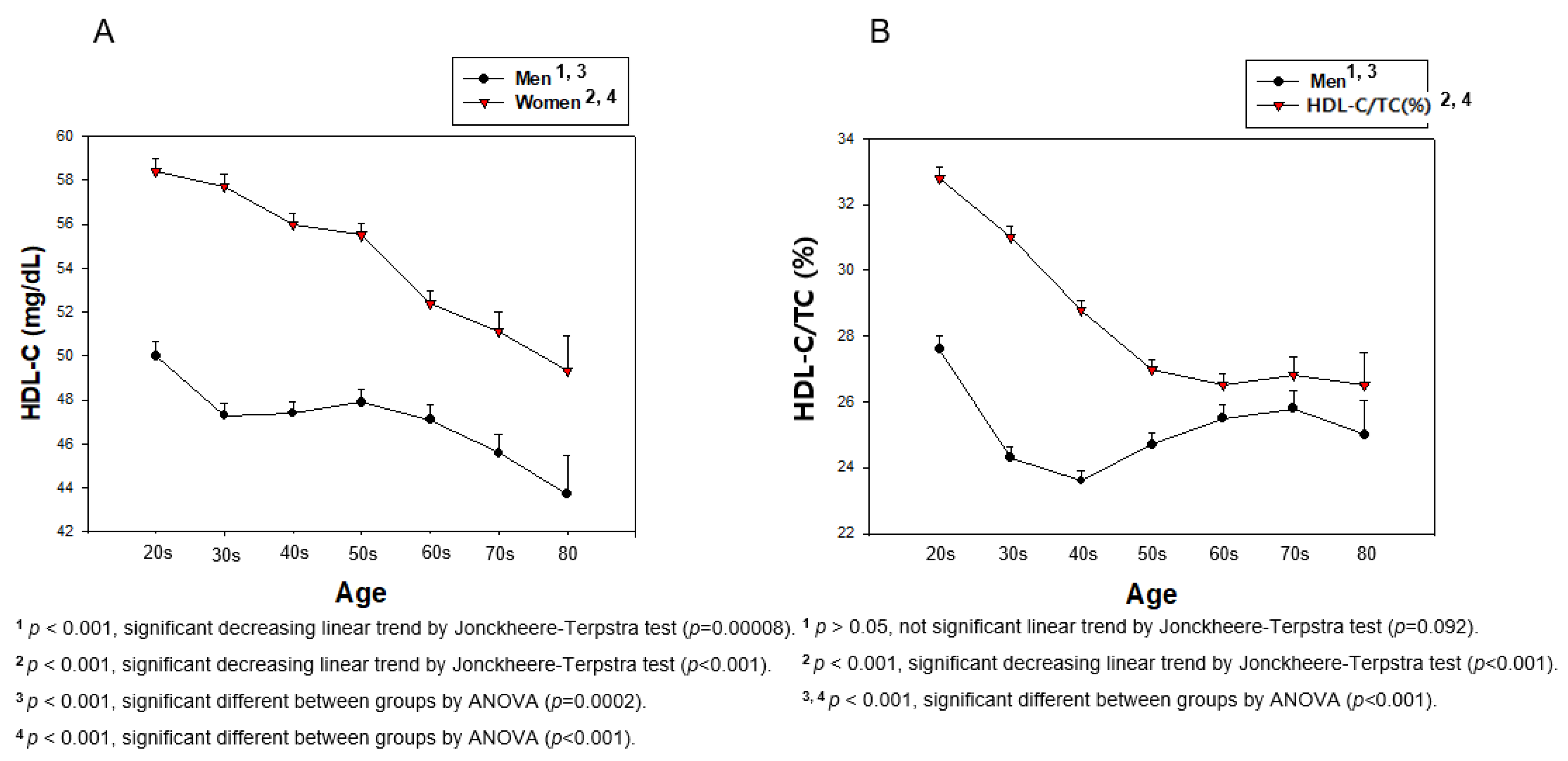
3.4. Lifetime Change in BP, HDL-C, and HDL-C/TC (%)
3.5. Correlation of BP and HDL-C
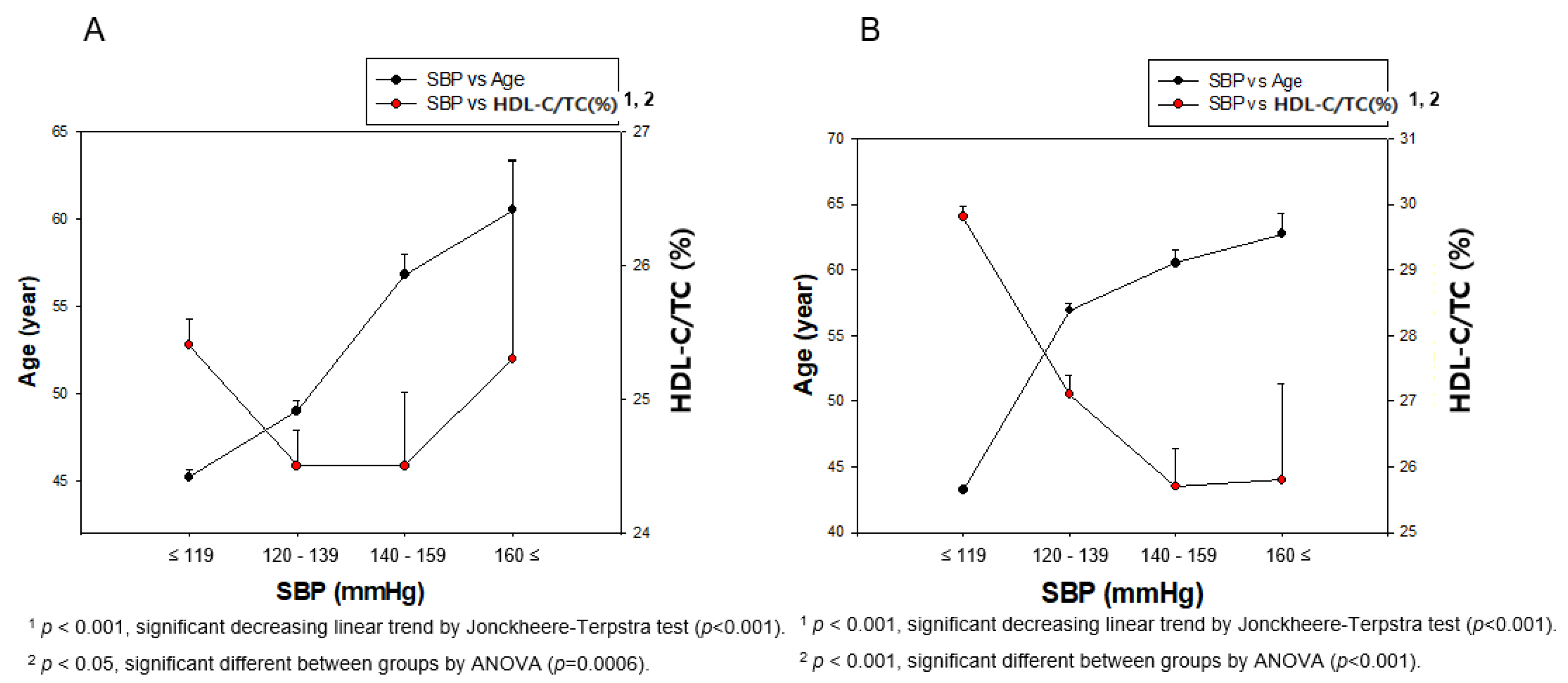
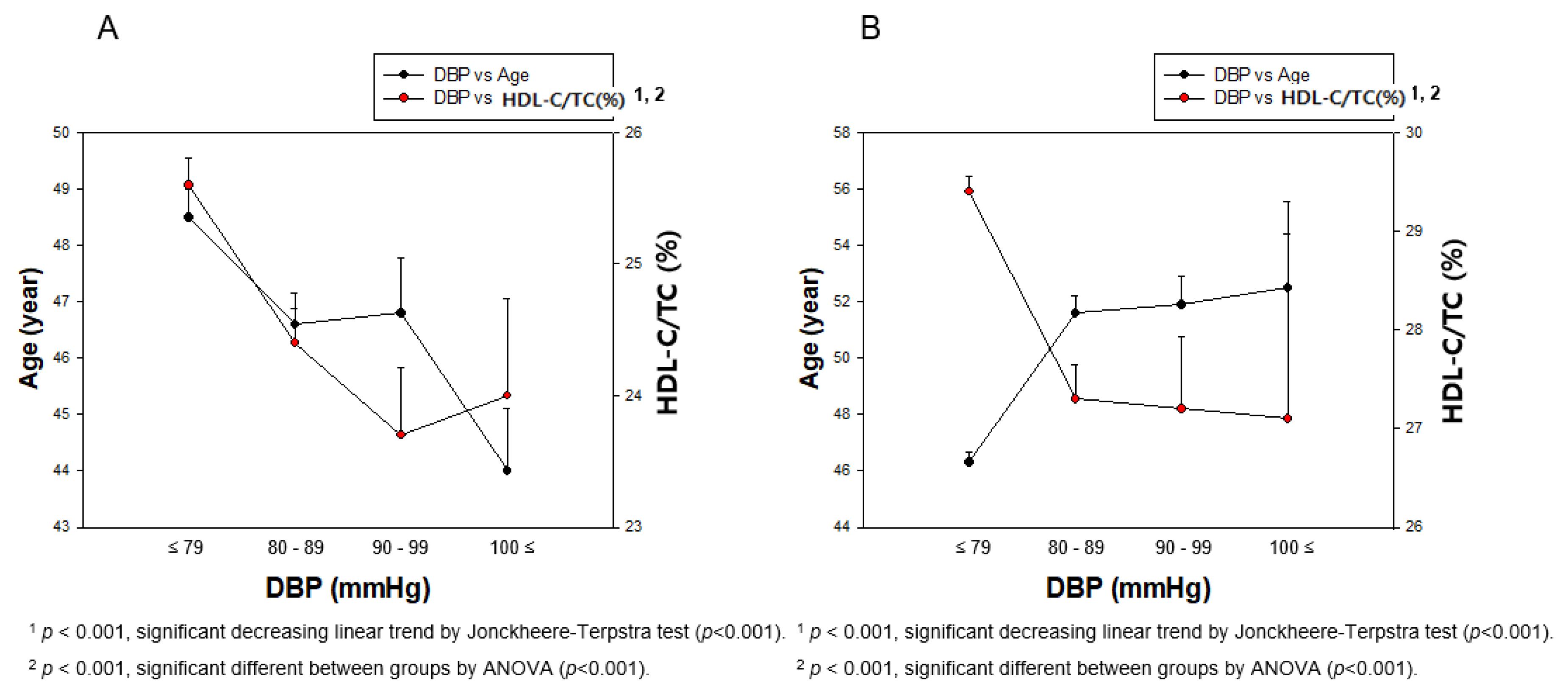
3.6. Correlation of BP and HDL-C/TC (%)
3.7. Correlation Analysis Among age, HDL-C and HDL-C/TC (%)
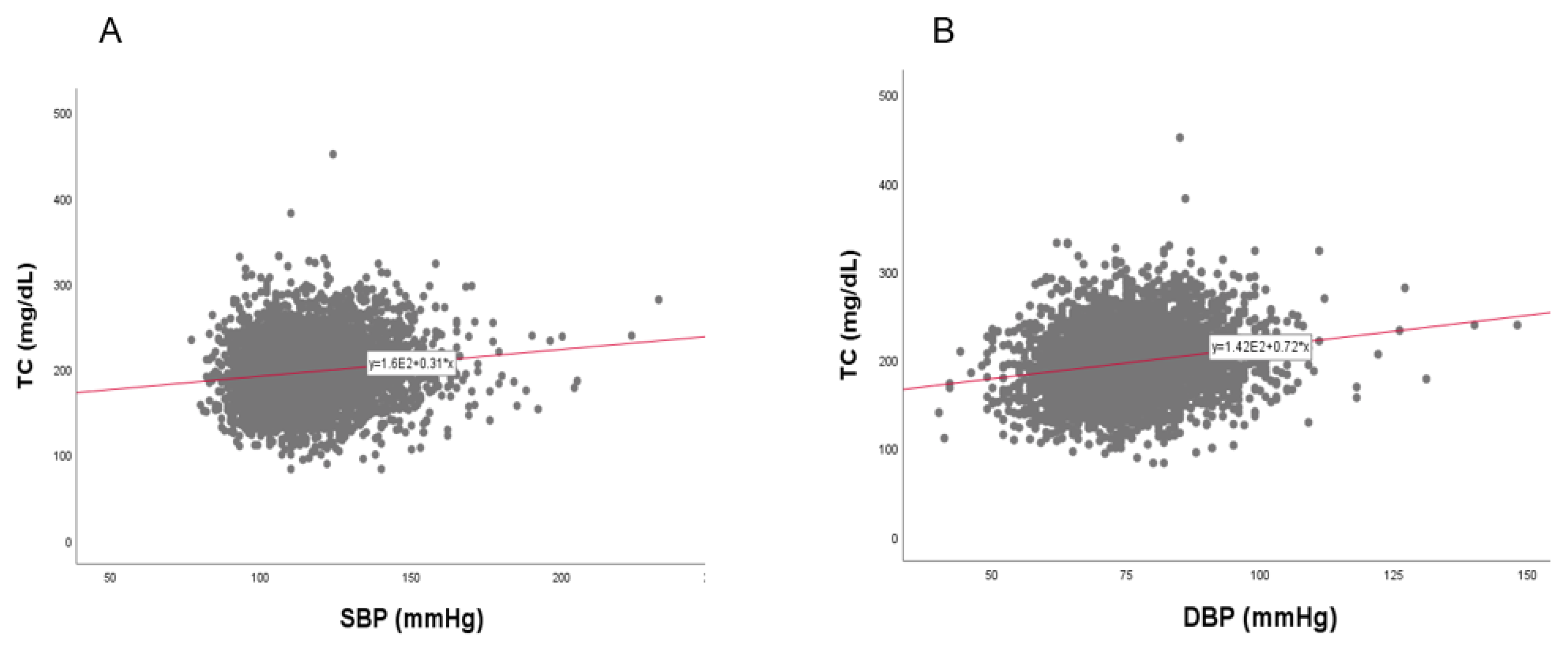
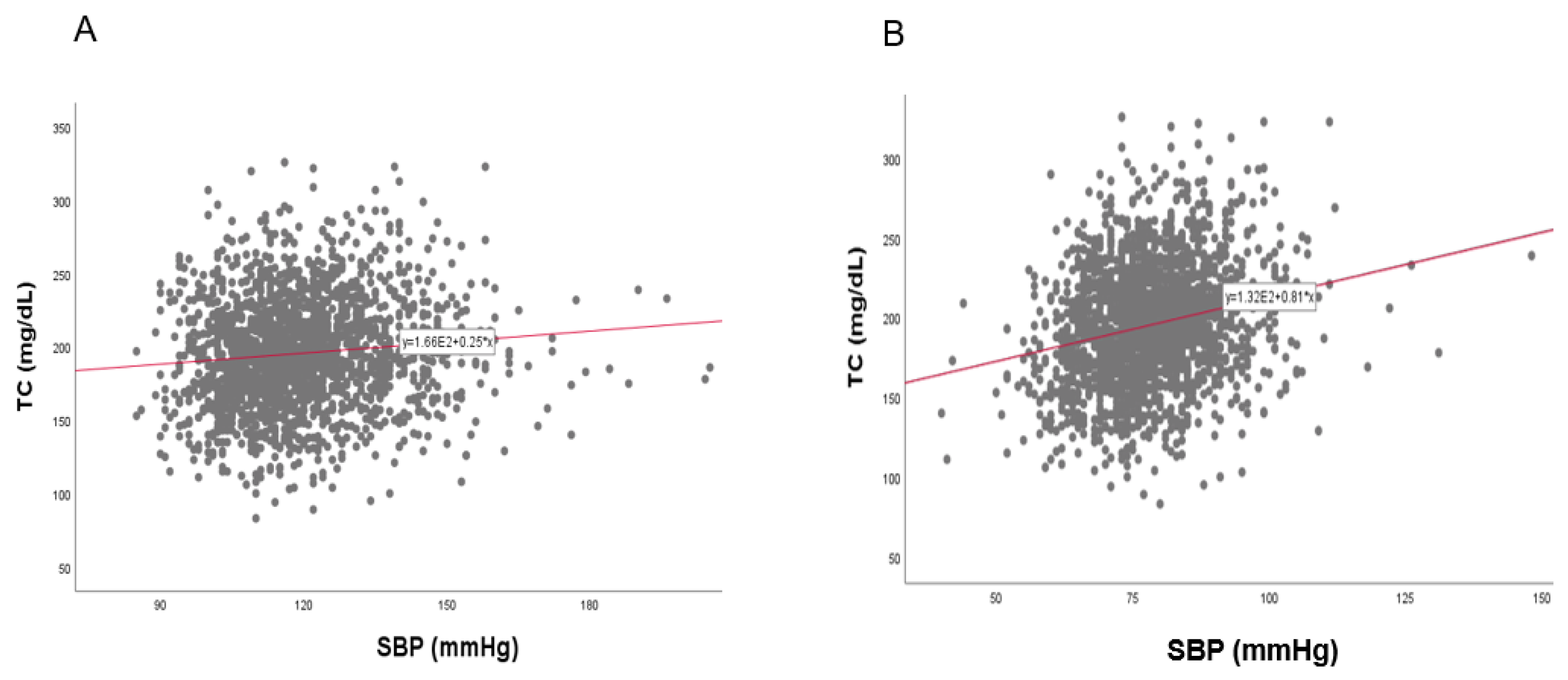
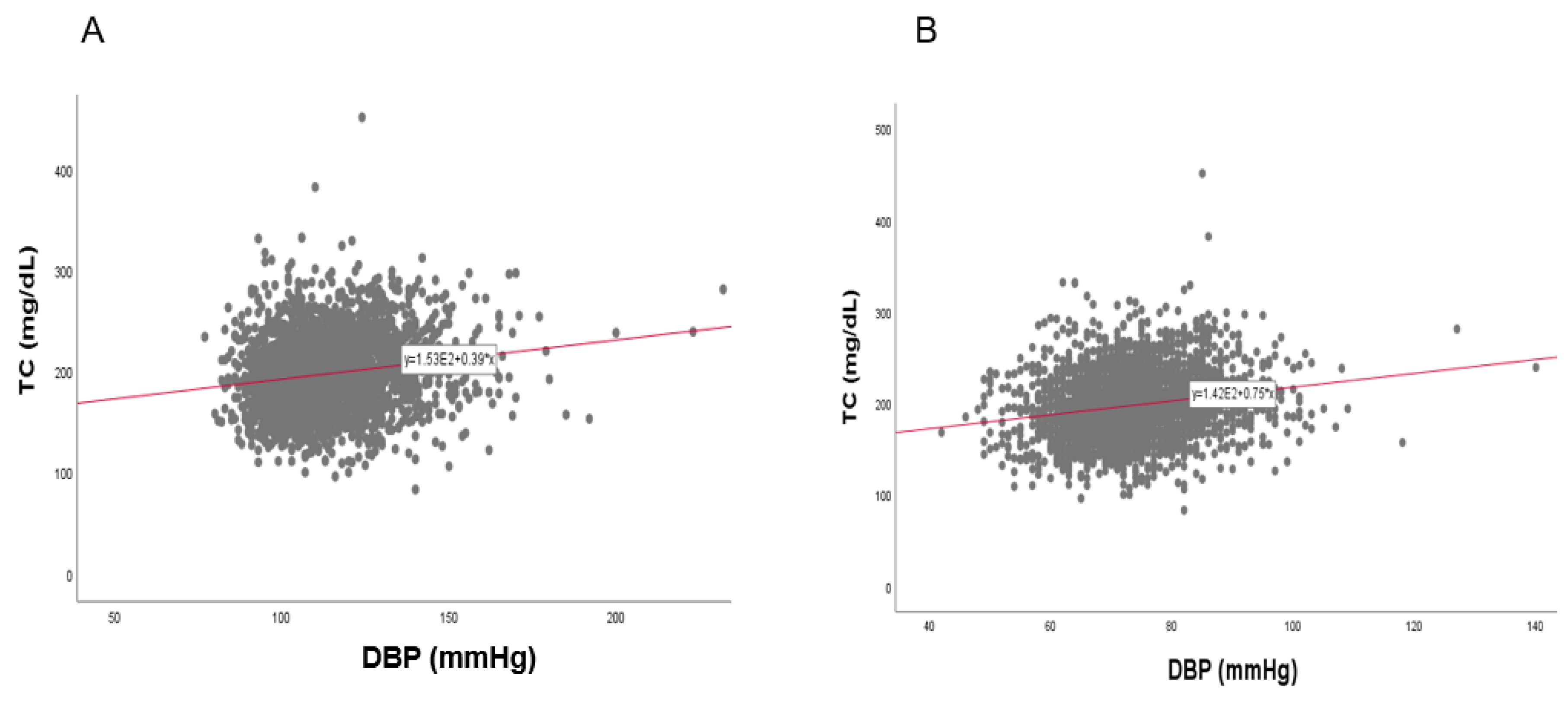
3.8. Correlation of BP and TC
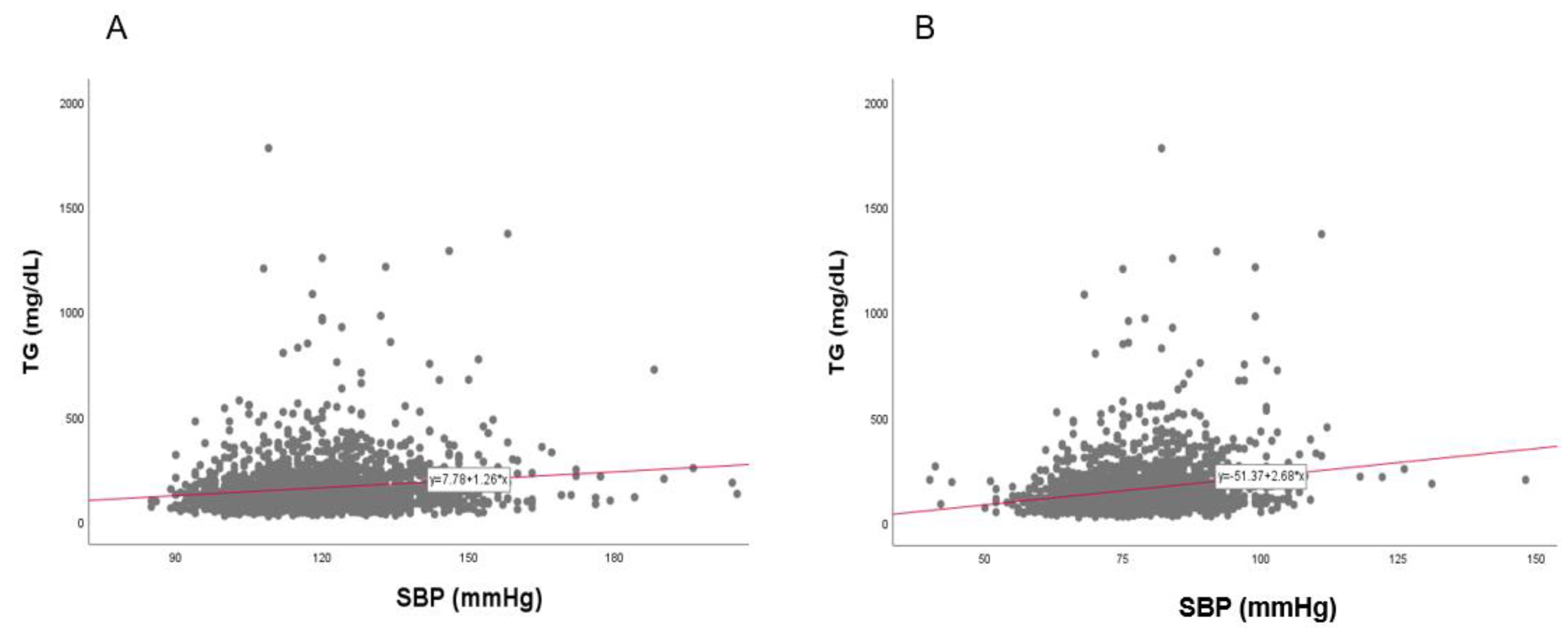
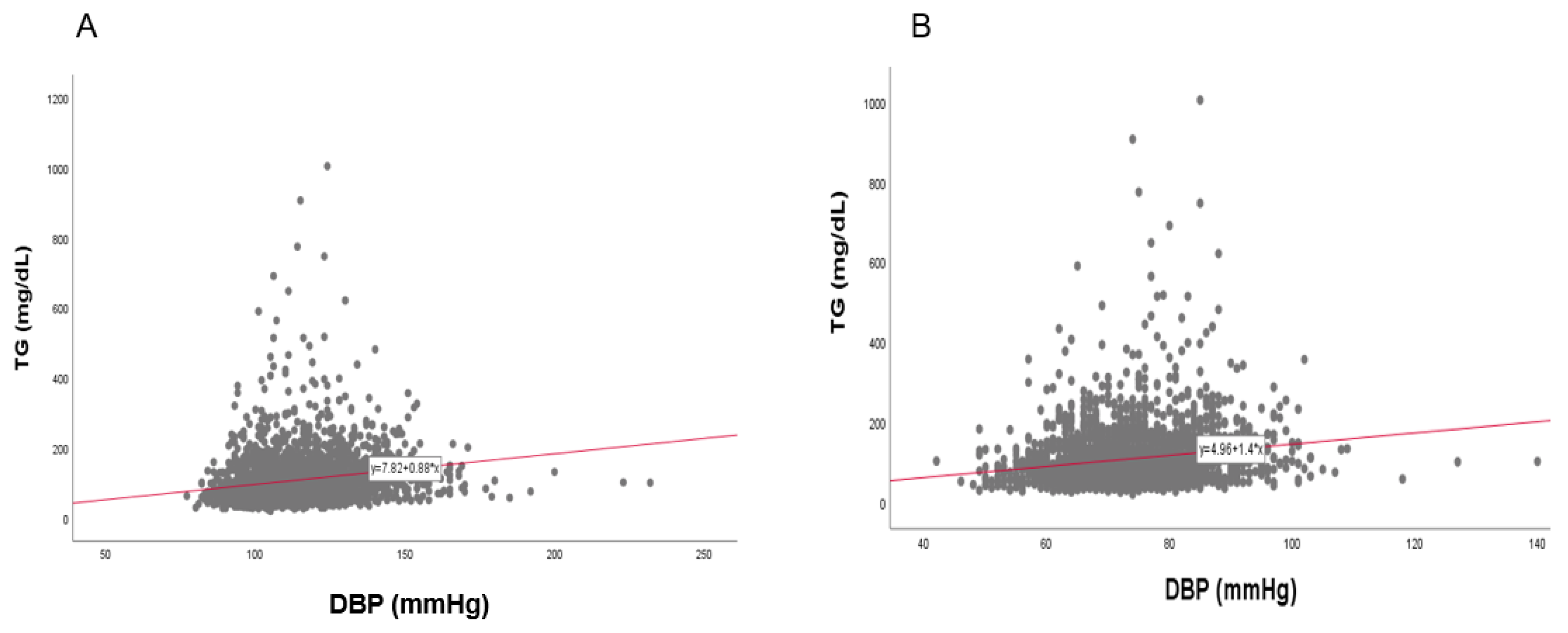
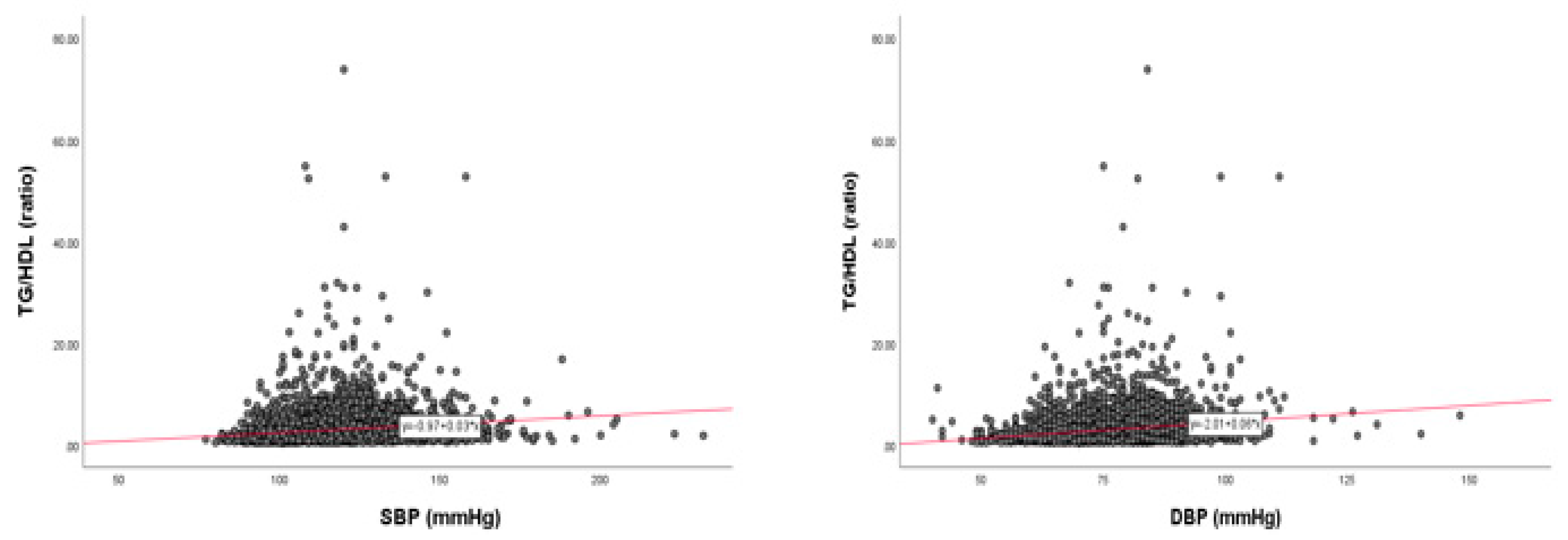
3.9. Correlation of BP and TG
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lithell, H. Hypertension and hyperlipidemia. A review. Am. J. Hypertens. 1993, 6, 303S–308S. [Google Scholar] [CrossRef] [PubMed]
- Collins, R.; Peto, R.; MacMahon, S.; Hebert, P.; Fiebach, N.H.; Eberlein, K.A.; Godwin, J.; Qizilbash, N.; Taylor, J.O.; Hennekens, C.H. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: Overview of randomised drug trials in their epidemiological context. Lancet 1990, 335, 827–838. [Google Scholar] [CrossRef]
- Mansukhani, M.P.; Kolla, B.P.; Somers, V.K. Hypertension and Cognitive Decline: Implications of Obstructive Sleep Apnea. Front. Cardiovasc. Med. 2019, 6, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennon, M.J.; Makkar, S.R.; Crawford, J.D.; Sachdev, P.S. Midlife Hypertension and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2019, 71, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Elkind, M.S. Lipids and Cerebrovascular Disease: Research and Practice. Stroke 2015, 46, 3322–3328. [Google Scholar] [CrossRef] [Green Version]
- Walker, K.A.; Sharrett, A.R.; Wu, A.; Schneider, A.L.C.; Albert, M.; Lutsey, P.L.; Bandeen-Roche, K.; Coresh, J.; Gross, A.L.; Windham, B.G.; et al. Association of Midlife to Late-Life Blood Pressure Patterns with Incident Dementia. JAMA 2019, 322, 535–545. [Google Scholar] [CrossRef]
