Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethical Approval and Consent to Participate
2.3. Measure of ARI Outcome
2.4. Measures of Exposure to IAP
2.5. Covariates and Potential Confounders
2.6. Data Analysis
3. Results
3.1. Sample Characteristics by Children’s ARI
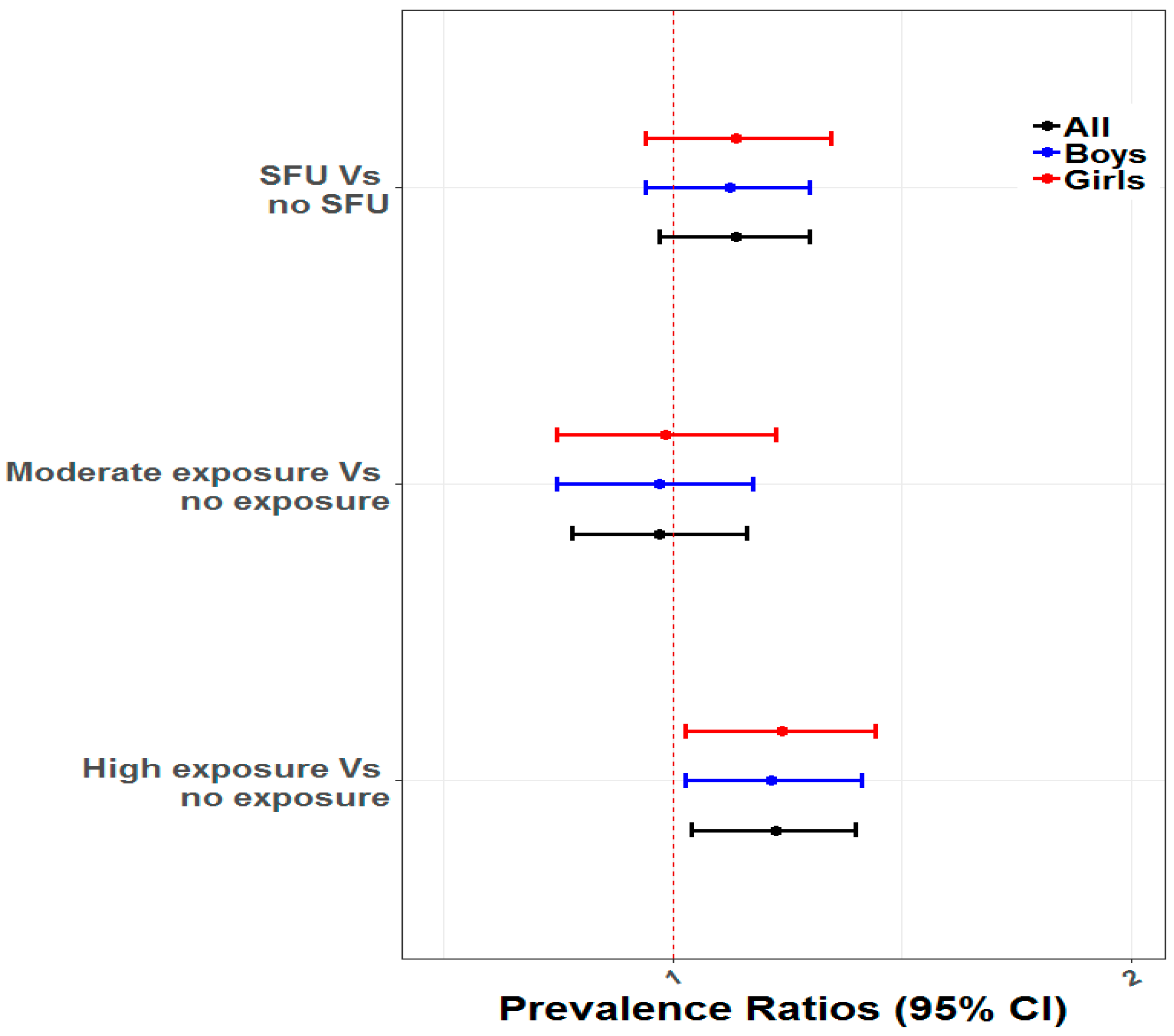
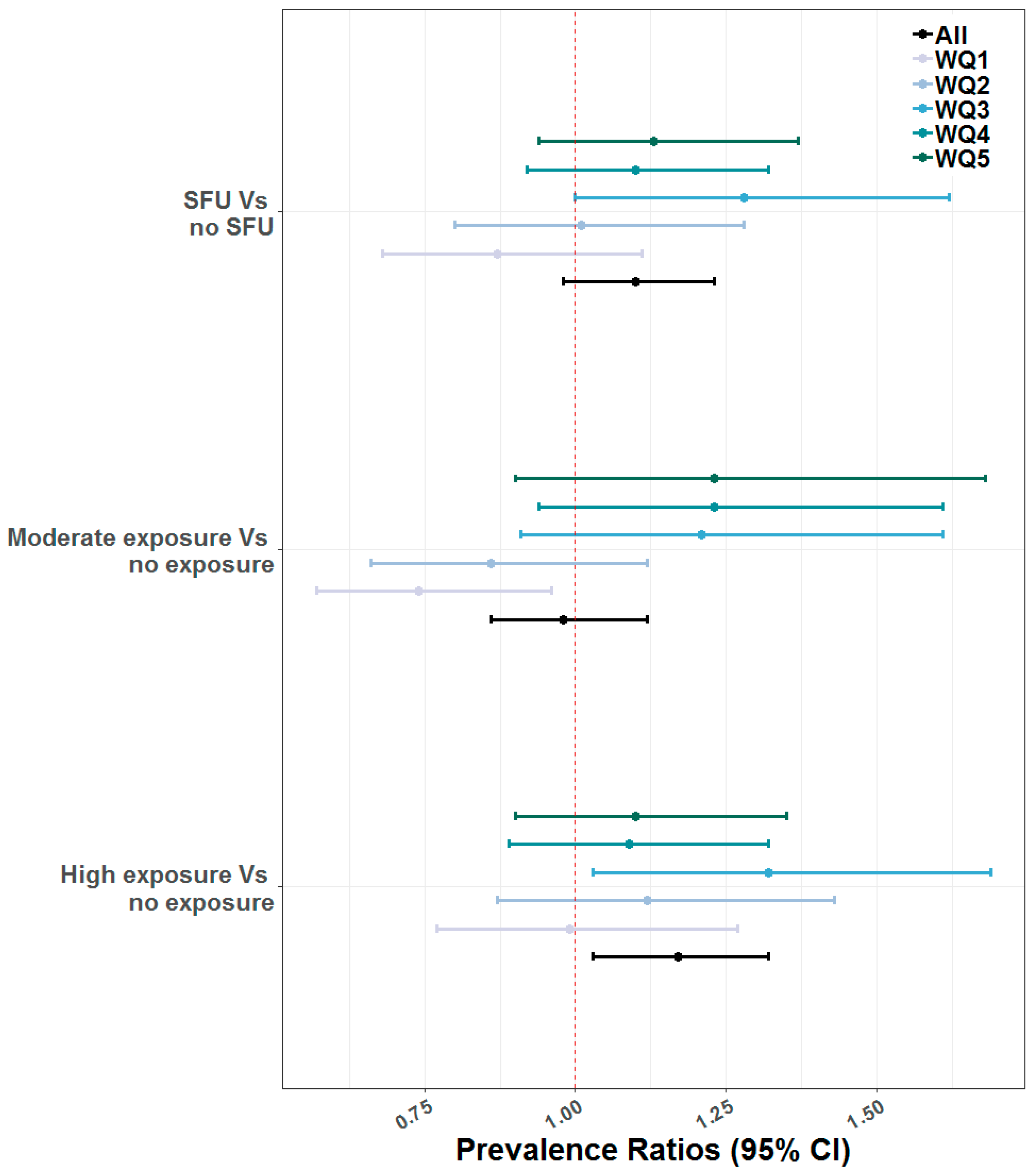
3.2. Multivariable Associations between SFU and ARI
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund (UNICEF); The World Health Organization (WHO); The World Bank. Levels and Trends in Child Malnutrition: Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Afghan Public Health Institute, Ministry of Public Health (APHI/MoPH); Central Statistics Organization (CSO) [Afghanistan]; ICF Macro; Indian Institute of Health Management Research (IIHMR) [India]; World Health Organization Regional Office for the Eastern Mediterranean (WHO/EMRO) [Egypt]. Afghanistan Mortality Survey 2010; APHI/MoPH; CSO; ICF Macro; IIHMR; WHO/EMRO: Calverton, MD, USA, 2011.
