Patterns of Life Lost to Cancers with High Risk of Death in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Analysis Index
2.3. High Death-Risk Cancers
2.4. Statistical Analysis
3. Results
3.1. Mortality and Ranks of Cancers
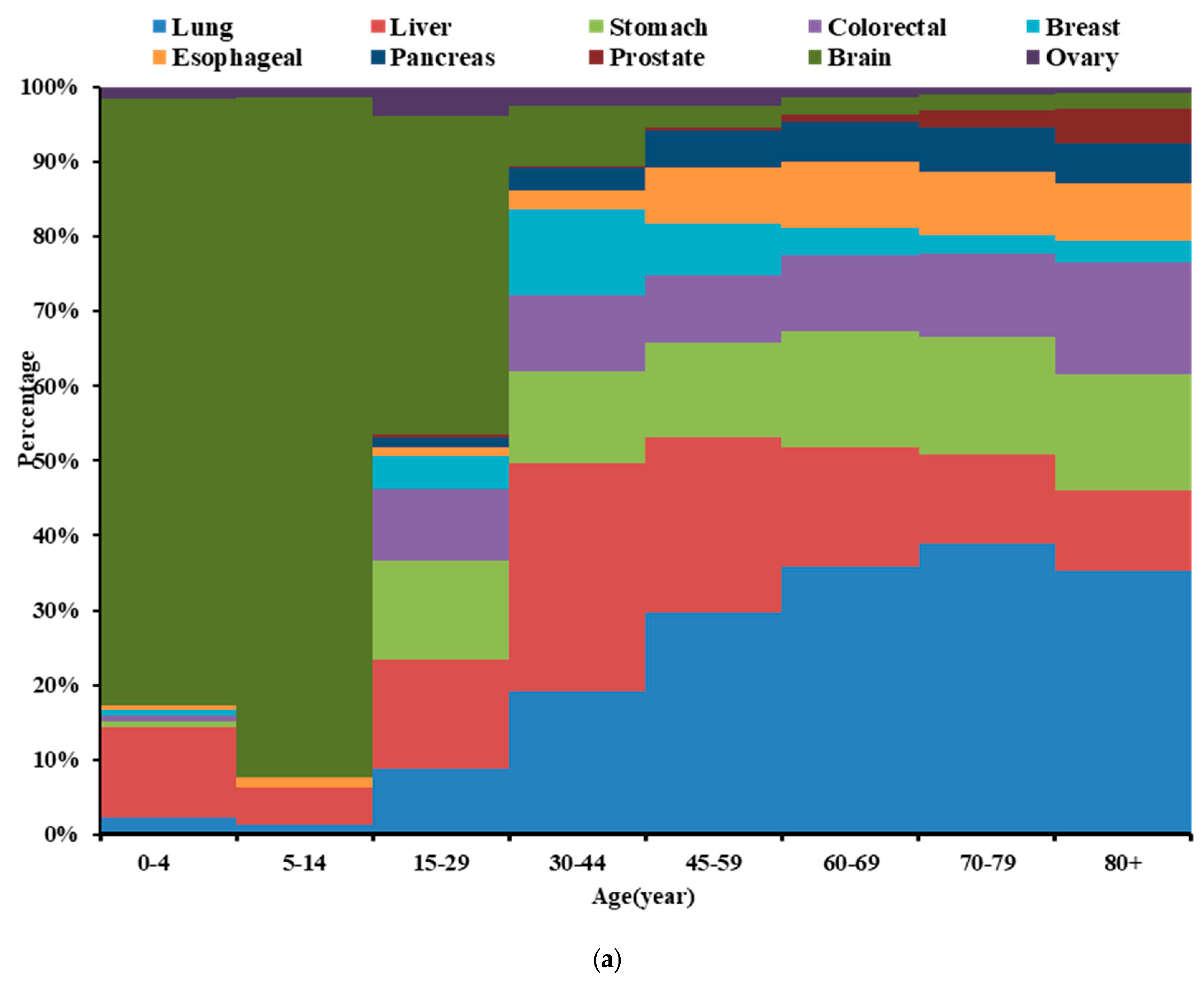
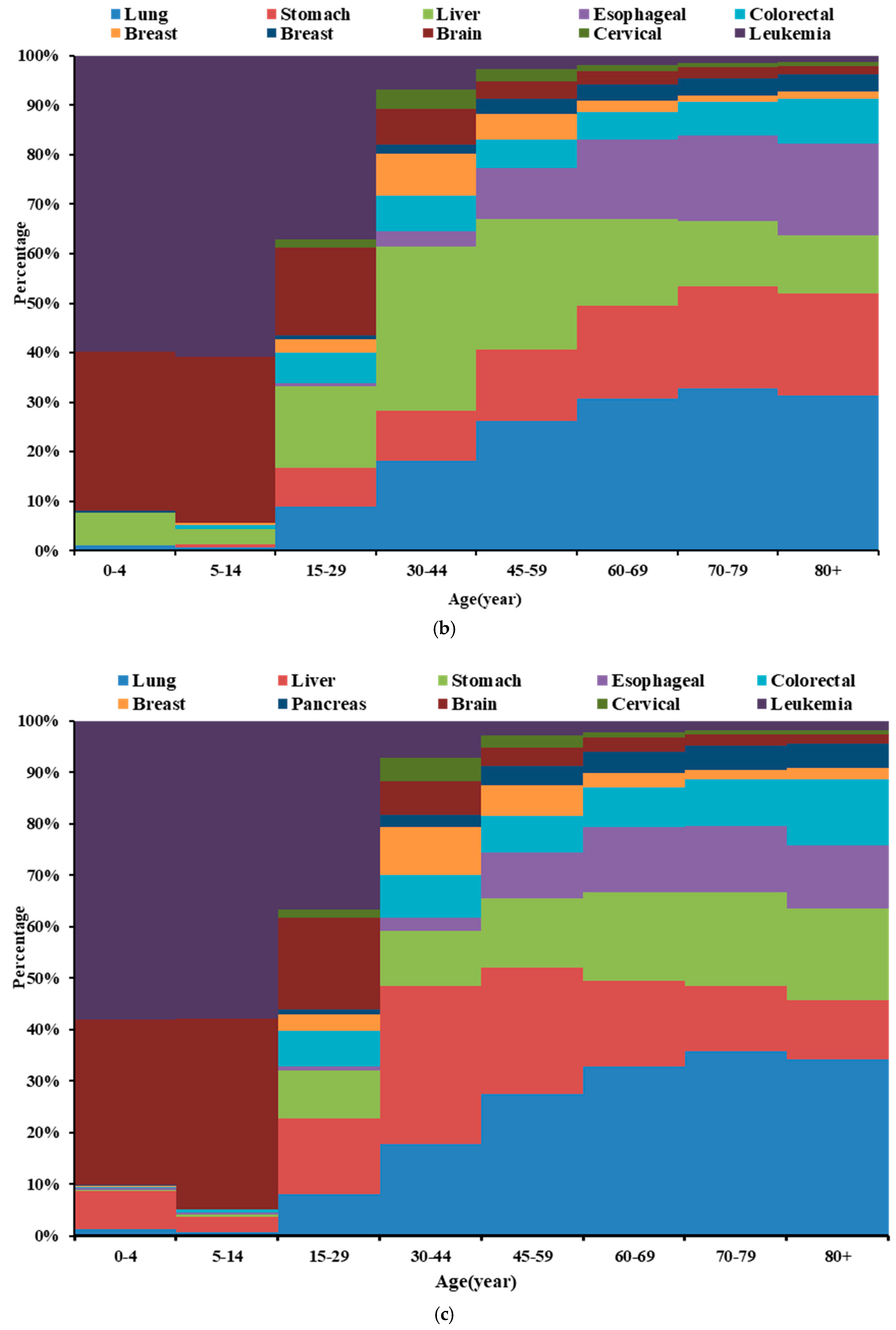
3.2. Age Distribution of High Death-Risk Cancers
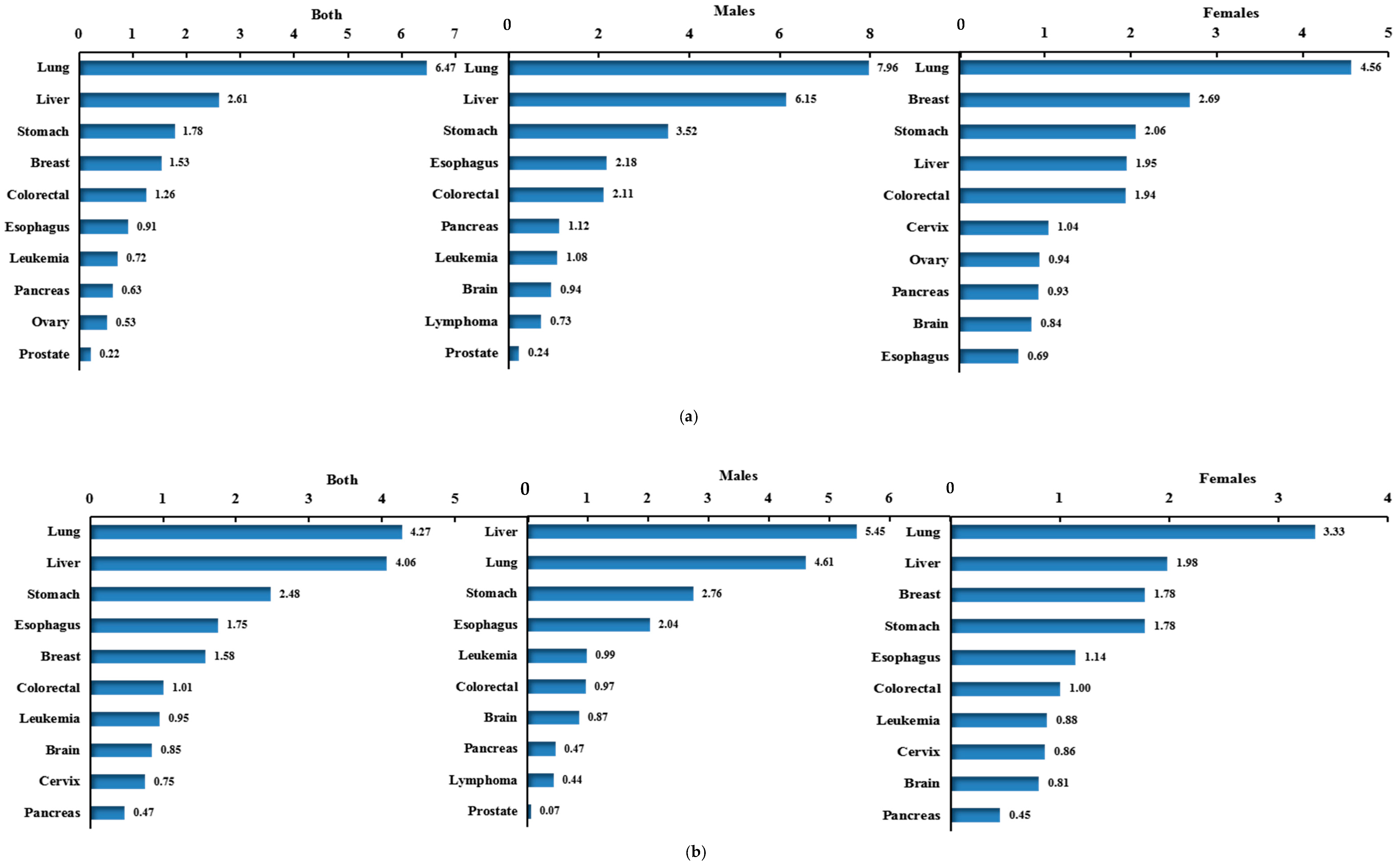
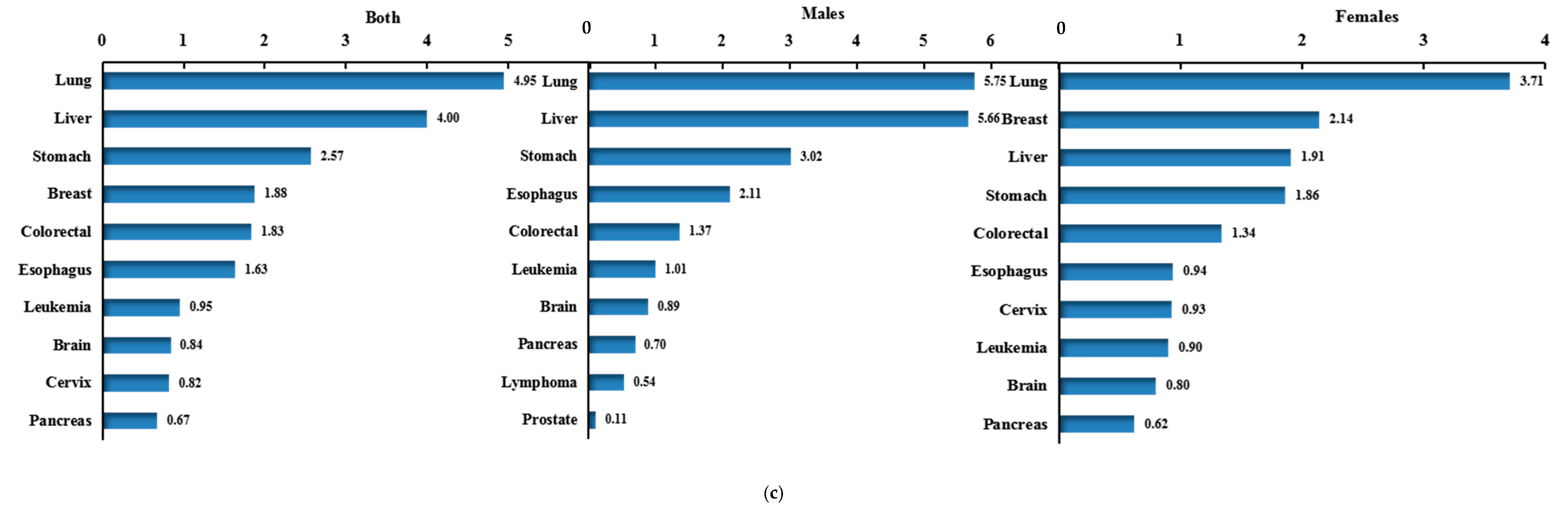
3.3. Potential Years of Life Lost (PYLL) and Ranks of High Death-Risk Cancers
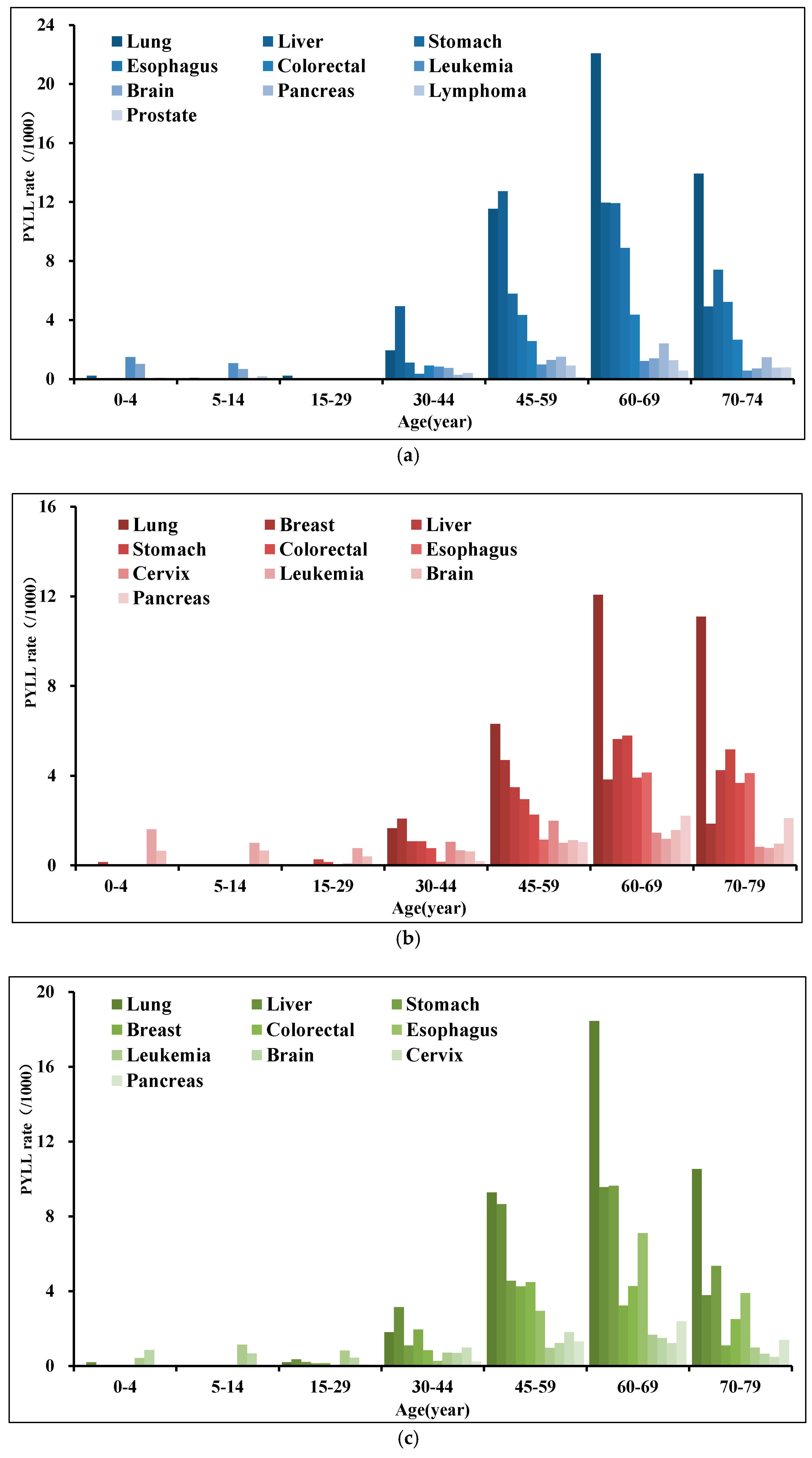
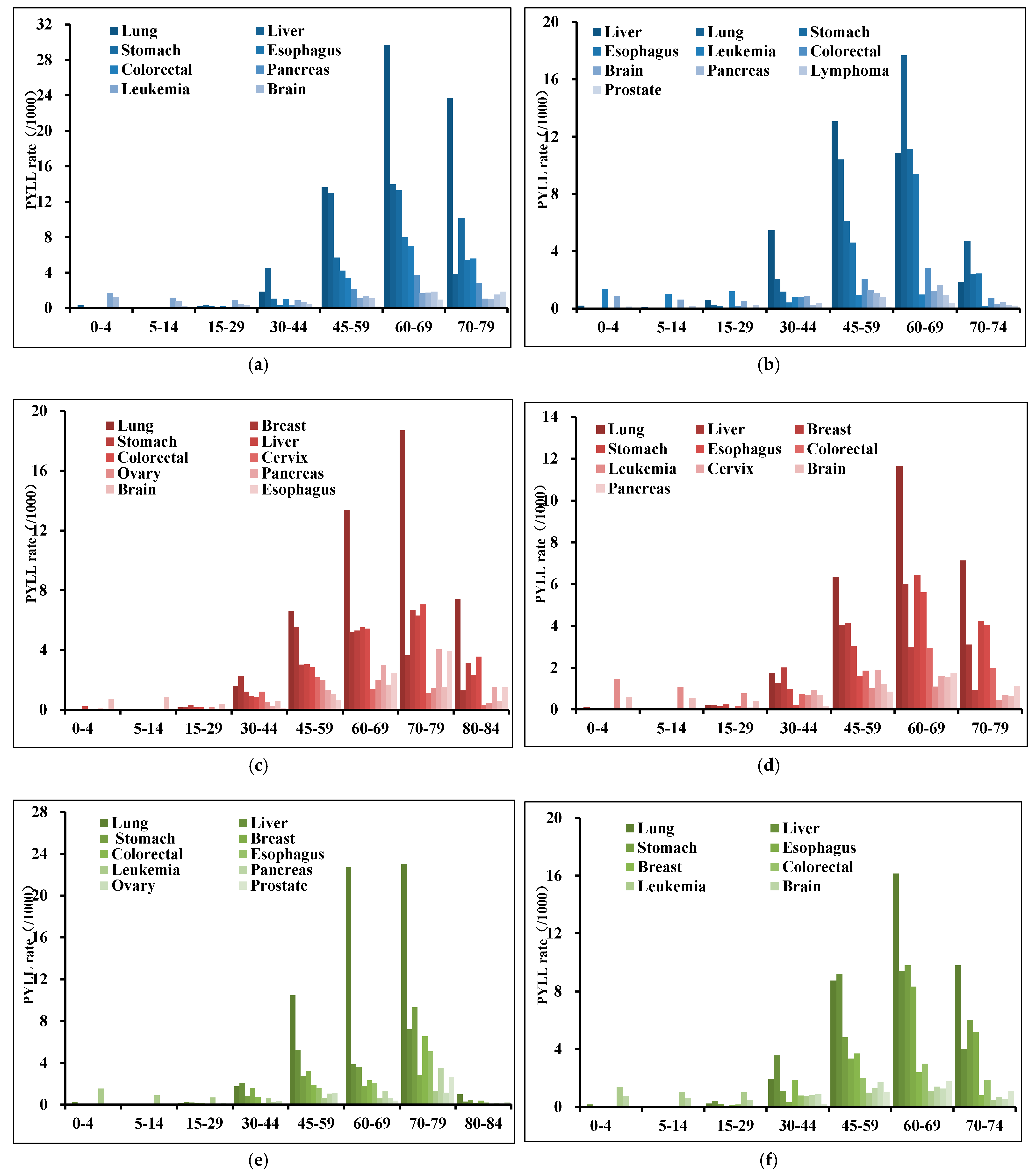
3.4. PYLL Age Distribution of High Death-Risk Cancers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soeriomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimate of incidence and mortality world wide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The Global Burden of Cancer 2013. JAMA J. Am. Med. Assoc. 2015, 1, 505–527. [Google Scholar]
- People’s Republic of China National Bureau of Statistics. Main Data Bulletin of the Sixth National Population Census 2010 (No. 1). Chin. J. Fam. Plan. 2011, 19, 511–512. [Google Scholar]
- Wang, Z.L.; Wang, R.S.; Zhou, C.B. Considerations on the current problems, causes and counter measures of China’s agricultural population. China’s Agric. Reclam. 2011, 12, 43–45. [Google Scholar]
- Li, L.; Fu, H. China’s health care system reform: Progress and prospects. Int. J. Health Plan. Manag. 2017, 32, 240–253. [Google Scholar] [CrossRef]
- Kamimura, A.; Armenta, B.; Nourian, M.; Assasnik, N.; Nourian, K.; Chernenko, A. Perceived environmental pollution and its impact on health in China, Japan, and South Korea. J. Prev. Med. Public Health 2017, 50, 188–194. [Google Scholar] [CrossRef]
- Shi, H.Y. Health problems and related strategies brought about by the aging population in China. Electron. J. Clin. Med. Lit. 2018, 5, 174–175. [Google Scholar]
