HIV Infection-Related Care Outcomes among U.S.-Born and Non-U.S.-Born Blacks with Diagnosed HIV in 40 U.S. Areas: The National HIV Surveillance System, 2016

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Collection and Classification
2.2. HIV Infection-Related Care Outcome Measures Defintions
2.3. Statistical Analysis
3. Results
3.1. HIV Infection Diagnoses
3.2. Late-Stage HIV Diagnosis (Stage 3 (AIDS) Classification at the Time of Diagnosis of HIV Infection)
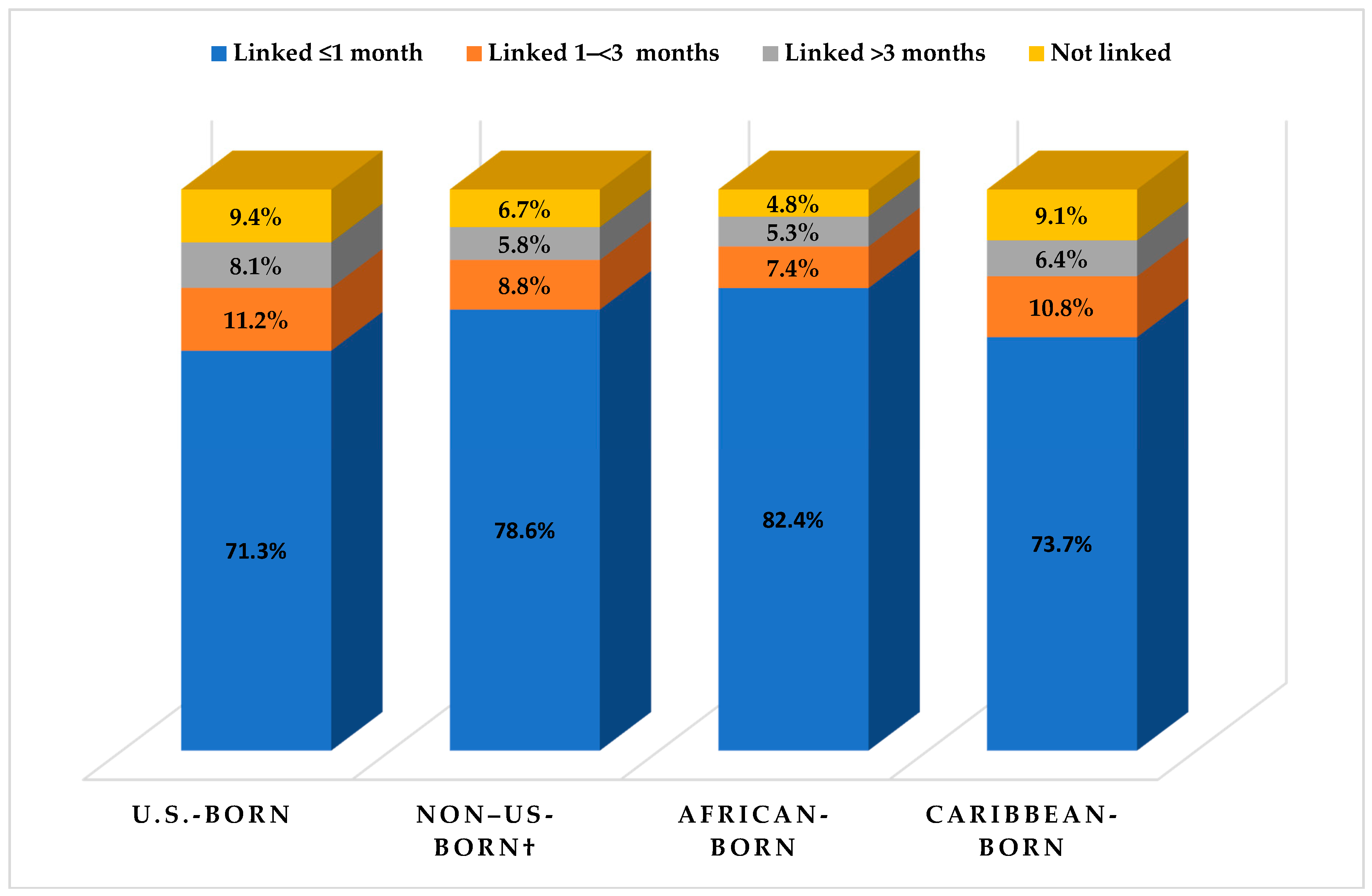
3.3. Linkage to HIV Infection-Related Medical Care
3.4. Retention and Viral Suppression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The White House. National HIV/AIDS Strategy for the United States: Updated to 2020; The White House: Washington, DC, USA, 2015.
