Predictors of Lymphoceles in Women Who Underwent Laparotomic Retroperitoneal Lymph Node Dissection for Early Gynecologic Cancer: A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mori, N. Clinical and experimental studies on the so-called lymphocyst which develops after radical hysterectomy in cancer of the uterine cervix. J. Jpn. Obstet. Gynecol. Soc. 1955, 2, 178–203. [Google Scholar] [PubMed]
- Logmans, A.; Kruyt, R.H.; De Bruin, H.G.; Cox, P.H.; Pillay, M.; Trimbos, J.B. Lymphedema and lymphoceles following lymphadenectomy may be prevented by omentoplasty: A pilot study. Gynecol. Oncol. 1999, 75, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.J.; Plentl, A.A.; Taylor, H.C., Jr. The lymphocyst: A complication of pelvic lymph node dissections. Am. J. Obstet. Gynecol. 1958, 75, 1059–1062. [Google Scholar] [CrossRef]
- Mann, W.J.; Vogel, F.; Patsner, B.; Chalas, E. Management of lymphoceles after radical gynecologic surgery. Gynecol. Oncol. 1989, 33, 248–250. [Google Scholar] [CrossRef]
- Benedetti-Panici, P.; Maneschi, F.; Cutillo, G.; D’Andrea, G.; di Palumbo, V.S.; Conte, M.; Scambia, G.; Mancuso, S. A randomized study comparing retroperitoneal drainage with no drainage after lymphadenectomy in gynecologic malignancies. Gynecol. Oncol. 1997, 65, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.; Benedetti-Panici, P.; Guariglia, L.; Scambia, G.; Greggi, S.; Mancuso, S. Pelvic lymphocele following radical para-aortic and pelvic lymphadenectomy for cervical carcinoma: Incidence rate and percutaneous management. Obstet. Gynecol. 1990, 76, 268–271. [Google Scholar] [PubMed]
- Kim, H.Y.; Kim, J.W.; Kim, S.H.; Kim, Y.T.; Kim, J.H. An analysis of the risk factors and management of lymphocele after pelvic lymphadenectomy in patients with gynecologic malignancies. Cancer Res. Treat. 2004, 36, 377–383. [Google Scholar] [CrossRef]
- Achouri, A.; Huchon, C.; Bats, A.S.; Bensaid, C.; Nos, C.; Lecuru, F. Complications of lymphadenectomy for gynecologic cancer. Eur. J. Surg. Oncol. 2013, 39, 81–86. [Google Scholar] [CrossRef]
- Petru, E.; Tamussino, K.; Lahousen, M.; Winter, R.; Pickel, H.; Haas, J. Pelvic and paraaortic lymphoceles after radical surgery because of cervical and ovarian cancer. Am. J. Obstet. Gynecol. 1989, 161, 937–941. [Google Scholar] [CrossRef]