- Chen, W.; Zheng, R.; Zeng, H.; Zhang, S. Trend analysis of the changes of male/female, urban/rural incidences and average age of cancer patients in China 1989–2008. Chin. J. Oncol. 2014, 36, 796–800. [Google Scholar]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [Green Version]
- Liu, L. The global significance of China’s cancer burden and control effort. Ann. Transl. Med. 2014, 2, 64. [Google Scholar]
- Li, S.; Zhang, X.; Yan, Y.; Wang, K.; Rui, D.; Pang, L.; Li, F. High Cancer Burden in Elderly Chinese, 2005–2011. Int. J. Environ. Res. Public. Health. 2015, 12, 12196–12211. [Google Scholar] [CrossRef]
- H, J.; Chen, W. Annual Report of China Cancer Registry, 2016; Tsinghua University Press: Beijing, China, 2013; pp. 70–120. [Google Scholar]
- Chen, W.; Zheng, R.; Zhang, S.; Zeng, H.; Zhou, X.; H, J. Report of Cancer Incidence and Mortality in China, 2013. China Cancer 2017, 26, 1–7. [Google Scholar]
- National Cancer Center. Chinese Guideline for Cancer Registration; Beijing People’s Med. Publ. House: Beijing, China, 2016; pp. 59–75.
- Gurado, M.P.; Edwards, B.; Shin, H.R.; Strom, H.; Ferlay, J.; Heanue, M. Cancer Incidence in Five Continents; IARC: Lyon, France, 2008; Volume IX, pp. 1–837. [Google Scholar]
- Bray, F.; Parkin, D.M. Evaluation of data quality in the cancer registry: principles and methods. Part I: comparability, validity and timeliness. Eur. J. Cancer 2009, 45, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Bray, F. Evaluation of data quality in the cancer registry: principles and methods. Part II: completeness. Eur. J. Cancer 2009, 45, 756–764. [Google Scholar] [CrossRef]
- Freyberger, H.J.; Schultemarkwort, E.; Dilling, H. WHO Crosswalk for the Tenth Revision of the International Classification of Diseases, Chapter V (F): ICD-9 vs. ICD-10. Fortschr. Der. Neurol. Psychiatr. 1993, 61, 128–143. [Google Scholar] [CrossRef]
- Ko, Y.S.; Tsai, H.C.; Chi, M.H.; Su, C.C.; Lee, I.H.; Chen, P.S.; Chen, K.C.; Yang, Y.K. Higher mortality and years of potential life lost of suicide in patients with schizophrenia. Psychiatry Res. 2018, 270, 531–537. [Google Scholar] [CrossRef]
