Association between Potentially Inappropriate Medication Use and Chronic Diseases in the Elderly

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Study Design
2.2. Study Population
2.3. Definitions of Terms
2.4. Measurements
2.5. Statistical Analysis
2.6. Ethics Approval
3. Results
3.1. Subjects’ Characteristics
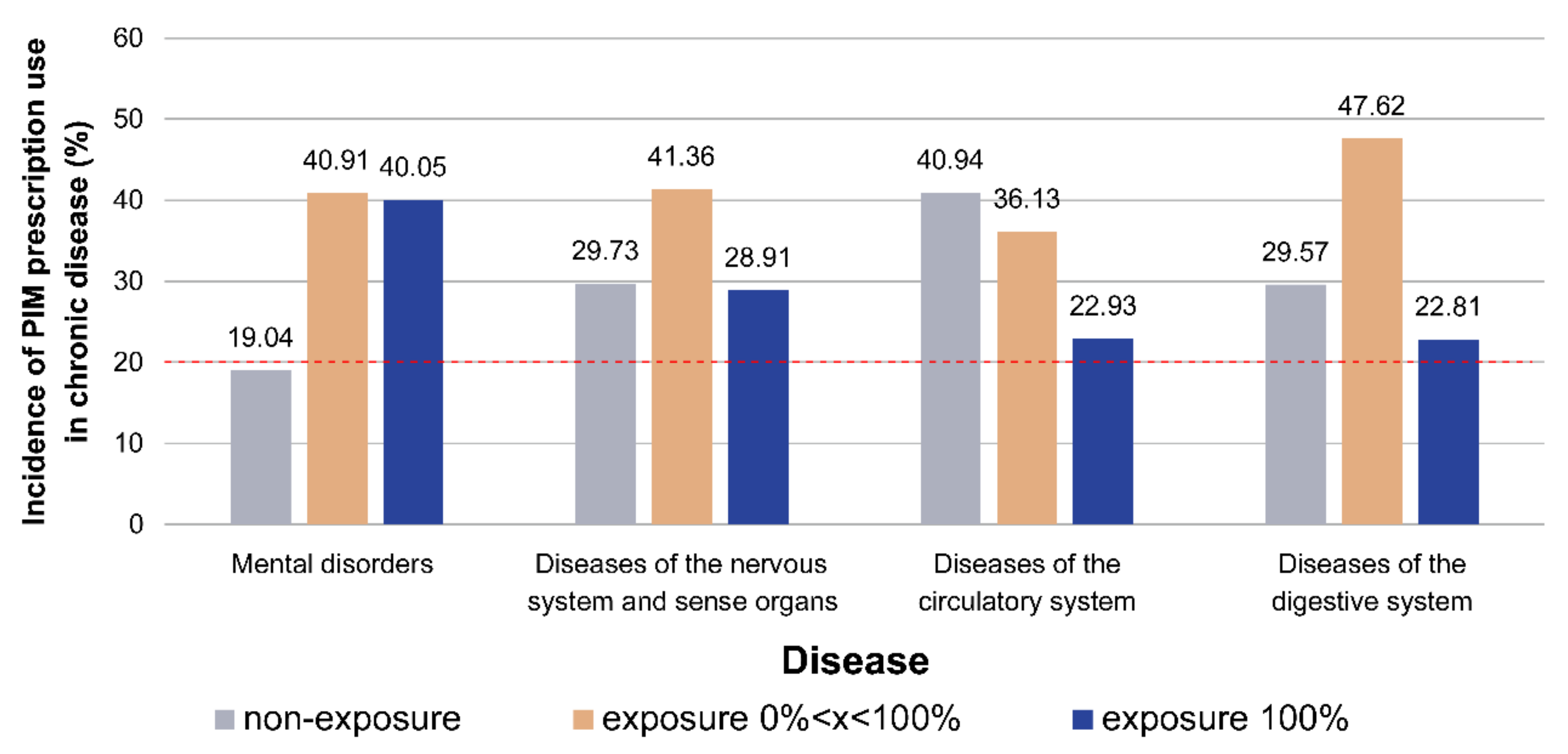
3.2. Probability of Sustained Exposure to PIM Amongst Patients with Various Chronic Diseases
3.3. Analysis of Drugs Prescribed to Patients with Chronic Diseases and Long-term Continuous Exposure to PIM Prescriptions
4. Discussion
4.1. Subject Characteristics
4.2. Long-term Exposure to PIM Prescriptions Amongst Patients with Various Chronic Diseases
4.3. Correlation between Different Chronic Diseases and PIM
4.4. Differences between Beers Criteria 2019 and 2015
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaufman, D.W.; Kelly, J.P.; Rosenberg, L.; Anderson, T.E.; Mitchell, A.A. Recent patterns of medication use in the ambulatory adult population of the United States: The Slone survey. JAMA 2002, 287, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Barat, I.; Andreasen, F.; Damsgaard, E.M.S. The consumption of drugs by 75-year-old individuals living in their own homes. Eur. J. Clin. Pharmacol. 2000, 56, 501–509. [Google Scholar] [CrossRef]
- Bertoldi, A.D.; Barros, A.J.; Hallal, P.C.; Lima, R.C. Drug utilization in adults: Prevalence and individuals determinants. Rev. Saude Publica 2004, 38, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.Q.; Rozenfeld, S.; Klein, C.H.; César, C.C.; Acurcio, F.D. A survey on medicine use by elderly retirees in Belo Horizonte, Southeastern Brazil. Rev. Saude Publica 2008, 42, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Rozenfeld, S.; Fonseca, M.J.; Acurcio, F.A. Drug utilization and polypharmacy among the elderly: A survey in Rio de Janeiro City, Brazil. Rev. Panam. Salud Publica 2008, 23, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Beers, M.; Baran, R.; Frenia, K. Drugs and the elderly, Part 1: The problems facing managed care. Am. J. Manag. Care 2000, 6, 1313–1320. [Google Scholar] [PubMed]
- Chang, C.-B.; Chan, D.-C. Comparison of published explicit criteria for potentially inappropriate medications in older adults. Drugs Aging 2010, 27, 947–957. [Google Scholar] [CrossRef]
- Jano, E.; Aparasu, R.R. Healthcare outcomes associated with beers’ criteria: A systematic review. Ann. Pharmacother. 2007, 41, 438–448. [Google Scholar] [CrossRef]
- Spinewine, A.; Schmader, K.E.; Barber, N.; Hughes, C.; Lapane, K.L.; Swine, C.; Hanlon, J.T. Appropriate prescribing in elderly people: How well can it be measured and optimised? Lancet 2007, 370, 173–184. [Google Scholar] [CrossRef]
- Bahat, G.; Ilhan, B.; Bay, I.; Avci, S.; Tufan, F.; Kilic, C.; Karan, M. Comparing the explicit tools vs. Implicit evaluation among turkish geriatric outpatients. Innov. Aging 2017, 1, 1048. [Google Scholar] [CrossRef]