- Centers for Disease Control and Prevention (CDC). Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data United States and 6 Dependent Areas, 2016; U.S. Department of Health and Human Services, CDC: Atlanta, GA, USA, 2018. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Diagnoses of HIV Infection in the United States and Dependent Areas, 2016; U.S. Department of Health and Human Services, CDC: Atlanta, GA, USA, 2018. [Google Scholar]
- Dailey, A.F.; Johnson, A.S.; Wu, B. HIV care outcomes among blacks with diagnosed HIV—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.I.; Tang, T.; Johnson, A.S.; Espinoza, L.; Harris, N.; McCray, E. Timing of linkage to care after HIV diagnosis and time to viral suppression. J. Acquir. Immune Defic. Syndr. 2016, 72, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Ku, L.; Jewers, M. Health Care for Immigrant Families: Current Policies and Issues; The Migration Policy Institute: Washington, DC, USA, 2013. [Google Scholar]
- Dey, A.N.; Lucas, J.W. Physical and mental health characteristics of U.S.- and foreign-born adults: United States, 1998–2003. Adv. Data 2006, 369, 1–19. [Google Scholar]
- Derose, K.P.; Jose, J.E.; Lurie, N. Immigrants and health care: Sources of vulnerability. Health Affairs 2007, 26, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Cunningham, C.O.; Hanna, D.B. HIV outcomes among migrants from low-income and middle-income countries living in high-income countries: A review of recent evidence. Curr. Opin. Infect. Dis. 2018, 31, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Okoro, O.N.; Whitson, S.O. HIV risk and barriers to care for African-born immigrant women: A sociocultural outlook. Int. J. Women’s Health 2017, 9, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Demeke, H.B.; Johnson, A.S.; Wu, B.; Nwangwu-Ike, N.; King, H.; Dean, H.D. Differences between U.S.-born and non-U.S.-born black adults reported with diagnosed HIV infection—United States, 2008–2014. J. Immigr. Minor. Health 2018, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Koku, E.F.; Rajab-Gyagenda, W.M.; Korto, M.D.; Morrison, S.D.; Beyene, Y.; Mbajah, J.; Ashton, C. HIV/AIDS among African Immigrants in the U.S.: The need for disaggregating HIV surveillance data by country of birth. J. Health Care Poor Underserved 2016, 27, 1316–1329. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.S.; Hu, X.; Dean, H.D. Epidemiologic differences between native-born and foreign-born black people diagnosed with HIV infection in 33 U.S. states, 2001–2007. Public Health Rep. 2010, 125 (Suppl. 4), 61–69. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. Foreign-Born; U.S. Census Bureau: Washington, DC, USA, 2016. Available online: http://www.census.gov/topics/population/foreign-born/about.html (accessed on 30 July 2018).
- United Nations Department of Economic and Social Affairs. Demographic Yearbook: 2014; United Nations: New York, NY, USA, 2015; Available online: http://www.un-ilibrary.org/population-and-demography/united-nations-demographic-yearbook-2014_f4dbfce9-en-fr (accessed on 30 July 2018).
- U.S. Census Bureau. Geography; U.S. Census Bureau: Washington, DC, USA, 2012. Available online: https://www.census.gov/geo/reference/gtc/gtc_urbanrural.html (accessed on 30 July 2018).