- Viswanathan, K.; Becker, S.; Hansen, P.M.; Kumar, D.; Kumar, B.; Niayesh, H.; Peters, D.H.; Burnham, G. Infant and under-five mortality in Afghanistan: Current estimates and limitations. Bull. World Health Organ. 2010, 88, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Bukalasa, J.S.; Eriksson, M. Indoor Air Pollution, Social Inequality and Acute Respiratory Diseases in Children in Tanzania; Umea University: Umeå, Sweden, 2011. [Google Scholar]
- Pollard, S.L.; Williams, D.L.; Breysse, P.N.; Baron, P.A.; Grajeda, L.M.; Gilman, R.H.; Jaime Miranda, J.; Checkley, W. A cross-sectional study of determinants of indoor environmental exposures in households with and without chronic exposure to biomass fuel smoke. Environ. Health Glob. Access Sci. Source 2014, 13, 21. [Google Scholar] [CrossRef] [PubMed]
- Adesanya, O.A.; Darboe, A.; Mendez Rojas, B.; Abiodun, D.E.; Beogo, I. Factors contributing to regional inequalities in acute respiratory infections symptoms among under-five children in Nigeria: A decomposition analysis. Int. J. Equity Health 2017, 16, 140. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.S.; Jerrett, M.; Kawachi, I.; Levy, J.I.; Cohen, A.J.; Gouveia, N.; Wilkinson, P.; Fletcher, T.; Cifuentes, L.; Schwartz, J.; et al. Health, wealth, and air pollution: Advancing theory and methods. Environ. Health Perspect. 2003, 111, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Janjua, N.Z.; Mahmood, B.; Dharma, V.K.; Sathiakumar, N.; Khan, M.I. Use of biomass fuel and acute respiratory infections in rural Pakistan. Public Health 2012, 126, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Bartington, S.E.; Bakolis, I.; Devakumar, D.; Kurmi, O.P.; Gulliver, J.; Chaube, G.; Manandhar, D.S.; Saville, N.M.; Costello, A.; Osrin, D.; et al. Patterns of domestic exposure to carbon monoxide and particulate matter in households using biomass fuel in Janakpur, Nepal. Environ. Pollut. 2017, 220, 38–45. [Google Scholar] [CrossRef]
- Chafe, Z.A.; Brauer, M.; Klimont, Z.; Van Dingenen, R.; Mehta, S.; Rao, S.; Riahi, K.; Dentener, F.; Smith, K.R. Household cooking with solid fuels contributes to ambient PM2.5 air pollution and the burden of disease. Environ. Health Perspect. 2015, 122, 1314–1320. [Google Scholar] [CrossRef]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Perera, F.P. Multiple threats to child health from fossil fuel combustion: Impacts of air pollution and climate change. Environ. Health Perspect. 2017, 125, 141–148. [Google Scholar] [CrossRef]
- Dasgupta, S.; Huq, M.; Khaliquzzaman, M.; Pandey, K.; Wheeler, D. Who suffers from indoor air pollution? Evidence from Bangladesh. Health Policy Plan. 2006, 21, 444–458. [Google Scholar] [CrossRef] [Green Version]
