Spatiotemporal Analysis of the Population Risk of Congenital Microcephaly in Pernambuco State, Brazil

 , , , , and
on behalf of the Microcephaly Epidemic Research Group (MERG)
, , , , and
on behalf of the Microcephaly Epidemic Research Group (MERG) 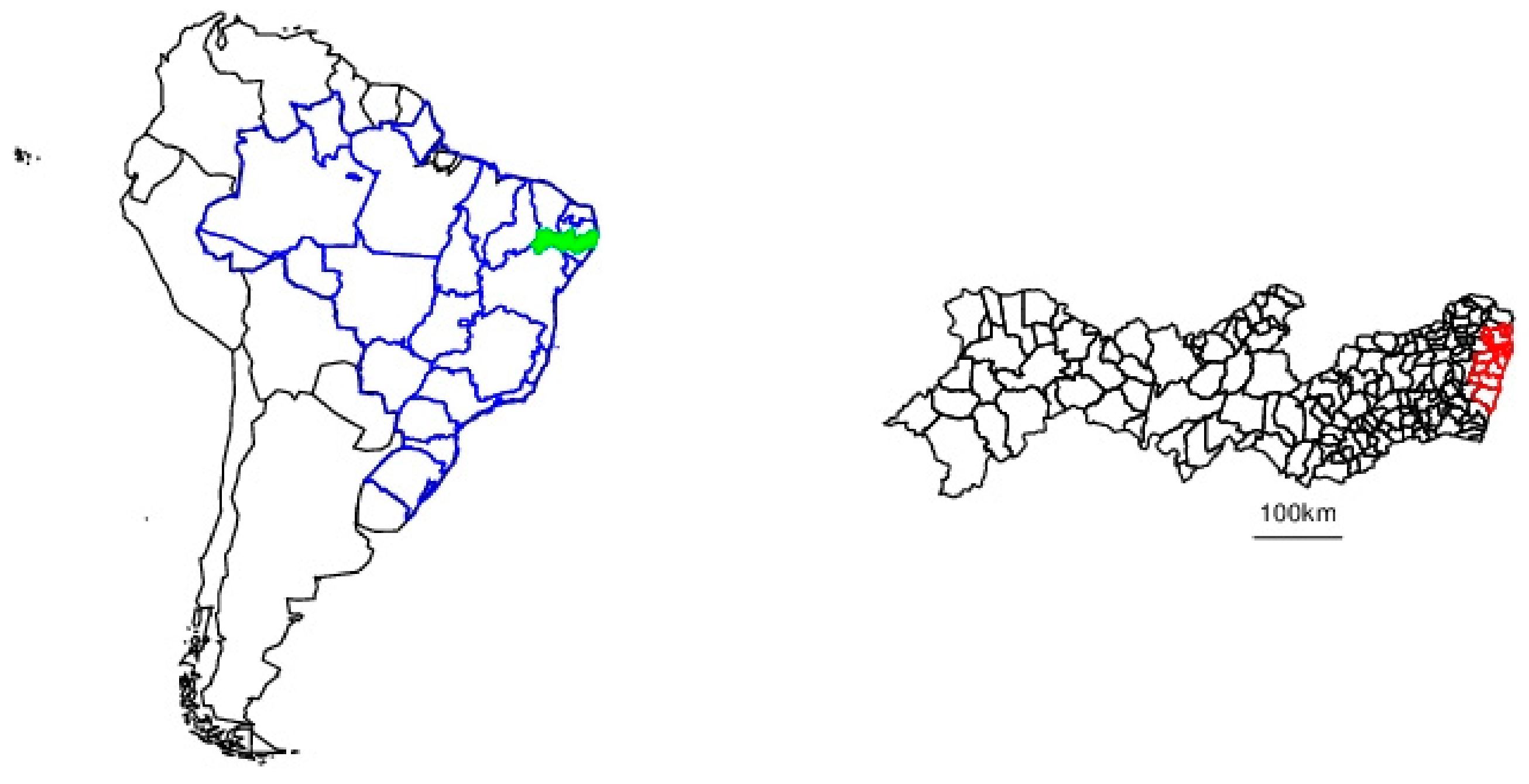{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
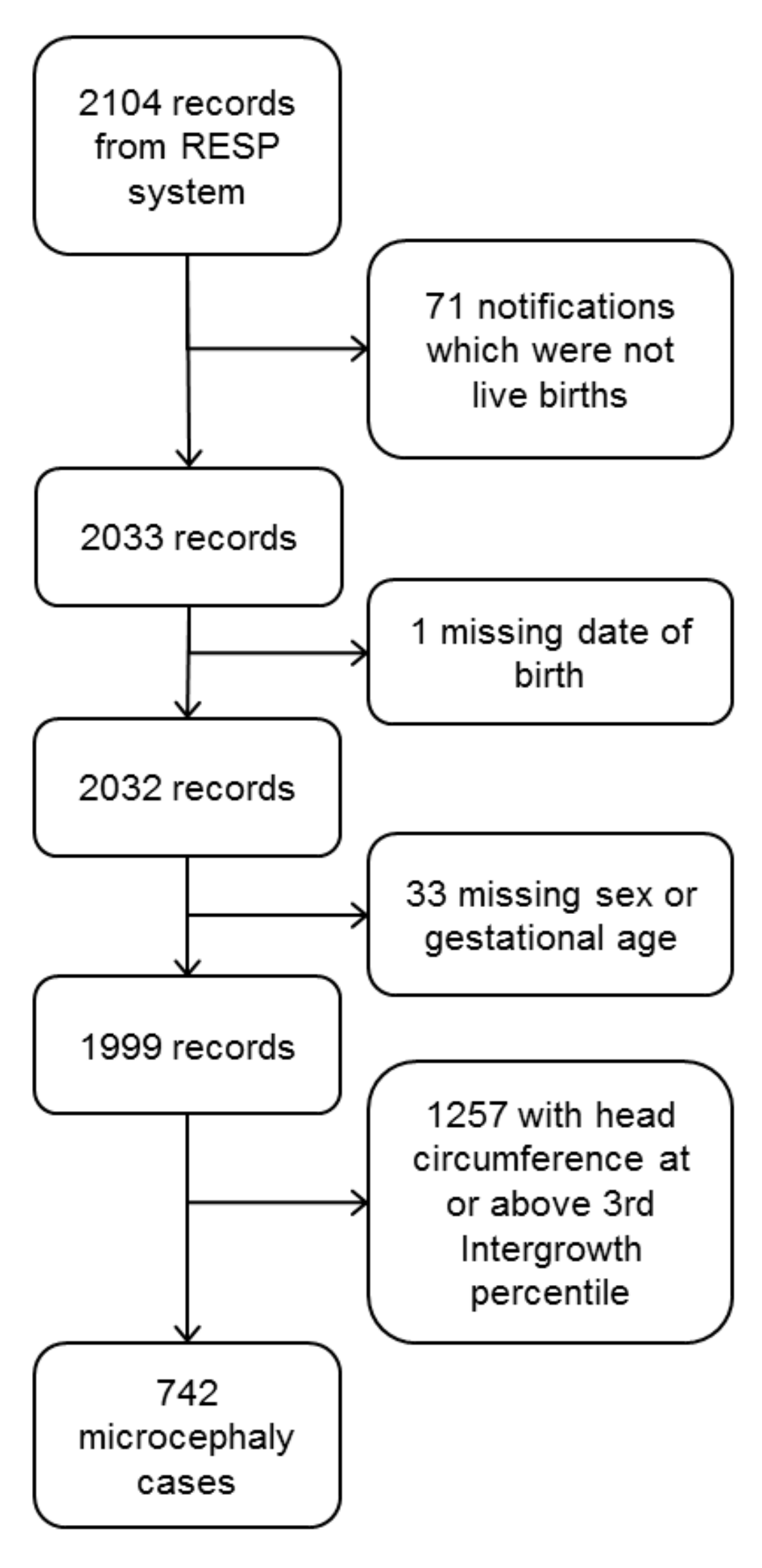
2.2. Microcephaly Surveillance
2.3. Live Birth Denominator
2.4. Statistical Analysis and Reporting
2.5. Ethics
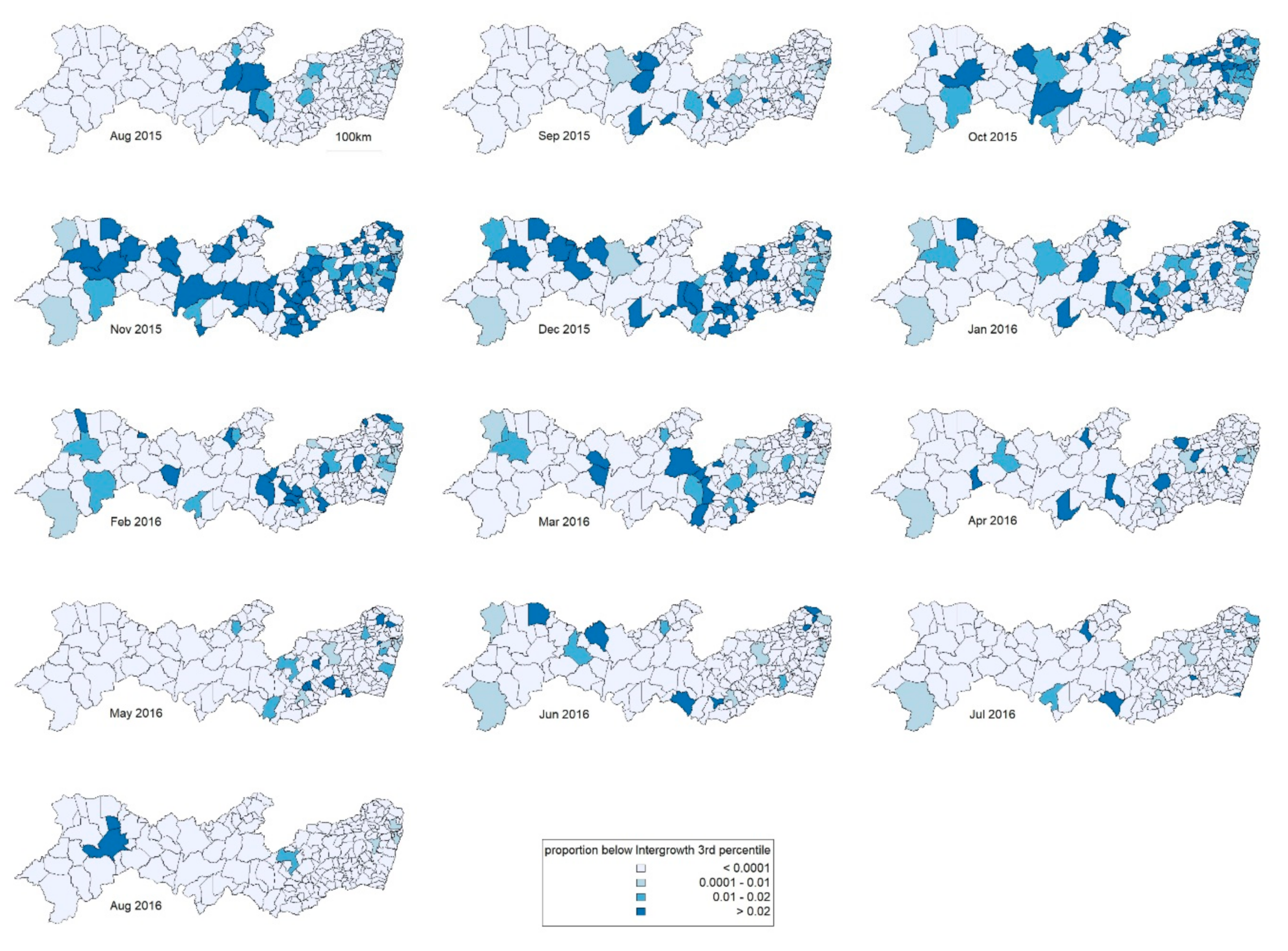
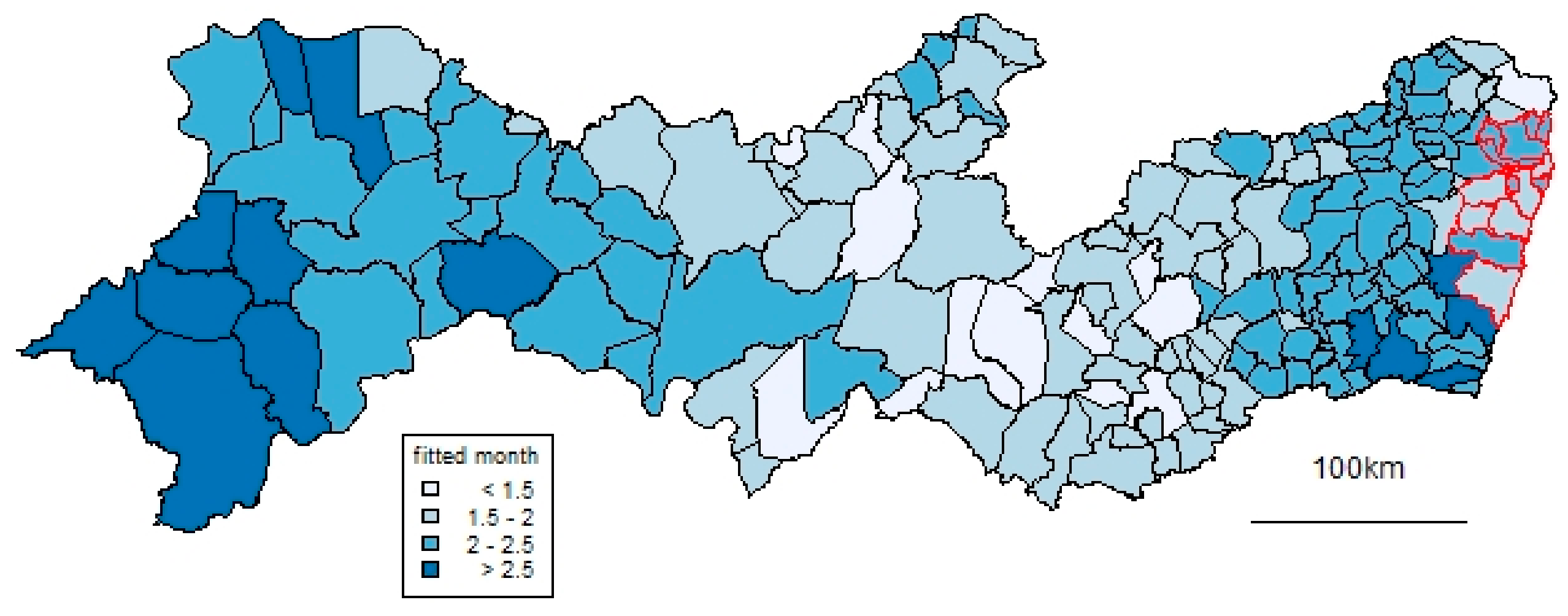
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ministério da Saúde. Ministério da Saúde Investiga Aumento de Casos de Microcefalia em Pernambuco. Available online: http://portalms.saude.gov.br/noticias/agencia-saude/20629-ministerio-da-saude-investiga-aumento-de-casos-de-microcefalia-em-pernambuco (accessed on 30 September 2018).
- Garcia, E.; Yactayo, S.; Nishino, K.; Millot, V.; Perea, W.; Briand, S. Zika virus infection: Global update on epidemiology and potentially associated clinical manifestations. Wkly. Epidemiol. Record 2016, 91, 73–81. [Google Scholar]
