1. Introduction
Social capital is an important social determinant of well-being among older populations across countries and cultures. Many studies have focused on the consequences of social capital [
1]. For example, social capital was found to have important effects on self-rated health (SRH), life satisfaction, depression, physical disease, and even mortality among older adults [
1,
2,
3,
4,
5]. However, studies on the determinants of social capital among older populations are limited. Many studies have controlled for a range of sociodemographic variables (e.g., age, gender, marital status, education) when testing the relationship between social capital and health [
2,
6]. However, there is a lack of research that can explain the associations between these variables and social capital. The findings of such studies would enhance the understanding of what matters for social capital, and would have important implications for policy and interventions aimed at improving the health of older populations through promoting social capital.
Many studies use a single indicator to represent the multidimensional concept of social capital. Different studies also tend to use different methods of assessing social capital [
7]. Therefore, it is difficult to compare findings among studies and generate meaningful conclusions. Moreover, social capital has different meanings and functions across different life stages [
1]. However, many studies on social capital draw their samples from the general population. Studies on the determinants of social capital in later life are limited. Furthermore, the majority of relevant studies have examined the effects of social capital on a range of health outcomes from the social causation perspective. However, the above relationships can be bidirectional, and the social selection model offers an alternative explanation [
8]. Compared with those with disabilities and severe illnesses, individuals who are free of health problems might be more likely to actively participate in both informal and formal social activities in local communities, and develop higher levels of community social capital.
Finally, social capital is culturally sensitive. Empirical evidence shows that ethnicity, migration, and historical background could explain variations in levels of social capital [
9]. There is a lack of research on what matters for social capital in China, where familism and Confucian ideology are greatly emphasized. Family and community are two of the most important sources of social capital for older adults in China [
10,
11]. However, the interplay between social capital indicators embedded from family and community systems have been largely unstudied (hereafter community social capital and family social capital). Therefore, the present study aimed to fill this gap in the research by building and testing latent constructs of community social capital, and examined the social determinants of community social capital in an urban Chinese context, with a particular emphasis on health and family social capital.
1.1. Defining Social Capital
Experts in different research fields have defined social capital from different perspectives. The most adopted definition is from the perspective of social cohesion, which defines social capital as “features of social organization, such as trust, norms, and networks that can improve the efficiency of society by facilitating coordinated action” [
12]. Social capital can also be viewed as social resources embedded from individuals’ social relationships in their local communities and/or family systems, where they have shared norms, values, and common memberships [
13]. Lin [
14] examined individuals’ investment in their social networks and how individuals invest their social supportive resources with expected returns. While previous researchers paid close attention to the closure or density of social networks, Lin proposed that bridges in social connections also play an important role in sharing information and knowledge, and searching for important social resources from other social networks. Furthermore, there is a lack of consensus on the measurement levels and instruments on social capital. Social capital can be measured from individual, family, and community levels [
1,
7]. In this study, we focused on the individual level of social capital, which inheres in the density or closure of community social networks. This level of social capital is recognized as a key predictor of older populations’ health [
1,
2,
3,
4,
5], which can be used by older adults to preserve social supportive resources and pursue their individual or collective interests [
12,
13,
14].
Community social capital is a multifaceted concept that can be divided into two categories, namely, cognitive and structural social capital [
1]. Cognitive social capital is relatively subjective, and consists of the norms, values, and beliefs that influence people’s participation in society [
7]. It is often measured by trust and reciprocity among neighbors [
1]. Structural social capital is relatively objective, and reflects social interactions among people, which are often organized by formal organizations in the community. Structural social capital is often measured through organization memberships and social participation [
7]. Family social capital is also considered as a multidimensional concept, which can be measured by both structural components and social support, interaction, and relationship in the family system [
15]. Compared with the structural components of family social capital (e.g., the number of children), family network and support components (e.g., quality of family relationship and family support) had stronger impacts on the health outcomes among older adults [
10,
11,
15]. Therefore, we examined family social capital from a family network support perspective in the present study.
1.2. Determinants of Community Social Capital
Community social capital is influenced by both microlevel determinants (e.g., income, education and health) and macrolevel determinants (e.g., income inequality and national cohesion). Microlevel determinants seem to be more influential for all of the dimensions of community social capital. Specifically, individuals’ socioeconomic status (i.e., income and education) is the most important determinant of community social capital [
16].
