1. Introduction
Global estimates report that 191 million population have moderate to extreme vision impairment (MEVI), and among them 32.4 million are blind, with a high proportion of females (60%) [
1]. Although South Asian countries encounter a high burden of age-related blindness, this is still lower than Sub Saharan countries (4.4% vs. 6.0%), whereas prevalence of the MEVI is slightly higher in South Asian countries (23.6%) than in Oceana (18.9%) [
1]. Uncontrolled refractive errors (43%) are the foremost reason for visual impairment (VI) and are trailed by cataracts (33%), diabetic retinopathy (DR), glaucoma and age-related macular degradation (ARMD) [
2]. Similarly, a study in Iran revealed that almost 32 out of 44 persons with blinding issues had cataracts, 10 out of 44 had diabetic retinopathy and more than two out of 44 had glaucoma [
3]. Additionally, other studies from Iran provided evidence of poor eye examination as only 22% of diabetic patient had had eye checkups and two out of five non-diabetic individuals with eye disease had a history of proper eye checkups [
4,
5]. The large-scale population-based survey in Pakistan in 2006 reported that prevalence of blindness was 2.7% and was highest in Punjab and Baluchistan and was severe in the rural areas, while it was lowest in North West Frontier Province (known as Khyber Pakhoonkhwa) [
6]. Similarly, the study by Dineen et al., in 2007 articulated that among the many causes of blindness the cataract (51.5%) is the foremost cause of blindness in Pakistan, followed by corneal opacity (11.8%), and glaucoma (7.1%) [
7].
Knowledge regarding the ARMD in Hong Kong Chinese population (9.2%) [
8] and related to glaucoma in Iranian population (46.6%) is really low [
9]. The level of public awareness related to major blindness causes has been reported to be low even in developed countries [
10,
11]. However, health promotion helps to reduce the encumbrance of eye ailments and ultimately limit avoidable causes of blindness [
12] as many studies revealed the importance of blood pressure and glycemic control in the development and progression of diabetic retinopathy reduces the numbers of cases [
13]. From the past evidences of knowledge, attitude and practice (KAP) studies it is obvious that immense need for the knowledge regarding risk factor, control, prevention diagnosis and management subsists among the community [
14,
15]. The need of the hour is to alleviate the diseases burden by proper implementation and reinforcement of public health policies specifically focusing on VI risk factors. Factors associated with the public health plans are scarcity of awareness of eye diseases [
16,
17] that is coupled with poorer prevention [
18], inappropriate eye care [
19] and inadequate treatment [
20].
Very few studies have been performed in Pakistan to evaluate the KAP ofblindness. The general public is never being interviewed about the KAP of eye disease, except only one study by Memon assessing the KAP regarding diabetes and diabetic retinopathy in Karachi [
21], which evaluated the knowledge of 271 respondents regarding diabetes and DR, and only focused on DR while all other eye diseases were not the subjects of interviews. Therefore, in order to construct the interventional and prevention policies the KAP of general population should be measured so it will be helpful to estimate the awareness gaps in general population which should be covered. Therefore, in our study we report the KAP and associated factors in terms of demographics in area of Punjab, Pakistan.
4. Discussion
Our study is the first of its kind, which evaluated the KAP of common eye ailments from the general population of Pakistan. The major conclusion of our study was that awareness about common eye conditions among the Pakistani population was poor. More than two thirds (68.5%) of the population were unaware of ARMD and deficiency was more prominent in old people, rural community and uneducated people. The outcome of this study is two-fold. Firstly, this study showed insignificant adequacy regarding knowledge and awareness about the common eye conditions among the general public which is more intense in population with rural locality, low SES, and low educational level. Secondly, the community with low education, low SES and rural locality were less likely to have regular eye checks. This suggests that increase in health literacy will ultimately improve health-seeking behavior surrounding eye conditions. Like some developing countries such as Bangladesh [
26], tertiary health care facilities are providing appropriate ophthalmic services in Pakistan. It was beyond this project to demonstrate the prevalence of different eye diseases in our population, but evidence suggested that increasing knowledge and understanding correspondingly increased the regular eye examinations which definitely reduce the ocular diseases and reduce economic burden due to ocular disturbances [
30].