- By the American Geriatrics Society Beers Criteria Update Expert Panel, American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 2227–2246. [CrossRef] [PubMed]
- Fick, D. Potentially Inappropriate Medication Use in a Medicare Managed Care Population: Association with Higher Costs and Utilization. J. Manag. Care Pharm. 2001, 7, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Hyttinen, V.; Jyrkkä, J.; Valtonen, H. A Systematic Review of the Impact of Potentially Inappropriate Medication on Health Care Utilization and Costs Among Older Adults. Med. Care 2016, 54, 950–964. [Google Scholar] [CrossRef] [PubMed]
- Reich, O.; Rosemann, T.; Rapold, R.; Blozik, E.; Senn, O. Potentially inappropriate medication use in older patients in Swiss managed care plans: Prevalence, determinants and association with hospitalization. PLoS ONE 2014, 9, e105425. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Dell’Aquila, G.; Gasperini, B.; Onder, G.; Lattanzio, F.; Volpato, S.; Corsonello, A.; Maraldi, C.; Bernabei, R.; Cherubini, A. Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents: The ULISSE project. Drugs Aging 2010, 27, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.Y.; Hwang, S.J.; Chen, Y.C.; Chen, T.J.; Lin, M.H.; Chen, L.K. Prevalence of the prescribing of potentially inappropriate medications at ambulatory care visits by elderly patients covered by the Taiwanese National Health Insurance program. Clin. Ther. 2009, 31, 1859–1870. [Google Scholar] [CrossRef]
- Nam, Y.-S.; Han, J.S.; Kim, J.Y.; Bae, W.K.; Lee, K. Prescription of potentially inappropriate medication in Korean older adults based on 2012 Beers Criteria: A cross-sectional population based study. BMC Geriatr. 2016, 16, 118. [Google Scholar] [CrossRef]
- Lin, H.Y.; Liao, C.C.; Cheng, S.H.; Wang, P.C.; Hsueh, Y.S. Association of potentially inappropriate medication use with adverse outcomes in ambulatory elderly patients with chronic diseases: Experience in a Taiwanese medical setting. Drugs Aging 2008, 25, 49–59. [Google Scholar] [CrossRef]
- Chu, H.Y.; Chen, C.C.; Cheng, S.H. Continuity of care, potentially inappropriate medication, and health care outcomes among the elderly: Evidence from a longitudinal analysis in Taiwan. Med. Care 2012, 50, 1002–1009. [Google Scholar] [CrossRef]
- Lu, W.H.; Wen, Y.W.; Chen, L.K.; Hsiao, F.Y. Effect of polypharmacy, potentially inappropriate medications and anticholinergic burden on clinical outcomes: A retrospective cohort study. CMAJ 2015, 187, e130–e137. [Google Scholar] [CrossRef]
- Jacob, L.; Breuer, J.; Kostev, K. Prevalence of chronic diseases among older patients in German general practices. Ger. Med. Sci. 2016, 14, 3. [Google Scholar]
- Marengoni, A.; Winblad, B.; Karp, A.; Fratiglioni, L. Prevalence of chronic diseases and multimorbidity among the elderly population in Sweden. Am. J. Public Health 2008, 98, 1198–1200. [Google Scholar] [CrossRef]