- Benedet, J.L.; Turko, M.; Boyes, D.A.; Nickerson, K.G.; Bienkowska, B.T. Radical hysterectomy in the treatment of cervical cancer. Am. J. Obstet. Gynecol. 1980, 137, 254–262. [Google Scholar] [CrossRef]
- Achouri, A.; Huchon, C.; Bats, A.S.; Bensaid, C.; Nos, C.; Lecuru, F. Postoperative lymphoceles after lymphadenectomy for gynaecological malignancies: Preventive techniques and prospects. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 161, 125–129. [Google Scholar] [CrossRef]
- Pennehouat, G.; Mosseri, V.; Durand, J.C.; Hamelin, J.P.; Asselain, B.; Pilleron, J.P.; Salmon, R.J. Lymphoceles and peritonization following lymphadenectomy for cancer of the uterus. J. Gynecol. Obstet. Biol. Reprod. 1988, 17, 373–378. (In French) [Google Scholar]
- Thome Saint Paul, M.; Bremond, A.; Rochet, Y. Absence of peritonization after pelvic cancer surgery. Results in 157 cases. J. Gynecol. Obstet. Biol. Reprod. 1991, 20, 957–960. (In French) [Google Scholar]
- Franchi, M.; Ghezzi, F.; Zanaboni, F.; Scarabelli, C.; Beretta, P.; Donadello, N. Nonclosure of peritoneum at radical abdominal hysterectomy and pelvic node dissection: A randomized study. Obstet. Gynecol. 1997, 90, 622–627. [Google Scholar] [CrossRef]
- Bafna, U.D.; Umadevi, K.; Savitha, M. Closed suction drainage versus no drainage following pelvic lymphadenectomy for gynecological malignancies. Int. J. Gynecol. Cancer 2001, 11, 143–146. [Google Scholar] [CrossRef]
- Symmond, R.E.; Pratt, J.H. Prevention of fistulas and lymphoceles in radical hysterectomy. Preliminary report of a new technique. Obstet. Gynecol. 1961, 17, 57–64. [Google Scholar]
- Charoenkwan, K.; Kietpeerakool, C. Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies. Cochrane Database Syst. Rev. 2017, 6, CD007387. [Google Scholar]
- Franchi, M.; Trimbos, J.B.; Zanaboni, F.; v d Velden, J.; Reed, N.; Coens, C.; Teodorovic, I.; Vergote, I. Randomised trial of drains versus no drains following radical hysterectomy and pelvic lymph node dissection: A European Organisation for Research and Treatment of Cancer-Gynaecological Cancer Group (EORTC-GCG) study in 234 patients. Eur. J. Cancer 2007, 43, 1265–1268. [Google Scholar] [CrossRef]
