Associations of Exposure to Air Pollution with Insulin Resistance: A Systematic Review and Meta-Analysis


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Selection of Studies
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
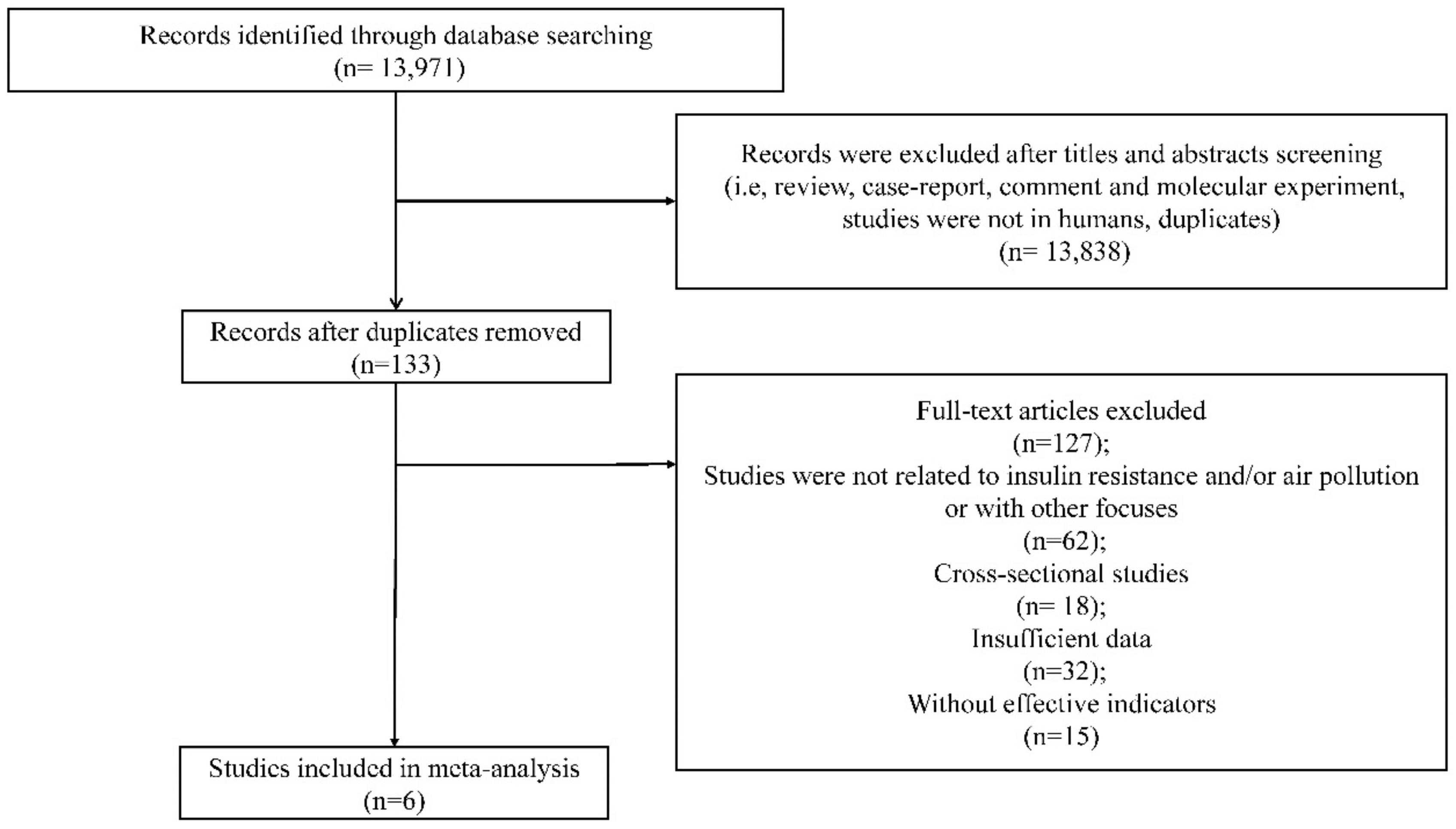
3.1. Literature Retrieval and Study Characteristics
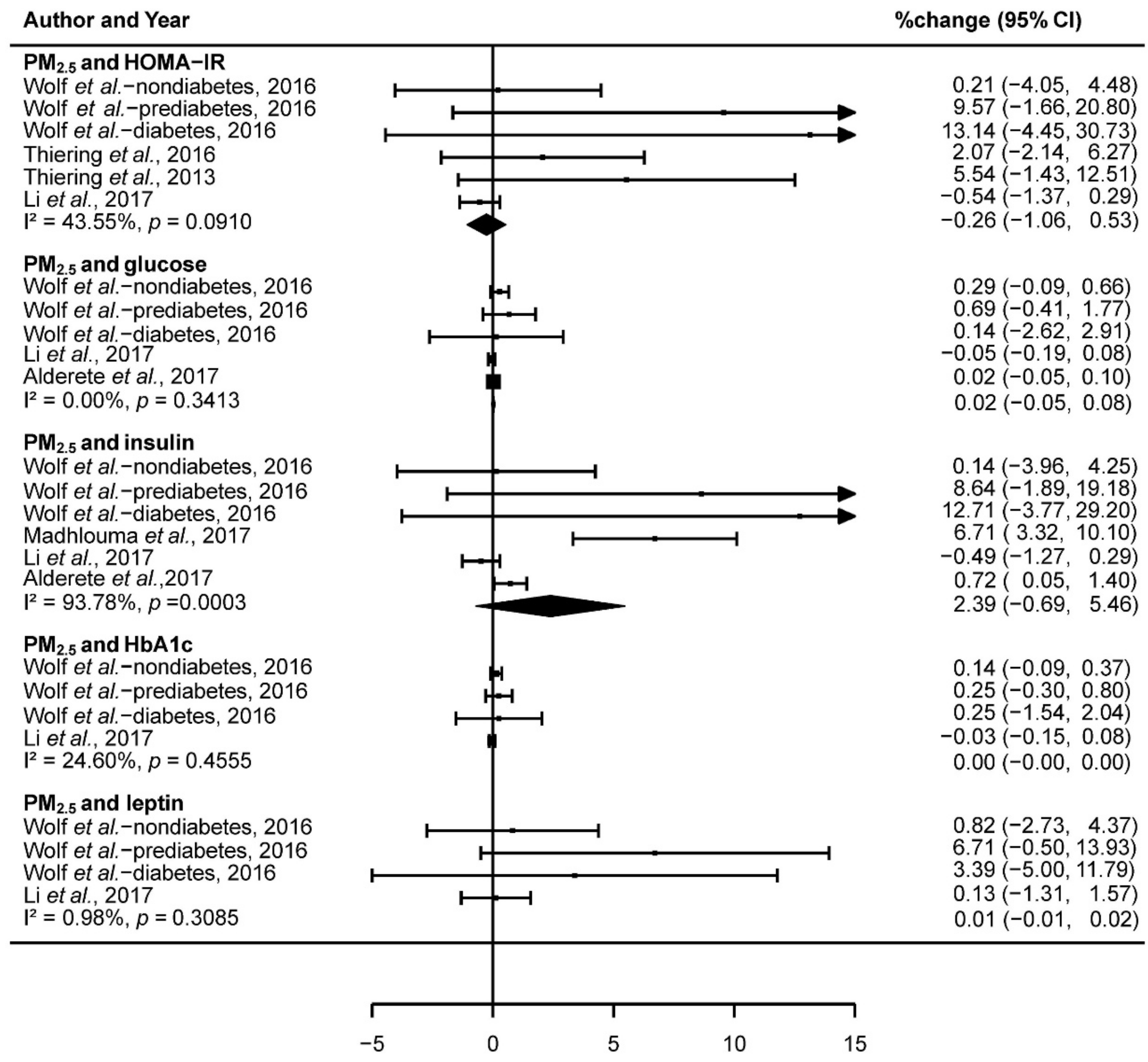