- Romeder, J.M.; Mcwhinnie, J.R. Potential Years of Life Lost Between Ages 1 and 70: An Indicator of Premature Mortality for Health Planning. Int. J. Epidemiol. 1977, 6, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.; Xu, H.; Li, H.; Xu, A.; Sun, B. Comparison of calculating methods for life lost. China Health Stat. 2004, 21, 222–223. [Google Scholar]
- National Statistical Bureau of the People’s Republic of China. Main Data Bulletin of the Sixth National Population Census 2010 (No. 1). Chin. J. Fam. Plan. 2011, 54, 511–512. [Google Scholar]
- Shu, X.Y.; Wen, Y.; Zong, Z.H.; Zhou, J.F. Indirect Estimation and Evaluation of the Average Life Expectancy of Population in China: Based on the Data of the Sixth National Population Census. J. Demogr. 2014, 36, 18–24. [Google Scholar]
- World Health Organization. WHO methods and data sources for global burden of disease estimates 2000–2015. Geneva WHO 2017, 1, 1–43. [Google Scholar]
- Robson, B.; Purdie, G.; Cram, F.; Simmonds, S. Age standardisation–an indigenous standard? Emerg. Themes Epidemiol. 2007, 4, 3. [Google Scholar] [CrossRef]
- Toriola, A.T.; Colditz, G.A. Trends in breast cancer incidence and mortality in the United States: Implications for prevention. Breast Cancer Res. Treat. 2013, 138, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Ghoncheh, M.; Pournamdar, Z.; Salehiniya, H. Incidence and Mortality and Epidemiology of Breast Cancer in the World. Asian Pac. J. Cancer Prev. 2016, 17, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Li, S.; Yan, Y.; Pang, L.; Guo, S.; Niu, Q.; Xu, S.; Xiang, H.; Ma, R. Burden of disease due to malignant neoplasms in China, 2006–2010. Chin. J. Cancer Prev. Treat. 2015, 22, 733–737. [Google Scholar]
- Yan, Y.; Li, S.; Liu, J.; Rui, D.; Zhang, X.; Zhao, R.; Wang, Y.; Wu, M.; Hao, H. Cancer burden and urban-rural differences in China, 2009. Chin. J. Cancer Prev. Treat. 2016, 23, 279–287. [Google Scholar]
- Pan, S.; Liu, J.; Hong, Q.; Zhu, A. Analysis of Disease Burden for Cancer in Jiangyin Residents, Jiangsu Province, 2012. China Cancer 2016, 25, 255–259. [Google Scholar]