- Panici, P.B.; Maggioni, A.; Hacker, N.; Landoni, F.; Ackermann, S.; Campagnutta, E.; Tamussino, K.; Winter, R.; Pellegrino, A.; Greggi, S.; et al. Systematic aortic and pelvic lymphadenectomy versus resection of bulky nodes only in optimally debulked advanced ovarian cancer: A randomized clinical trial. J. Natl. Cancer Inst. 2005, 97, 560–566. [Google Scholar] [CrossRef]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Hauth, J.C.; Rouse, D.J.; Spong, C.Y. William Obstetrics, 23rd ed.; McGraw-Hill: New York, NY, USA, 2010; pp. 189–214. [Google Scholar]
- Dimpfl, T.; Stumpfe, M.; Maassen, V.; Genz, T. Lymphocele and complications after pelvic/para-aortic lymph node excision in relation to closure of the peritoneum. GeburtshilfeFrauenheilkd 1994, 54, 233–236. (In German) [Google Scholar]
- Suzuki, M.; Ohwada, M.; Sato, I. Pelvic lymphoceles following retroperitoneal lymphadenectomy: Retroperitoneal partial “no-closure” for ovarian and endometrial cancers. J. Surg. Oncol. 1998, 68, 149–152. [Google Scholar] [CrossRef]
- Lopes, A.D.; Hall, J.R.; Monaghan, J.M. Drainage following radical hysterectomy and pelvic lymphadenectomy: Dogma or need? Obstet. Gynecol. 1995, 86, 960–963. [Google Scholar]
- Pansrikaew, P.; Cheewakriangkrai, C.; Taweevisit, M.; Khunamornpong, S.; Siriaunkgul, S. Correlation of mast cell density, tumor angiogenesis, and clinical outcomes in patients with endometrioid endometrial cancer. Asian Pac. J. Cancer Prev. 2010, 11, 623–626. [Google Scholar]
- Zikan, M.; Fischerova, D.; Pinkavova, I.; Slama, J.; Weinberger, V.; Dusek, L.; Cibula, D. A prospective study examining the incidence of asymptomatic and symptomatic lymphoceles following lymphadenectomy in patients with gynecological cancer. Gynecol. Oncol. 2015, 137, 291–298. [Google Scholar] [CrossRef]
- Sheyn, D.; Bretschneider, C.E.; Mahajan, S.T.; Ridgeway, B.; Davenport, A.; Pollard, R. Incidence and risk factors of early postoperative small bowel obstruction in patients undergoing hysterectomy for benign indications. Am. J. Obstet. Gynecol. 2018, in press. [Google Scholar] [CrossRef]