3.2. The Association of Exposure to PM2.5 and IR
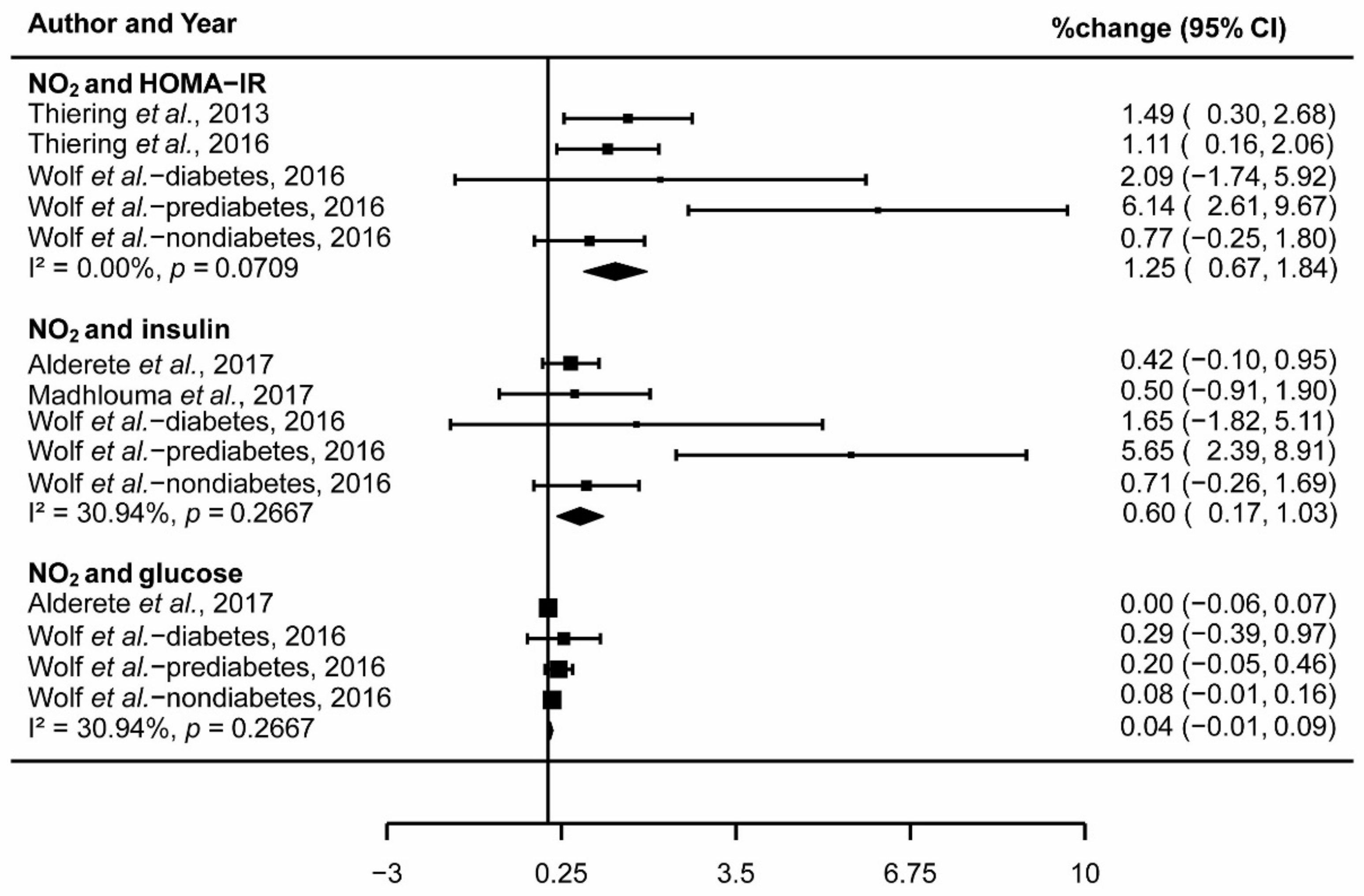
3.3. The Association of Exposure to NO2 and IR
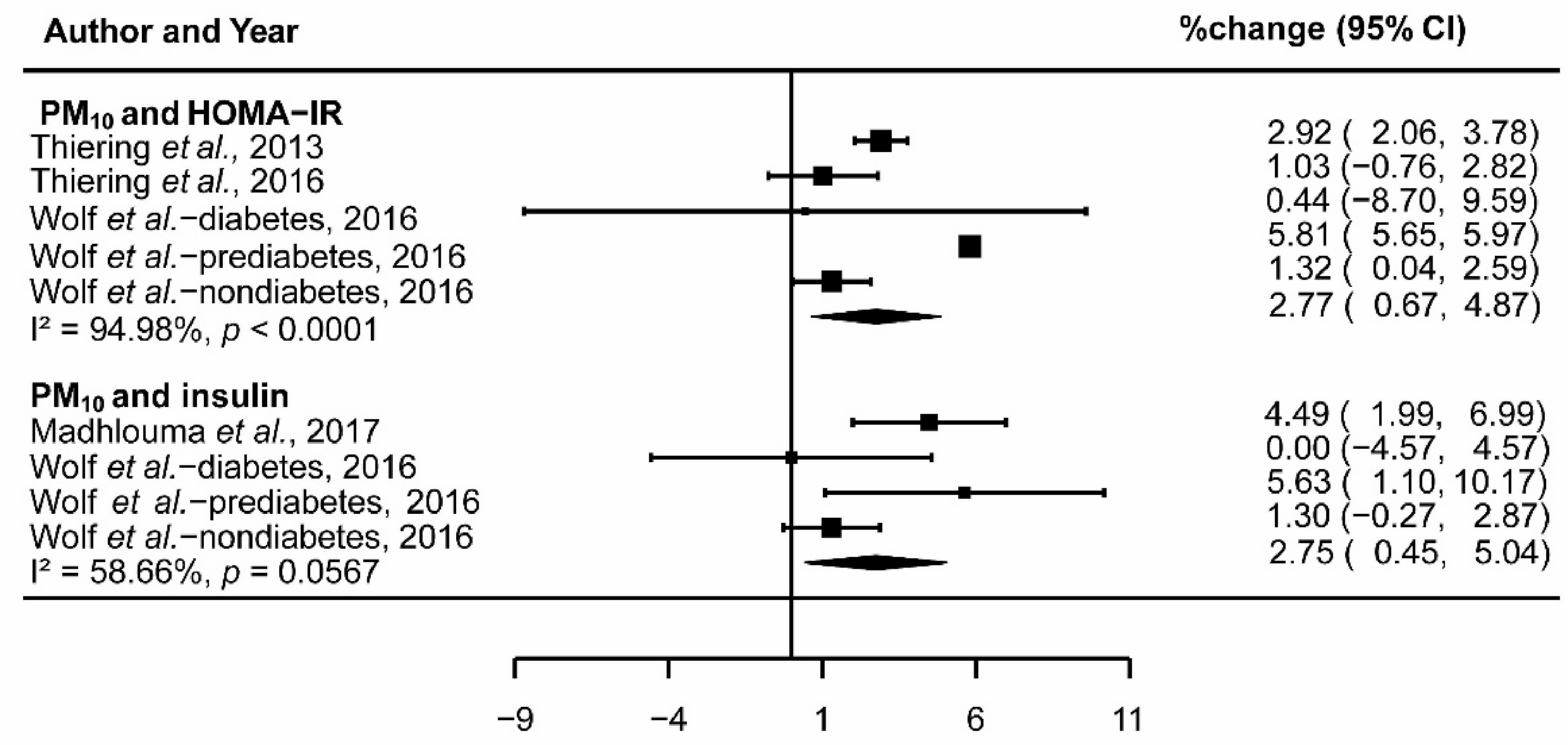
3.4. The Association of Exposure to PM10 and IR
3.5. Sensitivity Analysis
3.6. Meta-Regression
3.7. Publication Bias Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Air Quality Guidelines: Global Update; WHO Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- World Health Organization. Methods for Burden of Disease Attributable to Ambient Air Pollution for the Year 2012; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/phe/health_topics/outdoorair/data-bases/AAP_BoD_methods_March2018.pdf?ua=1 (accessed on 23 March 2018).