- Ojikutu, B.; Nnaji, C.; Sithole-Berk, J.; Bogart, L.M.; Gona, P. Barriers to HIV testing in black immigrants to the U.S. J. Health Care Poor Underserved 2014, 25, 1052–1066. [Google Scholar] [CrossRef] [PubMed]
- Wafula, E.G.; Snipes, S.A. Barriers to health care access faced by black immigrants in the U.S.: Theoretical considerations and recommendations. J. Immigr. Minor. Health 2014, 16, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Myers, T.R.; Lin, X.; Skarbinski, J. Antiretroviral therapy and viral suppression among foreign-born HIV-infected persons receiving medical care in the United States: A complex sample, cross-sectional survey. Medicine 2016, 95, e3051. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services (HHS). Overview: Ryan White HIV/AIDS Program Clients, 2016; HHS: Rockville, MD, USA, 2018.
- Levison, J.H.; Regan, S.; Khan, I.; Freedberg, K.A. Foreign-born status as a predictor of engagement in HIV care in a large U.S. metropolitan health system. AIDS Care 2017, 29, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Wang, C.C.; Gillani, F.; Alexander, N.; Dufort, E.; Rana, A.; Cu-Uvin, S. The changing face of HIV in pregnancy in Rhode Island 2004–2009. Infect. Dis. Obstet. Gynecol. 2012, 2012, 895047. [Google Scholar] [CrossRef] [PubMed]
- Myles, R.L.; Artstein-McNassar, M.; Dean, H.D.; Bohannon, B.; Melville, S.K.; Yeager, R.; Wheeling, J.; Rose, C.E.; Zhu, J.; Dominguez, K.L. Perinatal HIV prevention outcomes in U.S.-born versus foreign-born blacks, PSD Cohort, 1995–2004. J. Immigr. Minor. Health 2015, 17, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Weiser, J.; Beer, L.; Frazier, E.L.; Patel, R.; Dempsey, A.; Hauck, H.; Skarbinski, J. Service delivery and patient outcomes in Ryan White HIV/AIDS program-funded and -nonfunded health care facilities in the United States. JAMA Intern. Med. 2015, 175, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Bradley, H.; Viall, A.H.; Wortley, P.M.; Dempsey, A.; Hauck, H.; Skarbinski, J. Ryan White HIV/AIDS program assistance and HIV treatment outcomes. Clin. Infect. Dis. 2016, 62, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M. A Rising Share of the U.S. Black Population Is Foreign Born; 9 Percent Are Immigrants; and While Most Are from the Caribbean, Africans Drive Recent Growth; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Foley, E.E. HIV/AIDS and African immigrant women in Philadelphia: Structural and cultural barriers to care. AIDS Care 2005, 17, 1030–1043. [Google Scholar] [CrossRef] [PubMed]