As discussed previously, few studies have examined the multidimensional construct of social capital comprehensively. Instead, a range of indicators have been adopted to represent the levels of community social capital. For example, interpersonal trust, general trust, institutional trust, reciprocity among neighbors, and the sense of belonging are used to assess cognitive social capital [
16,
17,
18,
19,
20]. Specifically, individuals with higher incomes and more education have higher levels of interpersonal trust [
17,
18,
19]. Age, marital status, and religiosity are positively associated with both general and institutional trust [
18,
21]. Education tends to increase the likelihood of reciprocity, and age and general health were found to be positively associated with trust and the sense of belonging to local communities [
20]. However, findings on the relationship between education, income, gender, and institutional trust are inconsistent [
16,
18]. The inconsistent findings might have to do with the lack of consensus on the operationalization of social capital, as well as the cultural and historical contexts from which samples have been drawn.
With regard to structural social capital, the number of organization memberships, social participation, volunteering, and civic participation are common adopted indicators [
16,
21,
22,
23]. Specifically, individuals who are older, male, and employed are likely to have more organization memberships, as are those who have higher income and education [
16]. Ethnicity, marital status, and health are the most important determinants of social participation [
22,
24]. Furthermore, education, income, and health are the most important determinants of volunteering in later life [
23,
25]. Finally, higher income and education foster higher levels of civic participation [
16]. In addition, men tend to have significantly higher levels of civic participation than women [
21].
The majority of relevant studies have been conducted in Western contexts. Variations in levels of social capital by sociodemographic characteristics, socioeconomic status, and health status may be partly explained by variations in individuals’ health and financial resources, social status, time, and skills, which can further affect social involvement in the local community and society as a whole. These indicators tended to influence some components of social capital. However, few indicators were found to affect all of the components of social capital [
18]. We argue that social capital cannot be observed directly. This concept should be treated as a latent construct, which are manifested by a range of observed variables [
26]. Furthermore, microlevel determinants might have different impacts on different dimensions of social capital (i.e., cognitive and structural dimensions). Therefore, they should be studied separately while considering their specific cultural and historical contexts. In particular, most studies tend to depend on a single health indicator to assess the effect of health on social capital. Different components of health (e.g., activities of daily living (ADLs) and instrumental activities of daily living (IADLs)) might play different roles in influencing cognitive social capital and structural social capital.
1.3. Population Aging and Family Social Capital in China
China is one of the most rapidly aging countries in the world. The number of adults 65 or older in China increased from 118.9 million in 2010 to 223.0 million in 2015 [
27]. The proportion of older adults in the total population was 8.92% in 2010 and 10.47% in 2015. Given the rapid urbanization taking place in China, more and more older Chinese adults will be living in urban areas.
How can China meet the long-term care needs of its rapidly aging population? This will be a great challenge for both Chinese policy makers and professionals in the next few decades. Family is the most important source of old-age care in China. Unlike the individualist West, China has a unique culture of Confucianism. Filial piety, a key concept of Confucianism, refers to older adults being well-respected and cared for by families and children. This is the foundation of cultural values as well as the affective bond in Chinese families [
28]. However, traditional living arrangements for older adults have undergone a great transition. The majority of older Chinese lived with their adult children in the 1980s. However, the proportion of older adults who lived alone or with their spouse reached 22.84% in 2000 and 31.76% in 2010 [
29]. Modernization and rural-to-urban migration have also weakened family support resources for older adults, especially in terms of instrumental support.
In a word, the traditional family-based old-age care system has undergone great challenges. As the demand for long-term care will increase dramatically in the next half century, experts should consider how to build more sustainable support systems for older populations in China. Community social capital not only helps older adults achieve aging in place, but can also be considered a preventive strategy for sustaining the welfare of older adults [
1,
2,
7]. Fostering community social capital is also consistent with national policy development in China. In the recent seventh session of 13th National People’s Congress Standing Committee (December 2018), the Chinese government decided to extend the term of office of neighborhood committees from three years to five years. In doing so, neighborhood committees would have more stable teams to strengthen the functions of community and provide better quality of service for older residents in the communities. Under such circumstances, community social capital would play an important role in the future development of national long-term care systems in China.