- Kaneko, T.; Funahashi, K.; Ushigome, M.; Kagami, S.; Goto, M.; Koda, T.; Nagashima, Y.; Shiokawa, H.; Koike, J. Incidence of and risk factors for incisional hernia after closure of temporary ileostomy for colorectal malignancy. Hernia 2018, in press. [Google Scholar] [CrossRef]
- Arima, J.; Huang, C.; Rosner, B.; Akaishi, S.; Ogawa, R. Hypertension: A systemic key to understanding local keloid severity. Wound Repair Regen. 2015, 23, 213–221. [Google Scholar] [CrossRef]



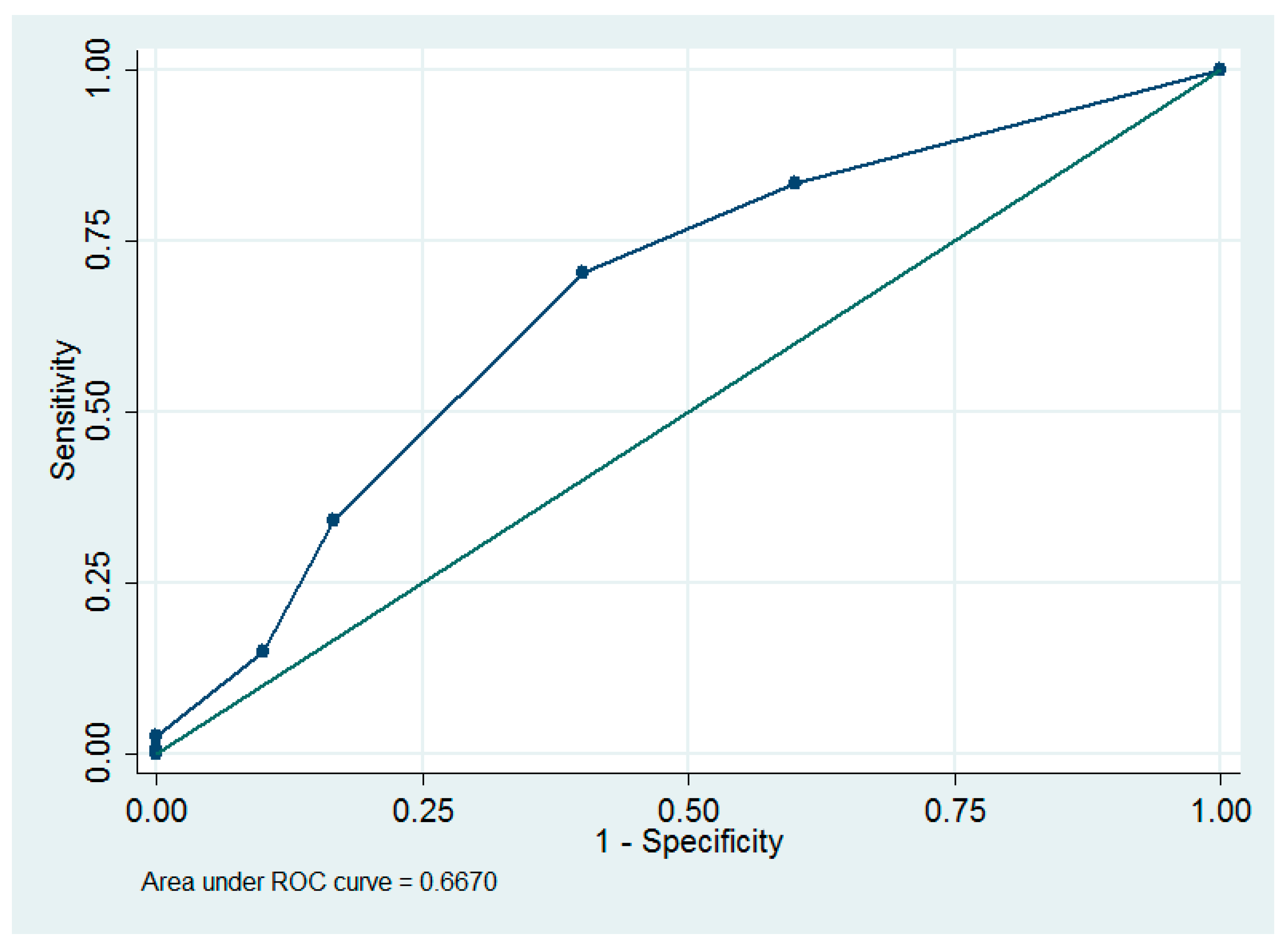{kind=link}
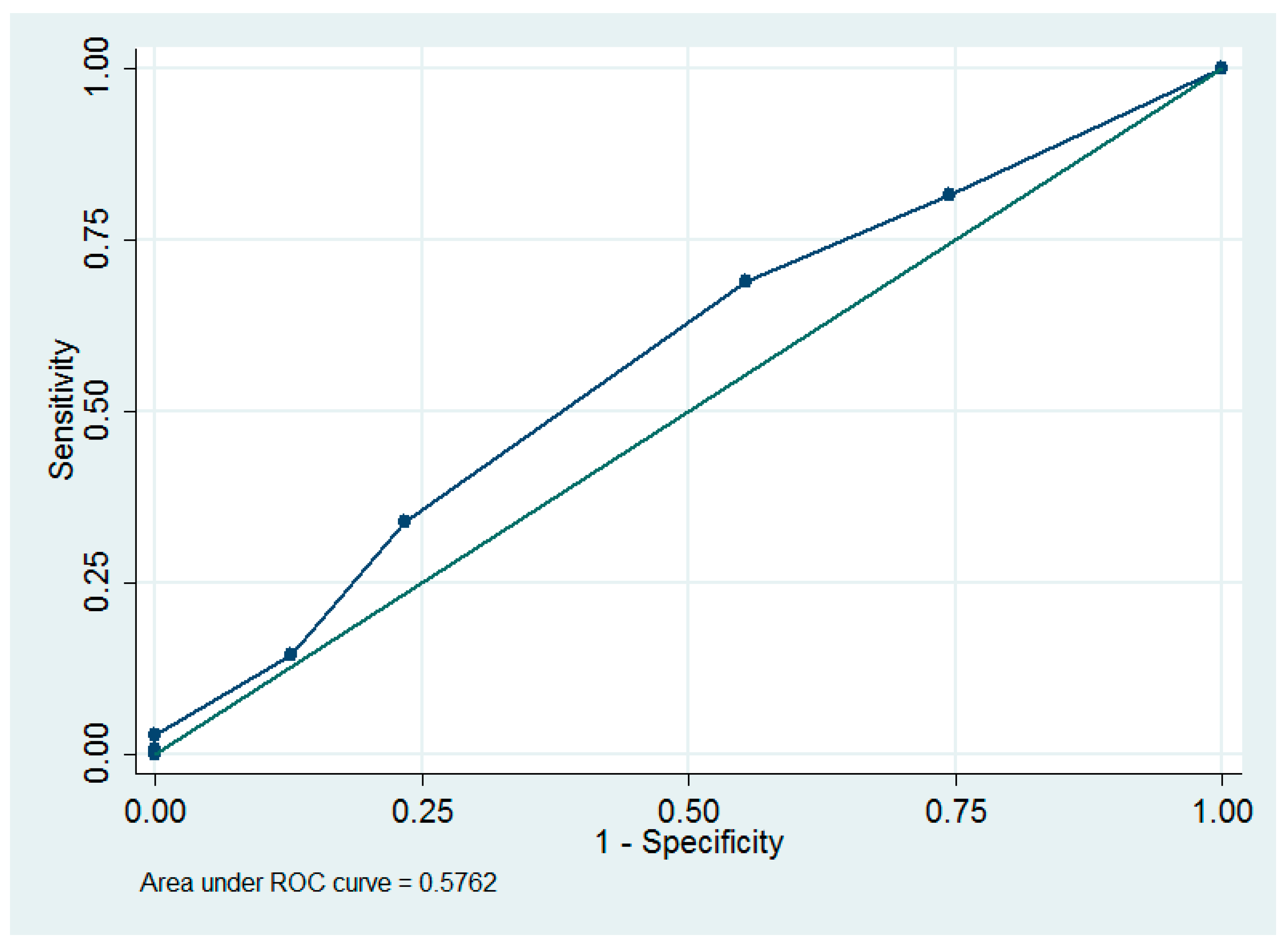{kind=link}
| Variables | Values |
|---|---|
| Age (years) | 53.3 ±10.6 |
| Parity | 1.9 ± 1.4 |
| Body mass index (kg/m2) | 26.0 ± 5.8 |
| Ovarian cancer or borderline tumor (stage I, n = 56; stage 2, n = 13) | 69 (34) |
| Endometrial cancer (stage I, n = 84; stage 2, n = 7) | 91 (45) |
| Cervical or vaginal cancer (stage I, n = 41; stage 2, n = 3) | 44 (22) |
| Diabetes | 24 (12) |
| Hypertension | 56 (27) |
| Peritoneal complete closure with pelvic drainage | 44 (22) |
| Peritoneal partial closure with pelvic drainage | 44 (22) |
| Peritoneal partial closure without pelvic drainage | 1 (1) |
| Peritoneal nonclosure with pelvic drainage | 24 (12) |
| Peritoneal nonclosure without pelvic drainage | 91 (45) |
| Pelvic drainage | 112 (55) |
| Adjuvant pelvic radiotherapy | 43 (21) |
| Adjuvant vaginal brachytherapy | 31 (15) |
| Adjuvant chemotherapy | 75 (34) |
| Complications | 50 (12) |
| Lymphocyst | 31 (14.7) |
| Symptomatic lymphocyst | 7 (3.4) |
| Postoperative ileus | 9 (4.4) |
| Miscellaneous | 11 (5.3) |
| Recurrence of cancer | 18 (8.8) |
| Variables | Peritoneal Complete Closure with Pelvic Drainage (a, n = 44) | Peritoneal Partial Closure with Pelvic Drainage (b, n = 44) | Peritoneal Partial Closure without Pelvic Drainage (c, n = 1) | Peritoneal Nonclosure with Pelvic Drainage (d, n = 24) | Peritoneal Nonclosure without Pelvic Drainage (e, n = 91) | † p | ‡ Post Hoc Analysis |
|---|---|---|---|---|---|---|---|
| Age (years) | 52.6 ± 10.8 | 53.7 ± 11.1 | - | 53.9 ± 8.3 | 53.4 ± 11.0 | 0.98 | |
| Parity | 2.1 ± 1.5 | 1.9 ± 1.4 | - | 1.6 ± 1.2 | 1.9 ± 1.3 | 0.68 | |