- Jiang, N.; Li, S.; Yan, Y.; Zhang, X.; Zhang, K.; Zhao, R.; Wang, Y.; Hao, H. Trends of disease burden of liver cancer in Chinese cancer registries, 2005–2009. Mod. Prev. Med. 2017, 44, 3483–3507. [Google Scholar]
- Li, S.; Meng, L.; Chiolero, A.; Ma, C.; Xi, B. Trends in smoking prevalence and attributable mortality in China, 1991–2011. Prev. Med. 2016, 93, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Yang, Y.; Li, Q.; Wang, C.; Yang, G.H. Population-based survey of secondhand smoke exposure in China. Biomed. Environ. Sci. 2010, 23, 430–436. [Google Scholar] [CrossRef]
- Chen, W.; Sun, K.; Zheng, R.; Zhang, S.; Zeng, H.; Zhou, X.; H, J. Report of Cancer Incidence and Mortality in Different Areas of Chin, 2014. China Cancer 2018, 27, 1–14. [Google Scholar]
- Liang, X.; Bi, S.; Yang, W.; Wang, L.; Cui, G.; Cui, F.; Zhang, Y.; Liu, J.; Gong, X.; Chen, Y.; et al. Epidemiological serosurvey of hepatitis B in China declining HBV prevalence due to hepatitis B vaccination. Vaccine 2009, 27, 6550–6557. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Chen, T.; Thorgeirsson, S.S.; Zhan, Q.; Chen, J.; Park, J.H.; Lu, P.; Hsia, C.C.; Wang, N.; Xu, L.; et al. Dramatic reduction of liver cancer incidence in young adults: 28 year follow-up of etiological interventions in an endemic area of China. Carcinogenesis 2013, 34, 1800–1805. [Google Scholar] [CrossRef]
- Xie, W.C.; Chan, M.H.; Mak, K.C.; Chan, W.T.; He, M. Trends in the incidence of 15 common cancers in Hong Kong, 1983–2008. Asian Pac. J. Cancer Prev. 2012, 13, 3911–3916. [Google Scholar] [CrossRef]
- Kitano, S.; Kitajima, M.; Konishi, F.; Kondo, H.; Satomi, S.; Shimizu, N. A multicenter study on laparoscopic surgery for colorectal cancer in Japan. Surg. Endosc. 2006, 20, 1348–1352. [Google Scholar] [CrossRef]
- Okuno, K. Surgical treatment for digestive cancer. Current issues colon cancer. Dig. Surg. 2007, 24, 108–114. [Google Scholar] [CrossRef]