- Launer, L.J.; Masaki, K.; Petrovitch, H.; Foley, D.; Havlik, R.J. The association between midlife blood pressure levels and late-life cognitive function. The Honolulu-Asia Aging Study. JAMA 1995, 274, 1846–1851. [Google Scholar] [CrossRef]
- Gottesman, R.F.; Schneider, A.L.; Albert, M.; Alonso, A.; Bandeen-Roche, K.; Coker, L.; Coresh, J.; Knopman, D.; Power, M.C.; Rawlings, A.; et al. Midlife hypertension and 20-year cognitive change: The atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014, 71, 1218–1227. [Google Scholar] [CrossRef]
- Revelas, M.; Thalamuthu, A.; Oldmeadow, C.; Evans, T.J.; Armstrong, N.J.; Riveros, C.; Kwok, J.B.; Schofield, P.R.; Brodaty, H.; Scott, R.J.; et al. Exceptional Longevity and Polygenic Risk for Cardiovascular Health. Genes 2019, 10, 227. [Google Scholar] [CrossRef] [Green Version]
- Muller, M.; Launer, L. Joint effect of mid- and late-life blood pressure on the brain: The AGES-Reykjavik Study. Author response. Neurology 2015, 84, 329–330. [Google Scholar] [CrossRef] [Green Version]
- Burt, V.L.; Whelton, P.; Roccella, E.J.; Brown, C.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988–1991. Hypertension 1995, 25, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies from 90 Countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Park, H.J.; Kim, S.J.; Kim, J.R. Decrease in HDL-C is Associated with Age and Household Income in Adults from the Korean National Health and Nutrition Examination Survey 2017: Correlation Analysis of Low HDL-C and Poverty. Int. J. Environ. Res. Public Health 2019, 16, 3329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, K.A.; Power, M.C.; Gottesman, R.F. Defining the Relationship Between Hypertension, Cognitive Decline, and Dementia: A Review. Curr. Hypertens. Rep. 2017, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Kim, N.S.; Lee, B.K.; Oh, I.; Kim, Y. Changes of Atmospheric and Blood Concentrations of Lead and Cadmium in the General Population of South Korea from 2008 to 2017. Int. J. Environ. Res. Public Health 2019, 16, 2096. [Google Scholar] [CrossRef] [Green Version]
- Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef]
- Lunneborg, C.E. Jonckheere–Terpstra Test. In Encyclopedia of Statistics in Behavioral Science; Wiley Online Library: Hoboken, NJ, USA, 2005. [Google Scholar]
- Matthews, D.E. Linear regression, simple. In Wiley StatsRef: Statistics Reference Online; Wiley Online Library: Hoboken, NJ, USA, 2014. [Google Scholar]
- Kunutsor, S.K.; Kieneker, L.M.; Bakker, S.J.L.; James, R.W.; Dullaart, R.P.F. The inverse association of HDL-cholesterol with future risk of hypertension is not modified by its antioxidant constituent, paraoxonase-1: The PREVEND prospective cohort study. Atherosclerosis 2017, 263, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Formiga, F.; Meco, J.F.; Pinto, X.; Jacob, J.; Moga, I.; Pujol, R. Lipid and lipoprotein levels in premenopausal systemic lupus erythematosus patients. Lupus 2001, 10, 359–363. [Google Scholar] [CrossRef]
- Chen, H.; Du, Y.; Liu, S.; Ge, B.; Ji, Y.; Huang, G. Association between serum cholesterol levels and Alzheimer’s disease in China: A case-control study. Int. J. Food Sci. Nutr. 2019, 70, 405–411. [Google Scholar] [CrossRef]
- Riggs, K.A.; Rohatgi, A. HDL and Reverse Cholesterol Transport Biomarkers. Methodist Debakey Cardiovasc. J. 2019, 15, 39–46. [Google Scholar]
- Kontush, A. HDL particle number and size as predictors of cardiovascular disease. Front. Pharmacol. 2015, 6, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merched, A.; Xia, Y.; Visvikis, S.; Serot, J.M.; Siest, G. Decreased high-density lipoprotein cholesterol and serum apolipoprotein AI concentrations are highly correlated with the severity of Alzheimer’s disease. Neurobiol. Aging 2000, 21, 27–30. [Google Scholar] [CrossRef]