- Wu, F.; Guo, Y.; Kowal, P.; Jiang, Y.; Yu, M.; Li, X.; Zheng, Y.; Xu, J. Prevalence of major chronic conditions among older Chinese adults: The Study on Global AGEing and adult health (SAGE) wave 1. PLoS ONE 2013, 8, e74176. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, R.M. Multiple chronic conditions: A public health challenge. Public Health Rep. 2010, 125, 626–627. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration List of Chronic Disease Included. Available online: https://www.nhi.gov.tw/Content_List.aspx?n=0205B47A1C459B5A&topn=D39E2B72B0BDFA15 (accessed on 20 April 2019).
- Guaraldo, L.; Cano, F.G.; Damasceno, G.S.; Rozenfeld, S. Inappropriate medication use among the elderly: A systematic review of administrative databases. BMC Geriatr. 2011, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Sheikh-Taha, M.; Dimassi, H. Potentially inappropriate home medications among older patients with cardiovascular disease admitted to a cardiology service in USA. BMC Cardiovasc. Disord. 2017, 17, 189. [Google Scholar] [CrossRef] [PubMed]
- Swanoski, M.T.; Little, M.M.; St Hill, C.A.; Ware, K.B.; Chapman, S.; Lutfiyya, M.N. Potentially Inappropriate Medication Prescribing in U.S. Older Adults with Selected Chronic Conditions. Consult. Pharm. 2017, 32, 525–534. [Google Scholar] [CrossRef]
- Kanagasanthosh, K.; Topno, I.; Aravindkumar, B. Prevalence of potentially inappropriate medication use and drug utilization pattern in elderly patients: A prospective study from a tertiary care hospital. Int. J. Res. Med. Sci. 2017, 3, 11. [Google Scholar] [CrossRef]
- Lang, P.O.; Hasso, Y.; Drame, M.; Vogt-Ferrier, N.; Prudent, M.; Gold, G.; Michel, J.P. Potentially inappropriate prescribing including under-use amongst older patients with cognitive or psychiatric co-morbidities. Age Ageing 2010, 39, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Huang, N.; Chou, Y.J. Trends in the prevalence of multiple chronic conditions in Taiwan from 2000 to 2010: A population-based study. Prev. Chronic Dis. 2014, 11, E187. [Google Scholar] [CrossRef]
- Naughton, C.; Bennett, K.; Feely, J. Regional variation in prescribing for chronic conditions among an elderly population using a pharmacy claims database. Ir. J. Med. Sci. 2006, 175, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.J.; Lee, Y.T.; Tzeng, S.L.; Lee, H.C.; Tsai, C.F.; Chen, C.C.; Chen, S.C.; Lee, M.C. Potentially Inappropriate Prescribing in Disabled Older Patients with Chronic Diseases: A Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions versus Beers 2012 Criteria. Med. Princ. Pract. 2015, 24, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, F.; Bennett, K.; Fahey, T.; Kenny, R.A.; Cahir, C. Longitudinal prevalence of potentially inappropriate medicines and potential prescribing omissions in a cohort of community-dwelling older people. Eur. J. Clin. Pharmacol. 2015, 71, 473–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, C.; Sangl, J.; Bierman, A.S.; Miller, M.R.; Friedman, B.; Wickizer, S.W.; Meyer, G.S. Potentially inappropriate medication use in the community-dwelling elderly: Findings from the 1996 Medical Expenditure Panel Survey. JAMA 2001, 286, 2823–2829. [Google Scholar] [CrossRef] [PubMed]
