The Use of a Quasi-Experimental Study on the Mortality Effect of a Heat Wave Warning System in Korea

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
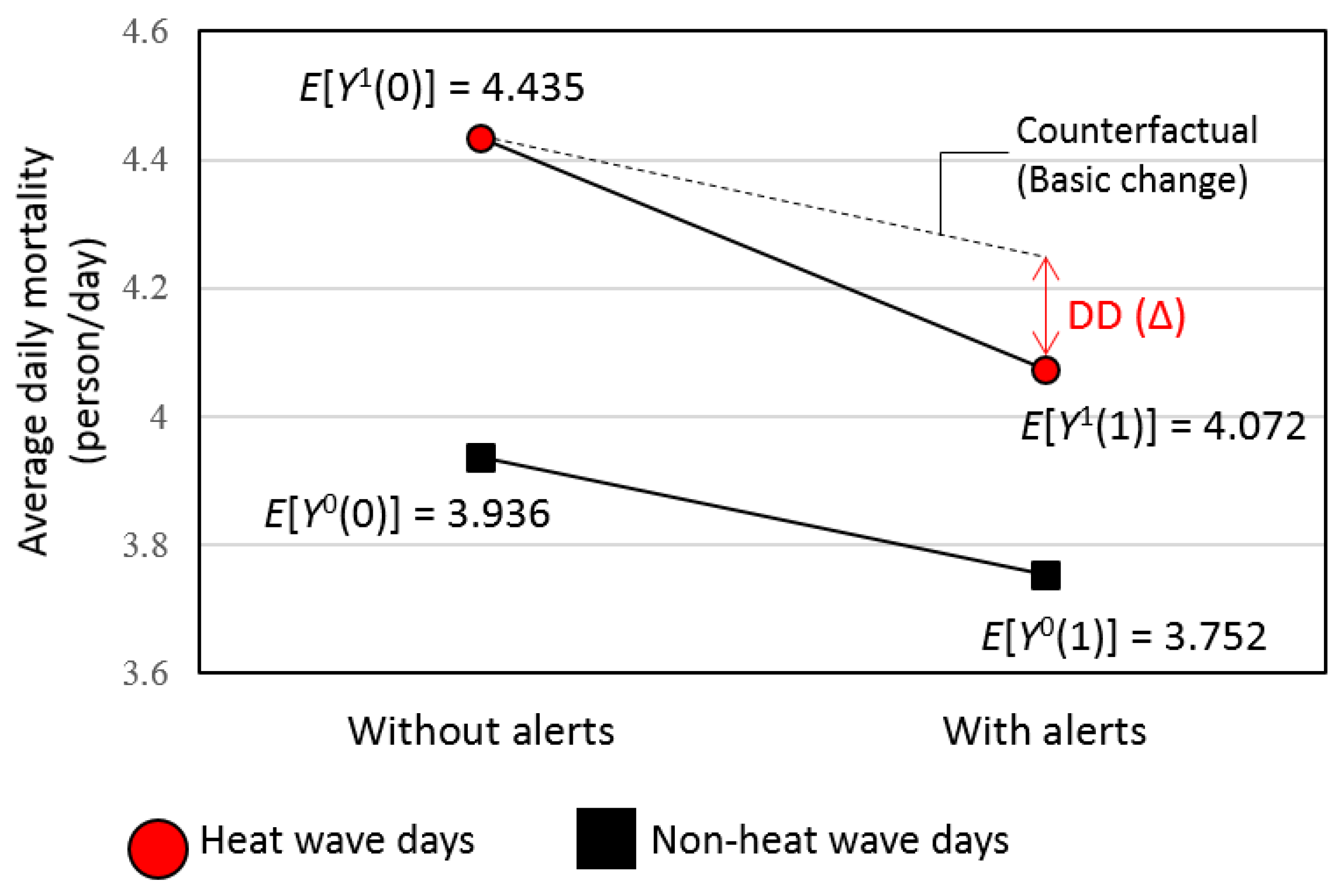
2.2.1. Approach of Difference-In-Differences Model
2.2.2. Propensity Score Weighting
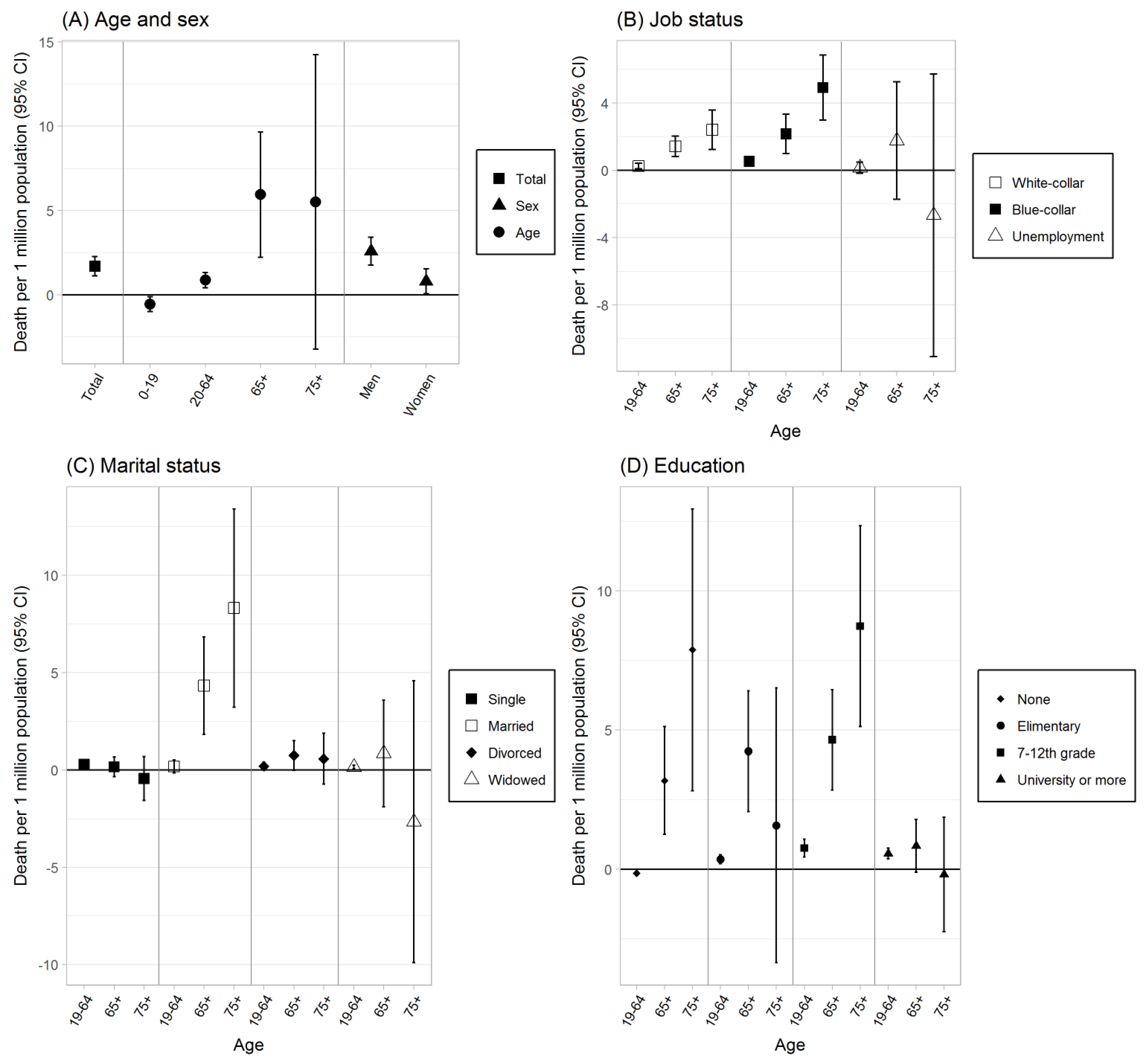
2.2.3. Subgroup Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- 2018 Was 4th Hottest Year on Record for the Globe. Available online: https://www.noaa.gov/news/2018-was-4th-hottest-year-on-record-for-globe (accessed on 4 July 2019).
- NASA. Fourth Warmest Year in Continued Warming Trend, According to NASA. Available online: https://www.nasa.gov/press-release/2018-fourth-warmest-year-in-continued-warming-trend-according-to-nasa-noaa (accessed on on 4 July 2019).
