Metabolic Outcomes in Southern Italian Preadolescents Residing Near an Industrial Complex: The Role of Residential Location and Socioeconomic Status

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Design and Enrollment
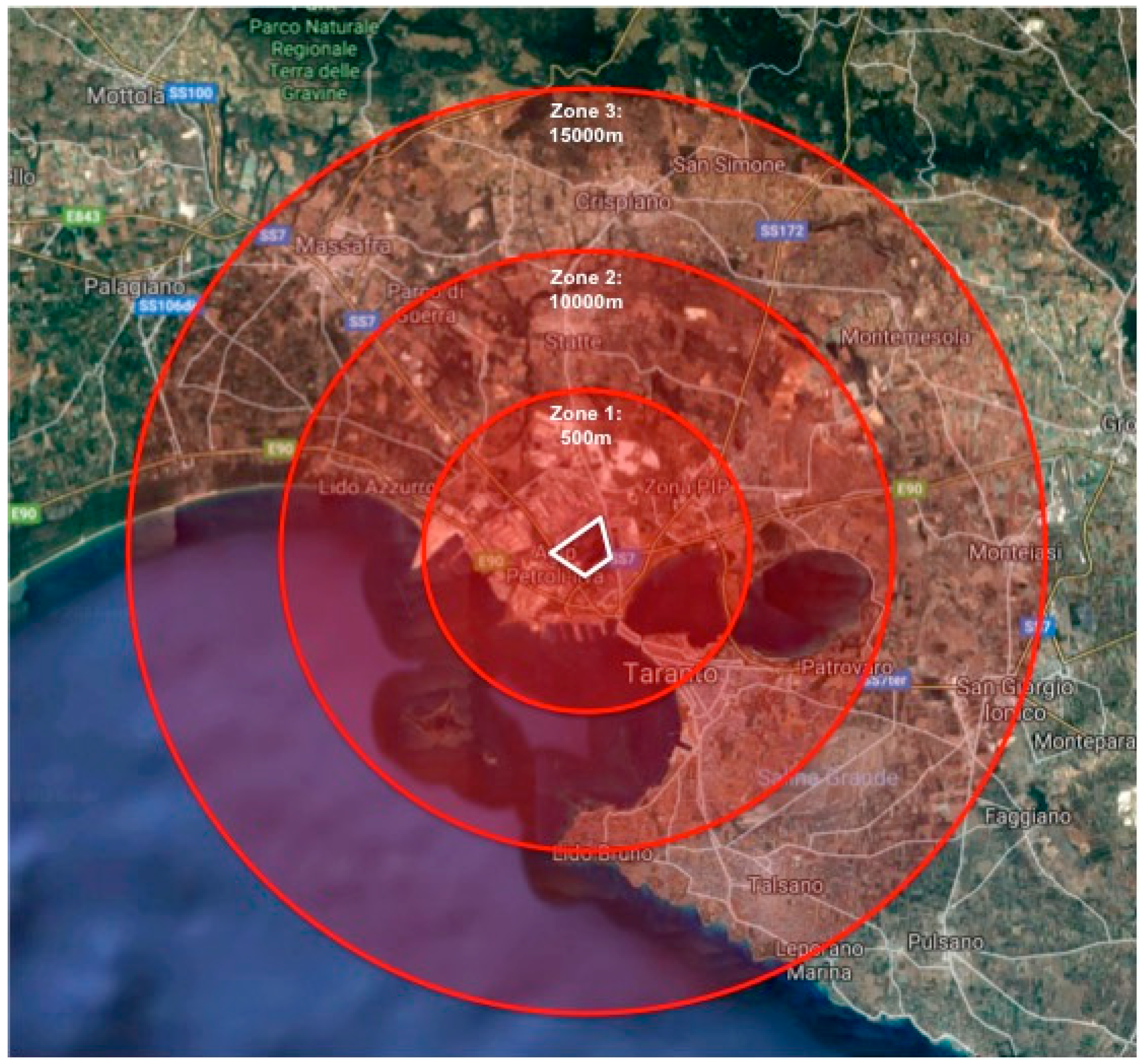
2.3. Division of Residential Location into Residential Zones
2.4. Collection and Analysis of Fasting Blood Glucose Data
2.5. Collection of BMI Z-Score, SES, and Lifestyle Data
2.6. Determination of BMI Z-Score
2.7. Determination of SES
2.8. Statistical Analysis
3. Results
3.1. Sociodemographic and Physical Characteristics of the Cohort
3.2. FBG by Sociodemographic Factors
3.3. BMI Z-Scores and Clinical Subgroups by Sociodemographic Factors
4. Discussion
4.1. Fasting Blood Glucose Concentration by Sociodemographic Factors
4.2. BMI Z-Scores and Clinical Subgroups by Sociodemographic Factors
4.3. Implications
4.4. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hanna-Attisha, M.; LaChance, J.; Sadler, R.C.; Champney Schnepp, A. Elevated blood lead levels in children associated with the Flint drinking water crisis: A spatial analysis of risk and public health response. Am. J. Pub. Health 2016, 106, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.B.; Im, M.H.; Kim, J.W.; Park, E.J.; Shin, M.S.; Kim, B.N.; Yoo, H.J.; Cho, I.H.; Bhang, S.Y.; Hong, Y.C.; et al. Environmental lead exposure and attention deficit/ hyperactivity disorder symptom domains in a community sample of South Korean school-age children. Environ. Health Perspect. 2015, 123, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; McConnell, R.; Wolch, J.; Chang, R.; Lam, C.; Dunton, G.; Gilliland, F.; Lurmann, F.; Islam, T.; Berhane, K. Traffic-related air pollution and obesity formation in children: A longitudinal, multilevel analysis. Environ. Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, F.L.; Spinelli, A.; Lazzeri, G.; Lamberti, A.; Mazzarella, G.; Nardone, P.; Pilato, V.; Buoncristiano, M.; Caroli, M. Severe obesity prevalence in 8-to 9-year-old Italian children: A large population-based study. Eur. J. Clin. Nutr. 2015, 69, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; De Donno, A.; Bagordo, F.; Serio, F.; Piscitelli, P.; Ceretti, E.; Zani, C.; Viola, G.; Villarini, M.; Moretti, M.; et al. Socio-Economic and environmental factors associated with overweight and obesity in children aged 6–8 years living in five Italian cities (the MAPEC_LIFE cohort). Int. J. Environ. Res. Public Health 2016, 13, 1002. [Google Scholar] [CrossRef] [PubMed]
- Olaya, B.; Moneta, M.V.; Pez, O.; Bitfoi, A.; Carta, M.G.; Eke, C.; Goelitz, D.; Keyes, K.M.; Kuijpers, R.; Lesinskiene, S.; et al. Country-level and individual correlates of overweight and obesity among primary school children: A cross-sectional study in seven European countries. Bmc Pub. Health 2015, 15, 475. [Google Scholar] [CrossRef]