- Vieira de Lima, T.J.; Garbin, C.A.; Garbin, A.J.; Sumida, D.H.; Saliba, O. Potentially inappropriate medications used by the elderly: Prevalence and risk factors in Brazilian care homes. BMC Geriatr. 2013, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Tsai, R.; Noone, M.; Johnson, B.; Pradeep, V.G.; Verghese, J. Potentially inappropriate medication use in individuals with mild cognitive impairment: Results from the Kerala Einstein Study. J. Am. Geriatr. Soc. 2012, 60, 1369–1370. [Google Scholar] [CrossRef]
- De Jong, M.R.; Van der Elst, M.; Hartholt, K.A. Drug-related falls in older patients: Implicated drugs, consequences, and possible prevention strategies. Ther. Adv. Drug Saf. 2013, 4, 147–154. [Google Scholar] [CrossRef]
- Lindsey, P.L. Psychotropic medication use among older adults: What all nurses need to know. J. Gerontol. Nurs. 2009, 35, 28–38. [Google Scholar] [CrossRef]
- Kumar, N.; Sharma, S.; Kapoor, V. Adverse Drug Events in Patients with Mental Disorder in an Ambulatory Setting. Int. J. Appl. Basic Med. Res. 2017, 7, 108–111. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.J.; Wu, J.; Kelton, C.M.; Jing, Y.; Fan, H.; Keck, P.E.; Patel, N.C. Exposure to potentially dangerous drug-drug interactions involving antipsychotics. Psychiatr. Serv. 2012, 63, 1080–1088. [Google Scholar] [CrossRef]
- Stewart, R.B.; Cerda, J.J.; Moore, M.T.; Hale, W.E. Metoclopramide: An analysis of inappropriate long-term use in the elderly. Ann. Pharmacother. 1992, 26, 977–979. [Google Scholar] [CrossRef] [PubMed]
- By the American Geriatrics Society Beers Criteria Update Expert Panel, American Geriatrics Society 2019 Updated AGS Beers Criteria (R) for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Patients with PIM Prescriptions (n = 16,766) | Patients without PIM Prescriptions (n = 14,987) | p-Value * |
|---|---|---|---|
| Age | <0.001 *** | ||
| 65–74 years | 8130(48.49) | 8442(56.33) | <0.001 *** |
| 75–84 years | 6242(37.23) | 4889(32.62) | <0.001 *** |
| ≥85 years | 2394(14.28) | 1656(11.05) | reference |
| Sex | 0.096 | ||
| Male | 7620(45.45) | 6672(44.52) | |
| Female | 9146(54.55) | 8315(55.48) | |
| Department | <0.001 *** | ||
| Cardiology | 4629(15.6) | 3248(16.97) | 0.022 * |
| Chest | 1032(3.48) | 496(2.59) | <0.001 *** |
| Endocrinology | 1696(5.72) | 1132(5.91) | 0.361 |
| Family medicine | 3785(12.75) | 3574(18.67) | <0.001 *** |
| Gastroenterology | 2040(6.88) | 612(3.2) | <0.001 *** |
| Internal medicine | 3987(13.43) | 3961(20.7) | <0.001 *** |
| Nephrology | 1053(3.55) | 456(2.38) | <0.001 *** |
| Neurology | 3886(13.09) | 1528(7.99) | <0.001 *** |
| Neurosurgery | 707(2.38) | 368(1.92) | 0.007 ** |
| Orthopedics | 1528(5.15) | 1058(5.53) | 0.116 |