- Khalequzzaman, M.; Kamijima, M.; Sakai, K.; Chowdhury, N.A.; Hamajima, N.; Nakajima, T. Indoor air pollution and its impact on children under five years old in Bangladesh. Indoor Air 2007, 17, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Kantrowitz, E. Socioeconomic status and health: The potential role of environmental risk exposure. Annu. Rev. Public Health 2002, 23, 303–331. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Marcynyszyn, L.A. Environmental justice, cumulative environmental risk, and health among low- and middle-income children in upstate New York. Am. J. Public Health 2004, 94, 1942–1944. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.S.; McMichael, A.J.; Schwartz, J.; Wartenberg, D. Poverty, environment, and health: The role of environmental epidemiology and environmental epidemiologists. Epidemiology 2007, 18, 664–668. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Shrestha, P.; Kumar, S. Urban residential energy use in Kandahar, Afghanistan. Cities 2013, 32, 135–142. [Google Scholar] [CrossRef]
- Akseer, N.; Bhatti, Z.; Rizvi, A.; Salehi, A.S.; Mashal, T.; Bhutta, Z.A. Coverage and inequalities in maternal and child health interventions in Afghanistan. BMC Public Health 2016, 16, 797. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Wagstaff, A.; Schellenberg, J.A.; Gwatkin, D.; Claeson, M.; Habicht, J.P. Applying an equity lens to child health and mortality: More of the same is not enough. Lancet 2003, 362, 233–241. [Google Scholar] [CrossRef]
- CSDH. Closing the Gap in a Generation; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Marmot, M.; Bell, R. Fair society, healthy lives. Public Health 2012, 126, S4–S10. [Google Scholar] [CrossRef]
- Central Statistics Organization (CSO); Ministry of Public Health (MoPH); ICF. Afghanistan Demographic and Health Survey 2015; CSO: Kabul, Afghanistan, 2017. [Google Scholar]
- Link, B.G.; Phelan, J. Social Conditions as Fundamental Causes of Disease. J. Health Soc. Behav. 1995, 35, 80–94. [Google Scholar] [CrossRef]
- Upadhyay, A.K.; Singh, A.; Kumar, K.; Singh, A. Impact of indoor air pollution from the use of solid fuels on the incidence of life threatening respiratory illnesses in children in India. BMC Public Health 2015, 15, 300. [Google Scholar] [CrossRef]
- Naz, S.; Page, A.; Agho, K.E. Household air pollution from use of cooking fuel and under-five mortality: The role of breastfeeding status and kitchen location in Pakistan. PLoS ONE 2017, 12, e0173256. [Google Scholar] [CrossRef]
- Filmer, D.; Pritchett, L.H. Estimating Wealth Effects without Expenditure Data-or Tears: An Application to Educational Enrollments in States of India. Demography 2001, 38, 115–132. [Google Scholar]
- Currie, J. Healthy, Wealthy, and Wise: Socioeconomic Status, Poor Health in Childhood, and Human Capital Development. J. Econ. Lit. 2009, 47, 87–122. [Google Scholar] [CrossRef] [Green Version]
- Rutstein, S.O.; Johnson, K. The DHS Wealth Index, DHS Comparative Report 6; ORC Macro: Calverton, MD, USA, 2004. [Google Scholar]
