Predictive Validity, Diagnostic Accuracy and Test-Retest Reliability of the Strength of Urges to Drink (SUTD) Scale

 ,
,
Abstract
:1. Introduction
- Test-retest reliability of the SUTD compared to the AUDIT.
- Predictive validity of the SUTD compared to the AUDIT in relation to (a) reported attempts to reduce alcohol consumption between baseline and follow-up; (b) reported alcohol consumption at follow-up and (c) change in alcohol consumption between baseline and follow-up.
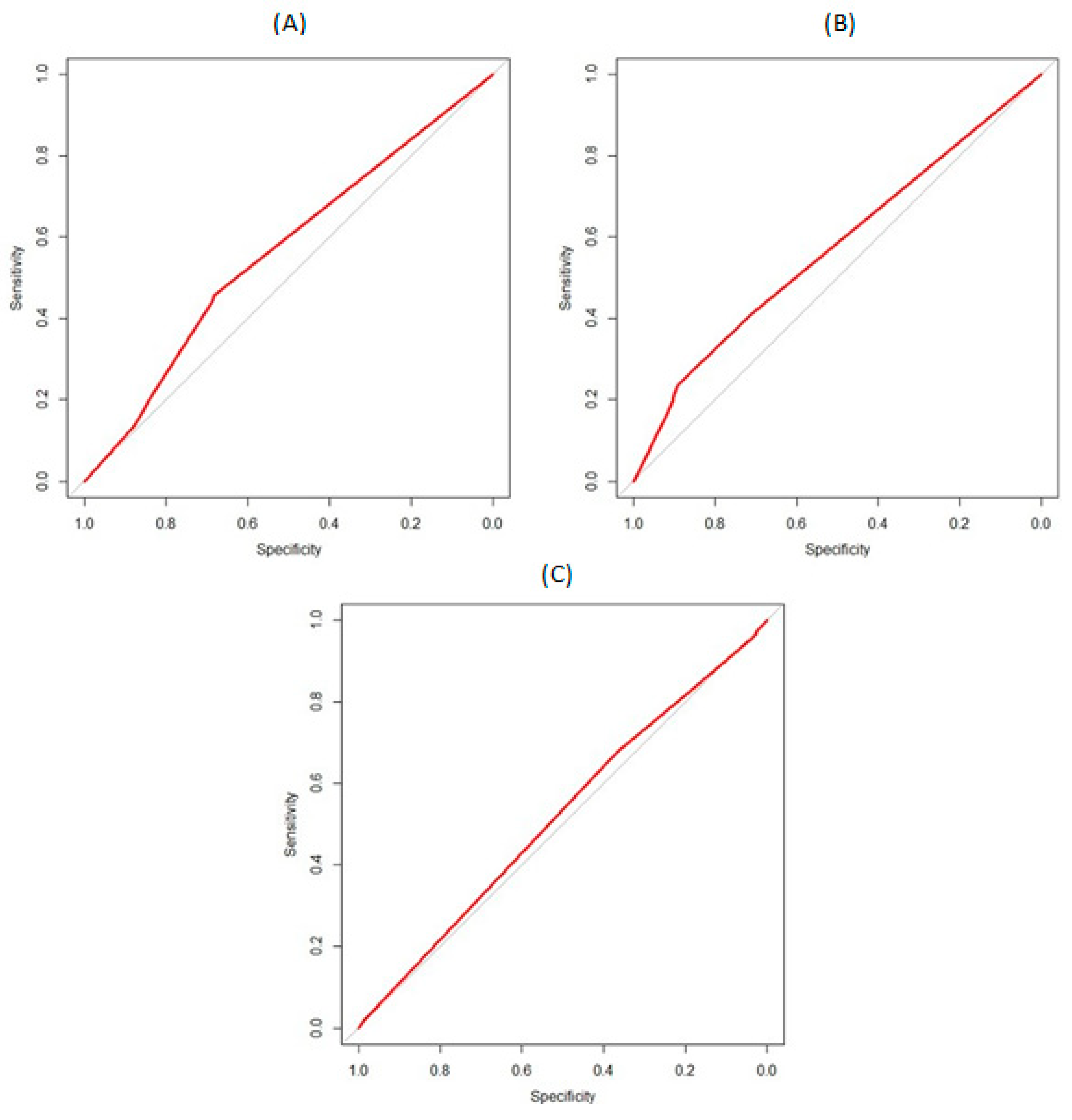
- Diagnostic accuracy of the SUTD compared to the AUDIT in relation to (a) attempts to reduce alcohol consumption between baseline and follow-up; (b) alcohol consumption at follow-up and (c) change in alcohol consumption between baseline and follow-up.
