Seasonality of Rotavirus Hospitalizations at Costa Rica’s National Children’s Hospital in 2010–2015

 ,
,
Abstract
:1. Introduction
2. Data and Methods
2.1. Study Area
2.2. Health Outcomes
2.3. Meteorological Data
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tate, J.E.; Burton, A.H.; Boshi-Pinto, C.; Parashar, U.D. Global, regional, and national estimates of rotavirus mortality in children <5 years of age, 2000–2013. Clin. Infect. Dis. 2016, 62, S96–S105. [Google Scholar] [PubMed]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Steele, A.D.; Duque, J.; Parashar, U.D. 2008 Estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programs: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 136–141. [Google Scholar] [CrossRef]
- Perez Schael, I.; O’Ryan, M.; Sáez-Llorens, X.; Linhares, A.; Velázquez, F.R.; Colindres, R.; Breuer, T.B.; Eduardo Ortega-Barria, E. Clinical development, registration, and introduction of human rotavirus vaccine: The Latin American experience. Tr. Vaccinol. 2012, 1, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Linhares, A.; Macias-Parra, M.; Sáez-Llorens, X.; Vergara, R.; Jimenez, E.; Velázquez, F.R.; Cervantes, Y.; Abate, H.J.; Rivera, L.; Ruttimann, R.; et al. Rotavirus gastroenteritis in Latin America: A hospital-based study in children undrer 3 years of age. Tr. Vaccinol. 2012, 1, 36–41. [Google Scholar] [CrossRef]
- Cook, S.M.; Glass, R.I.; LeBaron, C.W.; Ho, M.S. Global seasonality of rotavirus infections. WHO Bull. 1990, 68, 171–177. [Google Scholar]
- Patel, M.; Pitzer, V.E.; Alonso, W.; Vera, D.; Lopman, B.; Tate, J.; Parashar, U.D. Global seasonality of rotavirus disease. Pediatr. Infect. Dis. J. 2013, 32, el34–el47. [Google Scholar] [CrossRef] [PubMed]
- Jagai, J.S.; Sarkar, R.; Castronovo, D.; Kattula, D.; McEntee, J.; Ward, H.; Kang, G.; Naumova, E.N. Seasonality of Rotavirus in South Asia: A Meta-analysis approach assessing associations with temperature, precipitation, and vegetation index. PLoS ONE 2012, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.; Mamani, N.; Halvorsen, K.; Iñiguez, V. Enfermedades diarreicas agudas asociadas a rotavirus. Rev. Soc. Bol. Ped. 2005, 44, 75–82. [Google Scholar]
- Levy, K.; Hubbard, A.E.; Eisenberg, J.N. Seasonality of rotavirus disease in the tropics: A systematic review and meta-analysis. Int. J. Epidemiol. 2009, 38, 1487–1496. [Google Scholar] [CrossRef]
- D’Souza, R.M.; Hall, G.; Becker, N.G. Climatic factors associated with hospitalizations for rotavirus diarrhoea in children under 5 years of age. Epidemiol. Infect. 2008, 136, 56–64. [Google Scholar]
- Nitiema, L.W.; Nordgren, J.; Ouermi, D.; Dianou, D.; Traore, A.; Svensson, L.; Simpore, J. Burden of rotavirus and other enteropathogens among children with diarrhea in Burkina Faso. Int. J. Infect. Dis. 2011, 15, e646–e652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guardado, J.A.; Clará, W.; Turcios, R.M.; Fuentes, R.A.; Valencia, D.; Sandoval, R.; de Figueroa, J.B.; Bresee, J.S.; Glass, R.I. Rotavirus in El Salvador: An outbreak, surveillance and estimates of disease burden, 2000-2002. Pediatr. Infect. Dis. J. 2004, 23, S156–S160. [Google Scholar] [CrossRef] [PubMed]
- Cunliffe, N.A.; Kilgore, P.E.; Bresse, J.S.; Steele, A.D.; Luo, N.; Hart, C.A.; Glass, R.I. Epidemiology of rotavirus diarrhoea in Africa: A review to assess the need for rotavirus immunization. Bull. World Health Organ. 1998, 76, 525–537. [Google Scholar] [PubMed]