- Li, Y.R.; Xiao, C.C.; Li, J.; Tang, J.; Geng, X.Y.; Cui, L.J.; Zhai, J.X. Association between air pollution and upper respiratory tract infection in hospital outpatients aged 0–14 years in Hefei, China: A time series study. Public Health 2018, 156, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, S.; Adair-Rohani, H.; Wolf, J.; Bruce, N.G.; Mehta, S.; Prüss-Ustün, A.; Lahiff, M.; Rehfuess, E.A.; Mishra, V.; Smith, K.R. Solid fuel use for household cooking: Country and regional estimates for 1980–2010. Environ. Health Perspect. 2013, 121, 784–790. [Google Scholar] [CrossRef]
- Zhou, Z.; Dionisio, K.L.; Arku, R.E.; Quaye, A.; Hughes, A.F.; Vallarino, J.; Spengler, J.D.; Hill, A.; Agyei-Mensah, S.; Ezzati, M. Household and community poverty, biomass use, and air pollution in Accra, Ghana. Proc. Natl. Acad. Sci. USA 2011, 108, 11028–11033. [Google Scholar] [CrossRef] [Green Version]
- Mishra, V.; Smith, K.R.; Retherford, R.D. Effects of cooking smoke and environmental tobacco smoke on acute respiratory infections in young Indian children. Popul. Environ. 2005, 26, 375–396. [Google Scholar] [CrossRef]
- Gordon, S.; Bruce, N.; Grigg, J.; Hibberd, P.; Kurmi, O.; Lam, K.; Mortimer, K.; Asante, K.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef] [Green Version]
- Gebertsadik, A.; Worku, A.; Berhane, Y. Factors associated with acute respiratory infection in children under the age of 5 years: Evidence from the 2011 Ethiopia Demographic and Health Survey. Pediatr. Heal. Med. Ther. 2015, 6, 9–13. [Google Scholar]
- Sonego, M.; Pellegrin, M.C.; Becker, G.; Lazzerini, M. Risk factors for mortality from acute lower respiratory infections (ALRI) in children under five years of age in low and middle-income countries: A systematic review and meta-analysis of observational studies. PLoS ONE 2015, 10, e0116380. [Google Scholar] [CrossRef]
- Rojas, F. Poverty determinants of acute respiratory infections among Mapuche indigenous peoples in Chile’s Ninth Region of Araucania, using GIS and spatial statistics to identify health disparities. Int. J. Health Geogr. 2007, 6, 26. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Acute Respiratory Infection (ARI) | |||
|---|---|---|---|
| Characteristics | Sample Distribution (%) * | ARI (%) * | Chi-Square Test p-Value |
| Overall | 27,565 (100) | 17.6 | - |
| Sex of the children | |||
| Boy | 14,275 (51.7) | 18.2 | 0.12 |
| Girl | 13,290 (48.3) | 17.1 | |
| Size of child at birth | |||
| Smaller than average | 3936 (14. 4) | 18.2 | <0.001 |
| Average | 16,878 (61.8) | 16.5 | |
| More than average | 5731 (23.8) | 21.6 | |
| Ever Breastfed | |||
| No | 10,220 (37.0) | 18.3 | <0.001 |
| Yes | 17,221 (63.0) | 17.3 | |
| Children’s age (in years) | |||
| 0 | 5263 (19.2) | 17.3 | <0.001 |
| 1 | 5102 (18.4) | 19.0 | |
| 2 | 5951 (21.8) | 20.3 | |
| 3 | 5761 (21.0) | 16.4 | |
| 4 | 5488 (19.6) | 15.1 | |
| Mother’s age at birth (in years) | |||
| 15–24 years | 12,077 (44.5) | 16.5 | 0.007 |
| 25–35 years | 12,379 (44.3) | 19.0 | |
| 36–49 years | 3109 (11.2) | 16.8 | |
| Mother’s education | |||
| No education | 23,651 (83.5) | 18.1 | 0.08 |
| Primary | 1889 (8.1) | 17.2 | |