2. Methods
2.1. Design and Setting
2.2. Participants
2.3. Ethical Approval
2.4. Measures
- “How often do you have a drink containing alcohol?” Responses include: never, monthly or less, 2–4 times a month, 2–3 times a week and 4+ times a week.
- “How many units of alcohol do you drink on a typical day when you are drinking?” Responses include: 1–2 drinks, 3–4 drinks, 5–6 drinks, 7–9 drinks and 10+ drinkers.
2.5. Analyses
3. Results
3.1. Test-Retest Reliability
3.2. Predictive Validity
3.2.1. Attempts to Cut Down between Baseline and 6-Month Follow-Up
3.2.2. Reported Alcohol Consumption at 6-Month Follow-Up
All Participants
Participants Cutting Down at Baseline
3.2.3. Change in Alcohol Consumption between Baseline and 6-Month Follow-Up
All Participants
Participants Cutting Down at Baseline
3.3. Diagnostic Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ATS | Alcohol Toolkit Study |
| AUDIT | Alcohol Use Disorders Identification Test |
| SUTD | Strength of Urges to Drink |
References
- World Health Organization. Global Status Report on Alcohol and Health-2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Health and Social Care Information Centre. Statistics on Alcohol. 2016. Available online: https://www.gov.uk/government/statistics/statistics-on-alcohol-england-2016 (accessed on 19 August 2019).
- HSCIC. Statistics on Alcohol. 2015. Available online: http://www.hscic.gov.uk/catalogue/PUB17712/alc-eng-2015-rep.pdf (accessed on 19 August 2019).
- Beard, E.; Brown, J.; Michie, S.; Kaner, E.; Meier, P.; West, R. Use of aids for smoking cessation and alcohol reduction: A population survey of adults in England. BMC Public Health 2016, 16, 1237. [Google Scholar] [CrossRef] [PubMed]
- Lago, L.; Bruno, R.; Degenhardt, L. Concordance of ICD-11 and DSM-5 definitions of alcohol and cannabis use disorders: A population survey. Lancet Psychiatry 2016, 3, 673–684. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Washington, DC, USA, 2013. [Google Scholar]
- Reid, M.C.; Fiellin, D.A.; O’Connor, P.G. Hazardous and harmful alcohol consumption in primary care. Arch. Intern. Med. 1999, 159, 1681–1689. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care, 2nd ed.; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Bohn, M.J.; Babor, T.F.; Kranzler, H.R. The Alcohol Use Disorders Identification Test (AUDIT): Validation of a screening instrument for use in medical settings. J. Stud. Alcohol 1995, 56, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.P.; Litten, R.Z.; Fertig, J.B.; Babor, T. A Review of Research on the Alcohol Use Disorders Identification Test (AUDIT). Alcohol. Clin. Exp. Res. 1997, 21, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test (AUDIT): A review of recent research. Alcohol. Clin. Exp. Res. 2002, 26, 272–279. [Google Scholar] [CrossRef]
- Frank, D.; DeBenedetti, A.F.; Volk, R.J.; Williams, E.C.; Kivlahan, D.R.; Bradley, K.A. Effectiveness of the AUDIT-C as a Screening Test for Alcohol Misuse in Three Race/Ethnic Groups. J. Gen. Intern. Med. 2008, 23, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Li, T.K.; Hewitt, B.G.; Grant, B.F. The Alcohol Dependence Syndrome, 30 years later: A commentary. Addiction 2007, 102, 1522–1530. [Google Scholar] [CrossRef]
- Hasin, D.S.; Liu, X.; Alderson, D.; Grant, B.F. DSM-IV alcohol dependence: A categorical or dimensional phenotype? Psychol. Med. 2006, 36, 1695–1705. [Google Scholar] [CrossRef]
- Saunders, J.B.; Lee, N.K. Hazardous alcohol use: Its delineation as a subthreshold disorder, and approaches to its diagnosis and management. Compr. Psychiatry 2000, 41, 95–103. [Google Scholar] [CrossRef]