- Rasmussen, S.A.; Jamieson, D.J.; Honein, M.A.; Petersen, L.R. Zika Virus and Birth Defects—Reviewing the Evidence for Causality. N. Engl. J. Med. 2016, 374, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Congenital Zika Syndrome & Other Birth Defects. Available online: https://www.cdc.gov/pregnancy/zika/testing-follow-up/zika-syndrome-birth-defects.html (accessed on 22 September 2018).
- Baud, D.; Gubler, D.J.; Schaub, B.; Lanteri, M.C.; Musso, D. An update on Zika virus infection. Lancet 2017, 390, 2099–2109. [Google Scholar] [CrossRef] [Green Version]
- von der Hagen, M.; Pivarcsi, M.; Liebe, J.; von Bernuth, H.; Didonato, N.; Hennermann, J.B.; Buhrer, C.; Wieczorek, D.; Kaindl, A.M. Diagnostic approach to microcephaly in childhood: A two-center study and review of the literature. Dev. Med. Child Neurol. 2014, 56, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Filho, D.d.B.; Martelli, C.M.; Ximenes, R.A.; Araujo, T.V.; Rocha, M.A.; Ramos, R.C.; Dhalia, R.; Franca, R.F.; Marques Junior, E.T.; Rodrigues, L.C. Initial description of the presumed Congenital Zika Syndrome. Am. J. Public Health 2016, 106, 598–600. [Google Scholar] [CrossRef]
- Ministério da Saúde. Síndrome congênita associada à infecção pelo vírus Zika: Situação Epidemiológica, Ações Desenvolvidas e Desafios de 2015 a 2019. Boletim Epidemiológico 2019. Número Especial. [Google Scholar]
- Marinho, F.; de Araújo, V.E.M.; Porto, D.L.; Ferreira, H.L.; Coelho, M.R.S.; Lecca, R.C.R.; de Oliveira, H.; Poncioni, I.P.d.A.; Maranhão, M.H.N.; Mendes, Y.M.M.B. Microcephaly in Brazil: Prevalence and characterization of cases from the Information System on Live Births (Sinasc), 2000–2015. Epidemiol. Serv. Saude 2016, 25, 701–712. [Google Scholar] [CrossRef]
- de Oliveira, W.K.; de Franca, G.V.A.; Carmo, E.H.; Duncan, B.B.; de Souza Kuchenbecker, R.; Schmidt, M.I. Infection-related microcephaly after the 2015 and 2016 Zika virus outbreaks in Brazil: A surveillance-based analysis. Lancet 2017, 390, 861–870. [Google Scholar] [CrossRef] [Green Version]
