Association between the First Occurrence of Asthma and Residential Greenness in Children and Teenagers in Taiwan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Inclusion
2.2. Greenness Exposure
2.3. Air Pollution Monitoring Data
2.4. Data Management and Analysis
3. Results
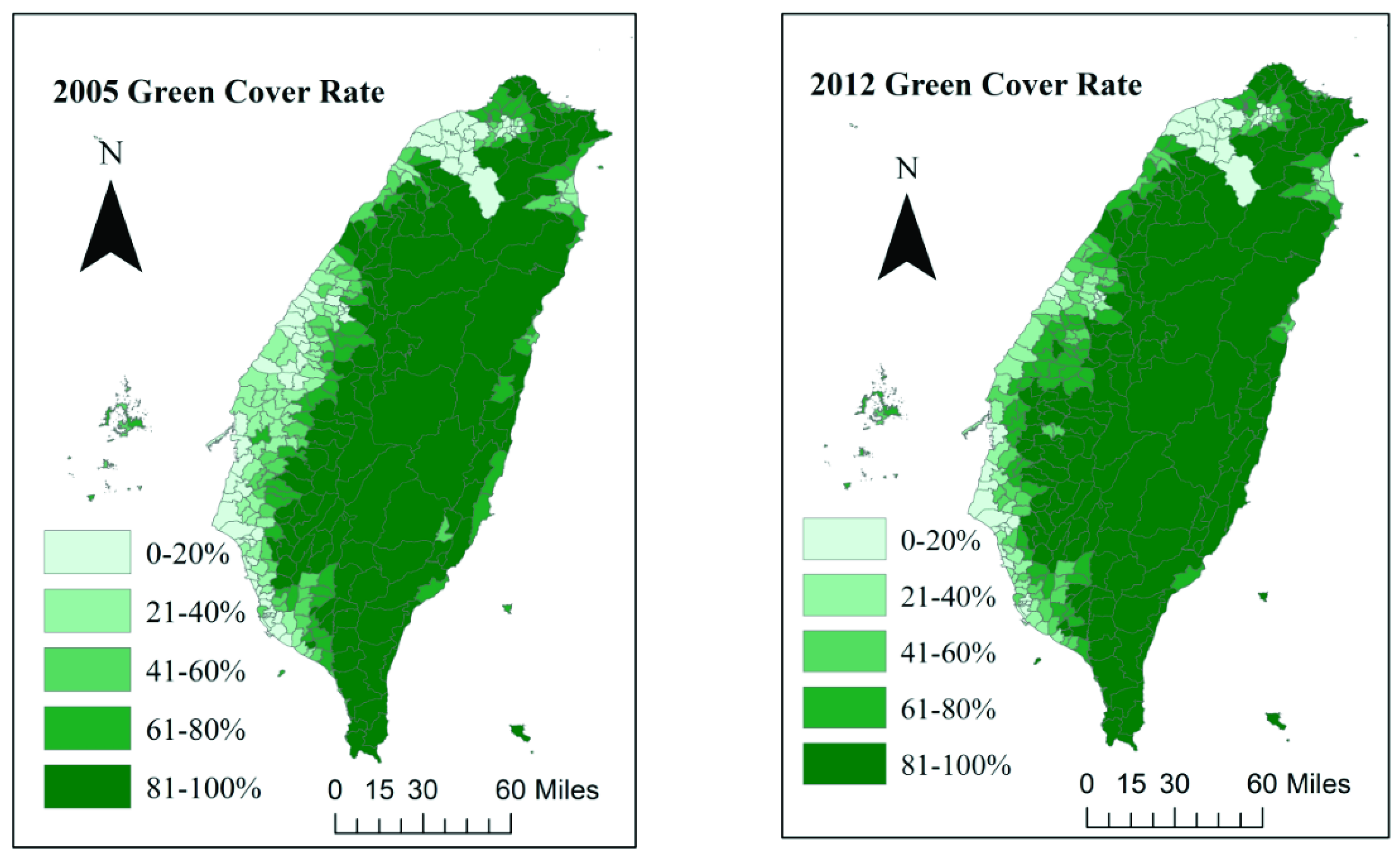
3.1. Green Coverage Change in Taiwan in the Past Decade
3.2. Characteristics of Asthma Cases and Controls
3.3. The Relationship Between Greenness Exposure and Asthma Incidence Before the Age of 18
3.4. The Relationship Between Greenness Exposure and Asthma Incidence in Preschool Children
3.5. The Relationship Between Greenness Exposure and Asthma Incidence in Subjects 6 to 17 Years Old
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ying, Y.H.; Weng, Y.C.; Chang, K. The Prevalence and Patient’s Quality of Life for Asthma in Taiwan. Int. J. Pul. Res. Sci. 2017, 1, 1–5. [Google Scholar]
- Gautier, C.; Charpin, D. Environmental triggers and avoidance in the management of asthma. J. Asthma Allergy 2017, 10, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.L.; Lin, Y.C.; Sung, F.C.; Huang, S.L.; Ko, Y.C.; Lai, J.S.; Su, H.J.; Shaw, C.K.; Lin, R.S.; Dockery, D.W. Climate, traffic-related air pollutants, and asthma prevalence in middle-school children in taiwan. Environ. Health Perspect. 1999, 107, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Studnicka, M.; Hackl, E.; Pischinger, J.; Fangmeyer, C.; Haschke, N.; Kuhr, J.; Urbanek, R.; Neumann, M.; Frischer, T. Traffic-related NO2 and the prevalence of asthma and respiratory symptoms in seven year olds. Eur. Respir. J. 1997, 10, 2275–2278. [Google Scholar] [CrossRef] [PubMed]
- Pennington, A.F.; Strickland, M.J.; Klein, M.; Zhai, X.; Bates, J.T.; Drews-Botsch, C.; Hansen, C.; Russell, A.G.; Tolbert, P.E.; Darrow, L.A. Exposure to Mobile Source Air Pollution in Early-life and Childhood Asthma Incidence: The Kaiser Air Pollution and Pediatric Asthma Study. Epidemiology (Camb. Mass.) 2018, 29, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagana, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and benefits of green spaces for children: A cross-sectional study of associations with sedentary behavior, obesity, asthma, and allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef]
- Fuertes, E.; Markevych, I.; Bowatte, G.; Gruzieva, O.; Gehring, U.; Becker, A.; Berdel, D.; von Berg, A.; Bergstrom, A.; Brauer, M.; et al. Residential greenness is differentially associated with childhood allergic rhinitis and aeroallergen sensitization in seven birth cohorts. Allergy 2016, 71, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Lovasi, G.S.; O’Neil-Dunne, J.P.; Lu, J.W.; Sheehan, D.; Perzanowski, M.S.; Macfaden, S.W.; King, K.L.; Matte, T.; Miller, R.L.; Hoepner, L.A.; et al. Urban tree canopy and asthma, wheeze, rhinitis, and allergic sensitization to tree pollen in a New York City birth cohort. Environ. Health Perspect. 2013, 121, 494–500. [Google Scholar] [CrossRef]