- Edwards, G.; Gross, M.M. Alcohol dependence: Provisional description of a clinical syndrome. Br. Med. J. 1976, 1, 1058. [Google Scholar] [CrossRef] [PubMed]
- Baker, T.B.; Morse, E.; Sherman, J.E. The Motivation to Use Drugs: A Psychobiological Analysis of Urges; Nebraska Symposium on Motivation; University of Nebraska Press: Lincoln, NE, USA, 1986. [Google Scholar]
- West, R.; Brown, J. Theory of Addiction; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Fidler, J.A.; Shahab, L.; West, R. Strength of urges to smoke as a measure of severity of cigarette dependence: Comparison with the Fagerström Test for Nicotine Dependence and its components. Addiction 2011, 106, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Kotz, D.; Brown, J.; West, R. Predictive validity of the Motivation to Stop Scale (MTSS): A single-item measure of motivation to stop smoking. Drug Alcohol Depend. 2013, 128, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Volkow, N.D. Neurocircuitry of addiction. Neuropsychopharmacology 2010, 35, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Garbutt, J.C.; West, S.L.; Carey, T.S.; Lohr, K.N.; Crews, F.T. Pharmacological treatment of alcohol dependence: A review of the evidence. JAMA 1999, 281, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.M.; Stojek, M.K.; Few, L.R.; Rothbaum, A.O.; MacKillop, J. Craving as an alcohol use disorder symptom in DSM-5: An empirical examination in a treatment-seeking sample. Exp. Clin. Psychopharmacol. 2014, 22, 43. [Google Scholar] [CrossRef] [PubMed]
- Bohn, M.J.; Krahn, D.D.; Staehler, B.A. Development and initial validation of a measure of drinking urges in abstinent alcoholics. Alcohol. Clin. Exp. Res. 1995, 19, 600–606. [Google Scholar] [CrossRef]
- Singleton, E.; Tiffany, S.; Henningfield, J. Development and validation of a new questionnaire to assess craving for alcohol: Problems of drug dependence. In Proceedings of the 56th Annual Meeting, The College on Problems of Drug Dependence, National Institute on Drug Abuse, Rockville, MD, USA, 18–23 June 1994; p. 289. [Google Scholar]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Delgado, P.; Heninger, G.R.; Charney, D.S. The yale-brown obsessive compulsive scale: II. Validity. Arch. Gen. Psychiatry 1989, 46, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, T.; Murphy, D.; Hodgson, R. The severity of alcohol dependence questionnaire: Its use, reliability and validity. Addiction 1983, 78, 145–155. [Google Scholar] [CrossRef]
- Drobes, D.J.; Thomas, S.E. Assessing craving for alcohol. Alcohol Res. Health 1999, 23, 179–186. [Google Scholar] [PubMed]
- Dev, R.; Parsons, H.A.; Palla, S.; Palmer, J.L.; Del Fabbro, E.; Bruera, E. Undocumented alcoholism and its correlation with tobacco and illegal drug use in advanced cancer patients. Cancer 2011, 117, 4551–4556. [Google Scholar] [CrossRef] [Green Version]
- Scott, C.M.; Popovich, D.J. Undiagnosed alcoholism & prescription drug misuse among the elderly. Special considerations for home assessment. Caring 2001, 20, 20–23. [Google Scholar] [PubMed]
- Beard, E.; Brown, J.; West, R.; Acton, C.; Brennan, A.; Drummond, C.; Hickman, M.; Holmes, J.; Kaner, E.; Lock, K. Protocol for a national monthly survey of alcohol use in England with 6-month follow-up: ‘The Alcohol Toolkit Study’. BMC Public Health 2015, 15, 230. [Google Scholar] [CrossRef] [PubMed]
- What Is ACORN? Available online: http://www.caci.co.uk/acorn/ (accessed on 19 August 2019).