- Myers, T.; Skarbinski, J. Viral suppression among foreign-born HIV-infected persons in the United States: Data from the Medical Monitoring Project, 2009. In Proceedings of the 2014 Conference on Retroviruses and Opportunistic Infections, Boston, MA, USA, 22–25 February 2014. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Estimated HIV Incidence and Prevalence in the United States, 2010–2015; U.S. Department of Health and Human Services, CDC: Atlanta, GA, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | U.S.-Born | Non-U.S.-Born | ||||||
|---|---|---|---|---|---|---|---|---|
| Total No. of Cases | Col% | Late-Stage Diagnosis a | Total No. of Cases | Col% | Late-Stage Diagnosis a | |||
| No. | % | No. | % | |||||
| Total | 9441 | 100 | 1807 | 19.1 | 1744 | 100 | 493 | 28.3 |
| Sex | ||||||||
| Male | 7386 | 78.2 | 1366 | 18.5 | 807 | 46.3 | 268 | 33.2 |
| Female | 2055 | 21.8 | 441 | 21.5 | 937 | 53.7 | 225 | 24.0 |
| Age (years) | ||||||||
| 13‒24 | 2839 | 30.1 | 277 | 9.8 | 143 | 8.2 | 25 | 17.5 |
| 25–34 | 3291 | 34.9 | 543 | 16.5 | 445 | 25.5 | 96 | 21.6 |
| 35–44 | 1364 | 14.4 | 359 | 26.3 | 509 | 29.2 | 175 | 34.4 |
| 44‒54 | 1118 | 11.8 | 343 | 30.7 | 361 | 20.7 | 110 | 30.5 |
| ≥55 | 829 | 8.8 | 285 | 34.4 | 286 | 16.4 | 87 | 30.4 |
| Transmission category (male) b | ||||||||
| Male-to-male sexual contact | 5899 | 79.9 | 994 | 16.9 | 376 | 46.5 | 99 | 26.3 |
| Injection-drug use (IDU) | 264 | 3.6 | 58 | 22.0 | 26 | 3.2 | 13 | 50.0 |
| Male-to-male sexual contact and IDU | 208 | 2.8 | 42 | 20.2 | 8 | 1.0 | 4 | 50.0 |
| Heterosexual contact c | 1005 | 13.6 | 267 | 26.6 | 396 | 49.0 | 151 | 38.1 |
| Other d | 10 | 0.1 | 4 | 40.0 | 2 | 0.2 | 1 | 50.0 |
| Transmission category (female) b | ||||||||
| IDU | 188 | 9.1 | 51 | 27.1 | 32 | 3.4 | 8 | 25.0 |
| Heterosexual contact c | 1860 | 90.5 | 388 | 20.9 | 889 | 94.9 | 214 | 24.1 |
| Other d | 7 | 0.3 | 2 | 28.6 | 16 | 1.7 | 3 | 18.8 |
| Type of residence at the time of diagnosis | ||||||||
| Metropolitan (population ≥500,000 persons) | 7472 | 79.1 | 1348 | 18.0 | 1559 | 89.4 | 444 | 28.5 |
| Urban (population 50,000–499,999 persons) | 1521 | 16.1 | 343 | 22.6 | 150 | 8.6 | 36 | 24.0 |
| Rural (population ≤49,999 persons) | 384 | 4.1 | 104 | 27.1 | 30 | 1.7 | 11 | 36.7 |
| Unknown | 64 | 0.7 | 12 | 18.8 | 5 | 0.3 | 2 | 40.0 |
| World region of birth | ||||||||
| Africa | — | — | — | — | 974 | 55.8 | 274 | 28.1 |
| Caribbean | — | — | — | — | 673 | 38.6 | 187 | 27.8 |
| Other | — | — | — | — | 97 | 5.6 | 32 | 33.0 |
| Characteristic | Percentage of Persons with ≥1 CD4+ Count or Viral Load Test After HIV Diagnosis | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| U.S.-Born | Non-U.S.-Born | |||||||||
| No. | ≤1 month | 1–≤3 months | >3 months | Not Linked | No. | ≤1 month | 1–≤3 months | >3 months | Not Linked | |