| Others | 1945(6.55) | 1237(6.47) | reference |
| Psychiatry | 1236(4.16) | 144(0.75) | <0.001 *** |
| Surgery | 500(1.68) | 379(1.98) | 0.023 * |
| Urology | 1655(5.58) | 945(4.94) | 0.048 * |
| Number of chronic disease | <0.001 *** | ||
| 1 | 4281(25.53) | 6495(43.34) | <0.001 *** |
| 2 | 5197(31) | 4701(31.37) | <0.001 *** |
| 3 | 3585(21.38) | 2619(17.48) | <0.001 *** |
| 4 | 2116(12.62) | 862(5.75) | <0.001 *** |
| ≧5 | 1587(9.47) | 310(2.07) | reference |
| Classification of Chronic Disease | Number of Patients with Chronic Diseases | Patients with 100% Continuous Exposure to PIM Prescriptions, n (%) | Number of Chronic Disease Prescriptions | PIM Prescription Rate, n (%) | PIM Prescription, ORa | 95% CI |
|---|---|---|---|---|---|---|
| Neoplasms | 1441 | 236 (16.38) | 17,593 | 5983(34.01) | 0.83 *** | 0.79–0.87 |
| Endocrine, nutritional and metabolic diseases and immunity disorders | 8798 | 1304 (14.82) | 121,854 | 41,141 (33.76) | 0.82 *** | 0.8–0.84 |
| Mental disorders | 3618 | 1449 (40.05) | 48,316 | 26,986 (55.85) | 3.16 *** | 3.06–3.28 |
| Diseases of the nervous system and sense organs | 1463 | 423 (28.91) | 19,850 | 9512 (47.92) | 1.72 *** | 1.64–1.80 |
| Diseases of the circulatory system | 8491 | 1947 (22.93) | 109,119 | 43,761 (40.10) | 1.33 *** | 1.31–1.36 |
| Diseases of the respiratory system | 1774 | 252 (14.21) | 24,664 | 9338 (37.86) | 0.78 *** | 0.74–0.82 |
| Diseases of the digestive system | 2012 | 459 (22.81) | 27,846 | 11,446 (41.10) | 1.09 ** | 1.04–1.15 |
| Diseases of the genitourinary system | 1201 | 226 (18.82) | 17,105 | 7423 (43.40) | 1.65 *** | 1.56–1.74 |
| Diseases of the musculoskeletal system and connective tissue | 3793 | 579 (15.26) | 45,063 | 16,784 (37.25) | 1.05 ** | 1.01–1.10 |
| Diseases of the eye and its accessory organs | 182 | 7 (3.85) | 2005 | 605 (30.17) | 0.24 *** | 0.18–0.32 |
| Infectious and parasitic diseases | 44 | 5 (11.36) | 224 | 66 (29.46) | 0.64 * | 0.43–0.93 |
| Congenital defects | 131 | 22 (16.79) | 1768 | 739 (41.80) | 1.46 *** | 1.24–1.72 |
| Diseases of the skin and subcutaneous tissue | 513 | 36 (7.02) | 8177 | 2906 (35.54) | 0.46 *** | 0.41–0.52 |
| Diseases of the blood and blood-forming organs | 217 | 28 (12.90) | 3180 | 1128 (35.47) | 0.73 *** | 0.63–0.85 |
| Diseases of the ear and mastoid | 415 | 72 (17.35) | 6333 | 2318 (36.6) | 1.05 | 0.95–1.15 |
| Other | 7505 | 1328 (17.69) | 104,392 | 38,933 (37.3) | 1.18 *** | 1.15–1.21 |
| PIM | Total (%) | Mental Disorders | Diseases of the Nervous System | Diseases of the Circulatory System | Diseases of the Digestive System |
|---|---|---|---|---|---|
| Anti-cholinergics | 6230 (4.84%) | ||||
| First-generation anti-histamines | 3321 | 833(25.08%) | 437(13.16%) | 1579(47.55%) | 472(14.21%) |
| Anti-Parkinsonian agents | 2159 | 618(28.62%) | 1006(46.6%) | 449(20.8%) | 86(3.98%) |
| Anti-spasmodics | 750 | 179(23.87%) | 70(9.33%) | 299(39.87%) | 202(26.93%) |
| Anti-thrombotics | 3416 (2.65%) | ||||