- Kiulia, N.M.; Netshikweta, R.; Page, N.A.; Zyl, W.B.; Kiraithe, N.M.; Nyachieo, A. The detection of enteric viruses in selected urban and rural river water and sewage in Kenya, with special reference to rotaviruses. J. Appl. Microbiol. 2010, 109, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Barril, P.A.; Fumian, T.M.; Prez, V.E.; Gil, P.I.; Martinez, L.C.; Giordano, M.O.; Masachessi, G.; Isa, M.B.; Ferreyra, L.J.; Ré, V.E.; et al. Rotavirus seasonality in urban sewage from Argentina: Effect of meteorological variables on the viral load and the genetic diversity. Environ. Res. 2015, 138, 409–415. [Google Scholar] [CrossRef]
- Kraay, A.N.M.; Brouwer, A.F.; Lin, N.; Collender, P.A.; Remais, J.V.; Eisenberg, J.N.S. Modeling environmentally mediated rotavirus transmission: The role of temperature and hydrologic factors. Proc. Natl. Acad. Sci. USA 2018, 115, E2782–E2790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, V.S.; Berezin, E.N.; Gurgel, R.Q. Rotavirus in Latin America: Current situation and perspectives. J. Pediatric Infect. Dis. Soc. 2017, 6, 1–2. [Google Scholar] [CrossRef]
- Ulloa-Gutierrez, R.; Avila-Aguero, M.L. Rotavirus vaccination in Central American children. Expert Rev Vaccines. 2014, 13, 687–690. [Google Scholar] [CrossRef] [Green Version]
- Vaccine Resource Library. Rotavirus Vaccine Country Introductions: Maps and List. Available online: https://vaccineresources.org/details.php?i=2235 (accessd on 19 May 2019).
- Kang, G. Rotavirus vaccines. Indian J. Med. Microbiol. 2006, 24, 252–257. [Google Scholar] [CrossRef]
- Geodatos.net. Coordenadas Geográficas de Costa Rica—Latitud y Longitud. Available online: https://www.geodatos.net/coordenadas/costa (accessd on 19 May 2019).
- Instituto Meteorológico Nacional (IMN). Cambio Climático: Segunda Comunicación Nacional. Clima Variabilidad y Cambio Climático en Costa Rica. Available online: http://users.clas.ufl.edu/prwaylen/geo3280articles/el_clima_variabilidad_y_cambio_climatico_en_cr_version_final.pdf (accessd on 19 May 2019).
- Instituto Meteorológico Nacional (Costa Rica) Boletín meteorológico—IMN 2018. Available online: https://www.imn.ac.cr/boletin-meteorologico (accessd on 19 May 2019).
- Aumova, E.N.; MacNeill, I.B. Seasonality Assessment for Biosurveillance. In Advances in Statistical Methods for the Health Sciences; Auget, J.L., Balakrishnan, N., Mesbah, M., Molenberghs, G., Eds.; Birkhauser: Basel, Switzerland, 2007; pp. 437–450. [Google Scholar]
- Alarcon Falconi, T.M.; Cruz, M.; Naumova, E.N. The shift in seasonality of legionellosis in the U.S. Epidemiol Infect. 2018, 146, 1824–1833. [Google Scholar] [CrossRef]
- Hieber, J.P.; Shelton, S.; Nelson, J.D.; Leon, J.; Mohs, E. Comparison of human rotavirus disease in tropical and temperate settings. Am. J. Dis. Child. 1978, 132, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Schael, I.; González, R.; Fernández, R.; Alfonzo, E.; Inaty, D.; Boher, Y.; Sarmiento, L. Epidemiological features of rotavirus infection in Caracas, Venezuela: Implications for rotavirus immunization programs. J. Med. Virol. 1999, 59, 520–526. [Google Scholar] [CrossRef]
- Omore, R.; Tate, H.; O’Reilly, C.; Ayers, T.; Williamson, J.; Moke, F.; Schilling, K.A.; Awuor, A.O.; Jaron, P.; Ochieng, J.B.; et al. Epidemiology, seasonality and factors associated with rotavirus infection among children with moderate-to-severe diarrhea in rural western Kenya, 2008-2012: The Global Enteric Multicenter Study (GEMS). PLoS ONE 2016, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.; Mouw, C.; Jutla, A.; Akanda, A. Quantification of rotavirus diarrheal risk due to hydroclimatic extremes over South Asia: Prospects of satellite-based observations in detecting outbreaks. GeoHealth 2018, 2, 70–86. [Google Scholar] [CrossRef]