In this study, family social capital is considered a key determinant of community social capital in Chinese contexts. However, the interplay between family and community social capital has been largely unstudied among older populations in China. On the one hand, family is not only the preferred source or support for older adults, but also plays an important role in helping elders find meaning in life and enhancing their self-esteem [
30]. Obedience and respect from offspring and family harmony are important indicators of success of life in older age [
28]. Therefore, we consider family the strong tie for older adults, and community the weak tie. Older adults with good-quality family social capital might be more confident and willing to participate in informal exchanges among neighbors and friends in the communities. Poor family social capital, in contrast, might make older adults feel as though they are “losing face” and decrease the likelihood of trust, reciprocity among neighbors, and the sense of belonging to local communities. On the other hand, compared to informal exchanges among neighbors, older adults are more likely to have wider social connections in social involvements that are organized by formal organizations, such as clubs, volunteering, and civic participation. Therefore, family social capital might not affect older adults’ structural social capital levels.
Therefore, based on social capital theory and the literature reviewed here, we investigated individual-level social determinants of cognitive and structural social capital among older adults in urban China, with a particular emphasis on health and family social capital.
4. Discussion
The relationship between socioeconomic status and social capital varies across different cultures and countries. Empirical evidence on the determinants of social capital in the Eastern Asian contexts is limited. The present study is one of the first attempts to use family social capital and health indicators to explain variations in the latent constructs of cognitive and structural social capital among older populations in an urban Chinese context. The findings not only provide new evidence to social capital theory from a Chinese perspective, but also have important implications for future policy and intervention development around healthy aging.
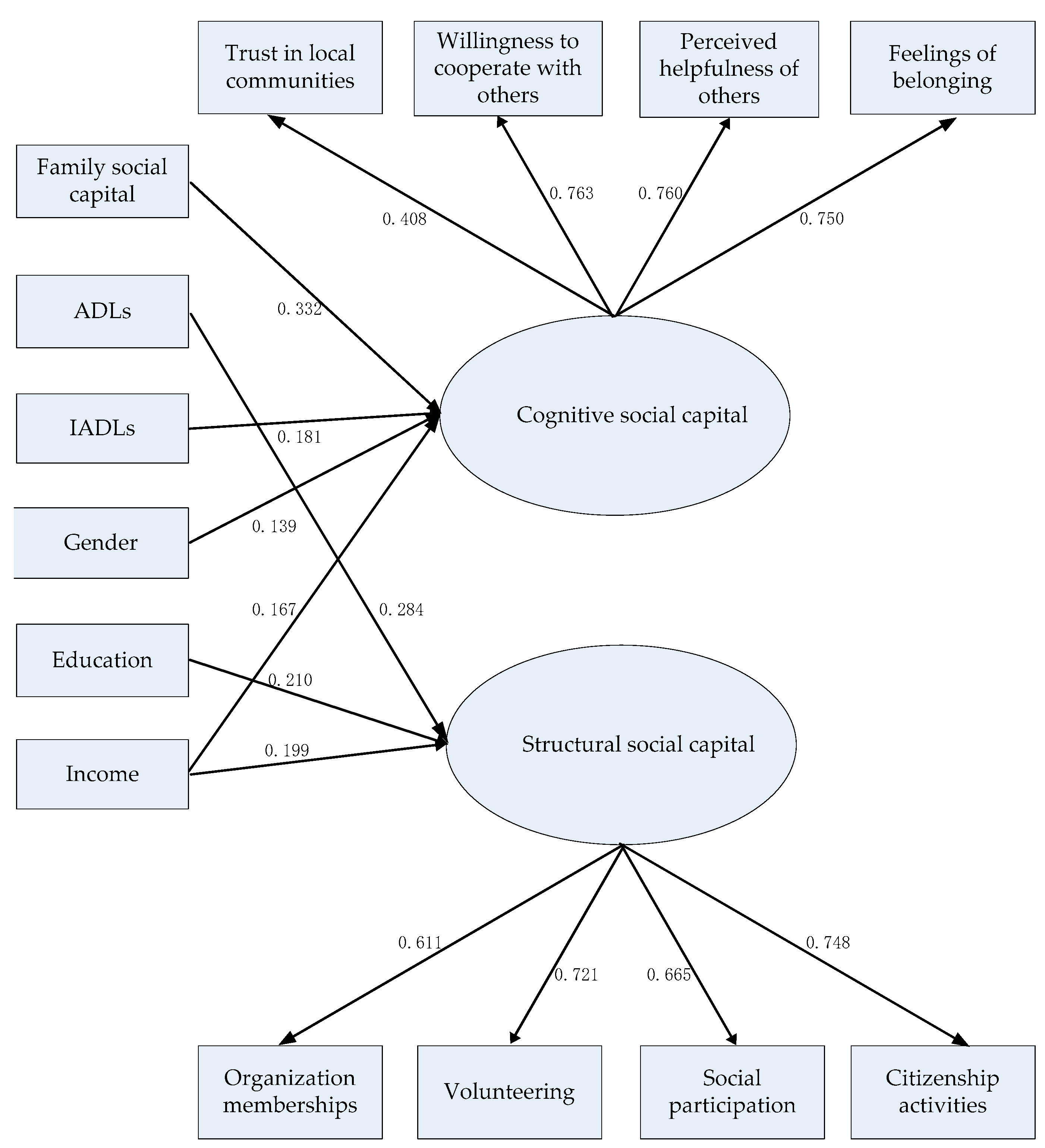
Our findings confirm that eight factor indicators measure two latent variables. These two latent constructs—cognitive and structural social capital—are consistent with the social capital framework. Older adults with more cognitive social capital tend to report more social trust and reciprocity in local communities. In contrast, older adults with more structural social capital have more organization memberships, more frequent social participation, and are involved in more volunteering and citizenship activities. These two latent constructs provide more accurate and comprehensive tools for assessing social capital that could be used in future social work interventions to promote social capital in Chinese contexts.
Consistent with previous studies, income was an influential determinant of both cognitive and structural social capital [