| Ticlopidine | 3416 | 436(12.76%) | 221(6.47%) | 2384(69.79%) | 375(10.98%) |
| Cardiovascular | 26,157 (20.32%) | ||||
| Peripheral alpha-1 blockers | 8753 | 1346(15.38%) | 641(7.32%) | 5713(65.27%) | 1053(12.03%) |
| Central alpha blockers | 935 | 79(8.45%) | 24(2.57%) | 623(66.63%) | 209(22.35%) |
| Dronedarone | 3288 | 327(9.95%) | 150(4.56%) | 2638(80.23%) | 173(5.26%) |
| Digoxin | 3181 | 299(9.4%) | 185(5.82%) | 2470(77.65%) | 227(7.14%) |
| Amiodarone | 935 | 79(8.45%) | 24(2.57%) | 623(66.63%) | 209(22.35%) |
| Central nervous system | 68,425 (53.16%) | ||||
| Anti-depressants, alone or in combination | 3501 | 1530(43.7%) | 428(12.23%) | 1189(33.96%) | 354(10.11%) |
| Anti-psychotics, first- (conventional) and second- (atypical) generation | 9087 | 4854(53.42%) | 1223(13.46%) | 2457(27.04%) | 553(6.09%) |
| Benzodiazepines | 45,242 | 17,977(39.74%) | 5105(11.28%) | 17,699(39.12%) | 4461(9.86%) |
| Non-benzodiazepine, benzodiazepine receptor agonist hypnotics | 10,588 | 5124(48.39%) | 773(7.3%) | 3673(34.69%) | 1018(9.61%) |
| Endocrine | 7094 (5.51%) | ||||
| Estrogens with or without progestins | 327 | 92(28.13%) | 39(11.93%) | 168(51.38%) | 28(8.56%) |
| Insulin, sliding scale | 5389 | 1112(20.63%) | 633(11.75%) | 2857(53.02%) | 787(14.6%) |
| Megestrol | 5 | 2(40%) | 0(0%) | 2(40%) | 1(20%) |
| Glyburide | 1373 | 314(22.87%) | 76(5.54%) | 751(54.7%) | 232(16.9%) |
| Gastrointestinal | 8666 (6.73%) | ||||
| Metoclopramide | 5961 | 1134(19.02%) | 474(7.95%) | 2428(40.73%) | 1925(32.29%) |
| Proton-pump inhibitors | 2705 | 294(10.87%) | 106(3.92%) | 863(31.9%) | 1442(53.31%) |
| Pain medications | 5435 (4.22%) | ||||
| Non-selective cyclooxygenase inhibitors | 3300 | 809(24.52%) | 488(14.79%) | 1581(47.91%) | 422(12.79%) |
| Indomethacin | 217 | 39(17.97%) | 12(5.53%) | 110(50.69%) | 56(25.81%) |
| Skeletal muscle relaxants | 1918 | 502(26.17%) | 285(14.86%) | 824(42.96%) | 307(16.01%) |
| Genitourinary | 3300(2.56) | ||||
| Desmopressin | 3300 | 173(5.24%) | 73(2.21%) | 264(8%) | 133(4.03%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-C.; Ku, P.-J.; Lu, H.-L.; Hsu, K.-C.; Trezise, D.; Wang, H.-Y. Association between Potentially Inappropriate Medication Use and Chronic Diseases in the Elderly. Int. J. Environ. Res. Public Health 2019, 16, 2189. https://doi.org/10.3390/ijerph16122189
Wang T-C, Ku P-J, Lu H-L, Hsu K-C, Trezise D, Wang H-Y. Association between Potentially Inappropriate Medication Use and Chronic Diseases in the Elderly. International Journal of Environmental Research and Public Health. 2019; 16(12):2189. https://doi.org/10.3390/ijerph16122189
Chicago/Turabian StyleWang, Tzu-Chueh, Pou-Jen Ku, Hai-Lin Lu, Kung-Chuan Hsu, Damien Trezise, and Hue-Yu Wang. 2019. "Association between Potentially Inappropriate Medication Use and Chronic Diseases in the Elderly" International Journal of Environmental Research and Public Health 16, no. 12: 2189. https://doi.org/10.3390/ijerph16122189