- Fisman, D. Seasonality of viral infections: Mechanisms and unknowns. Clin. Microbiol. Infect. 2012, 18, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.; Vesikari, T.; Van Damme, P.; Giaquinto, C.; Mrukowicz, J.; Guarino, A.; Dagan, R.; Szajewska, H.; Usonis, V. Rotavirus. J. Pediatr. Gastroenterol. Nutr. 2008, 46, S24–S31. [Google Scholar] [CrossRef]
- Van Asten, L.; Bijkerk, P.; Fanoy, E.; Van Ginkel, A.; Suijkerbuijk, A.; Van der Hoek, W.; Meijer, A.; Vennema, H. Early occurrence of influenza A epidemics coincided with changes in occurrence of other respiratory virus infections. Influenza Respir. Viruses. 2016, 10, 14–26. [Google Scholar] [CrossRef]
- Bourdett-Stanziola, L.; Jiménez, C.; Ortega-Barria, E. Diversity of human rotavirus G and P genotypes in Panama, Costa Rica, and the Dominican Republic. Am. J. Trop. Med. Hyg. 2008, 79, 921–924. [Google Scholar] [CrossRef]
- Bourdett-Stanziola, L.; Ortega-Barria, E.; Espinoza, F.; Bucardo, F.; Jimenez, C.; Ferrera, A. Rotavirus genotypes in Costa Rica, Nicaragua, Honduras and the Dominican Republic. Intervirology 2011, 54, 49–52. [Google Scholar] [CrossRef]
- Tate, J.E.; Panozzo, C.A.; Payne, D.C.; Patel, M.M.; Cortese, M.M.; Fowlkes, A.L.; Parashar, U.D. Decline and change in seasonality of US rotavirus activity after the introduction of rotavirus vaccine. Pediatrics 2009, 124, 465–471. [Google Scholar] [CrossRef]
- Esparza-Aguilar, M.; Gastañaduy, P.; Sánchez-Uribe, E.; Desai, R.; Parashar, U.D.; Richardson, V.; Patel, M. Diarrhoea-related hospitalizations in children before and after implementation of monovalent rotavirus vaccination in Mexico. Bull. World Health Organ. 2014, 92, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Masukawa, M.L.; Souza, E.M.; Gimenes, E.; Uchimura, N.S.; Moriwaki, A.M.; Uchimura, T.T. Time series investigation of changes in seasonality of acute diarrhea hospitalizations before and after rotavirus vaccine in Southern Brazil. Cad. Saude Pública 2016, 32, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.M.; Alonso, W.J. Rotavirus vaccination takes seasonal signature of childhood diarrhea back to pre-sanitation era in Brazil. J. Infect. 2018, 76, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.; Ramani, S.; Tate, J.; Parashar, U.; Svensson, L.; Hagbom, M.; Franco, M.; Greenberg, H.; O’Ryan, M.; Kang, G.; et al. Rotavirus infection. Nat. Rev. Dis. Primers 2017, 3, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Pitzer, V.E.; Viboud, C.; Lopman, B.A.; Patel, M.M.; Parashar, U.D.; Grenfell, B.T. Influence of birth rates and transmission rates on the global seasonality of rotavirus incidence. J. R. Soc. Interface 2011, 8, 1584–1593. [Google Scholar] [CrossRef]
- Sarkar, R.; Kang, G.; Naumova, E.N. Rotavirus seasonality and age effects in a Birth Cohort Study of Southern India. PLoS ONE 2013, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Prasetyo, D.; Ermaya, Y.; Maritza, I.; Yati, S. Correlation between climate variations and rotavirus diarrhea in under-five children in Bandung. Asian Pac. J. Trop. Dis. 2015, 5, 908–911. [Google Scholar] [CrossRef]
- Solano, J.; Villalobos, R. Aspectos fisiográficos aplicados a un bosquejo de regionalización geográfico-climático de Costa Rica. Top. Meteoro. Oceanog. 2001, 8, 26–39. [Google Scholar]
- Fernández, W.; Ramírez, P. El Niño, la Oscilación del Sur y sus efectos en Costa Rica. Una revisión. Tecnol. Marcha. 1991, 11, 3–10. [Google Scholar]
- Instituto Meteorológico Nacional (Costa Rica). Boletín ENOS—IMN 2018. Available online: https://www.imn.ac.cr/web/imn/43 (accessd on 19 May 2019).