- Andrusaityte, S.; Grazuleviciene, R.; Kudzyte, J.; Bernotiene, A.; Dedele, A.; Nieuwenhuijsen, M.J. Associations between neighbourhood greenness and asthma in preschool children in Kaunas, Lithuania: A case-control study. BMJ Open 2016, 6, e010341. [Google Scholar] [CrossRef]
- Sbihi, H.; Tamburic, L.; Koehoorn, M.; Brauer, M. Greenness and Incident Childhood Asthma: A 10-Year Follow-up in a Population-based Birth Cohort. Am. J. Respir. Crit. Care Med. 2015, 192, 1131–1133. [Google Scholar] [CrossRef] [PubMed]
- Eldeirawi, K.; Kunzweiler, C.; Zenk, S.; Finn, P.; Nyenhuis, S.; Rosenberg, N.; Persky, V. Associations of urban greenness with asthma and respiratory symptoms in Mexican American children. Ann. Allergy Asthma Immunol. 2019, 122, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Sbihi, H.; Koehoorn, M.; Tamburic, L.; Brauer, M. Asthma Trajectories in a Population-based Birth Cohort. Impacts of Air Pollution and Greenness. Am. J. Respir. Crit. Care Med. 2017, 195, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.H.; Chen, V.Y.J.; Wen, T.H. Revisiting the role of rainfall variability and its interactive effects with the built environment in urban dengue outbreaks. J. Appl. Geogr. 2018, 101, 14–22. [Google Scholar] [CrossRef]
- Lin, M.H.; Yang, A.C.; Wen, T.H. Using Regional Differences and Demographic Characteristics to Evaluate the Principles of Estimation of the Residence of the Population in National Health Insurance Research Databases (NHIRD). Taiwan J. Public Health 2011, 30, 347–361. [Google Scholar]
- Iwashita, K.; Kawasaki, H.; Sawada, M.; In, M.; Mataki, Y.; Kuwabara, T. Shortening of the induction period of allergic asthma in cynomolgus monkeys by Ascaris suum and house dust mite. J. Pharmacol. Sci. 2008, 106, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Oliveira, S.; Andrade, H.; Vaz, T. The cooling effect of green spaces as a contribution to the mitigation of urban heat: A case study in Lisbon. J. Build. Environ. 2011, 46, 2186–2194. [Google Scholar] [CrossRef]