17]. Individuals with higher incomes might be more optimistic than their counterparts, which leads to higher levels of trust, reciprocity, and group memberships. Poverty, in contrast, tends to foster distrust of others and society as a whole. It could also decrease one’s likelihood of being a member of an organization. Furthermore, the findings implied that education was associated with structural social capital only. The consequences of education include social status and adherence to social norms. Education systems provide people with additional access to social connections and foster social values of collaboration [
17,
40]. Education systems also help people be open-minded and develop knowledge and skills for basic social interactions [
18]. These factors increase individuals’ participation in community activities. However, the finding showed that levels of cognitive social capital do not vary across older adults with different educational backgrounds. We conducted a sensitivity analysis by using different cutoff points of education, and generated similar results. The study of Halman and Luijkx [
18] also found that education was not associated with interpersonal trust. The nonsignificant findings might partially be because less than 10% of the respondents had completed a college education. Future studies with larger national representative samples are needed to further examine the effect of education on cognitive social capital, and whether such association vary by cohorts. Furthermore, older women and men, and those with different economic status and educational background, tend to participate in different types of social and civic activities [
16,
21]. It is recommended that future studies examine the above issue and further test the social determinants of social capital through consideration of the contexts of different community organizations.
Furthermore, our findings supported the social selection model [
8]. Consistent with previous studies, health was found to be significantly associated with social capital [
20,
22,
24]. Our findings add new evidence that ADLs are more important for structural social capital, whereas IADLs are more important for cognitive social capital. This might be because ADL limitations could decrease the likelihood of participating in social activities organized by formal organizations. On the other hand, capacities of performing IADL tasks help older adults not only live independently in the community, they also foster informal reciprocity among neighbors and a sense of belonging to local communities. We regressed structural social capital on IADLs, and the results showed that the above association was statistically significant. However, the association became nonsignificant in the final model, after controlling for other determinants. This means that the above association can be explained by other determinants such as ADLs and socioeconomic status. We conducted similar analysis to examine the association between ADLs and cognitive social capital, and reached similar conclusions. Future longitudinal studies are needed to examine the interplay between health trajectories and social capital trajectories. Such findings can provide more in-depth understandings of how health and social capital interact with each other over the life course.