- Checkley, W.; Epstein, L.D.; Gilman, R.H.; Figueroa, D.; Cama, R.I.; Patz, J.A.; Black, R.E. Effects of El Niño and ambient temperature on hospital admissions for diarrhoeal diseases in Peruvian children. Lancet 2000, 355, 442–450. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
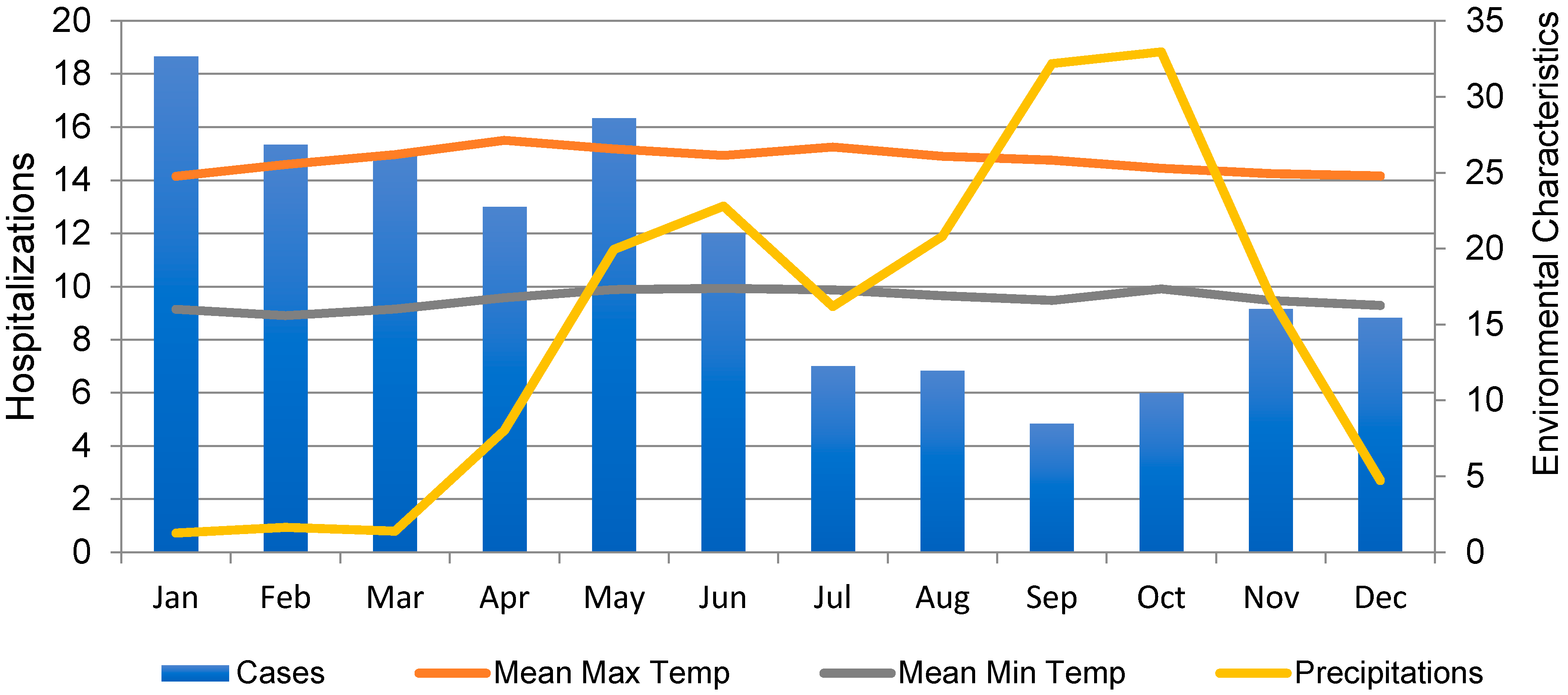
| Month | Rotavirus Counts | Precipitation (mm) | Minimum Temperature (°C) | Maximal Temperature (°C) | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| January | 18.6 | 29.78 | 12.6 | 9.39 | 16.00 | 1.29 | 24.77 | 0.92 |
| February | 15.3 | 16.74 | 16.4 | 9.97 | 15.58 | 0.80 | 25.53 | 0.92 |
| March | 15.0 | 15.27 | 13.9 | 10.28 | 16.01 | 0.97 | 26.18 | 0.89 |
| April | 13.0 | 11.95 | 80.2 | 48.38 | 16.76 | 0.71 | 27.13 | 0.26 |
| May | 16.3 | 20.68 | 199.5 | 55.11 | 17.30 | 0.63 | 26.57 | 0.75 |
| June | 12.0 | 14.10 | 228.0 | 47.25 | 17.37 | 0.77 | 26.13 | 0.56 |
| July | 7.0 | 9.14 | 161.9 | 88.29 | 17.27 | 0.75 | 26.68 | 2.44 |
| August | 6.8 | 5.98 | 208.1 | 99.23 | 16.88 | 0.79 | 26.07 | 0.71 |
| September | 4.8 | 4.95 | 321.9 | 133.86 | 16.58 | 0.51 | 25.82 | 0.91 |
| October | 6.0 | 6.16 | 329.6 | 124.13 | 17.35 | 1.94 | 25.28 | 1.15 |
| November | 9.1 | 11.30 | 167.8 | 77.04 | 16.58 | 0.65 | 24.93 | 1.18 |
| December | 8.8 | 11.96 | 47.2 | 19.16 | 16.25 | 1.11 | 24.78 | 1.41 |
| Overall | 11.1 | 14.31 | 148.9 | 129.7 | 16.66 | 1.08 | 25.82 | 1.29 |