- Esposito, K.; Petrizzo, M.; Maiorino, M.I.; Bellastella, G.; Giugliano, D. Particulate matter pollutants and risk of type 2 diabetes: A time for concern? Endocrine 2016, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Suresh, S.; Guo, H.; Weber, R.J.; Ng, N.L. Aerosol characterization over the southeastern United States using high resolution aerosol mass spectrometry: Spatial and seasonal variation of aerosol composition, sources, and organic nitrates. Atmos. Chem. Phys. 2015, 15, 10479–10552. [Google Scholar] [CrossRef]
- Zhang, Q.; Jimenez, J.L.; Canagaratna, M.R.; Allan, J.D.; Coe, H.; Ulbrich, I.; Alfarra, M.R.; Takami, A.; Middlebrook, A.M.; Sun, Y.L. Ubiquity and dominance of oxygenated species in organic aerosols in anthropogenically-influenced Northern Hemisphere midlatitudes. Geophys. Res. Lett. 2007, 34, L13801. [Google Scholar] [CrossRef]
- Donkelaar, A.V.; Martin, R.V.; Brauer, M.; Boys, B.L. Use of Satellite Observations for Long-Term Exposure Assessment of Global Concentrations of Fine Particulate Matter. Environ. Health Perspect. 2015, 123, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Cai, Y.; Zhang, B.; Ke, W.; Feng, B.; Lin, H.; Xiao, J.; Zeng, W.; Li, X.; Tao, J.; Yang, Z.; et al. Associations of Short-Term and Long-Term Exposure to Ambient Air Pollutants With Hypertension: A Systematic Review and Meta-Analysis. Hypertension 2016, 68, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Renzi, M.; Cerza, F.; Gariazzo, C.; Agabiti, N.; Cascini, S.; Di Domenicantonio, R.; Davoli, M.; Forastiere, F.; Cesaroni, G. Air pollution and occurrence of type 2 diabetes in a large cohort study. Environ. Int. 2017, 112, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Balti, E.V.; Echouffotcheugui, J.B.; Yako, Y.Y.; Kengne, A.P. Air pollution and risk of type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2014, 106, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Xu, X.; Bard, R.L.; Dvonch, J.T.; Morishita, M.; Kaciroti, N.; Sun, Q.; Harkema, J.; Rajagopalan, S. Reduced metabolic insulin sensitivity following sub-acute exposures to low levels of ambient fine particulate matter air pollution. Sci. Total Environ. 2013, 448, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.K.; Hong, Y.C. GSTM1, GSTT1, and GSTP1 Polymorphisms and Associations between Air Pollutants and Markers of Insulin Resistance in Elderly Koreans. Environ. Health Perspect. 2012, 120, 1378–1384. [Google Scholar]
- Thiering, E.; Cyrys, J.; Kratzsch, J.; Meisinger, C.; Hoffman, B.; Berdel, D.; von Berg, A.; Koletzko, S.; Bauer, C.P.; Heinrich, J. Long-term exposure to traffic-related air pollution and insulin resistance in children: Results from the GINIplus and LISAplus birth cohorts. Diabetologia 2013, 56, 1696–1704. [Google Scholar] [PubMed]
- Wolf, K.; Popp, A.; Schneider, A.; Breitner, S.; Hampel, R.; Rathmann, W.; Herder, C.; Roden, M.; Koenig, W.; Meisinger, C. Association Between Long-Term Exposure to Air Pollution and Biomarkers Related to Insulin Resistance, Subclinical Inflammation and Adipokines. Diabetes 2016, 65, 3314–3326. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, C.; Storm, H.; Christiansen, C.; Rasmussen, O.W.; Larsen, M.K.; Hermansen, K. The day-to-day variation in insulin sensitivity in non-insulin-dependent diabetes mellitus patients assessed by the hyperinsulinemic-euglycemic clamp method. Metabolism 1997, 46, 374–376. [Google Scholar] [CrossRef]
- Moberg, E.; Kollind, M.; Lins, P.E.; Adamson, U. Day-to-day variation of insulin sensitivity in patients with type 1 diabetes: Role of gender and menstrual cycle. Diabet. Med. 1995, 12, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and fJ-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Karne, R.J.; Chen, H.; Quon, M.J. Diagnosing insulin resistance by simple quantitative methods in subjects with normal glucose metabolism. Diabetes Care 2004, 27, 1247–1248. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Magliano, D.J.; Zimmet, P.Z.; Welborn, T.A.; Colagiuri, S.; Tonkin, A.M.; Shaw, J.E. The metabolic syndrome as a tool for predicting future diabetes: The AusDiab study. J. Intern. Med. 2010, 264, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.H.; Khunti, K.; Achana, F.; Srinivasan, B.; Gray, L.J.; Davies, M.J.; Webb, D. Progression rates from HbA 1c 6.0–6.4% and other prediabetes definitions to type 2 diabetes: A meta-analysis. Diabetologia 2013, 56, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Herder, C.; Roden, M. Genetics of type 2 diabetes: Pathophysiologic and clinical relevance. Eur. J. Clin. Investig. 2011, 41, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Olefsky, J.M.; Glass, C.K. Macrophages, Inflammation, and Insulin Resistance. Annu. Rev. Physiol. 2010, 72, 219–246. [Google Scholar] [CrossRef] [PubMed]