- Zuliani, G.; Cavalieri, M.; Galvani, M.; Volpato, S.; Cherubini, A.; Bandinelli, S.; Corsi, A.M.; Lauretani, F.; Guralnik, J.M.; Fellin, R.; et al. Relationship between low levels of high-density lipoprotein cholesterol and dementia in the elderly. The InChianti study. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koldamova, R.P.; Lefterov, I.M.; Lefterova, M.I.; Lazo, J.S. Apolipoprotein A-I directly interacts with amyloid precursor protein and inhibits A beta aggregation and toxicity. Biochemistry 2001, 40, 3553–3560. [Google Scholar] [CrossRef]
- Button, E.B.; Robert, J.; Caffrey, T.M.; Fan, J.; Zhao, W.; Wellington, C.L. HDL from an Alzheimer’s disease perspective. Curr. Opin. Lipidol. 2019, 30, 224–234. [Google Scholar] [CrossRef]
- Bonaa, K.H.; Thelle, D.S. Association between blood pressure and serum lipids in a population. The Tromso Study. Circulation 1991, 83, 1305–1314. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Cho, H.J.; Kim, Y.J.; Cho, M.J.; Choi, H.Y.; Eun, C.R.; Kim, J.H.; Yang, S.J.; Yoo, H.J.; Kim, H.Y.; et al. Combined effect of high-normal blood pressure and low HDL cholesterol on mortality in an elderly Korean population: The South-West Seoul (SWS) study. Am. J. Hypertens. 2011, 24, 918–923. [Google Scholar] [CrossRef] [Green Version]
- Xie, D.; Bollag, W.B. Obesity, hypertension and aldosterone: Is leptin the link? J. Endocrinol. 2016, 230, F7–F11. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.Y.; Rainey, W.E.; Bollag, W.B. Very low-density lipoprotein (VLDL)-induced signals mediating aldosterone production. J. Endocrinol. 2017, 232, R115–R129. [Google Scholar] [CrossRef] [Green Version]