- Goodman, M.T.; Shvetsov, Y.B.; Mcduffie, K.; Wilkens, L.R.; Zhu, X.; Thompson, P.J.; Ning, L.; Killeen, J.; Kamemoto, L.; Hernandez, B.Y. Sequential Acquisition of Human Papillomavirus (HPV) Infection of the Anus and Cervix: The Hawaii HPV Cohort Study. J. Infect. Dis. 2010, 201, 1331–1339. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Sex | All Areas | Urban Areas | Rural Areas | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CMR * | SM RC | SM RW | % | R | CMR* | SM RC | SM RW | % | R | CMR * | SM RC | SM RW | % | R | ||
| Esophagus | M | 23.0 | 14.9 | 15.0 | 10.5 | 4 | 16.8 | 10.1 | 10.2 | 7.5 | 5 | 29.0 | 20.2 | 20.2 | 13.5 | 4 |
| F | 10.1 | 5.6 | 5.6 | 7.6 | 6 | 6.2 | 3.1 | 3.1 | 4.5 | 7 | 13.9 | 8.4 | 8.3 | 11.0 | 4 | |
| B | 16.6 | 10.2 | 10.2 | 9.4 | 4 | 11.5 | 6.5 | 6.6 | 6.4 | 6 | 21.6 | 14.2 | 14.2 | 12.6 | 4 | |
| stomach | M | 32.9 | 21.4 | 21.3 | 15.0 | 3 | 29.5 | 17.8 | 17.7 | 13.2 | 3 | 36.0 | 25.4 | 25.2 | 16.8 | 3 |
| F | 15.1 | 8.8 | 8.6 | 11.4 | 2 | 13.6 | 7.4 | 7.2 | 9.8 | 3 | 16.6 | 10.3 | 10.2 | 13.2 | 2 | |
| B | 24.1 | 14.9 | 14.8 | 13.7 | 3 | 21.6 | 12.4 | 12.2 | 11.9 | 3 | 26.6 | 17.7 | 17.5 | 15.5 | 2 | |
| Colorectal | M | 14.6 | 9.4 | 11.1 | 6.7 | 5 | 18.5 | 10.9 | 12.9 | 8.3 | 4 | 10.9 | 7.7 | 8.9 | 5.0 | 5 |
| F | 11.4 | 6.4 | 7.5 | 8.7 | 4 | 14.4 | 7.4 | 8.8 | 10.4 | 2 | 8.4 | 5.3 | 6.0 | 6.7 | 5 | |
| B | 15.2 | 9.0 | 10.6 | 7.3 | 5 | 16.5 | 9.1 | 10.7 | 9.1 | 4 | 9.7 | 6.5 | 7.4 | 5.6 | 5 | |
| Liver | M | 35.8 | 24.4 | 24.0 | 16.4 | 2 | 33.3 | 21.2 | 20.9 | 14.9 | 2 | 38.3 | 27.8 | 27.3 | 17.8 | 2 |
| F | 13.3 | 7.9 | 7.8 | 10.0 | 3 | 12.3 | 6.7 | 6.7 | 8.8 | 4 | 14.3 | 9.2 | 9.1 | 11.3 | 3 | |
| B | 24.7 | 16.1 | 15.9 | 14.0 | 2 | 22.8 | 13.9 | 13.7 | 12.6 | 2 | 26.5 | 18.5 | 18.2 | 15.5 | 3 | |
| Pancreas | M | 6.9 | 4.6 | 4.5 | 3.2 | 6 | 8.7 | 5.2 | 5.2 | 3.9 | 6 | 5.4 | 3.8 | 3.8 | 2.5 | 6 |
| F | 5.6 | 3.2 | 3.1 | 4.2 | 7 | 7.0 | 3.7 | 3.6 | 5.0 | 6 | 4.2 | 2.6 | 2.6 | 3.3 | 7 | |
| B | 6.3 | 3.9 | 3.8 | 3.6 | 7 | 7.8 | 4.4 | 4.4 | 4.3 | 7 | 4.8 | 3.2 | 3.2 | 2.8 | 7 | |