- Silano, M.; Agostoni, C.; Fattore, G. Italy’s unsolved childhood obesity crisis. Arch. Dis Child. 2019, 104, 202–203. [Google Scholar] [CrossRef]
- Parrino, C.; Vinciguerra, F.; La Spina, N.; Romeo, L.; Tumminia, A.; Baratta, R.; Squatrito, S.; Vigneri, R.; Frittitta, L. Influence of early-life and parental factors on childhood overweight and obesity. J. Endocrinol. Investig. 2016, 39, 1315–1321. [Google Scholar] [CrossRef]
- Lazzeri, G.; Dalmasso, P.; Berchialla, P.; Borraccino, A.; Charrier, L.; Giacchi, M.V.; Simi, R.; Lenzi, M.; Vieno, A.; Lemma, P.; et al. Trends in adolescent overweight prevalence in Italy according to socioeconomic position. Ann. Ist. Super Sanità. 2017, 53, 283–290. [Google Scholar]
- Lazzeri, G.; Pammolli, A.; Simi, R.; Pilato, V.; Giacchi, M.V. BMI from nutritional surveillance of 8-9 years old children in Tuscany (Italy). J. Prev. Med. Hyg. 2011, 52, 181–185. [Google Scholar]
- Cortese, S.; Moreira-Maia, C.R.; St. Fleur, D.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association between ADHD and obesity: A systematic review and meta-analysis. Am. J. Psychiatry 2015, 173, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Sfera, A.; Osorio, C.; Inderias, L.A.; Parker, V.; Price, A.I.; Cummings, M. The obesity–impulsivity axis: Potential metabolic interventions in chronic psychiatric patients. Front. Psychiatry 2017, 13, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Janesick, A.S.; Blumberg, B. Obesogens: An emerging threat to public health. Am. J. Obs. Gynecol. 2016, 214, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Goldman, L.R. Children’s vulnerability to toxic chemicals: A challenge and opportunity to strengthen health and environmental policy. Health Aff. 2011, 30, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Lanzinger, S.; Rosenbauer, J.; Sugiri, D.; Schikowski, T.; Treiber, B.; Klee, D.; Holl, R.W. Impact of long-term air pollution exposure on metabolic control in children and adolescents with type 1 diabetes: Results from the DPV registry. Diabetologia 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Samarghandian, S.; Azimi-Nezhad, M. The role of arsenic in obesity and diabetes. J. Cell Physiol. 2019. [Google Scholar] [CrossRef]
- Bradley, R.H.; Caldwell, B.M.; Rock, S.L.; Hamrick, H.M.; Harris, P. Home Observation for Measurement of the Environment: Development of a Home Inventory for use with families having children 6 to 10 years old. Contemp. Educ. Psychol. 1988, 13, 58–71. [Google Scholar] [CrossRef]