- Yokokawa, H.; Yasumura, S.; Tanno, K.; Ohsawa, M.; Onoda, T.; Itai, K.; Sakata, K.; Kawamura, K.; Tanaka, F.; Yoshida, Y.; et al. Serum low-density lipoprotein to high-density lipoprotein ratio as a predictor of future acute myocardial infarction among men in a 2.7-year cohort study of a Japanese northern rural population. J. Atheroscler. Thromb. 2011, 18, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Hong, M.; Ling, Y.; Lu, Z.; Liu, Y.; Gu, P.; Shao, J.; Gao, X.; Li, X. Contribution and interaction of the low-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and triglyceride to diabetes in hypertensive patients: A cross-sectional study. J. Diabetes Investig. 2019, 10, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Dai, J.L. Triglyceride to high-density lipoprotein cholesterol (HDL-C) ratio and arterial stiffness in Japanese population: A secondary analysis based on a cross-sectional study. Lipids Health Dis. 2018, 17, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men N = 2017 (Mean ± SD) | Women N = 2535 (Mean ± SD) | * p | Total N = 4552 (Mean ± SD) |
|---|---|---|---|---|
| SBP (mmHg) | 119.2 ± 14.7 | 113.6 ± 16.1 | <0.001 | 116.1 ± 15.8 |
| DBP (mmHg) | 78.2 ± 10.2 | 73.4 ± 9.4 | <0.001 | 75.5 ± 10.0 |
| HDL-C (mg/dL) | 47.6 ± 11.0 | 55.6 ± 12.2 | <0.001 | 52.0 ± 12.3 |
| TC (mg/dL) | 195.6 ± 36.6 | 197.4 ± 36.9 | 0.103 | 196.6 ± 36.8 |
| TG (mg/ dL) | 158.5 ± 129.1 | 107.3 ± 73.1 | <0.001 | 130.0 ± 104.9 |
| HDL-C/TC (%) | 25.0 ± 6.9 | 28.9 ± 7.1 | <0.001 | 27.2 ± 7.3 |
| LDL-C (mg/dL) | 116.3 ± 34.9 | 120.4 ± 32.5 | 0.00006 | 118.6 ± 33.6 |
| LDL-C/HDL-C | 2.5 ± 0.9 | 2.3 ± 0.8 | <0.001 | 2.4 ± 0.9 |
| TG/HDL-C | 3.8 ± 4.3 | 2.2 ± 2.1 | <0.001 | 2.9 ± 3.4 |
| Age (year) | 47.6 ± 15.7 | 47.6 ± 15.0 | 0.988 | 47.6 ± 15.4 |
| Group | Covariates | SBP (mmHg) | DBP (mmHg) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤119 | 120–139 | 140–159 | ≥160 | ≤79 | 80–89 | 90–99 | ≥100 | * p | ¥p | ||