- Peters, A. Epidemiology: Air pollution and mortality from diabetes mellitus. Nature Rev. Endocrinol. 2012, 8, 706–707. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Brook, R.D. Air pollution and type 2 diabetes: Mechanistic insights. Diabetes 2012, 61, 3037–3045. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Yue, P.; Deiuliis, J.A.; Lumeng, C.N.; Kampfrath, T.; Mikolaj, M.B.; Cai, Y.; Ostrowski, M.C.; Lu, B.; Parthasarathy, S. Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation 2009, 119, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Anusree, S.S.; Sindhu, G.; Preetha, M.R.; Raghu, K.G. Insulin resistance in 3T3-L1 adipocytes by TNF-α is improved by punicic acid through upregulation of insulin signalling pathway and endocrine function, and downregulation of proinflammatory cytokines. Biochimie 2018, 146, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Völz, S.; Svedlund, S.; Andersson, B.; Gan, L.M.; Rundqvist, B. Coronary flow reserve in patients with resistant hypertension. Clin. Res. Cardiol. 2017, 106, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Gunji, T.; Matsuhashi, N.; Sato, H.; Iijima, K.; Fujibayashi, K.; Okumura, M.; Sasabe, N.; Urabe, A. Alcohol consumption is inversely correlated with insulin resistance, independent of metabolic syndrome factors and fatty liver diseases. J. Clin. Gastroenterol. 2011, 45, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Probsthensch, N.M. Chronic age-related diseases share risk factors: Do they share pathophysiological mechanisms and why does that matter? Swiss Med. Wkly. 2010, 140, w13072. [Google Scholar]
- Brook, R.D.; Sun, Z.; Brook, J.R.; Zhao, X.; Ruan, Y.; Yan, J.; Mukherjee, B.; Rao, X.; Duan, F.; Sun, L.; et al. Extreme Air Pollution Conditions Adversely Affect Blood Pressure and Insulin Resistance: The Air Pollution and Cardiometabolic Disease Study. Hypertension 2016, 67, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Thiering, E.; Markevych, I.; Brüske, I.; Fuertes, E.; Kratzsch, J.; Sugiri, D.; Hoffmann, B.; Von Berg, A.; Bauer, C.P.; Koletzko, S. Associations of Residential Long-Term Air Pollution Exposures and Satellite-Derived Greenness with Insulin Resistance in German Adolescents. Environ. Health Perspect. 2016, 124, 1291–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichert, T.; Vossoughi, M.; Vierkötter, A.; Sugiri, D.; Schikowski, T.; Schulte, T.; Roden, M.; Luckhaus, C.; Herder, C.; Krämer, U. Association between Traffic-Related Air Pollution, Subclinical Inflammation and Impaired Glucose Metabolism: Results from the SALIA Study. PLoS ONE 2013, 8, e83042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledocorral, C.M.; Alderete, T.L.; Habre, R.; Berhane, K.; Lurmann, F.W.; Weigensberg, M.J.; Goran, M.I.; Gilliland, F.D. Effects of air pollution exposure on glucose metabolism in LosAngeles minority children. Pediatr. Obes. 2016, 13, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Wardcaviness, C.K.; Kraus, W.E.; Blach, C.; Haynes, C.S.; Dowdy, E.; Miranda, M.L.; Devlin, R.B.; Diazsanchez, D.; Cascio, W.E.; Mukerjee, S. Association of Roadway Proximity with Fasting Plasma Glucose and Metabolic Risk Factors for Cardiovascular Disease in a Cross-Sectional Study of Cardiac Catheterization Patients. Environ. Health Perspect. 2015, 123, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Cai, J.; Chen, R.; Zhao, Z.; Ying, Z.; Wang, L.; Chen, J.; Hao, K.; Kinney, P.L.; Chen, H. Particulate Matter Exposure and Stress Hormone Levels: A Randomized, Double-Blind, Crossover Trial of Air Purification. Circulation 2017, 136, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Møller, P.; Loft, S. Oxidative Damage to DNA and Lipids as Biomarkers of Exposure to Air Pollution. Environ. Health Perspect. 2010, 118, 1126–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodovici, M.; Bigagli, E. Oxidative Stress and Air Pollution Exposure. J. Toxicol. 2011, 2011, 487074. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Integrated Science Assessment for Oxides of Nitrogen—Health Criteria; EPA/600/R-15/068; US EPA—Environmental Protection Agency: Washington, DC, USA, 2016.