- Conigrave, K.M.; Saunders, J.B.; Reznik, R.B. Predictive capacity of the AUDIT questionnaire for alcohol-related harm. Addiction 1995, 90, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Kaarne, T.; Aalto, M.; Kuokkanen, M.; Seppa, K. AUDIT-C, AUDIT-3 and AUDIT-QF in screening risky drinking among Finnish occupational health-care patients. Drug Alcohol Rev. 2010, 29, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Meneses-Gaya, C.; Zuardi, A.W.; Loureiro, S.R.; Hallak, J.E.; Trzesniak, C.; de Azevedo Marques, J.M.; Machado-de-Sousa, J.P.; Chagas, M.H.; Souza, R.M.; Crippa, J.A. Is the full version of the AUDIT really necessary? Study of the validity and internal construct of its abbreviated versions. Alcohol. Clin. Exp. Res. 2010, 34, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Peacock, J.L.; Sauzet, O.; Ewings, S.M.; Kerry, S.M. Dichotomising continuous data while retaining statistical power using a distributional approach. Stat. Med. 2012, 31, 3089–3103. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selin, K.H. Test-retest reliability of the alcohol use disorder identification test in a general population sample. Alcohol. Clin. Exp. Res. 2003, 27, 1428–1435. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Chen, W.J.; Cheng, A.T. New approach to the validity of the alcohol use disorders identification test: Stratum-specific likelihood ratios analysis. Alcohol. Clin. Exp. Res. 2005, 29, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Piccinelli, M.; Tessari, E.; Bortolomasi, M.; Piasere, O.; Semenzin, M.; Garzotto, N.; Tansella, M. Efficacy of the alcohol use disorders identification test as a screening tool for hazardous alcohol intake and related disorders in primary care: A validity study. BMJ 1997, 314, 420. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.; Jayawardana, P.; Pathmeswaran, A. Concurrent validity of the alcohol use disorders identification test (AUDIT). Alcohol Alcohol. 2008, 43, 49–50. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, R.D.; Pearson, M.R.; Sargent, E.M.; Stevenson, B.L.; Mfon, A.M. Daily associations between emotional functioning and alcohol involvement: Moderating effects of response inhibition and gender. Drug Alcohol Depend. 2016, 163 (Suppl. 1), S46–S53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.; West, R.; Angus, C.; Beard, E.; Brennan, A.; Drummond, C.; Hickman, M.; Holmes, J.; Kaner, E.; Michie, S. Comparison of brief interventions in primary care on smoking and excessive alcohol consumption: A population survey in England. Br. J. Gen. Pract. 2016, 66, e1–e9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All High-Risk Drinkers (n = 14,639) | Followed-Up (n = 2960) | Not Followed-Up (n = 11,679) | p | ||||
|---|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | ||
| Gender | |||||||
| Female | 35.1 | 34.4 to 35.9 | 35.1 | 33.4 to 36.9 | 35.1 | 34.3 to 36.0 | >0.990 |
| Male | 64.9 | 64.1 to 65.6 | 64.9 | 62.1 to 66.6 | 64.9 | 64.0 to 65.7 | |
| Age | |||||||
| 16–24 | 20.5 | 19.9 to 21.2 | 11.9 | 10.8 to 13.2 | 22.7 | 21.9 to 23.5 | <0.001 |
| 25–34 | 14.5 | 13.9 to 15.1 | 9.4 | 8.4 to 10.5 | 15.8 | 15.1 to 16.4 | |
| 35–44 | 14.5 | 13.9 to 15.0 | 13.9 | 12.6 to 15.2 | 14.6 | 14.0 to 15.3 | |
| 45–54 | 17.9 | 17.3 to 18.6 | 20.5 | 19.1 to 22.1 | 17.3 | 16.6 to 18.0 | |
| 55–64 | 16.7 | 16.1 to 17.3 | 21.9 | 20.5 to 23.5 | 15.3 | 14.7 to 16.0 | |
| 65+ | 16.0 | 15.4 to 16.6 | 22.3 | 20.9 to 23.9 | 14.3 | 13.7 to 15.0 | |
| Social grade | |||||||
| ABC1 | 62.0 | 61.2 to 62.8 | 70.1 | 68.4 to 71.7 | 59.9 | 59.0 to 60.8 | <0.001 |
| C2DE | 38.0 | 37.2 to 38.8 | 29.9 | 28.3 to 31.6 | 40.1 | 39.2 to 41.0 | |
| Educational qualification | |||||||
| Voluntary | 71.9 | 71.2 to 72.7 | 74.7 | 73.1 to 76.2 | 71.2 | 70.4 to 72.0 | <0.001 |
| Non-voluntary | 28.1 | 27.3 to 28.8 | 71.2 | 70.4 to 72.0 | 28.8 | 29.6 to 28.0 | |
| Disability | |||||||
| Yes | 8.6 | 8.1 to 9.0 | 11.1 | 10.0 to 12.3 | 7.9 | 7.4 to 8.4 | <0.001 |
| No | 91.4 | 91.0 to 91.9 | 88.9 | 87.7 to 90.0 | 92.1 | 91.6 to 92.6 | |
| Ethnicity | |||||||
| White | 95.4 | 95.1 to 95.8 | 96.3 | 95.6 to 97.0 | 95.2 | 94.8 to 95.6 | 0.011 |