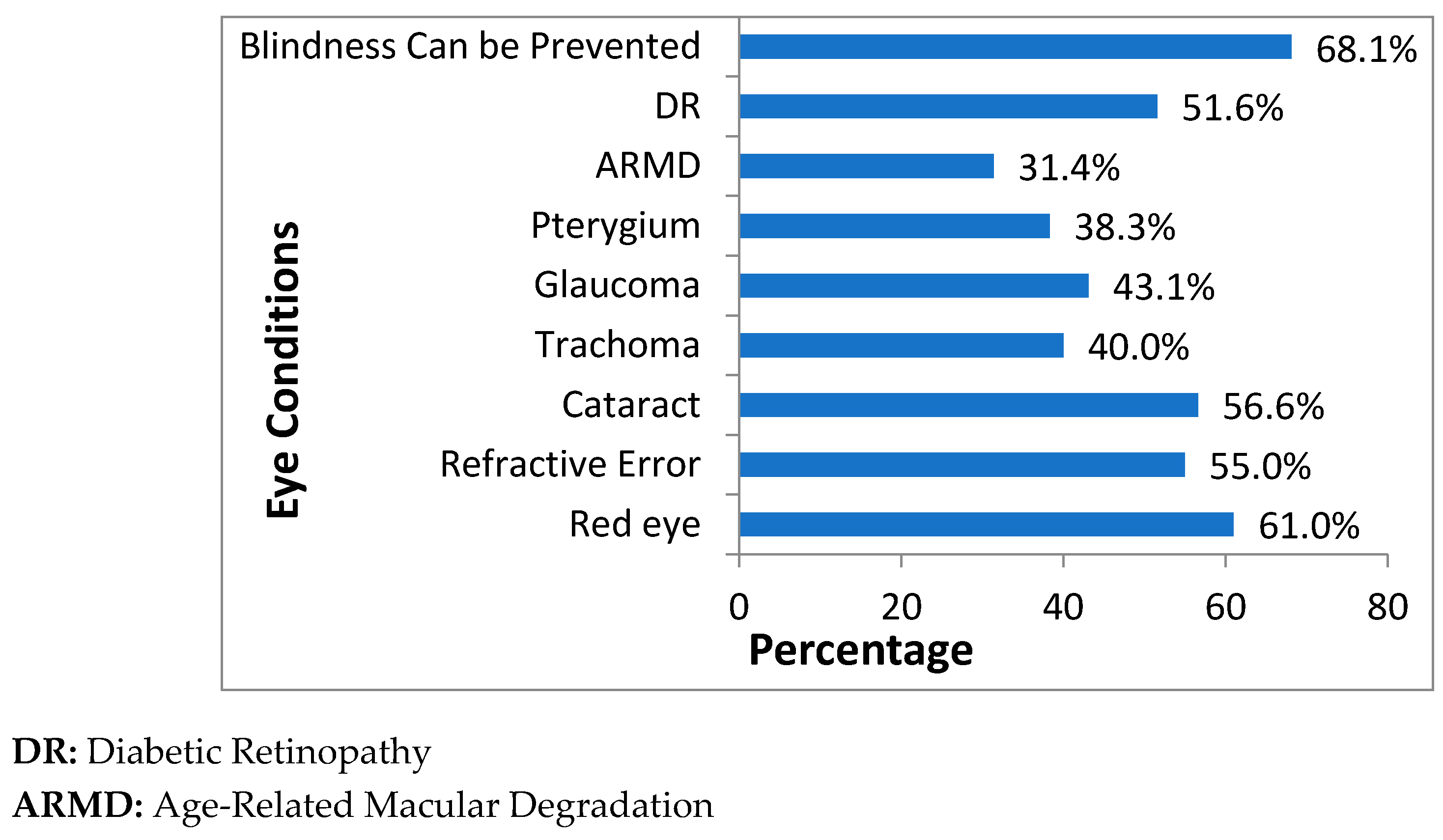
Our study results were dissimilar with the results from a study in Bangladesh. The lowest awareness, in our study, was seen about the ARMD which is 31.4% to highest awareness about the fact that blindness can be prevented (68.1%) whereas, in the study by Islam et al. the minimum awareness was seen for DR (4%) and maximum for cataracts (91%), although adequate awareness in both the studies was low and is associated with education status [
26]. Similarly, SES and educational status were associated with the increase in awareness of diabetes in Bangladesh [
31]. Low ocular disease awareness was seen among the population with low education and low SES in developing [
30,
32] as well as in developed countries [
33]. Slightly higher than half (55%) of our respondents showed good knowledge towards refractive error, which is in accordance with the study by Alemayehu et al., which showed that 55.9% of participants had good knowledge towards refractive error [
34]. In this study, awareness related to cataract and DR is 56.6% and 51.6%, respectively. These results are not in accordance with the results of the study by Marzieh et al., which showed 82.9% were aware of cataracts and 86.2% were aware of DR [
9]. Additionally, results regarding the cataract are dissimilar with the study of Lau et al., which showed awareness of 90% respondents [
8]. Another interesting finding is that the entire knowledge items were significantly associated with gender (females were significantly higher in awareness than males) which contradicts the results of a study in Bangladesh in which insignificant difference in awareness of almost all the items exists [
26]. Similarly, our results contradict the results of another study by Islam et al., where a significantly higher level of awareness about diabetes and its risk factors was seen among the males [
31]. However, these comparisons cannot be considered as true comparisons as the studies by Islam et al., which were conducted only in rural communities, as compared to our population which has both rural and urban population. However, these are close comparisons as almost half of our population is from rural areas with equivalent SES and educational status as in Bangladesh.