- Weden, M.M.; Brownell, P.B.; Rendall, M.S.; Lau, C.; Fernandes, M.; Nazarov, Z. Parent-reported height and weight as sources of bias in survey estimates of childhood obesity. Am. J. Epidemiol. 2013, 178, 461–473. [Google Scholar] [CrossRef]
- Garcia-Marcos, L.; Valverde-Molina, J.; Sanchez-Solis, M.; Soriano-Pérez, M.J.; Baeza-Alcaraz, A.; Martinez-Torres, A.; Perez-Fernandez, V.; Guillen-Perez, J.J. Validity of parent-reported height and weight for defining obesity among asthmatic and nonasthmatic schoolchildren. Int. Arch. Allergy Immunol. 2006, 139, 139–145. [Google Scholar] [CrossRef]
- Butte, N.F.; Garza, C.; De Onis, M. Feasibility of international growth standards for school-aged children and adolescents. J. Nutr. 2007, 137, 153–157. [Google Scholar] [CrossRef]
- De Onis, M.; Lobstein, T. Defining obesity risk in childhood population: Which cut-offs should we use? Int. J. Ped. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Cesana, G.C.; Ferrario, M.; De, G.V.; Sega, R.; Grieco, A. Evaluation of the socioeconomic status in epidemiological surveys: Hypotheses of research in the Brianza area MONICA project. Med. Lav. 1995, 86, 16–26. [Google Scholar]
- Wood, S.N. Fast stable restricted maximum likelihood and marginal likelihood estimation of semiparametric generalized linear models. J. R Stat. Soc. Ser. B Stat. Methodol. 2011, 73, 3–36. [Google Scholar] [CrossRef]
- Team, R. Core. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Rudesill, C.L.; Henderson, R.A. Normal blood sugar values in children. Am. J. Dis. Child. 1941, 61, 108–115. [Google Scholar] [CrossRef]
- González-Villalva, A.; Colín-Barenque, L.; Bizarro-Nevares, P.; Rojas-Lemus, M.; Rodríguez-Lara, V.; García-Pelaez, I.; Ustarroz-Cano, M.; López-Valdez, N.; Albarrán-Alonso, J.C.; Fortoul, T.I. Pollution by metals: Is there a relationship in glycemic control? Environ. Toxicol. Pharm. 2016, 46, 337–343. [Google Scholar] [CrossRef]
- Neisi, A.; Goudarzi, G.; Akbar Babaei, A.; Vosoughi, M.; Hashemzadeh, H.; Naimabadi, A.; Mohammadi, M.J.; Hashemzadeh, B. Study of heavy metal levels in indoor dust and their health risk assessment in children of Ahvaz city, Iran. Toxin. Rev. 2016, 35, 16–23. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Bitto, A.; Pallio, G.; Mannino, F.; Arcoraci, V.; Aliquò, F.; Minutoli, L.; de Ponte, C.; D’andrea, P.; et al. Cadmium-induced oxidative stress impairs glycemic control in adolescents. Oxid. Med. Cell Longev. 2017, 2017, 6341671. [Google Scholar] [CrossRef]
- Dunea, D.; Iordache, S.; Liu, H.Y.; Bøhler, T.; Pohoata, A.; Radulescu, C. Quantifying the impact of PM2.5 and associated heavy metals on respiratory health of children near metallurgical facilities. Environ. Sci. Poll. Res. 2016, 23, 15395–15406. [Google Scholar] [CrossRef]