- Pachauri, R.K.; Allen, M.R.; Barros, V.R.; Broome, J.; Cramer, W.; Christ, R.; Church, J.A.; Clarke, L.; Dahe, Q.; Dasgupta, P. Climate Change: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014; ISBN 9291691437. [Google Scholar]
- Korea Meteorological Administration. Korea Climate Change Evaluation Report; Korea Meteorological Administration: Seoul, Korea, 2014. [Google Scholar]
- Smith, K.R.; Woodward, A.; Campbell-Lenderum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R.; Aranda, C.; et al. Climate Change: Impacts, Adaptation, and Vulnerability Part A: Global and Sectoral Aspects Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Human Health: Impacts, Adaptation, and Co-Ben; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar]
- Kim, H.; Ha, J.; Park, J. High temperature, heat index, and mortality in 6 major cities in Korea. Arch. Environ. Occup. Health 2006, 61, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-Y.; Bell, M.L.; Lee, J.-T. The impact of heat, cold, and heat waves on hospital admissions in eight cities in Korea. Int. J. Biometeorol. 2014, 58, 1893–1903. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.; Bell, M.L.; Lee, J.-T. Comparison of health risks by heat wave definition: Applicability of wet-bulb globe temperature for heat wave criteria. Environ. Res. 2019, 168, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.; Bell, M.L. Heat waves in Korea: Differences of heat wave characteristics by thermal indices. J. Expo. Sci. Environ. Epidemiol. 2018, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Son, J.Y.; Lee, J.T.; Brooke Anderson, G.; Bell, M.L. The impact of heat waves on mortality in seven major cities in Korea. Environ. Health Perspect. 2012, 120, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-M.; Kim, S.; Cheong, H.-K.; Kim, E.-H. Comparison of temperature indexes for the impact assessment of heat stress on heat-related mortality. Environ. Health Toxicol. 2011, 26, e2011009. [Google Scholar] [CrossRef] [PubMed]
- Buscail, C.; Upegui, E.; Viel, J.F. Mapping heatwave health risk at the community level for public health action. Int. J. Health Geogr 2012, 11, 38. [Google Scholar] [CrossRef]
- Basu, R.; Samet, J.M. An exposure assessment study of ambient heat exposure in an elderly population in Baltimore, Maryland. Environ. Health Perspect. 2002, 110, 1219–1224. [Google Scholar] [CrossRef]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Vulnerability to Heat-related Mortality A Systematic Review, Meta-analysis, and Meta-regression Analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef]
- Arbuthnott, K.G.; Hajat, S. The health effects of hotter summers and heat waves in the population of the United Kingdom: A review of the evidence. Environ. Health Glob. Access Sci. Source 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Picture of America Report: Heat-Related Illness; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016. [Google Scholar]
- Korea Center for Disease Control and Prevention. Introduction of Health Management Program for Response to Heat Waves. Available online: http://www.cdc.go.kr/CDC/cms/content/mobile/26/125926_view.html (accessed on 13 May 2019). (In Korean).
- Matzarakis, A. The Heat Health Warning System of DWD—Concept and Lessons Learned. In Perspectives on Atmospheric Sciences; Springer: Cham, Switzerland, 2017; pp. 191–196. [Google Scholar]
- Korea Meteorological Administration. Criteria for Advisory/Warning Information. Available online: https://web.kma.go.kr/eng/weather/forecast/notice.jsp (accessed on 22 April 2019).