| Men N = 2017 (Mean ± SD) | N (%) | 1134 (56.2) | 699 (34.7) | 159 (7.9) | 25 (1.2) | 1158 (57.4) | 627 (31.1) | 177 (8.8) | 55 (2.7) | ||
| Age (year) | 45.2 ± 15.1 | 49.0 ± 15.9 | 56.8 ± 15.2 | 60.5 ± 13.9 | 48.5 ± 17.2 | 46.6 ± 13.9 | 46.8 ±13.0 | 44.0 ± 8.3 | <0.001 | 0.023 | |
| HDL-C (mg/dL) | 47.5 ± 10.6 | 47.5 ± 11.1 | 48.5 ± 13.0 | 47.2 ± 12.3 | 47.2 ± 10.4 | 48.3 ± 11.5 | 47.3 ± 11.8 | 48.8 ± 13.7 | 0.764 | 0.196 | |
| HDL-C/TC (%) | 25.4 ± 6.7 | 24.5 ± 7.0 | 24.5 ± 6.9 | 25.3 ± 7.5 | 25.6 ± 6.9 | 24.4 ± 6.7 | 23.7 ± 6.8 | 24.0 ± 7.4 | 0.025 | 0.0001 | |
| Women N = 2535 (Mean ± SD) | N (%) | 1771 (69.9) | 581 (22.9) | 154 (6.1) | 29 (1.1) | 1940 (76.5) | 462 (18.2) | 112 (4.4) | 21 (0.8) | ||
| Age (year) | 43.2 ± 13.6 | 56.9 ± 13.3 | 60.5 ± 12.1 | 62.7 ± 8.9 | 46.3 ± 15.6 | 51.6 ± 12.7 | 51.9 ± 10.8 | 52.5 ± 14.0 | <0.001 | <0.001 | |
| HDL-C (mg/dL) | 56.4 ± 12.0 | 54.2 ± 12.3 | 51.8 ± 12.3 | 53.3 ± 11.9 | 55.7 ± 12.0 | 55.3 ± 12.6 | 55.1 ± 13.4 | 54.0 ± 11.5 | <0.001 | 0.820 | |
| HDL-C/TC (%) | 29.8 ± 6.9 | 27.1 ± 7.2 | 25.7 ± 7.1 | 25.8 ± 7.9 | 29.4 ± 6.9 | 27.3 ± 7.5 | 27.2 ± 7.7 | 27.1 ± 8.6 | <0.001 | <0.001 | |
| †p | 0.0003 | <0.001 | 0.017 | 0.485 | 0.0006 | <0.001 | 0.0003 | 0.015 | |||
| ₸p | <0.001 | <0.001 | 0.019 | 0.069 | <0.001 | <0.001 | <0.001 | 0.127 | |||
| €p | <0.001 | <0.001 | 0.139 | 0.837 | <0.001 | <0.001 | <0.001 | 0.120 | |||
| Total N = 4552 (Mean ± SD) | N (%) | 2905 (63.8) | 1280 (28.1) | 313 (6.9) | 54 (1.2) | 3098 (68.1) | 1089 (23.9) | 289 (6.3) | 76 (1.7) | ||
| Age (year) | 43.9 ± 14.2 | 52.6 ± 15.2 | 58.6 ± 13.9 | 61.7 ± 11.4 | 47.1 ± 16.2 | 48.7 ± 13.6 | 48.8 ± 12.4 | 46.3 ± 10.8 | <0.001 | 0.012 | |
| HDL-C (mg/dL) | 52.9 ± 12.3 | 50.5 ± 12.1 | 50.1 ± 12.7 | 50.5 ± 12.4 | 52.5 ± 12.1 | 51.2 ± 12.5 | 50.3 ± 13.0 | 50.2 ± 13.3 | <0.001 | 0.0009 | |
| HDL-C/TC (%) | 28.1 ± 7.2 | 25.7 ± 7.2 | 25.1 ± 7.0 | 25.5 ± 7.7 | 28.0 ± 7.1 | 25.6 ± 7.2 | 25.1 ± 7.3 | 24.8 ± 7.8 | <0.001 | <0.001 | |