| Body mass index (kg/m2) | 26.7 ± 5.4 | 28.0 ± 7.5 | - | 23.2 ± 4.8 | 25.3 ± 4.9 | 0.01 | b vs. c, p = 0.001 |
| Diabetes | |||||||
| Yes | 2 (5) | 9 (20) | 0 (0) | 2 (9) | 11 (12) | 0.21 | |
| No | 42 (95) | 35 (80) | 1 (100) | 22 (91) | 80 (88) | ||
| Hypertension | |||||||
| Yes | 8 (18) | 14 (32) | 0 (0) | 4 (17) | 30 (33) | 0.23 | |
| No | 36 (82) | 30 (68) | 1 (100) | 20 (83) | 61 (67) | ||
| Stage | |||||||
| I | 41 (93) | 35 (80) | 1 (100) | 20 (83) | 84 (92) | 0.15 | |
| II | 3 (7) | 9 (20) | 0 (0) | 4 (17) | 7 (8) | ||
| Lymphocele | |||||||
| Yes | 4 (9) | 4 (9) | 0 (0) | 4 (17) | 19 (21) | 0.28 | |
| No | 40 (91) | 40 (91) | 1 (100) | 20 (83) | 72 (79) | ||
| Complication | |||||||
| Yes | 7 (16) | 5 (11) | 0 (0) | 9 (38) | 29 (32) | 0.02 | a vs. d, p = 0.045 |
| No | 37 (84) | 39 (89) | 1 (100) | 15 (62) | 62 (68) | b vs. d, p = 0.01 b vs. e, p = 0.01 |
| Variables | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | †p | Odds Ratio (95% CI) | ‡p | |
| Age (years) | 0.99 (0.95–1.02) | 0.53 | - | - |
| Parity | 0.62 (0.45–0.86) | 0.004 | 0.59 (0.42–0.84) | 0.003 |
| Body mass index (kg/m2) | 0.97 (0.91–1.05) | 0.48 | - | - |
| Diabetes | 1.13 (0.36–3.58) | 0.83 | - | - |
| Hypertension | 1.10 (0.47–2.55) | 0.83 | - | - |
| Ovarian cancer | 1.09 (0.49–2.43) | 0.83 | - | - |
| Radical hysterectomy | 0.82 (0.32–2.15) | 0.69 | - | - |
| Stage of cancer | 0.82 (0.23–2.94) | 0.76 | - | - |
| Adjuvant chemotherapy | 1.77 (0.82–3.82) | 0.15 | - | - |
| Adjuvant pelvic radiotherapy | 2.42 (1.06–5.56) | 0.04 | 2.60 (1.05–6.45) | 0.039 |
| Adjuvant vaginal brachytherapy | 1.42 (0.53–3.81) | 0.49 | - | - |
| Peritoneal complete closure with pelvic drainage (n = 44) | 0.49 (0.16–1.49) | 0.21 | - | - |
| Peritoneal partial closure with pelvic drainage (n = 44) | 0.49 (0.16–1.48) | 0.21 | - | - |
| § Peritoneal partial closure without pelvic drainage (n = 1) | - | - | - | - |
| Peritoneal nonclosure with pelvic drainage (n = 24) | 1.13 (0.36–3.58) | 0.83 | - | - |
| Peritoneal nonclosure without pelvic drainage (n = 91) | 2.22 (1.01–4.86) | 0.046 | 2.31 (1.01–5.30) | 0.048 |
| Variables | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | †p | Odds Ratio (95% CI) | ‡p | |
| Age (years) | 1.02 (0.99–1.05) | 0.19 | - | - |