- Pilat, M.A.; McFarland, A.; Snelgrove, A.; Collins, K.; Waliczek, T.M.; Zajicek, J.J.H. The effect of tree cover and vegetation on incidence of childhood asthma in metropolitan statistical areas of Texas. J. Horttechnol. 2012, 22, 631–637. [Google Scholar] [CrossRef]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.J.; Wakayama, Y.; et al. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost. Agents 2008, 22, 45–55. [Google Scholar]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Makela, M.J.; et al. Environmental biodiversity, human microbiota, and allergy are interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rook, G.A. Regulation of the immune system by biodiversity from the natural environment: An ecosystem service essential to health. J. Proc. Natl. Acad. Sci. 2013, 110, 18360–18367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luyt, D.K.; Burton, P.R.; Simpson, H. Epidemiological study of wheeze, doctor diagnosed asthma, and cough in preschool children in Leicestershire. BMJ (Clin. Res. Ed.) 1993, 306, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Zein, J.G.; Erzurum, S.C. Asthma is Different in Women. Curr. Allergy Asthma Rep. 2015, 15, 28. [Google Scholar] [CrossRef] [PubMed]
- Cariñanos, P.; Casares-Porcel, M. Urban green zones and related pollen allergy: A review. Some guidelines for designing spaces with low allergy impact. J. Landsc. Urban. Plan. 2011, 101, 205–214. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Non-Asthma (N = 3520) | Asthma (N = 3520) | p-Value |
|---|---|---|---|
| N (%) | |||
| Age | 1.0000 | ||
| 0–5 | 2531 (71.9) | 2531 (71.9) | |
| 6–18 | 989 (28.1) | 989 (28.1) | |
| Gender | 1.0000 | ||
| Male | 2007 (57.0) | 2007 (57.0) | |
| Female | 1513 (43.0) | 1513 (43.0) | |
| Greenness | 0.0367 | ||
| 0–20% | 855 (24.3) | 842 (23.9) | |
| 21–40% | 961 (27.3) | 1031 (29.3) | |
| 41–60% | 815 (23.2) | 745 (21.2) | |
| 61–80% | 555 (15.8) | 606 (17.2) | |
| 81–100% | 334 (9.5) | 296 (8.4) | |
| Urbanization | <0.0001 | ||
| 1 (Most urbanized) | 738 (21.0) | 1030 (29.3) | |
| 2 | 2359 (67.0) | 2228 (63.3) | |
| 3 | 346 (9.8) | 225 (6.4) | |
| 4 (Least urbanized) | 77 (2.2) | 37 (1.0) | |
| Frequency of visits to healthcare providers | <0.0001 | ||
| ≤15 times/year | 1558 (44.3) | 668 (19.0) | |
| 16–44 times/year | 1274 (36.2) | 1350 (38.4) | |
| 45–60 times/year | 502 (14.2) | 968 (27.5) | |
| >60 times/year | 186 (5.3) | 534 (15.1) | |
| Mean family income of townships | <0.0001 | ||
| <794,000 NTD | 1020 (29.0) | 772 (21.9) | |
| 794,000–862,000 NTD | 935 (26.6) | 802 (22.8) | |
| 862,000–989,000 NTD | 637 (18.1) | 774 (22.0) | |
| >989,000 NTD | 928 (26.4) | 1172 (33.3) | |
| Greenness Exposure | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| 0–20% | Reference | Reference | ||
| 21–40% | 1.17 (1.06–1.30) | 0.0027 | 1.17 (1.06–1.30) | 0.0027 |
| 41–60% | 1.28 (1.12–1.46) | 0.0003 | 1.28 (1.12–1.46) | 0.0002 |
| 61–80% | 1.32 (1.13–1.53) | 0.0003 | 1.34 (1.15–1.56) | 0.0002 |