- Dong, G.H.; Chen, T.; Liu, M.M.; Wang, D.; Ma, Y.N.; Ren, W.H.; Lee, Y.L.; Zhao, Y.D.; He, Q.C. Gender differences and effect of air pollution on asthma in children with and without allergic predisposition: Northeast Chinese children health study. PLoS ONE 2017, 6, e22470. [Google Scholar] [CrossRef]
- Liu, M.M.; Wang, D.; Zhao, Y.; Liu, Y.Q.; Huang, M.M.; Liu, Y.; Sun, J.; Ren, W.H.; Zhao, Y.D.; He, Q.C.; et al. Effects of outdoor and indoor air pollution on respiratory health of Chinese children from 50 kindergartens. J. Epidemiol. 2013, 23, 280–287. [Google Scholar] [CrossRef]
- Alderete, T.L.; Habre, R.; Toledo-Corral, C.M.; Berhane, K.; Chen, Z.; Lurmann, F.W.; Weigensberg, M.J.; Goran, M.I.; Gilliland, F.D. Longitudinal associations between ambient air pollution with insulin sensitive, beat-cell function, and adiposity in Los Angeles Latino children. Diabetes 2017, 66, 1989–1996. [Google Scholar] [CrossRef]
- Frederick, C.B.; Snellman, K.; Putnam, R.D. Increasing socioeconomic disparities in adolescent obesity. PNAS 2014, 111, 1338–1342. [Google Scholar] [CrossRef] [Green Version]
- Chung, A.; Backholer, K.; Wong, E.; Palermo, C.; Keating, C.; Peeters, A. Trends in child and adolescent obesity prevalence in economically advanced countries according to socioeconomic position: A systematic review. Obes. Rev. 2016, 17, 276–295. [Google Scholar] [CrossRef]
- Walsh, B.; Cullinan, J. Decomposing socioeconomic inequalities in childhood obesity: Evidence from Ireland. Econ. Hum. Biol. 2015, 16, 60–72. [Google Scholar] [CrossRef]
- Suglia, S.F.; Shelton, R.C.; Hsiao, A.; Wang, Y.C.; Rundle, A.; Link, B.G. Why the neighborhood social environment is critical in obesity prevention. J. Urban. Health 2016, 93, 206–212. [Google Scholar] [CrossRef]
- Sullivan, S.M.; Peters, E.S.; Trapido, E.J.; Oral, E.; Scribner, R.A.; Rung, A.L. Neighborhood environment measurements and anthropometric indicators of obesity: Results from the Women and Their Children’s Health (WaTCH) study. Environ. Behav. 2018, 50, 1032–1055. [Google Scholar] [CrossRef]
- Van der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The relationship between health, education, and health literacy: Results from the Dutch adult literacy and life skills survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef]
- Lauria, L.; Spinelli, A.; Buoncristiano, M.; Nardone, P. Decline of childhood overweight and obesity in Italy from 2008 to 2016: Results from 5 rounds of the population-based surveillance system. Bmc Public Health 2019, 19, 618. [Google Scholar] [CrossRef]