- Kelishadi, R.; Mirghaffari, N.; Poursafa, P.; Gidding, S.S. Lifestyle and environmental factors associated with inflammation, oxidative stress and insulin resistance in children. Atherosclerosis 2009, 203, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Alderete, T.L.; Habre, R.; Toledocorral, C.M.; Berhane, K.; Chen, Z.; Lurmann, F.W.; Weigensberg, M.J.; Goran, M.I.; Gilliland, F.D. Longitudinal Associations Between Ambient Air Pollution with Insulin Sensitivity, β-Cell Function, and Adiposity in Los Angeles Latino Children. Diabetes 2017, 66, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Madhloum, N.; Janssen, B.G.; Martens, D.S.; Saenen, N.D.; Bijnens, E.; Gyselaers, W.; Penders, J.; Vanpoucke, C.; Lefebvre, W.; Plusquin, M. Cord plasma insulin and in utero exposure to ambient air pollution. Environ. Int. 2017, 105, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, M.; Daneshvar, B.; Hansen, M.; Dragsted, L.O.; Hertel, O.; Knudsen, L.; Loft, S. Personal PM2.5 exposure and markers of oxidative stress in blood. Environ. Health Perspect. 2003, 111, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; Brook, R.; White, L.F.; Burnett, R.T.; Yu, J.; Su, J.; Seto, E.; Marshall, J.; Palmer, J.R.; Rosenberg, L. Ambient ozone and incident diabetes: A prospective analysis in a large cohort of African American women. Environ. Int. 2017, 102, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Ying, Z.; Harkema, J.; Sun, Q.; Rajagopalan, S. Epidemiological and experimental links between air pollution and type 2 diabetes. Toxicol. Pathol. 2013, 41, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, C.; Xu, Z.; Tzan, K.; Zhong, M.; Wang, A.; Lippmann, M.; Chen, L.C.; Rajagopalan, S.; Sun, Q. Long-term exposure to ambient fine particulate pollution induces insulin resistance and mitochondrial alteration in adipose tissue. Toxicol. Sci. 2011, 124, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Xu, X.; Zhang, X.; Wang, A.; Zhang, C.; Hüttemann, M.; Grossman, L.I.; Chen, L.C.; Rajagopalan, S.; Sun, Q. Exposure to Ambient Particulate Matter Induces a NASH-like Phenotype and Impairs Hepatic Glucose Metabolism in an Animal Model. J. Hepatol. 2013, 58, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.J.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. A Appl. Eng. Agric. 2012, 18, 727–734. [Google Scholar]
- Dersimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Normand, S.L. Meta-analysis: Formulating, evaluating, combining, and reporting. Stat. Med. 1999, 18, 321–359. [Google Scholar] [CrossRef]
- Thompson, S.G.; Sharp, S.J. Explaining heterogeneity in meta-analysis: A comparison of methods. Control. Clin. Trials 1999, 18, 2693–2708. [Google Scholar] [CrossRef]
- Stuck, A.E.; Rubenstein, L.Z.; Wieland, D.; Vandenbroucke, J.P.; Irwig, L.; Macaskill, P.; Berry, G.; Glasziou, P.; Seagroatt, V.; Stratton, I. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar]
- Li, W.; Dorans, K.S.; Wilker, E.H.; Rice, M.B.; Kloog, I.; Schwartz, J.D.; Koutrakis, P.; Coull, B.A.; Gold, D.R.; Meigs, J.B. Ambient air pollution, adipokines, and glucose homeostasis: The Framingham Heart Study. Environ. Int. 2017, 111, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Sabin, M.A.; Magnussen, C.G.; Juonala, M.; Shield, J.P.; Kähönen, M.; Lehtimäki, T.; Rönnemaa, T.; Koskinen, J.; Loo, B.M.; Knip, M. Insulin and BMI as predictors of adult type 2 diabetes mellitus. Pediatrics 2015, 135, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Fang, D.; Xu, D.; Wang, B.; Zhao, S.; Yan, S.; Wang, Y. Main air pollutants and diabetes-associated mortality: A systematic review and meta-analysis. Eur. J. Endocrinol. 2014, 171, R183. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A.; Barendregt, J.J.; Williams, G.M.; Khan, S.; Thalib, L. Simulation Comparison of the Quality Effects and Random Effects Methods of Meta-analysis. Epidemiology 2015, 26, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Fleisch, A.F.; Luttmann-Gibson, H.; Perng, W.; Rifas-Shiman, S.L.; Coull, B.A.; Kloog, I.; Koutrakis, P.; Schwartz, J.D.; Zanobetti, A.; Mantzoros, C.S. Prenatal and early life exposure to traffic pollution and cardiometabolic health in childhood. Pediatr. Obes. 2016, 12, 48–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Wang, W. Ambient Air Pollution and Type 2 Diabetes Mellitus: A Systematic Review of Epidemiologic Research. Curr. Environ. Health Rep. 2014, 1, 275–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eze, I.C.; Imboden, M.; Kumar, A.; Von, E.A.; Stolz, D.; Gerbase, M.W.; Künzli, N.; Pons, M.; Kronenberg, F.; Schindler, C. Air pollution and diabetes association: Modification by type 2 diabetes genetic risk score. Environ. Int. 2016, 94, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coogan, P.F.; White, L.F.; Yu, J.; Burnett, R.T.; Marshall, J.D.; Seto, E.; Brook, R.D.; Palmer, J.R.; Rosenberg, L.; Jerrett, M. Long term exposure to NO2 and diabetes incidence in the Black Women’s Health Study. Environ. Res. 2016, 148, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Salam, M.T.; Toledocorral, C.; Watanabe, R.M.; Xiang, A.H.; Buchanan, T.A.; Habre, R.; Bastain, T.M.; Lurmann, F.; Wilson, J.P. Ambient Air Pollutants Have Adverse Effects on Insulin and Glucose Homeostasis in Mexican Americans. Diabetes Care 2016, 39, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, K.J.; Yan, Y.H.; Cheng, T.J. Effect of air pollution on blood pressure, blood lipids, and blood sugar: A population-based approach. J. Occup. Environ. Med. 2010, 52, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.J.; Yan, Y.H.; Chiu, S.Y.; Cheng, T.J. Long-term air pollution exposure and risk factors for cardiovascular diseases among the elderly in Taiwan. Occup. Environ. Med. 2011, 68, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Eliot, M.N.; Kuchel, G.A.; Schwartz, J.; Coull, B.A.; Mittleman, M.A.; Lipsitz, L.A.; Wellenius, G.A. Long-term exposure to ambient air pollution and serum leptin in older adults: Results from the MOBILIZE Boston study. J. Occup. Environ. Med. 2014, 56, 73–77. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Thiering et al. [13] | Wolf et al. [14] | Thiering et al. [31] | Madhloum et al. [41] | Alderete et al. [40] | Li et al. [53] |
|---|---|---|---|---|---|---|
| Published Year | 2013 | 2016 | 2016 | 2017 | 2017 | 2018 |
| Age | 10.2±0.2 | Average age 56.2 | 15 | Newborns | 8~15 | Average age 51 |
| Study country | German | Southern Germany | German | Belgium | USA | US |
| Sample size | 397 | 2944 | 837 | 590 | 314 | 5958 |
| Study period | 10 years | 2006–2008 | 15 years | 2010–2014 | 2001–2012 | 1998–2011 |
| Exposure | NO2, PM10, PM2.5, per 500 m decrease in distance to major road (m) | PM2.5, PM10, PM coarse, nitrogen monoxides (NOx), NO2 | NO2, PM10, PM2.5 | PM2.5, PM10, NO2 | NO2, PM2.5 | PM2.5, traffic-related pollution |
| Exposure assessment (methods) | LUR models were used to estimate long-term spatial variability of NO2, PM10, PM2.5, and PM2.5 absorbance at the birth address of each individual. The concentrations of NO2 were measured at 40 monitoring sites, and concentrations of PM2.5 and filter absorbance of PM2.5 were measured at 20 monitoring sites in Munich-Augsburg and the Ruhr area. The measurement period in Munich was between October 2008 and November 2009, and measurements at all selected sites were carried out three times for 14 consecutive days in different seasons. | Air pollution measurements of PM10, PM2.5, NO2, and the sum of NO2 and nitrogen monoxides (NOx) were collected at 20 (PM) and 40 (NOx) monitoring sites for three periods of two weeks in the cold, warm, and one intermediate season during the period from October 2008 to July 2009. LUR models were then applied to the residence addresses of study participants to assess individual long-term concentrations. | Measurements of particulate matter were conducted at 20 monitoring sites distributed throughout each study area for three, two-week periods in cold, warm, and intermediate temperature seasons between October 2008 and July 2009. For NO2, parallel measurements using these 20 and additional 20 monitoring sites were performed. The annual mean concentrations of the pollutants were estimated for all residences at the time of the 15-year examination (2011–2014) using the European Study of Cohorts for Air Pollution Effects (ESCAPE) area-specific LUR models. | The regional background levels of air pollutants (PM2.5, PM10, NO2) for each mother’s residential address were interpolated using a spatial temporal interpolation method (Kriging) that uses pollution data collected in the official fixed site monitoring network (n = 34) and land-cover data obtained from satellite images (CORINE land-cover data set) in combination with a dispersion model. To explore potentially critical exposures windows during pregnancy, individual mean air pollutant concentrations (micrograms per cubic meter) were calculated for each of the three trimesters of pregnancy, with trimesters being defined as 1–13 weeks (1st trimester), 14–26 weeks (2nd trimester), and 27 weeks to delivery (3rd trimester). | Hourly air quality data from ambient monitoring stations were downloaded from the U.S. Environmental Protection Agency’s Air Quality System (AQS) for the relevant time period and averaged to daily level. Monthly averages were calculated from the daily data using a 75% completeness criterion, and monthly exposure values were spatially interpolated from the air quality monitoring station’s locations to the finest geographic resolution possible (usually parcel-level) based on the participant’s geocoded street level residence using an inverse distance-squared weighting (IDW2) algorithm. | Annual average concentration of PM2.5: ArcGIS software and a hybrid spatial-temporal model were used to estimate PM2.5 concentration at residential address. Short-term exposure assessment: central-site hourly measure of PM2.5 from the Harvard Supersite air pollution monitoring station located on the rooftop of the Francis A. A tapered element oscillating microbalance was used to measure PM2.5. Ambient levels of NOx and O3 were computed by averaging data collected from local state monitors (three for NOx and two for O3) within the Greater Boston area. |