| 81–100% | 1.09 (0.91–1.31) | 0.3674 | 1.10 (0.92–1.32) | 0.3142 |
| p for trend | 0.0393 | 0.0289 | ||
| Males | ||||
| 0–20% | Reference | Reference | ||
| 21–40% | 1.19 (1.04–1.37) | 0.0128 | 1.19 (1.04–1.37) | 0.0137 |
| 41–60% | 1.27 (1.06–1.51) | 0.0081 | 1.26 (1.06–1.50) | 0.0085 |
| 61–80% | 1.35 (1.10–1.64) | 0.0032 | 1.35 (1.11–1.65) | 0.0029 |
| 81–100% | 1.12 (0.88–1.43) | 0.3563 | 1.12 (0.88–1.43) | 0.3439 |
| p for trend | 0.0742 | 0.0750 | ||
| Females | ||||
| 0–20% | Reference | Reference | ||
| 21–40% | 1.14 (0.97–1.34) | 0.1021 | 1.15 (0.98–1.35) | 0.0936 |
| 41–60% | 1.28 (1.05–1.57) | 0.0156 | 1.30 (1.06–1.58) | 0.0102 |
| 61–80% | 1.28 (1.02–1.62) | 0.0371 | 1.32 (1.04–1.67) | 0.0213 |
| 81–100% | 1.05 (0.79–1.39) | 0.7491 | 1.07 (0.81–1.41) | 0.6433 |
| p for trend | 0.2702 | 0.1915 | ||
| Greenness Exposure | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| 0–20% | Reference | Reference | ||
| 21–40% | 1.18 (1.04–1.33) | 0.0106 | 1.18 (1.04–1.33) | 0.0107 |
| 41–60% | 1.28 (1.10–1.50) | 0.0017 | 1.29 (1.11–1.50) | 0.0012 |
| 61–80% | 1.31 (1.10–1.57) | 0.0031 | 1.33 (1.11–1.60) | 0.0017 |
| 81–100% | 1.07 (0.86–1.33) | 0.5464 | 1.09 (0.88–1.34) | 0.4470 |
| p for trend | 0.1180 | 0.0828 | ||
| Greenness Exposure | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| 0–20% | Reference | Reference | ||
| 21–40% | 1.17 (0.96–1.43) | 0.1226 | 1.17 (0.96–1.43) | 0.1314 |
| 41–60% | 1.25 (0.97–1.62) | 0.0840 | 1.24 (0.96–1.60) | 0.0946 |
| 61–80% | 1.36 (1.02–1.81) | 0.0344 | 1.36 (1.03–1.81) | 0.0332 |
| 81–100% | 1.17 (0.82–1.67) | 0.3963 | 1.15 (0.81–1.64) | 0.4315 |
| p for trend | 0.1309 | 0.1442 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, C.-J.; Yu, P.-Y.; Tai, C.-J.; Jan, R.-H.; Wen, T.-H.; Lin, S.-W.; Tseng, C.-C. Association between the First Occurrence of Asthma and Residential Greenness in Children and Teenagers in Taiwan. Int. J. Environ. Res. Public Health 2019, 16, 2076. https://doi.org/10.3390/ijerph16122076
Hsieh C-J, Yu P-Y, Tai C-J, Jan R-H, Wen T-H, Lin S-W, Tseng C-C. Association between the First Occurrence of Asthma and Residential Greenness in Children and Teenagers in Taiwan. International Journal of Environmental Research and Public Health. 2019; 16(12):2076. https://doi.org/10.3390/ijerph16122076
Chicago/Turabian StyleHsieh, Chia-Jung, Pei-Ying Yu, Chun-Ju Tai, Rong-Hwa Jan, Tzai-Hung Wen, Shyang-Woei Lin, and Chun-Chieh Tseng. 2019. "Association between the First Occurrence of Asthma and Residential Greenness in Children and Teenagers in Taiwan" International Journal of Environmental Research and Public Health 16, no. 12: 2076. https://doi.org/10.3390/ijerph16122076