| Secondary | 1640 (7.0) | 13.6 | |
| Higher | 385 (1.4) | 12.7 | |
| Mother’s Occupation | |||
| Not working | 24,085 (87.8) | 17.2 | 0.08 |
| Professional | 1224 (6.7) | 24.5 | |
| Agriculture/self-employed | 1370 (1.8) | 16.9 | |
| Skilled manual | 440 (2.7) | 16.9 | |
| Unskilled manual | 429 (0.9) | 14.1 | |
| Mother’s smoking status | |||
| Non-smoker | 26,470 (95.9) | 17.5 | 0.03 |
| Smoker | 1095 (4.1) | 22.0 | |
| Father’s education | |||
| No education | 15,681 (57.6) | 17.7 | 0.54 |
| Primary | 3804 (14.9) | 18.0 | |
| Secondary | 6187 (21.3) | 18.0 | |
| Higher | 1893 (6.2) | 15.2 | |
| Father’s Occupation | |||
| Professional | 5762 (17.6) | 16.2 | 0.007 |
| Clerical/Services | 5068 (18.1) | 15.6 | |
| Agriculture/self-employed | 7909 (29.6) | 20.6 | |
| Skilled manual | 4112 (17.1) | 16.0 | |
| Unskilled manual | 4714 (17.7) | 17.9 | |
| Wealth quintile | |||
| Poorest | 5802 (21.4) | 22.9 | <0.001 |
| Poorer | 5860 (20.2) | 18.2 | |
| Middle | 5825 (19.0) | 16.6 | |
| Richer | 5850 (20.6) | 13.4 | |
| Richest | 4228 (18.8) | 16.6 | |
| Urbanity | |||
| Urban | 6590 (22.7) | 17.6 | 0.95 |
| Rural | 20,975 (77.3) | 17.7 | |
| Region | |||
| North Eastern | 2682 (12.5) | 19.4 | <0.001 |
| Northern | 3417 (17.6) | 15.1 | |
| Western | 3818 (15.7) | 29.7 | |
| Central Highland | 1187 (2.1) | 10.2 | |
| Capitals | 4016 (17.6) | 11.5 | |
| Eastern | 4346 (8.7) | 20.1 | |
| Southern | 4428 (17.3) | 18.5 | |
| South Eastern | 3671 (8.5) | 8.6 | |
| Season | |||
| Summer | 4786 (20.1) | 13.8 | <0.001 |
| Autumn | 14,890 (49.8) | 16.1 | |
| Winter | 7889 (30.1) | 22.8 | |
| Location of Cooking | |||
| Indoor Kitchen | 17,645 (59.0) | 19.1 | <0.001 |
| Outdoor Kitchen | 9920 (41.0) | 15.5 | |
| Solid Fuel Use (SFU) | |||
| Unexposed | 6799 (29.8) | 15.2 | 0.02 |
| Exposed | 20,766 (70.2) | 18.7 | |
| Exposure to IAP | |||
| Unexposed | 6799 (29.8) | 15.2 | <0.001 |
| Moderately exposed | 7622 (30.0) | 15.8 | |
| Highly exposed | 13,144 (40.2) | 20.8 | |
| Characteristics | Solid Fuel Use (SFU) | Exposure to IAP | ||||
|---|---|---|---|---|---|---|
| Prevalence of SFU * | p-Value | Unexposed * | Moderately Exposed * | Highly Exposed * | p-Value | |
| Overall | 70.2 | - | 29.8 | 30.0 | 40.2 | - |
| Sex of the children | ||||||
| Boy | 69.7 | 0.31 | 30.3 | 30.0 | 39.7 | 0.46 |
| Girl | 70.8 | 29.3 | 30.0 | 40.7 | ||
| Size of child at birth | ||||||
| Smaller than average | 67.2 | 0.01 | 32.8 | 31.1 | 36.0 | 0.005 |
| Average | 71.5 | 28.5 | 30.7 | 40.8 | ||
| More than average | 66.9 | 33.1 | 26.6 | 40.3 | ||
| Ever breastfed | ||||||
| No | 68.7 | 0.007 | 31.4 | 29.4 | 39.2 | 0.01 |
| Yes | 71.1 | 28.9 | 30.4 | 40.8 | ||
| Children’s age (in years) | ||||||
| 0 | 68.6 | 0.09 | 31.4 | 28.8 | 39.9 | 0.10 |
| 1 | 68.8 | 31.3 | 31.2 | 37.6 | ||
| 2 | 70.4 | 29.6 | 29.9 | 40.5 | ||
| 3 | 70.2 | 29.8 | 29.6 | 40.6 | ||
| 4 | 72.9 | 27.1 | 30.8 | 42.1 | ||
| Mother’s age at birth (in years) | ||||||
| 15–24 years | 69.5 | 0.03 | 30.5 | 29.1 | 40.4 | 0.03 |