- Toloo, G.; FitzGerald, G.; Aitken, P.; Verrall, K.; Tong, S. Evaluating the effectiveness of heat warning systems: Systematic review of epidemiological evidence. Int. J. Public Health 2013, 58, 667–681. [Google Scholar] [CrossRef] [PubMed]
- Wing, C.; Simon, K.; Bello-gomez, R.A. Designing Difference in Difference Studies: Best Practices for Public Health Policy Research. Annu. Rev. Public Health 2018, 39, 453–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angrist, J.D.; Pischke, J.-S. Mostly Harmless Econometrics: An Empiricist’s Companion; Princeton University Press: Princeton, NJ, USA, 2008; ISBN 1400829828. [Google Scholar]
- Stuart, E.A.; Huskamp, H.A.; Duckworth, K. Using propensity scores in difference-in-differences models to estimate the effects of a policy change. Health Serv. Outcomes Res. Methodol. 2014, 14, 166–182. [Google Scholar] [CrossRef] [PubMed]
- Deb, S.; Austin, P.C.; Tu, J. V.; Ko, D.T.; Mazer, C.D.; Kiss, A.; Fremes, S.E. A Review of Propensity-Score Methods and Their Use in Cardiovascular Research. Can. J. Cardiol. 2016, 32, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Gertler, P.J.; Martinez, S.; Premand, P.; Rawlings, L.B.; Vermeersch, C.M.J. Impact Evaluation in Practice, 2nd, ed.; The World Bank: Washington, DC, USA, 2016; ISBN 1464807795. [Google Scholar]
- Pirracchio, R.; Resche-Rigon, M.; Chevret, S. Evaluation of the propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Med. Res. Methodol. 2012, 12, 70. [Google Scholar] [CrossRef] [PubMed]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.J.; Glynn, R.J. Variable Selection for Propensity Score Models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Barnett, A.G.; Pan, X.; Yu, W.; Tong, S. The impact of temperature on mortality in Tianjin, china: A case-crossover design with a distributed lag nonlinear model. Environ. Health Perspect. 2011, 119, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Bobb, J.F.; Peng, R.D.; Bell, M.L.; Dominici, F. Heat-related mortality and adaptation to heat in the United States. Environ. Health Perspect. 2014, 122, 811–816. [Google Scholar] [CrossRef]
- Hahn, J.; Robins, J.; Rubin, D.; Wooldridge, J.; Hopkins, J. Efficient Estimation of Average Treatment Effects Using the Estimated Propensity Score. Econometrica 2003, 71, 1161–1189. [Google Scholar] [Green Version]
- Rubin, D.B. Using propensity scores to help design observational studies: Application to the tobacco litigation. Health Serv. Outcomes Res. Methodol. 2001, 2, 169–188. [Google Scholar] [CrossRef]
- Cole, S.R.; Hernán, M.A. Constructing inverse probability weights for marginal structural models. Am. J. Epidemiol. 2008, 168, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Interaction revisited: The difference between two estimates. BMJ 2003, 326, 219. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.; Ebi, K.L.; Forsberg, B. Heatwave early warning systems and adaptation advice to reduce human health consequences of heatwaves. Int. J. Environ. Res. Public Health 2011, 8, 4623–4648. [Google Scholar] [CrossRef] [PubMed]
- Fouillet, A.; Rey, G.; Wagner, V.; Laaidi, K.; Empereur-Bissonnet, P.; Le Tertre, A.; Frayssinet, P.; Bessemoulin, P.; Laurent, F.; De Crouy-Chanel, P.; et al. Has the impact of heat waves on mortality changed in France since the European heat wave of summer 2003? A study of the 2006 heat wave. Int. J. Epidemiol. 2008, 37, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Kyselý, J.; Kříž, B. Decreased impacts of the 2003 heat waves on mortality in the Czech Republic: An improved response? Int. J. Biometeorol. 2008, 52, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Profili, F.; Crisci, A.; Francesconi, P.; Gensini, G.F.; Orlandini, S. Heat-related mortality in the Florentine area (Italy) before and after the exceptional 2003 heat wave in Europe: An improved public health response? Int. J. Biometeorol. 2012, 56, 801–810. [Google Scholar] [CrossRef]
- De’donato, F.; Scortichini, M.; De Sario, M.; De Martino, A.; Michelozzi, P. Temporal variation in the effect of heat and the role of the Italian heat prevention plan. Public Health 2018, 161, 154–162. [Google Scholar] [CrossRef]
- Benmarhnia, T.; Bailey, Z.; Kaiser, D.; Auger, N.; King, N.; Kaufman, J.S.; Benmarhnia, T.; Bailey, Z.; Kaiser, D.; Auger, N.; et al. A Difference-in-Differences Approach to Assess the Effect of a Heat Action Plan on Heat-Related Mortality, and Differences in Effectiveness According to Sex, Age, and Socioeconomic Status (Montreal, Quebec). Environ. Health Perspect. 2016, 124, 1694–1699. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, K.R.; Zanobetti, A.; Schwartz, J.; Wellenius, G.A. Effectiveness of National Weather Service heat alerts in preventing mortality in 20 US cities. Environ. Int. 2018, 116, 30–38. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Causes of Death Statistics. Available online: http://kosis.kr/index/index.do (accessed on 12 June 2019).