| Total | 9441 | 71.3 | 11.2 | 8.1 | 9.4 | 1744 | 78.6 | 8.8 | 5.8 | 6.7 |
| Sex | ||||||||||
| Male | 7386 | 70.4 | 11.5 | 8.4 | 9.6 | 807 | 77.8 | 8.7 | 5.9 | 7.6 |
| Female | 2055 | 74.5 | 9.9 | 7.0 | 8.6 | 937 | 79.3 | 9.0 | 5.8 | 6.0 |
| Age (years) | ||||||||||
| 13‒24 | 2839 | 69.5 | 12.6 | 9.5 | 8.4 | 143 | 77.6 | 11.2 | 6.3 | 4.9 |
| 25–34 | 3291 | 70.4 | 11.6 | 8.9 | 9.1 | 445 | 80.7 | 7.2 | 4.7 | 7.4 |
| 35–44 | 1364 | 71.6 | 10.1 | 7.4 | 10.9 | 509 | 80.2 | 9.2 | 5.5 | 5.1 |
| 44‒54 | 1118 | 75.1 | 8.7 | 4.9 | 11.3 | 361 | 75.1 | 10 | 7.2 | 7.8 |
| ≥55 | 829 | 75.3 | 9.7 | 5.7 | 9.4 | 286 | 77.6 | 8.0 | 6.3 | 8.0 |
| Transmission category (male) a | ||||||||||
| Male-to-male sexual contact | 5899 | 70.8 | 11.6 | 8.5 | 9.0 | 376 | 76.9 | 9.6 | 5.1 | 8.2 |
| Injection-drug use (IDU) | 264 | 72.0 | 7.2 | 6.1 | 14.8 | 26 | 84.6 | 3.8 | 3.8 | 7.7 |
| Male-to-male sexual contact and IDU | 208 | 70.7 | 14.4 | 3.8 | 11.1 | 8 | 87.5 | 12.5 | 0 | 12.5 |
| Heterosexual contact b | 1005 | 67.4 | 11.6 | 9.4 | 11.5 | 396 | 77.8 | 8.1 | 7.1 | 6.8 |
| Other c | 10 | 70 | 0 | 10 | 10 | 2 | 100 | 0 | 0 | 0 |
| Transmission category (female) a | ||||||||||
| IDU | 188 | 75.0 | 8.5 | 8.0 | 9.0 | 32 | 81.3 | 9.4 | 3.1 | 6.3 |
| Heterosexual contact b | 1860 | 74.4 | 10.1 | 6.9 | 8.6 | 889 | 78.9 | 9.1 | 6.0 | 6.1 |
| Other c | 7 | 85.7 | 0 | 0 | 14.3 | 16 | 100 | 0 | 0 | 0 |
| Type of residence at the time of diagnosis | ||||||||||
| Metropolitan (population ≥500,000 persons) | 7472 | 66.6 | 10.6 | 8.2 | 9.5 | 1559 | 78.2 | 9.0 | 6.0 | 6.8 |
| Urban (population 50,000–499,999) | 1521 | 66.7 | 13.2 | 8.0 | 9.9 | 150 | 82.7 | 7.3 | 4.0 | 6.0 |
| Rural (population ≤49,999 persons) | 384 | 76.4 | 14.3 | 6.5 | 5.5 | 30 | 80 | 6.7 | 6.7 | 6.7 |
| Unknown | 64 | 60.9 | 10.9 | 15.6 | 12.5 | 5 | 80 | 20 | 0 | 0 |
| World region of birth | ||||||||||
| Africa | — | — | — | — | — | 974 | 82.4 | 7.4 | 5.3 | 4.8 |
| Caribbean | — | — | — | — | — | 673 | 73.7 | 10.8 | 6.4 | 9.1 |
| Other | — | — | — | — | — | 97 | 74.2 | 9.3 | 7.2 | 9.3 |
| Late-stage diagnosis d | 1807 | 89.7 | 10 | 0.3 | 0.1 | 493 | 90.5 | 7.7 | 1.2 | 0.6 |
| Characteristic | U.S.-Born | Non-U.S.-Born | ||||||
|---|---|---|---|---|---|---|---|---|
| No. | Col% | Retained a (%) | Virally Suppressed (%) | No. | Col% | Retained a (%) | Virally Suppressed a (%) | |
| Total | 10,200 | 100 | 61.1 | 57.8 | 1542 | 100 | 67.8 | 68.7 |
| Sex | ||||||||
| Male | 7891 | 77.4 | 59.7 | 57.2 | 645 | 41.8 | 68.1 | 68.2 |
| Female | 2309 | 22.6 | 65.7 | 60.1 | 897 | 58.2 | 67.7 | 69.0 |
| Age (years) | ||||||||
| 13‒24 | 3097 | 30.4 | 59.0 | 53.6 | 134 | 8.7 | 67.2 | 59.7 |
| 25–34 | 3413 | 33.5 | 59.6 | 57.5 | 401 | 26.0 | 69.1 | 70.6 |