Family social capital was the most influential determinant of cognitive social capital, even after we controlled for sociodemographic characteristics, socioeconomic status, and health variables. The findings indicate that family social capital plays a crucial role in older adults’ social involvements in local communities. Good-quality family social capital fulfills cultural expectations and enhances self-esteem, which (a) makes adults more likely to trust other residents in the local community and become involved in reciprocal exchanges with neighbors, and (b) fosters a sense of belonging in local communities. However, the correlation analysis showed that the association between family social capital and structural social capital was only marginally significant at the 0.1 level. This association became statistically nonsignificant when we controlled for other variables. This means that the relationship between family social capital and structural social capital can be explained by other third variables (i.e., age, socioeconomic status, and ADLs). Future studies are needed to examine the effects of family social capital on social participation in different social organizations. It is also recommended that future studies test regional disparities in terms of the social determinants of social capital in older age.
The present study has the following implications for policy and intervention. Organization membership and citizenship activity are Western-oriented concepts, which reflect individuals’ civic engagements in formal organizations to pursue individual and collective interests. While older Chinese adults are still involved in informal groups, the establishment of measurement models of social capital supports that formal organizations are becoming more important in urban Chinese communities. Older adults share knowledge, information, and social resources in both informal and formal organizations in Suzhou. Policy makers should put great emphasis on promoting the role of formal organizations in enhancing older residents’ independence, autonomy, meaning in life, and senses of attachment and belonging in their communities. Specifically, the latent constructs of cognitive social capital and structural social capital can be used in evaluation programs for community-building programs. Different types of social organizations should be established in the communities so that older adults have adequate access to actively participate in community activities. Neighborhood committees and community social workers could help older adults address their collective interests through promoting volunteering programs and citizenship activities. Social capital programs can be used to meet older adults’ personal and collective interests from a community perspective. To some extent, this is more cost-effective and efficient than programs that provide direct services to individuals. In other words, social capital would play an important role in developing prevention programs targeting the health among older populations, and reducing financial burden in the long-term-care systems in China.
Additionally, older adults of low socioeconomic status and poor health conditions deserve attention from both policy makers and designers of interventions. While this specific population tends to report lower levels of social capital than their counterparts, they might also be the groups that benefit most from the promotion of social capital. In this case, their levels of social capital should be further evaluated in comprehensive needs assessments. Such information is valuable for both anti-poverty policies and long-term care policies. In particular, given the health benefits of volunteering and social participation in later life, interventions that aim to promote structural social capital should pay particular attention to social needs and potential barriers among less educated older adults. Motivational prompts and engagement in team building should be used to explain the health benefits of volunteering, and promote altruism and goal setting [
41,
42].
Moreover, given the different impacts of ADLs and IADLs on community social capital, it is recommended that community social capital can be promoted through rigorously improving the physical environment, facilitating information diffusion and enhancing community service utilization. Furthermore, the findings suggest that interventions that aim to promote family social capital might improve older adults’ levels of cognitive social capital (i.e., individuals’ subjective evaluations of trust and reciprocity in their local communities). However, such interventions might not have significant impacts on their levels of structural social capital (e.g., social participation and group membership). On the other hand, older adults with low levels of family social capital might also experience low levels of community social capital, which means that they could experience double jeopardy. Therefore, the interplay between family social capital and community social capital should not be ignored in future policy strategies and intervention designs.
Despite these strengths, this study has a few limitations. First, the nature of the cross-sectional data did not allow us to examine the direction of causality between family social capital, health status, and community social capital. Based on social capital theory and the relevant literature, we discussed the theoretical rationale for the proposed model. Second, the present study focused on individual-level determinants of social capital in later life. Future studies need to examine macro-level determinants, such as the role of welfare systems, education systems, and labor markets. Third, the data were not randomly selected. As discussed previously, the majority of old urban communities are preserved in the Gusu district of Suzhou city, which leads to relatively high levels of community social capital through strong social trust, informal reciprocity, and the provision of aged care service. The findings of this study should be considered illustrative of older adults living in NORC in urban China. Finally, the latent constructs of social capital should be further tested in other community contexts (e.g., rural areas and small cities). For example, future social capital studies should be conducted in Chinese communities with higher proportions of migrant populations. Low levels of social trust and reciprocity might be identified in these communities. Findings based on NORC can be used as important references for community development programs in other urban Chinese communities.



{kind=link}