- Van Steen, Y.; Ntarladima, A.-M.; Grobbee, R.; Karssenberg, D.; Vaartjes, I. Sex differences in mortality after heat waves: Are elderly women at higher risk? Int. Arch. Occup. Environ. Health 2019, 92, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.; Carmona, R.; Mirón, I.J.; Ortiz, C.; Linares, C. Comparison of the effects of extreme temperatures on daily mortality in Madrid (Spain), by age group: The need for a cold wave prevention plan. Environ. Res. 2015, 143, 186–191. [Google Scholar] [CrossRef]
- Xu, W.; Thach, T.-Q.; Chau, Y.-K.; Lai, H.-K.; Lam, T.-H.; Chan, W.-M.; Lee, R.S.Y.; Hedley, A.J.; Wong, C.-M. Thermal stress associated mortality risk and effect modification by sex and obesity in an elderly cohort of Chinese in Hong Kong. Environ. Pollut. 2013, 178, 288–293. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, World Meteorological Organization. Heatwaves and Health: Guidance on Warning-System Development; World Meteorological Organization: Geneva, Switzerland, 2015; ISBN 9789263111425. [Google Scholar]
- Heo, S.; Lee, E.; Kwon, B.Y.; Lee, S.; Jo, K.H.; Kim, J. Long-term changes in the heat–mortality relationship according to heterogeneous regional climate: A time-series study in Korea. BMJ Open 2016, 6, e011786. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Krackowizer, A.; Hansen, A.; Bi, P.; Tucker, G. Heat health messages: A randomized controlled trial of a preventative messages tool in the older population of South Australia. Int. J. Environ. Res. Public Health 2017, 14, 992. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, S.C. A survey of public perception and response to heat warnings across four North American cities: An evaluation of municipal effectiveness. Int. J. Biometeorol. 2007, 52, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Petitti, D.B.; Harlan, S.L.; Chowell-Puente, G.; Ruddell, D. Occupation and environmental heat-associated deaths in Maricopa County, Arizona: A case-control study. PLoS ONE 2013, 8, e62596. [Google Scholar] [CrossRef] [PubMed]
- Arbury, S.; Jacklitsch, B.; Farquah, O.; Hodgson, M.; Lamson, G.; Martin, H.; Profitt, A. Heat illness and death among workers—United States, 2012–2013. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 661. [Google Scholar] [PubMed]
- Xiang, J.; Bi, P.; Pisaniello, D.; Hansen, A. The impact of heatwaves on workers’ health and safety in Adelaide, South Australia. Environ. Res. 2014, 133, 90–95. [Google Scholar] [CrossRef]
- Gubernot, D.M.; Anderson, G.B.; Hunting, K.L. Characterizing occupational heat-related mortality in the United States, 2000–2010: An analysis using the census of fatal occupational injuries database. Am. J. Ind. Med. 2015, 58, 203–211. [Google Scholar] [CrossRef]
- Dutta, P.; Rajiva, A.; Andhare, D.; Azhar, G.S.; Tiwari, A.; Sheffield, P.; Group, C.S. Perceived heat stress and health effects on construction workers. Indian J. Occup. Environ. Med. 2015, 19, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Website of Ministry of Employment and Labor. Available online: http://www.moel.go.kr/skin/doc.html?fn=200907090505140f3c435860b64bb2895c8199ed2ea359.hwp&rs=/viewer/ENEWS/2009//%0A%0A%0A (accessed on 4 May 2019).