| Other | 4.6 | 4.9 to 4.2 | 3.7 | 3.0 to 4.4 | 4.8 | 4.4 to 5.2 | |
| Government Office Region | |||||||
| North | 58.6 | 57.8 to 59.4 | 57.5 | 55.7 to 59.3 | 58.9 | 58.0 to 59.8 | 0.153 |
| South | 41.4 | 40.6 to 42.2 | 42.5 | 40.7 to 44.3 | 41.4 | 40.2 to 40.2 | |
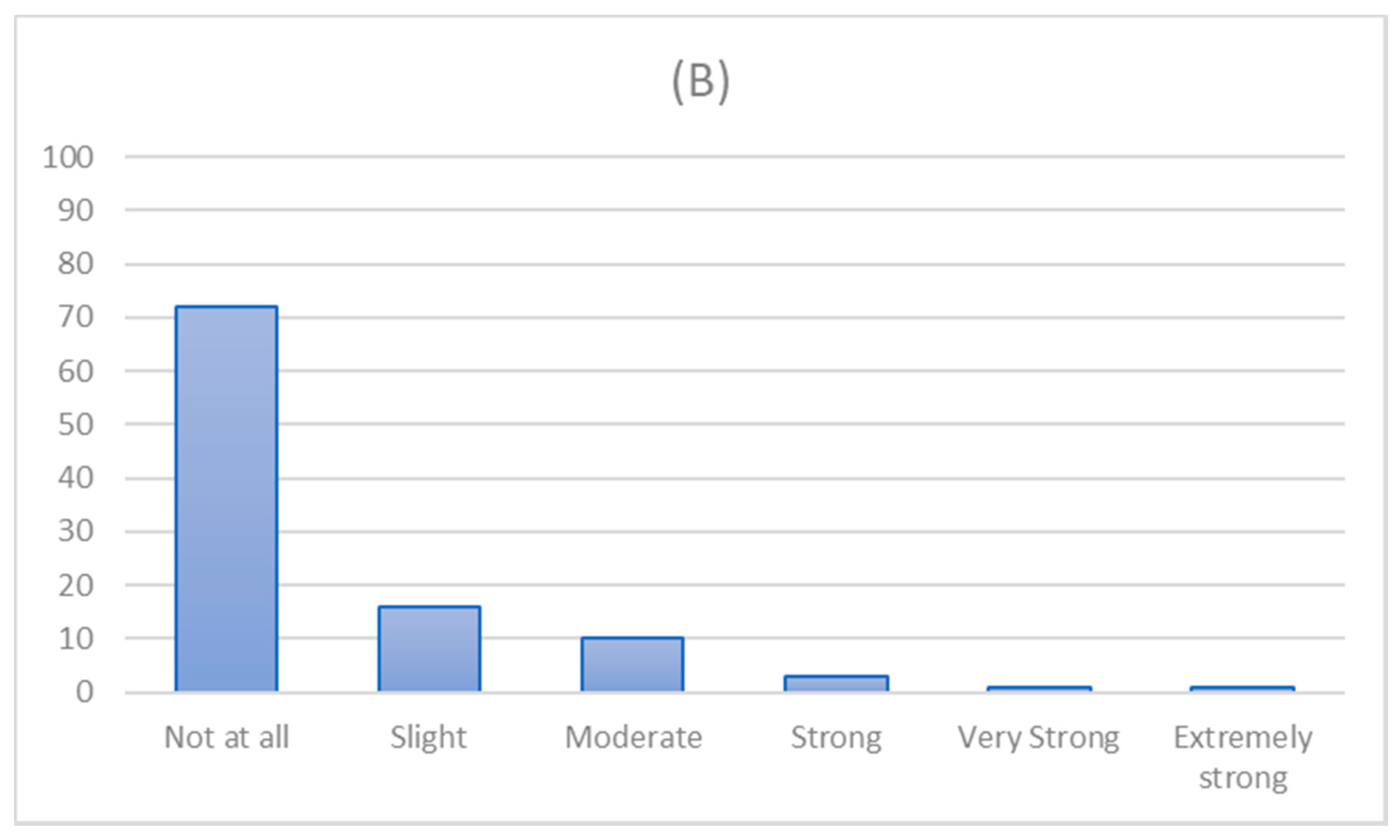
| Urges to drink (baseline) | |||||||
| Not at all | 64.1 | 63.4 to 64.9 | 64.7 | 63.0 to 66.4 | 64.0 | 63.1 to 64.9 | 0.382 |
| Slight | 17.1 | 16.5 to 17.7 | 17.0 | 15.7 to 18.4 | 17.1 | 16.4 to 17.8 | |
| Moderate | 12.9 | 12.3 to 13.4 | 13.2 | 12 to 14.5 | 12.8 | 12.2 to 13.4 | |
| Strong | 3.5 | 3.2 to 3.8 | 2.9 | 2.3 to 2.6 | 3.6 | 3.3 to 4.0 | |
| Very strong | 1.4 | 1.3 to 1.6 | 1.3 | 0.9 to 1.8 | 1.5 | 1.3 to 1.7 | |
| Extremely strong | 0.9 | 0.7 to 1.0 | 0.8 | 0.5 to 1.2 | 0.9 | 0.7 to 1.1 | |
| Cutting down (baseline) | |||||||
| Yes | 19.8 | 19.1 to 20.4 | 23.4 | 21.9 to 25.0 | 18.9 | 18.2 to 19.6 | |
| No | 80.2 | 79.6 to 80.9 | 76.6 | 75.0 to 78.1 | 81.1 | 80.4 to 81.8 | <0.001 |
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | ||
| AUDIT-score (baseline) | 8.5 | 8.4 to 8.6 | 8.3 | 8.2 to 8.5 | 8.5 | 8.5 to 8.6 | 0.218 |
| Levels of Urges to Drink at Baseline | Attempt to Cut Down at Follow-Up % (n) | OR | 95% CI | Adjusted OR | 95% CI | |||
| SUTD | No | Yes | Lower | Upper | Lower | Upper | ||
| Not at all | 78.8 (1510) | 21.2 (406) | ||||||
| Slight | 65.7 (331) | 34.3 (173) | 1.94 | 1.57 *** | 2.41 | 1.78 *** | 1.43 | 2.22 |
| Moderate | 65.7 (257) | 34.3 (134) | 1.94 | 1.53 *** | 2.45 | 1.54 *** | 1.20 | 1.96 |
| Strong | 65.1 (56) | 34.9 (30) | 1.99 | 1.25 ** | 3.12 | 1.43 | 0.87 | 2.30 |
| Very strong | 63.2 (24) | 36.8 (14) | 2.17 | 1.09 * | 4.18 | 1.62 | 0.79 | 3.22 |
| Extremely strong | 62.5 (15) | 37.5 (9) | 2.23 | 0.93 | 5.05 | 1.16 | 0.45 | 2.78 |
| SUTD-3 | ||||||||
| Not all | 78.8 (1510) | 21.2 (406) | ||||||
| Slight | 65.7 (331) | 34.3 (173) | 1.94 *** | 1.57 | 2.41 | 1.78 *** | 1.43 | 2.22 |
| >Moderate | 65.3 (352) | 34.7 (187) | 1.98 *** | 1.60 | 2.43 | 1.51 *** | 1.21 | 1.88 |