| Group | Age | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80 | * p |
|---|---|---|---|---|---|---|---|---|---|
| Men N = 2017 (Mean ± SD) | N (%) | 303 (15.0) | 388 (19.2) | 436 (21.6) | 392 (19.4) | 287 (14.2) | 168 (8.3) | 43 (2.1) | |
| SBP (mmHg) | 114.9 ± 11.1 | 116.6 ± 12.0 | 117.3 ± 13.8 | 120.9 ± 15.3 | 122.8 ± 16.3 | 125.4 ± 17.1 | 129.3 ± 20.4 | <0.001 | |
| DBP (mmHg) | 75.0 ± 9.3 | 79.7 ± 9.9 | 80.7 ± 10.4 | 80.7 ± 9.5 | 76.4 ± 9.5 | 73.0 ± 9.2 | 70.6 ± 10.5 | <0.001 | |
| HDL-C (mg/dL) | 50.0 ± 11.2 | 47.3 ± 10.3 | 47.4 ± 10.5 | 47.9 ± 11.4 | 47.1 ± 11.5 | 45.6 ± 10.5 | 43.7 ± 11.5 | 0.0002 | |
| HDL-C/TC (%) | 27.6 ± 7.2 | 24.3 ± 6.5 | 23.6 ± 6.3 | 24.7 ± 6.7 | 25.5 ± 7.2 | 25.8 ± 7.1 | 25.0 ± 6.7 | <0.001 | |
| Women N = 2535 (Mean ± SD) | N (%) | 340 (13.4) | 481 (19.0) | 594 (23.4) | 536 (21.1) | 367 (14.5) | 172 (6.8) | 45 (1.8) | |
| SBP (mmHg) | 104.5 ± 9.0 | 106.3 ± 11.0 | 110.4 ± 13.6 | 117.4 ± 16.9 | 123.2 ± 17.0 | 127.9 ± 17.4 | 127.3 ± 14.6 | <0.001 | |
| DBP (mmHg) | 69.0 ± 7.7 | 71.4 ± 8.7 | 74.1 ± 9.0 | 76.7 ± 9.5 | 74.8 ± 9.5 | 72.8 ± 10.4 | 69.0 ± 9.8 | <0.001 | |
| HDL-C (mg/dL) | 58.4 ± 11.3 | 57.7 ± 12.4 | 56.0 ± 12.4 | 55.5 ± 12.0 | 52.4 ± 11.4 | 51.1 ± 11.7 | 49.3 ± 10.7 | <0.001 | |
| HDL-C/TC (%) | 32.8 ± 6.3 | 31.0 ± 7.3 | 28.8 ± 6.8 | 27.0 ± 6.5 | 26.5 ± 6.6 | 26.8 ± 7.5 | 26.5 ± 6.8 | <0.001 | |
| †p | <0.001 | <0.001 | <0.001 | 0.0014 | 0.732 | 0.183 | 0.603 | ||
| ₸p | <0.001 | <0.001 | <0.001 | <0.001 | 0.04 | 0.819 | 0.473 | ||
| €p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.000006 | 0.022 | ||
| ǂp | <0.001 | <0.001 | <0.001 | <0.001 | 0.058 | 0.208 | 0.316 | ||
| Total N = 4552 (Mean ± SD) | N (%) | 643 (14.1) | 869 (19.1) | 1030 (22.6) | 928 (20.4) | 654 (14.4) | 340 (7.5) | 88 (1.9) | |
| SBP (mmHg) | 109.4 ± 11.3 | 110.9 ± 12.6 | 113.3 ± 14.1 | 118.9 ± 16.3 | 123.0 ± 16.7 | 126.6 ± 17.3 | 128.3 ± 17.6 | <0.001 | |