- Son, J.Y.; Gouveia, N.; Bravo, M.A.; de Freitas, C.U.; Bell, M.L. The impact of temperature on mortality in a subtropical city: Effects of cold, heat, and heat waves in São Paulo, Brazil. Int. J. Biometeorol. 2016, 60, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, S.; Han, J.; Zhou, L.; Liu, Y.; Yang, L.; Zhang, J.; Zhang, Y. Impact of heat waves on nonaccidental deaths in Jinan, China, and associated risk factors. Int. J. Biometeorol. 2016, 60, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-J.; Kim, H. Effect modification of individual- and regional-scale characteristics on heat wave-related mortality rates between 2009 and 2012 in Seoul, Korea. Sci. Total Environ. 2017, 595, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Gronlund, C.J.; Berrocal, V.J.; White-Newsome, J.L.; Conlon, K.C.; O’Neill, M.S. Vulnerability to extreme heat by socio-demographic characteristics and area green space among the elderly in Michigan, 1990–2007. Environ. Res. 2015, 136, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Isaksen, T.B.; Fenske, R.A.; Hom, E.K.; Ren, Y.; Lyons, H.; Yost, M.G. Increased mortality associated with extreme-heat exposure in King County, Washington, 1980–2010. Int. J. Biometeorol. 2016, 60, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Pike, N. Using false discovery rates for multiple comparisons in ecology and evolution. Methods Ecol. Evol. 2011, 2, 278–282. [Google Scholar] [CrossRef]
- Liotta, G.; Inzerilli, M.C.; Palombi, L.; Madaro, O.; Orlando, S.; Scarcella, P.; Betti, D.; Marazzi, M.C. Social interventions to prevent heat-related mortality in the older adult in Rome, Italy: A quasi-experimental study. Int. J. Environ. Res. Public Health 2018, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Temperature Monitoring Data | Change | ||
|---|---|---|---|
| Heat Wave Days | Non-Heat Wave Days | ||
| HW alert + | E[Y1(1)] | E[Y0(1)] | E[Y1(1) − Y0(1)) |
| HW alert − | E[Y1(0)] | E[Y0(0)] | E[Y1(0) − Y0(0)] |
| Difference | E[Y1(1) − Y1(0)] | E[Y0(1) − Y0(0)] | Δ= E[Y1(1) − Y1(0)] − E[Y0(1)−Y0(0)] |
| Variable | All Days | Eligible Days * (26 °C < Daily Mean Temperature ≤ 30.5 °C) | ||
|---|---|---|---|---|
| Sum | (%) | Sum | (%) | |
| Total | 194,409 | 100 | 50,002 | 100 |
| Sex | ||||
| Men | 109,241 | 0.56 | 28,088 | 56.2 |
| Women | 85,168 | 0.44 | 21,914 | 43.8 |
| Age | ||||
| Age 0–19 | 2711 | 1.4 | 715 | 1.4 |
| Age 20–64 | 60,914 | 31.3 | 15,675 | 31.4 |
| Age 65+ | 130,738 | 67.3 | 33,600 | 67.2 |
| Cause-specific | ||||
| Cardiovascular disease | 38,684 | 19.9 | 9917 | 19.8 |
| Respiratory disease | 16,491 | 8.5 | 4127 | 8.3 |
| Job (People age ≥ 19) | ||||
| White-collar | 13,574 | 7.0 | 3600 | 7.2 |
| Blue-collar | 22,597 | 11.6 | 5676 | 11.4 |
| Unemployment* | 151,520 | 77.9 | 38,970 | 77.9 |
| Education (People age ≥ 19) | ||||
| None | 30,622 | 15.8 | 8453 | 16.9 |
| Elementary | 52,077 | 26.8 | 13,468 | 26.9 |
| 7th–12th grade | 47,046 | 24.2 | 12,456 | 24.9 |
| University or more | 56,562 | 29.1 | 13,366 | 26.7 |
| Heat wave days | ||||
| True heat wave | 2677 | 5.4 | 2202 | 17.5 |
| True non-heat wave | 44,576 | 89.1 | 7997 | 63.4 |
| False positive heat wave | 1956 | 3.9 | 1639 | 13.0 |
| False negative heat wave | 818 | 1.6 | 766 | 6.1 |
| Monitored weather (mean, Q1–Q3) | ||||
| Daily maximum temperature (°C) | 28.33 | 14.00–38.80 | 32.08 | 30.80–33.30 |