| Levels of Urges to Drink at Baseline | Mean (SD) Consumption at Follow-Up | Β | 95% CI | Adjusted β | 95% CI | |||
| Lower | Upper | Lower | Upper | |||||
| Not at all | 4.46 (1.48) | |||||||
| Slight | 4.77 (1.39) | 0.30 *** | 0.16 | 0.45 | 0.22 ** | 0.08 | 0.35 | |
| Moderate | 5.23 (1.39) | 0.77 *** | 0.61 | 0.93 | 0.53 *** | 0.38 | 0.69 | |
| Strong | 5.27 (1.45) | 0.80 *** | 0.49 | 1.12 | 0.40 * | 0.09 | 0.70 | |
| Very strong | 5.03 (1.73) | 0.56 * | 0.09 | 1.03 | 0.19 | −0.26 | 0.64 | |
| Extremely strong | 5.26 (2.40) | 0.80 ** | 0.20 | 1.40 | −0.22 | −0.81 | 0.36 | |
| SUTD-3 | ||||||||
| Not all | 4.46 (1.48) | |||||||
| Slight | 4.77 (1.39) | 0.30 *** | 0.16 | 0.45 | 0.22 ** | 0.08 | 0.35 | |
| >Moderate | 5.22 (1.48) | 0.78 *** | 0.62 | 0.90 | 0.46 *** | 0.32 | 0.60 | |
| Levels of Urges to Drink at Baseline | Change Consumption (Follow-Up—Baseline) a | Β | 95% CI | Adjusted β | 95% CI | |||
| Lower | Upper | Lower | Upper | |||||
| Not at all | 0.39 (1.51) | |||||||
| Slight | 0.24 (1.43) | −0.14 | −0.29 | 0.00 | −0.16 * | −0.31 | −0.02 | |
| Moderate | 0.06 (1.43) | −0.33 *** | −0.49 | −0.16 | −0.40 *** | −0.56 | −0.24 | |
| Strong | 0.22 (1.25) | −0.17 | −0.49 | 0.16 | −0.37 * | −0.69 | −0.05 | |
| Very strong | 0.29 (1.80) | −0.10 | −0.58 | 0.38 | −0.36 | −0.84 | 0.12 | |
| Extremely strong | 1.43 (2.43) | 1.05 *** | 0.44 | 1.66 | 0.47 | −0.15 | 1.09 | |
| SUTD-3 | ||||||||
| Not all | 0.39 (1.51) | |||||||
| Slight | 0.24 (1.43) | −0.14 | −0.29 | 0.00 | −0.16 * | −0.31 | −0.02 | |
| >Moderate | 0.16 (1.51) | −0.23 ** | −0.37 | −0.08 | −0.36 *** | −0.51 | −0.22 | |
| Levels of Urges to Drink at Baseline | Mean (SD) Consumption at Follow-Up | Β | 95% CI | Adjusted β | 95% CI | ||
| Lower | Upper | Lower | Upper | ||||
| Not at all | 4.74 (1.49) | ||||||
| Slight | 4.91 (1.29) | 0.15 | −0.14 | 0.45 | 0.08 | −0.20 | 0.37 |
| Moderate | 5.30 (1.51) | 0.26 | −0.31 | 0.83 * | 0.32 | 0.02 | 0.61 |
| Strong | 5.00 (1.33) | 0.55 *** | 0.25 | 0.85 | −0.12 | −0.68 | 0.45 |