In terms of association of an individual disease item with the demographics, in our study population over the age of 60 were 1.21 times (AOR = 1.21 95%CI = 0.56, 2.61) more aware of trachoma as compared to population in age group 18–30. These outcomes were out of line with the previous findings of Dandona, in which odds of being aware increase with age, i.e., population in age group 60–69 were 3.25 times (AOR = 3.25 95%CI = 2.10–5.0) more aware of cataract than population in age group 16–29 [
30]. In case of glaucoma and DR, our study has provided evidence that there is increase in awareness with the increase of education level, which is also apparent in the previous studies [
8,
30]. Inequity subsists in awareness intensity among the males and females. In current study, the females were 1.54 times (AOR = 1.54 95%CI = 1.25, 1.88) more aware for cataract, 1.68 times (AOR = 1.68 95%CI = 1.37, 2.07) more for trachoma and 1.51 times (AOR=1.51 95%CI = 1.23, 1.84) more aware for glaucoma. These results are in accordance with the previous study in Iran where females were 1.48 times more (AOR 1.48 95% CI 1.06, 2.06) aware about cataract and 1.93 times more aware about glaucoma (AOR 1.93 95%CI 1.13, 3.32) [
9] but are absolutely contrary to the findings of study in Nepal where males were 1.77 times (OR = 1.77 95% CI = 1.46–2.14), 1.38 times (OR = 1.38 95% CI = 1.09, 1.75) and 1.67 times (OR = 1.67 95%CI = 1.10–2.52) more aware about cataract, glaucoma and trachoma, respectively [
32].
Attitude concerning treatment of ocular diseases among our cohort was remarkably high and 82% of our population was of the view that they would go to a physician to seek treatment upon noticing any eye ailment. These results were in accordance with the previous study of Islam et al., which showed that 90% of the population was willing to accept medical care for ocular disturbances [
26]. Despite the fact, it is apparent from the previous finding that attending eye examinations is a challenge for the general population in developing countries [
26]. However, evidence also signifies that alleviating the scarcity of knowledge and awareness ultimately reduces the delay in diagnosis among rheumatoid arthritis patients in UAE [
33] and augments the involvement of participants in screening of breast cancer in Hawaii [
35].
Practice regarding the eye examination among our cohort was positive, and only 24% of our population had never had an eye examination, while 17.2% had an eye check more than once in a year. Practice of our population is far better than that seen in the study by Paudel et al., in which 53.5% of respondents had never had an eye check [
36]. In the present study, frequency of at least one visit to the doctor was considerably high among those who had eye disease (24.5%) than those who did not have eye disease (19.5%). These results coincide with a study on Bangladesh [
26]. Similarly, results from developed countries like Australia illustrate good health-seeking practices and 61% of the participants visited either an optometrist or ophthalmologist, at least once in the past two years [
11]. Studies related to DR in Low Resource Nations indicated the poor practice and behavior of patients toward eye checks. Those patients are motivated to visit a doctor if their vision is threatened or there is an abrupt disturbance in vision [
37].
Limitations
Our study had some strengths and drawbacks. In terms of strengths, to begin with, our study consisted of face-to-face interviews by trained data collectors that ensure completeness and validity of data collection. Furthermore, face-to-face interviews remove ambiguities among the general population and are helpful in describing the purposes of research activities. Secondly, a sophisticated and reliable technique (Rasch analysis) was adopted to analyze the data. In terms of drawbacks, first we selected the cities randomly and similarly village in selected districts were targeted randomly. However, efforts were made to collect the data from different geographic region of Punjab. Second, the sample mainly consists of male students which may indicate a bias in the random selection of the respondents. Our response to this is that we did not randomly select participants from multiple members of one house; we adopted a well-developed and validated lottery method which gives the same probability of each willing individual being recruited for the study. Students or the educated communities are more likely to understand research activities and show more willingness to participate in such surveys. Third, our sample consisted of 2/3 males whereas the census shows a higher percentage of females; this creates unequal distribution, and the sample may not be truely representative. This effect is due to the reluctance of females to participate, and also the lower education level of females, which is also a hindering factor in being part of an epidemiological study. This could be overcome by introducing female research assistants for interviewing females. Fourth, we selected only one individual from a house even if multiple members were willing. This effect reduced the repetition of the same responses, as observed in previous studies, since when we approach multiple members the answers are almost the same and sometimes they even ask us to copy the answers from another member’s questionnaire. Fifth, this study focused in Punjab only so cannot be generalized to the whole country. Nevertheless, as the first survey of its kind from the most populated region in Pakistan, the current study provided us a clearer picture of the KAP of common ocular conditions among the general public in Pakistan. Lastly, we were unable to check interviewer reliability. Our resources, time and population did not allow two interviewers to check inter-rater reliability (two interviewers interviewing the same individual). However, data collection was carried out by trained and diligent data collectors, and was cross-checked for completeness and thoroughness by the PI.

 ,
, 

{kind=link}