| Daily mean temperature (°C) | 23.97 | 22.00–33.20 | 27.62 | 26.70–28.40 |
| Daily minimum temperature (°C) | 20.56 | 18.40–29.40 | 24.12 | 23.10–25.20 |
| Relative humidity (%) | 73.59 | 65.60–82.10 | 71.57 | 65.40–78.60 |
| Wind speed (m/s2) | 2.06 | 1.30–2.50 | 2.18 | 1.40–2.70 |
| Air quality (mean, Q1–Q3) | ||||
| O3 (ppm) | 0.025 | 0.017–0.033 | 0.024 | 0.014–0.031 |
| SO2 (ppm) | 0.005 | 0.003–0.006 | 0.005 | 0.003–0.006 |
| CO (ppm) | 0.423 | 0.311–0.530 | 0.412 | 0.288–0.513 |
| NO2 (ppm) | 0.023 | 0.014–0.030 | 0.021 | 0.013–0.027 |
| PM10 (µg/m3) | 38.02 | 24.50–48.00 | 36.74 | 23.56–46.46 |
| Cardiovascular Mortality | Respiratory Mortality | |||
|---|---|---|---|---|
| Estimate | (95% CI) | Estimate | (95% CI) | |
| Age | ||||
| 0–19 | −0.016 | (−0.072, 0.039) | −0.090 | (−0.128, −0.053) * |
| 20–64 | 0.261 | (0.091, 0.432) | −0.014 | (−0.082, 0.054) |
| 65+ | 0.390 | (−1.561, 2.341) | 0.996 | (−0.173, 2.165) |
| 75+ | 0.266 | (−4.523, 5.055) | 2.838 | (−0.067, 5.743) |
| Sex | ||||
| Men | 0.605 | (0.244, 0.965) | −0.102 | (−0.330, 0.126) |
| Women | −0.065 | (−0.444, 0.315) | 0.326 | (0.149, 0.503) |
| Job status (age) | ||||
| White-collar (19–64) | 0.105 | (0.056, 0.153) | −0.008 | (−0.031, 0.015) |
| White-collar (65+) | 0.099 | (−0.261, 0.460) | 0.379 | (0.165, 0.593) |
| White-collar (75+) | −0.212 | (−1.167, 0.744) | 0.544 | (0.010, 1.079) |
| Blue-collar (19–64) | 0.150 | (0.072, 0.228) | 0.015 | (−0.004, 0.035) |
| Blue-collar (65+) | −0.006 | (−0.591, 0.578) | −0.598 | (−0.961, −0.235) * |
| Blue-collar (75+) | −1.305 | (−2.789, 0.179) | −0.748 | (−1.480, −0.016) * |
| Unemployment (19–64) | 0.108 | (−0.011, 0.226) | 0.040 | (−0.007, 0.086) |
| Unemployment (65+) | −0.739 | (−2.628, 1.149) | 0.924 | (−0.150, 1.997) |
| Unemployment (75+) | −5.797 | (−10.856, −0.739) * | 0.922 | (−1.986, 3.831) |
| Marital status (age) | ||||
| Single (19–64) | 0.030 | (−0.030, 0.090) | 0.028 | (−0.001, 0.058) |
| Single (65+) | −0.044 | (−0.374, 0.287) | −0.349 | (−0.534, −0.163) * |
| Single (75+) | −0.409 | (−1.285, 0.466) | −1.236 | (−1.730, −0.742) * |
| Married (19–64) | 0.185 | (0.075, 0.294) | −0.015 | (−0.057, 0.028) |
| Married (65+) | 0.597 | (−0.658, 1.853) | −0.301 | (−1.090, 0.489) |
| Married (75+) | −1.294 | (−4.523, 1.935) | −1.310 | (−3.206, 0.585) |
| Divorced (19–64) | 0.168 | (0.092, 0.244) | −0.005 | (−0.018, 0.008) |
| Divorced (65+) | 0.057 | (−0.383, 0.497) | 1.292 | (0.494, 2.090) |
| Divorced (75+) | 0.061 | (−1.013, 1.134) | 3.090 | (0.850, 5.330) |
| Widowed (19–64) | −0.025 | (−0.058, 0.008) | 0.020 | (0.000, 0.041) |
| Widowed (65+) | −0.944 | (−2.438, 0.550) | −0.310 | (−0.526, −0.094) * |
| Widowed (75+) | −4.524 | (−8.617, −0.431) * | −1.040 | (−1.609, −0.470) * |
| Education (age) | ||||
| None (19–64) | −0.091 | (−0.140, −0.042) * | −0.032 | (−0.055, −0.009) * |
| None (65+) | −1.092 | (−2.231, 0.047) | 0.944 | (0.341, 1.546) |
| None (75+) | −2.948 | (−6.096, 0.199) | 2.432 | (0.764, 4.100) |
| Elementary (19–64) | 0.090 | (0.036, 0.145) | 0.012 | (−0.012, 0.036) |
| Elementary (65+) | 0.631 | (−0.597, 1.859) | −0.884 | (−1.582, −0.185) * |
| Elementary (75+) | −1.669 | (−4.888, 1.550) | −3.167 | (−5.030, −1.305) * |
| 7–12th grade (19–64) | 0.323 | (0.204, 0.441) | 0.042 | (−0.003, 0.088) |