- França, G.V.A.; Pedi, V.D.; Garcia, M.H.d.O.; do Carmo, G.M.I.; Leal, M.B.; Garcia, L.P. Congenital syndrome associated with Zika virus infection among live births in Brazil: A description of the distribution of reported and confirmed cases in 2015–2016. Epidemiol. Serv. Saude 2018, 27, e2017473. [Google Scholar]
- Vissoci, J.R.N.; Rocha, T.A.H.; Silva, N.C.D.; de Sousa Queiroz, R.C.; Thomaz, E.; Amaral, P.V.M.; Lein, A.; Branco, M.; Aquino, J.J.; Rodrigues, Z.M.R.; et al. Zika virus infection and microcephaly: Evidence regarding geospatial associations. PLoS Negl. Trop. Dis. 2018, 12, e0006392. [Google Scholar] [CrossRef] [Green Version]
- Souza, W.V.; Albuquerque, M.; Vazquez, E.; Bezerra, L.C.A.; Mendes, A.; Lyra, T.M.; Araujo, T.V.B.; Oliveira, A.L.S.; Braga, M.C.; Ximenes, R.A.A.; et al. Microcephaly epidemic related to the Zika virus and living conditions in Recife, Northeast Brazil. BMC Public Health 2018, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Brady, O.J.; Osgood-Zimmerman, A.; Kassebaum, N.J.; Ray, S.E.; de