| Parity | 0.82 (0.63–1.05) | 0.11 | 0.73 (0.55–0.96) | 0.03 |
| Body mass index (kg/m2) | 0.97 (0.91–1.03) | 0.25 | - | - |
| Diabetes | 0.79 (0.28–2.24) | 0.66 | - | - |
| Hypertension | 1.94 (0.98–3.83) | 0.057 | 2.62 (1.18–5.81) | 0.02 |
| Ovarian cancer | 1.14 (0.58–2.22) | 0.71 | - | - |
| Radical hysterectomy | 1.34 (0.64–2.81) | 0.44 | - | - |
| Stage of cancer | 1.40 (0.54–3.64) | 0.49 | - | - |
| Adjuvant chemotherapy | 1.07 (0.56–2.07) | 0.84 | - | - |
| Adjuvant pelvic radiotherapy | 1.45 (0.69–3.07) | 0.33 | - | - |
| Adjuvant vaginal brachytherapy | 0.88 (0.36–2.19) | 0.79 | - | - |
| Peritoneal complete closure with pelvic drainage (n = 44) | 0.51 (0.21–1.24) | 0.14 | - | - |
| Peritoneal partial closure with pelvic drainage (n = 44) | 0.32 (0.12–0.88) | 0.03 | 0.27 (0.09–0.83) | 0.02 |
| § Peritoneal partial closure without pelvic drainage (n = 1) | - | - | - | - |
| Peritoneal nonclosure with pelvic drainage (n = 24) | 2.03 (0.83–4.99) | 0.12 | - | - |
| Peritoneal nonclosure without pelvic drainage (n = 91) | 2.05 (1.07–3.91) | 0.03 | - | - |
| Variables | Spearman’s Rho | †p |
|---|---|---|
| Peritoneal partial closure with pelvic drainage | −0.08 | 0.26 |
| Pelvic drainage | −0.10 | 0.15 |
| Presence of lymphoceles | −0.04 | 0.62 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-H.; Ting, W.-H.; Lin, H.-H.; Hsiao, S.-M. Predictors of Lymphoceles in Women Who Underwent Laparotomic Retroperitoneal Lymph Node Dissection for Early Gynecologic Cancer: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 936. https://doi.org/10.3390/ijerph16060936
Chen H-H, Ting W-H, Lin H-H, Hsiao S-M. Predictors of Lymphoceles in Women Who Underwent Laparotomic Retroperitoneal Lymph Node Dissection for Early Gynecologic Cancer: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(6):936. https://doi.org/10.3390/ijerph16060936
Chicago/Turabian StyleChen, Hui-Hua, Wan-Hua Ting, Ho-Hsiung Lin, and Sheng-Mou Hsiao. 2019. "Predictors of Lymphoceles in Women Who Underwent Laparotomic Retroperitoneal Lymph Node Dissection for Early Gynecologic Cancer: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 6: 936. https://doi.org/10.3390/ijerph16060936