| 7–12th grade (65+) | 0.860 | (−0.116, 1.837) | 0.647 | (0.080, 1.214) |
| 7–12th grade (75+) | 0.260 | (−2.226, 2.746) | 2.617 | (1.289, 3.944) |
| University or more (19–64) | 0.040 | (−0.014, 0.093) | 0.005 | (−0.003, 0.014) |
| University or more (65+) | −0.612 | (−1.140, −0.084) * | −0.141 | (−0.507, 0.226) |
| University or more (75+) | −1.688 | (−3.050, −0.325) * | −1.566 | (−2.518, −0.615) * |
| Study Period (2009–2014) | Period 1 (2009–2011) | Period 2 (2012–2014) | ||||
|---|---|---|---|---|---|---|
| Estimate | (95% CI) | Estimate | (95% CI) | Estimate | (95% CI) | |
| All-cause mortality | ||||||
| Marital status (age) | ||||||
| Widowed (65+) | 0.844 | (−1.895, 3.583) | −8.919 | (−13.533, −4.306) * | 2.795 | (−1.296, 6.887) |
| Widowed (75+) | −2.671 | (−9.906, 4.563) | −21.640 | (−35.97, −7.310) * | −3.673 | (−15.721, 8.376) |
| Education (age) | ||||||
| None (19–64) | −0.144 | (−0.227, −0.061) * | −0.065 | (−0.188, 0.057) | −0.401 | (−0.544, −0.258) * |
| Elementary (65+) | 4.239 | (2.070, 6.408) | −6.979 | (−10.693, −3.266) * | 3.995 | (0.466, 7.524) |
| Elementary (75+) | 1.577 | (−3.359, 6.512) | −18.660 | (−28.563, −8.757) * | −0.004 | (−9.234, 9.226) |
| Cardiovascular mortality | ||||||
| Marital status (age) | ||||||
| Widowed (65+) | −0.944 | (−2.438, 0.550) | −0.880 | (−3.396, 1.636) | −1.409 | (−3.604, 0.787) |
| Widowed (75+) | −4.524 | (−8.617, −0.431) * | −2.471 | (−10.24, 5.298) | −9.140 | (−15.776, −2.504) * |
| Education (age) | ||||||
| None (19–64) | −0.091 | (−0.140, −0.042) * | −0.005 | (−0.053, 0.043) | −0.284 | (−0.382, −0.187) * |
| Elementary (65+) | 0.631 | (−0.597, 1.859) | 0.100 | (−1.784, 1.984) | 0.510 | (−1.352, 2.372) |
| Elementary (75+) | −1.669 | (−4.888, 1.550) | −1.911 | (−6.938, 3.116) | −1.650 | (−6.956, 3.657) |
| Respiratory mortality | ||||||
| Marital status (age) | ||||||
| Widowed (65+) | −0.944 | (−2.438, 0.550) | 0.714 | (−0.594, 2.021) | 2.158 | (0.894, 3.423) |
| Widowed (75+) | −4.524 | (−8.617, −0.431) * | 1.239 | (−2.840, 5.318) | 6.705 | (2.778, 10.632) |
| Education (age) | ||||||
| None (19–64) | −0.032 | (−0.055, −0.009) * | 0.008 | (−0.013, 0.030) | −0.167 | (−0.221, −0.114) * |
| Elementary (65+) | −0.884 | (−1.582, −0.185) * | −2.024 | (−3.084, −0.964) * | 2.084 | (1.025, 3.142) |
| Elementary (75+) | −3.167 | (−5.030, −1.305) * | −5.123 | (−8.204, −2.041) * | 5.752 | (2.686, 8.818) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, S.; Nori-Sarma, A.; Lee, K.; Benmarhnia, T.; Dominici, F.; Bell, M.L. The Use of a Quasi-Experimental Study on the Mortality Effect of a Heat Wave Warning System in Korea. Int. J. Environ. Res. Public Health 2019, 16, 2245. https://doi.org/10.3390/ijerph16122245
Heo S, Nori-Sarma A, Lee K, Benmarhnia T, Dominici F, Bell ML. The Use of a Quasi-Experimental Study on the Mortality Effect of a Heat Wave Warning System in Korea. International Journal of Environmental Research and Public Health. 2019; 16(12):2245. https://doi.org/10.3390/ijerph16122245
Chicago/Turabian StyleHeo, Seulkee, Amruta Nori-Sarma, Kwonsang Lee, Tarik Benmarhnia, Francesca Dominici, and Michelle L. Bell. 2019. "The Use of a Quasi-Experimental Study on the Mortality Effect of a Heat Wave Warning System in Korea" International Journal of Environmental Research and Public Health 16, no. 12: 2245. https://doi.org/10.3390/ijerph16122245