Araujo, V.E.M.; da Nobrega, A.A.; Frutuoso, L.C.V.; Lecca, R.C.R.; Stevens, A.; Zoca de Oliveira, B.; et al. The association between Zika virus infection and microcephaly in Brazil 2015-2017: An observational analysis of over 4 million births. PLoS Med. 2019, 16, e1002755. [Google Scholar] [CrossRef] [PubMed]
- Instituto de Pesquisa Econômica Aplicada; Fundação João Pinheiro; Programa das Nações Unidas para o Desenvolvimento. Atlas do Desenvolvimento Humano nas Regiões Metropolitanas Brasileiras; Instituto de Pesquisa Econômica Aplicada: Brasília, Brazil, 2014.
- França, G.V.; Schuler-Faccini, L.; Oliveira, W.K.; Henriques, C.M.; Carmo, E.H.; Pedi, V.D.; Nunes, M.L.; Castro, M.C.; Serruya, S.; Silveira, M.F.; et al. Congenital Zika virus syndrome in Brazil: A case series of the first 1501 livebirths with complete investigation. Lancet 2016, 388, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde. Protocolo de Vigilância e Resposta à Ocorrência de Microcefalia Relacionada à Infecção pelo Vírus Zika; Ministério da Saúde: Brasília, Brazil, 2015.