| 25–35 years | 69.7 | 30.4 | 29.8 | 39.8 | ||
| 36–49 years | 75.2 | 24.8 | 34.5 | 40.7 | ||
| Mother’s education | ||||||
| No education | 75.5 | <0.0001 | 24.5 | 31.5 | 44.0 | <0.001 |
| Primary | 49.1 | 50.9 | 22.9 | 26.2 | ||
| Secondary | 40.2 | 59.8 | 23.3 | 16.9 | ||
| Higher | 25.2 | 74.9 | 15.6 | 9.6 | ||
| Mother’s occupation | ||||||
| Not working | 70.3 | <0.0001 | 29.7 | 30.1 | 40.2 | <0.001 |
| Professional | 57.7 | 42.3 | 19.3 | 38.4 | ||
| Agriculture/self-employed | 99.8 | 0.2 | 42.2 | 57.5 | ||
| Skilled manual | 76.5 | 23.5 | 47.7 | 28.8 | ||
| Unskilled manual | 76.0 | 24.0 | 24.7 | 51.3 | ||
| Mother’s smoking status | ||||||
| Non-smoker | 69.7 | 0.002 | 30.3 | 29.8 | 39.8 | 0.002 |
| Smoker | 82.9 | 17.1 | 35.1 | 47.9 | ||
| Father’s education | ||||||
| No education | 78.2 | <0.0001 | 21.8 | 34.4 | 43.8 | <0.001 |
| Primary | 63.6 | 36.5 | 27.1 | 36.4 | ||
| Secondary | 60.4 | 39.6 | 24.1 | 36.3 | ||
| Higher | 46.1 | 54.0 | 17.1 | 28.9 | ||
| Father’s occupation | ||||||
| Professional | 69.9 | <0.0001 | 30.1 | 31.0 | 38.9 | <0.001 |
| Clerical/Services | 50.6 | 49.4 | 19.8 | 30.9 | ||
| Agriculture/self-employed | 91.2 | 8.8 | 36.0 | 55.2 | ||
| Skilled manual | 52.4 | 47.6 | 26.0 | 26.4 | ||
| Unskilled manual | 72.6 | 27.4 | 33.5 | 39.2 | ||
| Wealth quintile | ||||||
| Poorest | 94.7 | <0.0001 | 5.3 | 51.0 | 43.7 | <0.001 |
| Poorer | 88.0 | 12.0 | 37.7 | 50.4 | ||
| Middle | 76.9 | 23.1 | 25.3 | 51.6 | ||
| Richer | 58.1 | 41.9 | 19.6 | 38.5 | ||
| Richest | 29.6 | 70.4 | 14.2 | 15.5 | ||
| Urbanity | ||||||
| Urban | 19.3 | <0.0001 | 80.7 | 9.0 | 10.3 | <0.001 |
| Rural | 85.1 | 14.9 | 36.2 | 48.9 | ||
| Region | ||||||
| North Eastern | 85.7 | <0.0001 | 14.3 | 62.8 | 22.9 | <0.001 |
| Northern | 67.7 | 32.3 | 38.6 | 29.1 | ||
| Western | 80.3 | 19.7 | 40.3 | 40.0 | ||
| Central Highland | 92.6 | 7.4 | 29.1 | 63.5 | ||
| Capitals | 37.7 | 62.3 | 18.9 | 18.9 | ||
| Eastern | 85.1 | 14.9 | 6.4 | 78.6 | ||
| Southern | 69.2 | 30.8 | 10.6 | 58.7 | ||
| South Eastern | 82.2 | 17.8 | 32.2 | 50.1 | ||
| Season | ||||||
| Summer | 22.8 | <0.0001 | 77.2 | 10.3 | 12.5 | <0.001 |
| Autumn | 76.4 | 23.6 | 35.2 | 41.2 | ||
| Winter | 91.7 | 8.3 | 34.7 | 57.0 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, J.; Uddin, J.; Peltier, R.; Oulhote, Y. Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter? Int. J. Environ. Res. Public Health 2019, 16, 2910. https://doi.org/10.3390/ijerph16162910
Rana J, Uddin J, Peltier R, Oulhote Y. Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter? International Journal of Environmental Research and Public Health. 2019; 16(16):2910. https://doi.org/10.3390/ijerph16162910
Chicago/Turabian StyleRana, Juwel, Jalal Uddin, Richard Peltier, and Youssef Oulhote. 2019. "Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter?" International Journal of Environmental Research and Public Health 16, no. 16: 2910. https://doi.org/10.3390/ijerph16162910