- Schrempft, S.; van Jaarsveld, C.H.; Fisher, A.; Herle, M.; Smith, A.D.; Fildes, A.; Llewellyn, C.H. Variation in the Heritability of Child Body Mass Index by Obesogenic Home Environment. Jama Pediatr. 2018. Advance online publication. [Google Scholar] [CrossRef]
- Faith, M.S.; Epstein, L.H. Healthy homes and obesogenic genes in young children: Rigorous behavioral theory and measurement and the detection of gene-environment interactions. Jama Pediatr. 2018, 172, 1121–1122. [Google Scholar] [CrossRef]
- National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: The evidence report. Obes. Res. 1998, 6, 51S–210S. [Google Scholar]
- Lucas, E.L.; Bertrand, P.; Guazzetti, S.; Donna, F.; Peli, M.; Jursa, T.P.; Lucchini, R.; Smith, D.R. Impact of ferromanganese alloy plants on household dust manganese levels: Implications for childhood exposure. Environ. Res. 2015, 138, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Diez Roux, A.V.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar] [CrossRef] [Green Version]
- Christian, H.; Zubrick, S.R.; Foster, S.; Giles-Corti, B.; Bull, F.; Wood, L.; Knuiman, M.; Brinkman, S.; Houghton, S.; Boruff, B. The influence of the neighborhood physical environment on early child health and development: A review and call for research. Health Place 2015, 33, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Barlow, S.E.; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, S164–S192. [Google Scholar] [CrossRef]
- Società Italiana di Pediatria. Società Italiana di Endocrinologia e Diabetologia; Consensus su diagnosi, trattamento e prevenzione dell’obesità del bambino e dell’adolescente: Rome, Italy, 2017. [Google Scholar]
- Pavilonis, B.T.; Lioy, P.J.; Guazzetti, S.; Bostick, B.C.; Donna, F.; Peli, M.; Zimmerman, N.J.; Bertrand, P.; Lucas, E.; Georgopoulos, P.G. Manganese concentrations in soil and settled dust in an area with historic ferroalloy production. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 443–450. [Google Scholar] [CrossRef]
- Lucchini, R.; Placidi, D.; Cagna, G.; Fedrighi, C.; Oppini, M.; Peli, M.; Zoni, S. Manganese and developmental neurotoxicity. In Neurotoxicity of Metals; Aschner, M., Costa, L.G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 13–34. [Google Scholar]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Relationship between lifestyle behaviors and obesity in children ages 9–11: Results from a 12-country study. Obesity 2015, 23, 1696–1702. [Google Scholar] [CrossRef]
- Li, X.M.; Ma, Y.T.; Xie, X.; Yang, Y.N.; Zheng, Y.Y. Relationship between serum creatinine and obesity in children in Xinjiang, China. Genet. Mol. Res. 2014, 13, 2409–2416. [Google Scholar] [CrossRef]
- Protano, C.; Andreoli, R.; Manini, P.; Vitali, M. Urinary trans, trans-muconic acid and S-phenylmercapturic acid are indicative of exposure to urban benzene pollution during childhood. Sci. Total Environ. 2012, 435–436, 115–123. [Google Scholar] [CrossRef]