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Spiegelhalter, D.; Thomas, A.; Best, N.; Lunn, D. WinBUGS Version 1.4 User Manual; MRC Biostatistics Unit: Cambridge, UK, 2003. [Google Scholar]
- Lawson, A. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology, 2nd ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2013. [Google Scholar]
- Knorr-Held, L. Bayesian modelling of inseparable space-time variation in disease risk. Stat. Med. 2000, 19, 2555–2567. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sorensen, H.T.; von Elm, E.; Langan, S.M.; RECORD Working Committee. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Kraemer, M.U.; Brady, O.J.; Pigott, D.M.; Shearer, F.M.; Weiss, D.J.; Golding, N.; Ruktanonchai, C.W.; Gething, P.W.; Cohn, E.; et al. Mapping global environmental suitability for Zika virus. eLife 2016, 5. [Google Scholar] [CrossRef]
- de Araujo, T.V.B.; Ximenes, R.A.A.; Miranda-Filho, D.B.; Souza, W.V.; Montarroyos, U.R.; de Melo, A.P.L.; Valongueiro, S.; de Albuquerque, M.; Braga, C.; Filho, S.P.B.; et al. Association between microcephaly, Zika virus infection, and other risk factors in Brazil: Final report of a case-control study. Lancet Infect. Dis. 2017. [Google Scholar] [CrossRef] [Green Version]
- Alvarado-Socarras, J.L.; Idrovo, A.J.; Contreras-Garcia, G.A.; Rodriguez-Morales, A.J.; Audcent, T.A.; Mogollon-Mendoza, A.C.; Paniz-Mondolfi, A. Congenital microcephaly: A diagnostic challenge during Zika epidemics. Travel Med. Infect. Dis. 2018, 23, 14–20. [Google Scholar] [CrossRef]
- Cragan, J.D.; Isenburg, J.L.; Parker, S.E.; Alverson, C.J.; Meyer, R.E.; Stallings, E.B.; Kirby, R.S.; Lupo, P.J.; Liu, J.S.; Seagroves, A.; et al. Population-based microcephaly surveillance in the United States, 2009 to 2013: An analysis of potential sources of variation. Birth Defects Res. A Clin. Mol. Teratol. 2016, 106, 972–982. [Google Scholar] [CrossRef] [Green Version]
- Orioli, I.M.; Dolk, H.; Lopez-Camelo, J.S.; Mattos, D.; Poletta, F.A.; Dutra, M.G.; Carvalho, F.M.; Castilla, E.E. Prevalence and clinical profile of microcephaly in South America pre-Zika, 2005–2014: Prevalence and case-control study. BMJ 2017, 359, j5018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, M.F.; Souza, W.V.; Mendes, A.D.; Lyra, T.M.; Ximenes, R.A.; Araujo, T.V.; Braga, C.; Miranda-Filho, D.B.; Martelli, C.M.; Rodrigues, L.C. Pyriproxyfen and the microcephaly epidemic in Brazil—An ecological approach to explore the hypothesis of their association. Mem. Inst. Oswaldo Cruz 2016, 111, 774–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeSilva, M.; Vazquez-Benitez, G.; Nordin, J.D.; Lipkind, H.S.; Romitti, P.A.; DeStefano, F.; Kharbanda, E.O. Tdap vaccination during pregnancy and microcephaly and other structural birth defects in offspring. JAMA 2016, 316, 1823–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paixão, E.S.; Rodrigues, M.S.; Cardim, L.L.; Oliveira, J.F.; Catharina, L.C.; Costa, M.; Barreto, M.L.; Rodrigues, L.C.; Smeeth, L.; Andrade, R.F.S.; et al. Impact evaluation of Zika epidemic on congenital anomalies registration in Brazil: An interrupted time series analysis. PLoS Negl. Trop. Dis. 2019, 13, e0007721. [Google Scholar] [CrossRef]
- Elliott, P.; Martuzzi, M.; Shaddick, G. Spatial statistical methods in environmental epidemiology: A critique. Stat. Methods Med. Res. 1995, 4, 137–159. [Google Scholar] [CrossRef]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alexander, N.D.E.; Souza, W.V.; Rodrigues, L.C.; Braga, C.; Sá, A.; Albuquerque Bezerra, L.C.; Turchi Martelli, C.M., on behalf of the Microcephaly Epidemic Research Group (MERG). Spatiotemporal Analysis of the Population Risk of Congenital Microcephaly in Pernambuco State, Brazil. Int. J. Environ. Res. Public Health 2020, 17, 700. https://doi.org/10.3390/ijerph17030700
Alexander NDE, Souza WV, Rodrigues LC, Braga C, Sá A, Albuquerque Bezerra LC, Turchi Martelli CM on behalf of the Microcephaly Epidemic Research Group (MERG). Spatiotemporal Analysis of the Population Risk of Congenital Microcephaly in Pernambuco State, Brazil. International Journal of Environmental Research and Public Health. 2020; 17(3):700. https://doi.org/10.3390/ijerph17030700
Chicago/Turabian StyleAlexander, Neal D. E., Wayner V. Souza, Laura C. Rodrigues, Cynthia Braga, André Sá, Luciana Caroline Albuquerque Bezerra, and Celina Maria Turchi Martelli on behalf of the Microcephaly Epidemic Research Group (MERG). 2020. "Spatiotemporal Analysis of the Population Risk of Congenital Microcephaly in Pernambuco State, Brazil" International Journal of Environmental Research and Public Health 17, no. 3: 700. https://doi.org/10.3390/ijerph17030700