| Measurement period | October 2008~November 2009 | October 2008~July 2009 | October 2008~July 2009 | Three trimesters of pregnancy: 1–13 weeks (1st trimester), 14–26 weeks (2nd trimester), and 27 weeks to delivery (3rd trimester). | - | - |
| Outcome (IR) | HOMA-IR, glucose, and fasting insulin | HOMA-IR, serum glucose, insulin, HbA1c, and leptin | HOMA-IR, glucose, and fasting insulin | Plasma insulin | Glucose and insulin | HOMA-IR, fasting glucose, HbA1c, insulin, and leptin |
| Outcome measurement | Glucose measurements in blood were performed by standard laboratory methods by the individual hospitals. Fasting insulin in serum was measured centrally by a fully mechanized system, LIAISON (DiaSorin, Saluggia, Italy). | Serum glucose was measured using a hexokinase method (GLU Flex; Dade Behring Marburg, Marburg, Germany). Insulin was determined using ELISA kits from Invitrogen (Camarillo, CA). HbA1c was measured with a reverse-phase, cation exchange, high-performance liquid chromatography method (analyzer HA 8160; Menarini Group). Leptin concentrations were assessed using ELISA kits from Mercodia (Uppsala, Sweden). | Glucose measurements in blood were performed by standard laboratory methods by the two individual hospitals. Fasting insulin in serum was measured centrally by a fully mechanized system, LIAISON (DiaSorin, Saluggia, Italy). | Plasma insulin levels (pmol/L) of umbilical cord blood were measured by an electrochemiluminescence immunoassay on a Modular-E170 (Roche, Basel, Switzerland) immunoanalyzer. | Glucose was assayed using a Yellow Springs Instruments analyzer (YSI INC., Yellow Springs, OH). Insulin was assayed using an automated enzyme immunoassay (Tosoh AIA 600 II analyzer, Tosoh Bioscience, Inc., South San Francisco, CA). | Fasting glucose was measured by the hexokinase method twice in each cohort. Insulin was evaluated by commercially available enzyme-linked immunosorbent assay kits from Linco Research (St. Charles, MO) in Third Generation cohort examination 1, and Roche reagents (R&D Systems, Minneapolis, MN) in Offspring cohort examination 8 and Third Generation cohort examination 2. HbA1c was measured by turbidimetric immunoassay in Offspring cohort examination8 and Third Generation cohort examination 2. Leptin was measured using enzyme-linked immunosorbent assay (R&D Systems, Minneapolis, MN) in Third Generation cohort examination 1. |
| Adjusted factors | 1–3, 7 (paternal), 24–29 | 1–4, 16–18 | 1–4, 7 (paternal), 9, 11, 19–23 | 1–4, 7 (paternal), 9, 11, 19–23 | 2, 10, 15, 33–37 | 1 (centered), (1 (centered))2, 2, 4–8, 9(median), 11–14, 38, 39 |
| NOS quality score | 7 | 7 | 6 | 7 | 6 | 8 |
| Pollutants and IR Biomarkers | Percentage change | SE | Z-Egger | p-Egger |
|---|---|---|---|---|
| PM2.5 and HOMA-IR | −0.26 | 0.41 | 2.91 | 0.004 |
| PM2.5 and glucose | 0.02 | 0.03 | 1.19 | 0.23 |
| PM2.5 and insulin | 2.39 | 1.57 | 2.12 | 0.03 |
| PM2.5 and HbA1c | 0.00 | 0.00 | 1.19 | 0.24 |
| PM2.5 and leptin | 0.01 | 0.01 | 1.67 | 0.09 |
| NO2 and HOMA-IR | 1.25 | 0.30 | 2.31 | 0.02 |
| NO2 and glucose | 0.04 | 0.03 | 1.60 | 0.11 |
| NO2 and insulin | 0.60 | 0.22 | 2.39 | 0.02 |
| PM10 and HOMA-IR | 2.77 | 1.07 | −1.18 | 0.24 |
| PM10 and insulin | 2.75 | 1.17 | 0.26 | 0.80 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, J.; Yang, M.; Zhang, X.; Ruan, H.; Qin, G.; Fu, J.; Shen, Z.; Tan, A.; Li, R.; Moore, J. Associations of Exposure to Air Pollution with Insulin Resistance: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2593. https://doi.org/10.3390/ijerph15112593
Dang J, Yang M, Zhang X, Ruan H, Qin G, Fu J, Shen Z, Tan A, Li R, Moore J. Associations of Exposure to Air Pollution with Insulin Resistance: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(11):2593. https://doi.org/10.3390/ijerph15112593
Chicago/Turabian StyleDang, Jiajia, Mengtong Yang, Xinge Zhang, Haotian Ruan, Guiyu Qin, Jialin Fu, Ziqiong Shen, Anran Tan, Rui Li, and Justin Moore. 2018. "Associations of Exposure to Air Pollution with Insulin Resistance: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 11: 2593. https://doi.org/10.3390/ijerph15112593