| Study Group | Peak Time (month) | Relative Intensity (counts) | ||||
|---|---|---|---|---|---|---|
| Estimate | LCI | UCI | Estimate | LCI | UCI | |
| 0–23 months | 3.12 | 1.55 | 4.68 | 2.47 | 1.50 | 3.45 |
| 24+ months | 2.89 | 1.65 | 4.13 | 2.68 | 1.51 | 3.85 |
| All children | 2.96 | 1.63 | 4.30 | 2.75 | 1.54 | 3.96 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ureña-Castro, K.; Ávila, S.; Gutierrez, M.; Naumova, E.N.; Ulloa-Gutierrez, R.; Mora-Guevara, A. Seasonality of Rotavirus Hospitalizations at Costa Rica’s National Children’s Hospital in 2010–2015. Int. J. Environ. Res. Public Health 2019, 16, 2321. https://doi.org/10.3390/ijerph16132321
Ureña-Castro K, Ávila S, Gutierrez M, Naumova EN, Ulloa-Gutierrez R, Mora-Guevara A. Seasonality of Rotavirus Hospitalizations at Costa Rica’s National Children’s Hospital in 2010–2015. International Journal of Environmental Research and Public Health. 2019; 16(13):2321. https://doi.org/10.3390/ijerph16132321
Chicago/Turabian StyleUreña-Castro, Katarina, Silvia Ávila, Mariela Gutierrez, Elena N. Naumova, Rolando Ulloa-Gutierrez, and Alfredo Mora-Guevara. 2019. "Seasonality of Rotavirus Hospitalizations at Costa Rica’s National Children’s Hospital in 2010–2015" International Journal of Environmental Research and Public Health 16, no. 13: 2321. https://doi.org/10.3390/ijerph16132321