| 35–44 | 1572 | 15.4 | 62.8 | 60.9 | 457 | 29.6 | 67.2 | 71.1 |
| 44‒54 | 1287 | 12.6 | 64.4 | 60.9 | 298 | 19.3 | 70.1 | 70.8 |
| ≥55 | 831 | 8.1 | 66.2 | 64.3 | 252 | 16.3 | 64.7 | 63.5 |
| Transmission category (male) b | ||||||||
| Male-to-male sexual contact | 6355 | 80.5 | 60.5 | 58.0 | 298 | 46.3 | 67.8 | 70.5 |
| Injection-drug use (IDU) | 293 | 3.7 | 55.3 | 52.2 | 28 | 4.3 | 60.7 | 67.9 |
| Male-to-male sexual contact and IDU | 239 | 3.0 | 56.9 | 47.3 | 7 | 1.1 | 71.4 | 57.1 |
| Heterosexual contact c | 994 | 12.6 | 56.7 | 56.0 | 307 | 47.7 | 68.7 | 66.4 |
| Other d | 11 | 0.1 | 45.5 | 36.4 | 4 | 0.6 | 50.0 | 75.0 |
| Transmission category (female) b | ||||||||
| IDU | 233 | 10.1 | 63.1 | 55.8 | 34 | 3.8 | 61.8 | 64.7 |
| Heterosexual contact c | 2070 | 89.6 | 65.9 | 60.6 | 852 | 95.0 | 68.0 | 69.4 |
| Other d | 6 | 0.3 | 50.0 | 50.0 | 11 | 1.2 | 63.6 | 54.5 |
| Type of residence at the time of diagnosis | ||||||||
| Metropolitan (Population ≥500,000 persons) | 7781 | 76.3 | 60.1 | 57.2 | 1366 | 88.6 | 67.2 | 67.8 |
| Urban (Population 50,000–499,999) | 1565 | 15.3 | 62.8 | 58.1 | 112 | 7.3 | 74.1 | 77.7 |
| Rural (Population ≤49,999) | 385 | 3.8 | 67.3 | 61.6 | 15 | 1.0 | 66.7 | 66.7 |
| Unknown | 469 | 4.6 | 65.2 | 63.5 | 49 | 3.2 | 71.4 | 73.5 |
| World region of birth | ||||||||
| Africa | — | — | — | — | 899 | 58.3 | 64.8 | 68.6 |
| Caribbean | — | — | — | — | 565 | 36.6 | 72.6 | 68.3 |
| Other | — | — | — | — | 78 | 5.1 | 67.9 | 71.8 |
| Late-stage diagnosis e | 2011 | 19.7 | 78.4 | 71.2 | 416 | 27.0 | 77.4 | 73.8 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demeke, H.B.; Johnson, A.S.; Zhu, H.; Gant, Z.; Duffus, W.A.; Dean, H.D. HIV Infection-Related Care Outcomes among U.S.-Born and Non-U.S.-Born Blacks with Diagnosed HIV in 40 U.S. Areas: The National HIV Surveillance System, 2016. Int. J. Environ. Res. Public Health 2018, 15, 2404. https://doi.org/10.3390/ijerph15112404
Demeke HB, Johnson AS, Zhu H, Gant Z, Duffus WA, Dean HD. HIV Infection-Related Care Outcomes among U.S.-Born and Non-U.S.-Born Blacks with Diagnosed HIV in 40 U.S. Areas: The National HIV Surveillance System, 2016. International Journal of Environmental Research and Public Health. 2018; 15(11):2404. https://doi.org/10.3390/ijerph15112404
Chicago/Turabian StyleDemeke, Hanna B., Anna S. Johnson, Hong Zhu, Zanetta Gant, Wayne A. Duffus, and Hazel D. Dean. 2018. "HIV Infection-Related Care Outcomes among U.S.-Born and Non-U.S.-Born Blacks with Diagnosed HIV in 40 U.S. Areas: The National HIV Surveillance System, 2016" International Journal of Environmental Research and Public Health 15, no. 11: 2404. https://doi.org/10.3390/ijerph15112404