{kind=link}
| Residential Zone | Radial Distance from Industrial Complex (km) | Neighborhoods | Primary Schools |
|---|---|---|---|
| 1 | 0.000–4.999 | Tamburi, Città Vecchia, Borgo | Vico, Deledda, Giusti, XXV Luglio |
| 2 | 5.000–9.999 | Italia Montegranaro, Tre Carrare Battisti, Solito Corvisea, Salinella, Paolo VI, Comune di Statte | Alfieri, Viola, Pertini, Giovanni XXIII |
| 3 | 10.000–15.000 | Talsano-San Vito-Lama | Frascolla, Salvemini, Sciascia, De Amicis |
| Measured Characteristic | Total (n = 214) | Zone 1 (n = 62) | Zone 2 (n = 77) | Zone 3 (n = 75) | Females (n = 114) | Males (n = 100) |
|---|---|---|---|---|---|---|
| Sex (F) | 114 (53.3%) | 39 (62.9%) | 38 (49.4%) | 37 (49.3%) | ||
| Age (years) | 8.6 (±1.5) | 8.9 (±1.6) | 8.2 (±1.4) | 8.6 (±1.5) | 8.5 (±1.5) | 8.6 (±1.5) |
| Weight (kg) | 33.1 (±10.1) | 35.4 (±10.9) | 31.5 (±9.4) | 33.0 (±10.0) | 31.8 (±9.0) | 34.7 (±11.2) |
| Height (cm) | 133.6 (±11.5) | 134.5 (±13.5) | 132.3 (±10.6) | 134.0 (±10.8) | 132.9 (±11.2) | 134.3 (±11.9) |
| BMI Z-Score | 0.8 (±1.5) | 1.1 (±1.5) | 0.62 (±1.5) | 0.66 (±1.6) | 0.56 (±1.3) | 1.0 (±1.7) |
| Underweight | 9 (4.2%) | 2 (3.2%) | 5 (6.5%) | 2 (2.7%) | 5 (4.4%) | 4 (4%) |
| Healthy Weight | 109 (50.9%) | 27 (43.6%) | 39 (50.6%) | 43 (57.3%) | 64 (56.1%) | 45 (45%) |
| Overweight | 47 (22.0%) | 16 (25.8%) | 20 (26.0%) | 11 (14.7%) | 32 (28.1%) | 15 (15%) |
| Obese | 49 (22.9%) | 17 (27.4%) | 13 (16.9%) | 19 (25.3%) | 13 (11.4%) | 36 (36%) |
| SES | ||||||
| Low | 91 (42.5%) | 41 (66.1%) | 26 (33.8%) | 24 (32.0%) | 48 (42.1%) | 43 (43%) |
| Medium | 70 (32.7%) | 16 (25.8%) | 25 (32.5%) | 29 (38.7%) | 41 (36.0%) | 29 (29%) |
| High | 53 (24.8%) | 5 (8.1%) | 26 (33.8%) | 22 (29.3%) | 25 (21.9%) | 28 (28%) |
| FBG (mg/dL)1 | 85.5 (±6.6) | 87.8 (±6.3) | 85.5 (±7.1) | 83.5 (±5.6) | 85.4 (±6.8) | 85.6 (±6.3) |
| Sociodemographic Variable | BMI Z-Score | FBG Adjusted by BMI Z-Score |
|---|---|---|
| BMI Z-Score | 0.337 | |
| (−0.254, 0.928) | ||
| Zone 2 vs. Zone 1 | −0.223 | −2.518 * |
| (−0.755, 0.309) | (−4.813, −0.224) | |
| Zone 3 vs. Zone 1 | −0.052 | −4.638 *** |
| (−0.606, 0.501) | (−7.020, −2.255) | |
| SES: Medium vs. Low | −0.23 | 1.453 |
| (−0.729, 0.269) | (−0.699, 3.606) | |
| SES: High vs. Low | 0.199 | 1.71 |
| (−0.699, 1.096) | (−2.157, 5.576) | |
| Maternal Education: 13 years vs. 5–8 years | −0.539 * (−1.056, 0.023) | −0.203 (−2.450, 2.044) |
| Maternal Education: 16+ years vs. 5–8 years | −1.031 * (−2.014, −0.048) | −0.761 (−5.037, 3.514) |
| Constant | 1.347 *** | 87.036 *** |
| (0.934, 1.760) | (85.089, 88.983) |