| Lung | M | 62.9 | 40.7 | 40.6 | 28.7 | 1 | 67.8 | 40.5 | 40.4 | 30.3 | 1 | 58.1 | 40.8 | 40.6 | 27.1 | 1 |
| F | 30.5 | 17.6 | 17.3 | 23.1 | 1 | 32.9 | 17.4 | 17.1 | 23.7 | 1 | 28.1 | 17.8 | 17.6 | 22.4 | 1 | |
| B | 46.9 | 28.8 | 28.6 | 26.6 | 1 | 50.5 | 28.5 | 28.3 | 27.8 | 1 | 43.5 | 29.0 | 28.8 | 25.4 | 1 | |
| Breast | M | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| F | 10.1 | 6.6 | 6.4 | 7.6 | 5 | 11.9 | 7.2 | 7.0 | 8.6 | 5 | 8.2 | 5.8 | 5.6 | 6.5 | 6 | |
| B | 10.1 | 6.6 | 6.4 | 2.9 | 6 | 11.9 | 7.2 | 7.0 | 3.3 | 5 | 8.2 | 5.8 | 5.6 | 2.4 | 6 | |
| Ovary | M | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| F | 4.1 | 2.8 | 2.7 | 3.1 | 8 | 4.0 | 2.6 | 2.4 | 2.9 | 9 | 4.2 | 3.0 | 2.9 | 3.4 | ||
| B | 4.1 | 2.8 | 2.7 | 1.2 | 9 | 4.0 | 2.6 | 2.4 | 1.1 | 13 | 4.2 | 3.0 | 2.9 | 1.2 | 9 | |
| Cervix | M | - | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| F | 3.3 | 2.2 | 2.1 | 2.5 | 11 | 4.2 | 2.5 | 2.5 | 3.0 | 8 | 2.5 | 1.7 | 1.7 | 2.0 | 11 | |
| B | 3.3 | 2.2 | 2.1 | 0.9 | 13 | 4.2 | 2.5 | 2.5 | 1.2 | 10 | 2.5 | 1.7 | 1.7 | 0.7 | 12 | |
| Prostate | M | 4.0 | 2.4 | 2.4 | 1.8 | 10 | 5.7 | 2.9 | 3.0 | 2.5 | 7 | 2.4 | 1.6 | 1.6 | 1.1 | 10 |
| F | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| B | 4.0 | 2.3 | 2.4 | 1.2 | 11 | 5.7 | 2.9 | 3.0 | 1.6 | 8 | 2.4 | 1.6 | 1.6 | 0.7 | 13 | |
| Brain, nervous system | M | 4.7 | 3.5 | 3.5 | 2.1 | 7 | 4.4 | 3.1 | 3.1 | 2.0 | 10 | 5.0 | 3.9 | 3.8 | 2.3 | 7 |
| F | 3.9 | 2.7 | 2.6 | 2.9 | 9 | 3.8 | 2.5 | 2.5 | 2.7 | 10 | 3.9 | 2.9 | 2.8 | 3.1 | 9 | |
| B | 4.3 | 3.1 | 3.0 | 2.4 | 8 | 4.1 | 2.8 | 2.8 | 2.3 | 11 | 4.5 | 3.4 | 3.3 | 2.6 | 8 | |
| Lymphoma | M | 4.0 | 2.8 | 3.1 | 1.8 | 9 | 4.8 | 3.1 | 3.4 | 2.2 | 9 | 3.3 | 2.5 | 2.6 | 1.6 | 9 |
| F | 2.8 | 1.7 | 1.9 | 2.1 | 12 | 3.3 | 1.9 | 2.1 | 2.4 | 12 | 2.2 | 1.5 | 1.6 | 1.7 | 12 | |
| B | 3.4 | 2.2 | 2.5 | 2.0 | 12 | 4.1 | 2.5 | 2.8 | 2.2 | 12 | 2.7 | 1.9 | 2.1 | 1.6 | 11 | |
| Leukemia | M | 4.6 | 3.6 | 3.8 | 2.0 | 8 | 4.9 | 3.6 | 3.9 | 2.2 | 8 | 4.3 | 3.6 | 3.8 | 2.1 | 8 |