| Very strong | 5.00 (2.16) | 0.26 | −0.56 | 1.09 | −0.14 | −0.95 | 0.67 |
| Extremely strong | 4.62 (3.11) | −0.11 | −1.16 | 0.93 | −1.21 * | −2.27 | −0.15 |
| SUTD−3 | |||||||
| Not all | 4.74 (1.49) | ||||||
| Slight | 4.91 (1.29) | 0.15 | −0.14 | 0.45 | 0.08 | −0.21 | 0.37 |
| >Moderate | 5.20 (1.63) | 0.45 *** | 0.19 | 0.72 | 0.18 | −0.09 | 0.45 |
| Levels of Urges to Drink at Baseline | Change Consumption (Follow-Up—Baseline) a | Β | 95% CI | Adjusted β | 95% CI | ||
| Lower | Upper | Lower | Upper | ||||
| Not at all | 0.22 (1.60) | ||||||
| Slight | −0.01 (1.32) | −0.23 | −0.55 | 0.08 | −0.20 | −0.51 | 0.12 |
| Moderate | 0.09 (1.60) | −0.13 | −0.45 | 0.19 | −0.20 | −0.52 | 0.12 |
| Strong | 0.43 (1.20) | 0.20 | −0.40 | 0.81 | −0.13 | −0.75 | 0.48 |
| Very strong | 0.46 (2.11) | 0.24 | −0.64 | 1.11 | −0.12 | −1.00 | 0.76 |
| Extremely strong | 2.75 (3.58) | 2.53 *** | 1.42 | 3.63 | 1.66 ** | 0.51 | 2.80 |
| SUTD-3 | |||||||
| Not all | 0.22 (1.60) | ||||||
| Slight | −0.01 (1.32) | −0.23 | −0.55 | 0.08 | −0.19 | −0.51 | 0.12 |
| >Moderate | 0.30 (1.79) | 0.07 | −0.22 | 0.36 | −0.13 | −0.43 | 0.16 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beard, E.; Brown, J.; West, R.; Drummond, C.; Kaner, E.; Michie, S. Predictive Validity, Diagnostic Accuracy and Test-Retest Reliability of the Strength of Urges to Drink (SUTD) Scale. Int. J. Environ. Res. Public Health 2019, 16, 3714. https://doi.org/10.3390/ijerph16193714
Beard E, Brown J, West R, Drummond C, Kaner E, Michie S. Predictive Validity, Diagnostic Accuracy and Test-Retest Reliability of the Strength of Urges to Drink (SUTD) Scale. International Journal of Environmental Research and Public Health. 2019; 16(19):3714. https://doi.org/10.3390/ijerph16193714
Chicago/Turabian StyleBeard, Emma, Jamie Brown, Robert West, Colin Drummond, Eileen Kaner, and Susan Michie. 2019. "Predictive Validity, Diagnostic Accuracy and Test-Retest Reliability of the Strength of Urges to Drink (SUTD) Scale" International Journal of Environmental Research and Public Health 16, no. 19: 3714. https://doi.org/10.3390/ijerph16193714