| DBP (mmHg) | 71.8 ± 9.0 | 75.1 ± 10.1 | 76.9 ± 10.2 | 78.4 ± 9.7 | 75.5 ± 9.5 | 72.9 ± 9.8 | 69.8 ± 10.1 | <0.001 | |
| HDL-C (mg/dL) | 54.4 ± 12.0 | 53.1 ± 12.6 | 52.4 ± 12.4 | 52.3 ± 12.3 | 50.1 ± 11.7 | 48.4 ± 11.5 | 46.6 ± 11.3 | <0.001 | |
| HDL-C/TC (%) | 30.4 ± 7.2 | 28.0 ± 7.7 | 26.6 ± 7.1 | 26.0 ± 6.7 | 26.1 ± 6.9 | 26.3 ± 7.3 | 25.8 ± 6.8 | <0.001 |
| Dependent Variable | Independent Variable | Standard Error | β | t-Value | p-Value | VIF |
|---|---|---|---|---|---|---|
| SBP | HDL-C | 0.019 | −0.148 | −7.880 | <0.001 *** | 1.000 |
| R = 0.116, R2 = 0.013, Adjusted R2 = 0.013 F = 62.088, p < 0.001, Dublin-Watson = 1.132 | ||||||
| DBP | HDL-C | 0.012 | −0.065 | −5.376 | <0.001 *** | 1.000 |
| R = 0.079, R2 = 0.006, Adjusted R2 = 0.006 F = 28.900, p < 0.001, Dublin-Watson = 0.560 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, K.-H.; Park, H.-J.; Kim, J.-R. Decrease in Serum HDL-C Level Is Associated with Elevation of Blood Pressure: Correlation Analysis from the Korean National Health and Nutrition Examination Survey 2017. Int. J. Environ. Res. Public Health 2020, 17, 1101. https://doi.org/10.3390/ijerph17031101
Cho K-H, Park H-J, Kim J-R. Decrease in Serum HDL-C Level Is Associated with Elevation of Blood Pressure: Correlation Analysis from the Korean National Health and Nutrition Examination Survey 2017. International Journal of Environmental Research and Public Health. 2020; 17(3):1101. https://doi.org/10.3390/ijerph17031101
Chicago/Turabian StyleCho, Kyung-Hyun, Hye-Jeong Park, and Jae-Ryong Kim. 2020. "Decrease in Serum HDL-C Level Is Associated with Elevation of Blood Pressure: Correlation Analysis from the Korean National Health and Nutrition Examination Survey 2017" International Journal of Environmental Research and Public Health 17, no. 3: 1101. https://doi.org/10.3390/ijerph17031101