| F | 3.5 | 2.6 | 2.8 | 2.6 | 10 | 3.7 | 2.6 | 2.8 | 2.6 | 11 | 3.3 | 2.6 | 2.7 | 2.6 | 10 | |
| B | 4.0 | 3.1 | 3.3 | 2.3 | 10 | 4.3 | 3.1 | 3.3 | 2.4 | 9 | 3.8 | 3.1 | 3.3 | 2.2 | 10 | |
| R1 | Sex | All Areas | Urban Areas | Rural Areas | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Site | PR | SPR | R2 | Site | PR | SPR | R2 | Site | PR | SPR | R2 | ||
| 1 | M | Lung | 5.75 | 5.17 | 1 | Lung | 7.96 | 5.99 | 1 | Lung | 4.61 | 4.41 | 2 |
| F | Lung | 3.71 | 3.20 | 1 | Lung | 4.56 | 3.50 | 1 | Lung | 3.33 | 3.35 | 1 | |
| B | Lung | 4.95 | 4.26 | 1 | Lung | 6.47 | 4.94 | 1 | Lung | 4.27 | 4.07 | 1 | |
| 2 | M | Liver | 5.66 | 5.07 | 2 | Liver | 6.15 | 5.11 | 2 | Liver | 5.45 | 5.20 | 1 |
| F | Stomach | 1.86 | 1.63 | 4 | Colorectal | 1.94 | 1.52 | 5 | Stomach | 1.78 | 1.72 | 4 | |
| B | Liver | 4.00 | 3.57 | 2 | Liver | 2.61 | 2.20 | 2 | Stomach | 2.48 | 2.37 | 3 | |
| 3 | M | Stomach | 3.02 | 2.73 | 3 | Stomach | 3.52 | 2.68 | 3 | Stomach | 2.76 | 2.64 | 3 |
| F | Liver | 1.91 | 1.68 | 3 | Stomach | 2.06 | 1.67 | 3 | Liver | 1.98 | 1.94 | 2 | |
| B | Stomach | 2.57 | 2.23 | 3 | Stomach | 1.78 | 1.42 | 3 | Liver | 4.06 | 3.87 | 2 | |
| 4 | M | Esophageal | 2.11 | 1.88 | 4 | Colorectal | 2.11 | 1.67 | 5 | Esophagus | 2.04 | 1.95 | 4 |
| F | Colorectal | 1.34 | 1.17 | 5 | Liver | 1.95 | 1.55 | 4 | Esophageal | 1.14 | 1.22 | 5 | |
| B | Esophageal | 1.63 | 1.38 | 6 | Colorectal | 1.26 | 1.01 | 5 | Esophageal | 1.75 | 1.67 | 4 | |
| 5 | M | Colorectal | 1.37 | 1.24 | 5 | Esophageal | 2.18 | 1.63 | 4 | Colorectal | 0.97 | 0.93 | 6 |
| F | Breast | 2.14 | 1.93 | 2 | Breast | 2.69 | 2.28 | 2 | Colorectal | 1.00 | 1.00 | 6 | |
| B | Colorectal | 1.83 | 1.60 | 5 | Breast | 1.53 | 1.33 | 4 | Colorectal | 1.01 | 0.96 | 6 | |
| 6 | M | Pancreas | 0.70 | 0.63 | 8 | Pancreas | 1.12 | 0.85 | 6 | Pancreas | 0.47 | 0.44 | 8 |
| F | Esophagus | 0.94 | 0.79 | 6 | Pancreas | 0.93 | 0.70 | 8 | Breast | 1.78 | 1.66 | 3 | |
| B | Breast | 1.88 | 1.70 | 4 | Esophageal | 0.91 | 0.69 | 6 | Breast | 1.58 | 1.50 | 5 | |