| Sociodemographic Variable | BMI Z-Score | FBG Adjusted by BMI Z-Score |
|---|---|---|
| BMI Z-Score | 0.537 | |
| (−0.412, 1.485) | ||
| Zone 2 vs. Zone 1 | −0.011 | −3.033 |
| (−0.629, 0.608) | (−6.080, 0.015) | |
| Zone 3 vs. Zone 1 | 0.015 | −6.312 *** |
| (−0.676, 0.706) | (−9.717, −2.907) | |
| SES: Medium vs. Low | −0.209 | 0.659 |
| (−0.825, 0.408) | (−2.383, 3.702) | |
| SES: High vs. Low | −0.002 | 3.623 |
| (−1.406, 1.402) | (−3.291, 10.536) | |
| Maternal Education: 13 years vs. 5–8 years | −0.664 * (−1.279, −0.048) | 1.037 (−2.059, 4.132) |
| Maternal Education: 16+ years vs. 5–8 years | −0.537 (−2.015, 0.942) | −2.899 (−10.199, 4.401) |
| Constant | 0.998 *** | 87.319 *** |
| (0.527, 1.469) | (84.813, 89.825) |
| Sociodemographic Variable | BMI Z-Score | FBG Adjusted by BMI Z-Score |
|---|---|---|
| BMI Z-Score | 0.265 | |
| (−0.536, 1.066) | ||
| Zone 2 vs. Zone 1 | −0.664 | −1.213 |
| (−1.617, 0.289) | (-4.918, 2.491) | |
| Zone 3 vs. Zone 1 | −0.458 | −1.659 |
| (−1.414, 0.498) | (−5.354, 2.036) | |
| SES: Medium vs. Low | −0.104 | 2.994 |
| (−0.945, 0.737) | (−0.241, 6.229) | |
| SES: High vs. Low | 0.196 | 1.303 |
| (−1.090, 1.483) | (−3.649, 6.255) | |
| Maternal Education: 13 years vs. 5–8 years | −0.462 (−1.344, 0.419) | −1.959 (−5.369, 1.452) |
| Maternal Education: 16+ years vs. 5–8 years | −1.311 (−2.788, 0.166) | 0.196 (−5.582, 5.974) |
| Constant | 1.923 *** | 85.993 *** |
| (1.173, 2.674) | (82.721, 89.266) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bansal, E.; Placidi, D.; Carver, S.; Renzetti, S.; Giorgino, A.; Cagna, G.; Zoni, S.; Fedrighi, C.; Montemurro, M.; Oppini, M.; et al. Metabolic Outcomes in Southern Italian Preadolescents Residing Near an Industrial Complex: The Role of Residential Location and Socioeconomic Status. Int. J. Environ. Res. Public Health 2019, 16, 2036. https://doi.org/10.3390/ijerph16112036
Bansal E, Placidi D, Carver S, Renzetti S, Giorgino A, Cagna G, Zoni S, Fedrighi C, Montemurro M, Oppini M, et al. Metabolic Outcomes in Southern Italian Preadolescents Residing Near an Industrial Complex: The Role of Residential Location and Socioeconomic Status. International Journal of Environmental Research and Public Health. 2019; 16(11):2036. https://doi.org/10.3390/ijerph16112036
Chicago/Turabian StyleBansal, Esha, Donatella Placidi, Shaye Carver, Stefano Renzetti, Augusto Giorgino, Giuseppa Cagna, Silvia Zoni, Chiara Fedrighi, Miriana Montemurro, Manuela Oppini, and et al. 2019. "Metabolic Outcomes in Southern Italian Preadolescents Residing Near an Industrial Complex: The Role of Residential Location and Socioeconomic Status" International Journal of Environmental Research and Public Health 16, no. 11: 2036. https://doi.org/10.3390/ijerph16112036