| 7 | M | Brain | 0.89 | 0.85 | 7 | Prostate | 0.24 | 0.17 | 10 | Brain | 0.87 | 0.86 | 7 |
| F | Pancreas | 0.62 | 0.53 | 10 | Esophageal | 0.69 | 0.51 | 10 | Pancreas | 0.45 | 0.46 | 10 | |
| B | Pancreas | 0.67 | 0.57 | 10 | Pancreas | 0.63 | 0.49 | 8 | Pancreas | 0.47 | 0.45 | 10 | |
| 8 | M | Leukemia | 1.01 | 0.99 | 6 | Leukemia | 1.08 | 1.04 | 7 | Leukemia | 0.99 | 0.99 | 5 |
| F | Cervix | 0.93 | 0.85 | 7 | Ovary | 0.94 | 0.78 | 7 | Cervix | 0.86 | 0.81 | 8 | |
| B | Brain | 0.84 | 0.81 | 8 | Prostate | 0.22 | 0.15 | 10 | Brain | 0.85 | 0.84 | 8 | |
| 9 | M | Lymphoma | 0.54 | 0.47 | 9 | Lymphoma | 0.73 | 0.63 | 9 | Lymphoma | 0.44 | 0.43 | 9 |
| F | Brain | 0.80 | 0.76 | 9 | Cervix | 1.04 | 0.92 | 6 | Brain | 0.81 | 0.79 | 9 | |
| B | Cervix | 0.82 | 0.75 | 9 | Leukemia | 0.72 | 0.71 | 7 | Cervix | 0.75 | 0.72 | 9 | |
| 10 | M | Prostate | 0.11 | 0.10 | 10 | Brain | 0.94 | 0.85 | 8 | Prostate | 0.07 | 0.06 | 10 |
| F | Leukemia | 0.90 | 0.89 | 8 | Brain | 0.84 | 0.75 | 9 | Leukemia | 0.88 | 0.87 | 7 | |
| B | Leukemia | 0.95 | 0.91 | 7 | Ovary | 0.53 | 0.45 | 9 | Leukemia | 0.95 | 0.96 | 7 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, Y.; Chen, Y.; Jia, H.; Liu, J.; Ding, Y.; Wang, H.; Hu, Y.; Ma, J.; Zhang, X.; Li, S. Patterns of Life Lost to Cancers with High Risk of Death in China. Int. J. Environ. Res. Public Health 2019, 16, 2175. https://doi.org/10.3390/ijerph16122175
Yan Y, Chen Y, Jia H, Liu J, Ding Y, Wang H, Hu Y, Ma J, Zhang X, Li S. Patterns of Life Lost to Cancers with High Risk of Death in China. International Journal of Environmental Research and Public Health. 2019; 16(12):2175. https://doi.org/10.3390/ijerph16122175
Chicago/Turabian StyleYan, Yizhong, Yu Chen, Huaimiao Jia, Jiaming Liu, Yusong Ding, Haixia Wang, Yunhua Hu, Jiaolong Ma, Xianghui Zhang, and Shugang Li. 2019. "Patterns of Life Lost to Cancers with High Risk of Death in China" International Journal of Environmental Research and Public Health 16, no. 12: 2175. https://doi.org/10.3390/ijerph16122175