The Use of Antidepressive Agents and Bone Mineral Density in Women: A Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
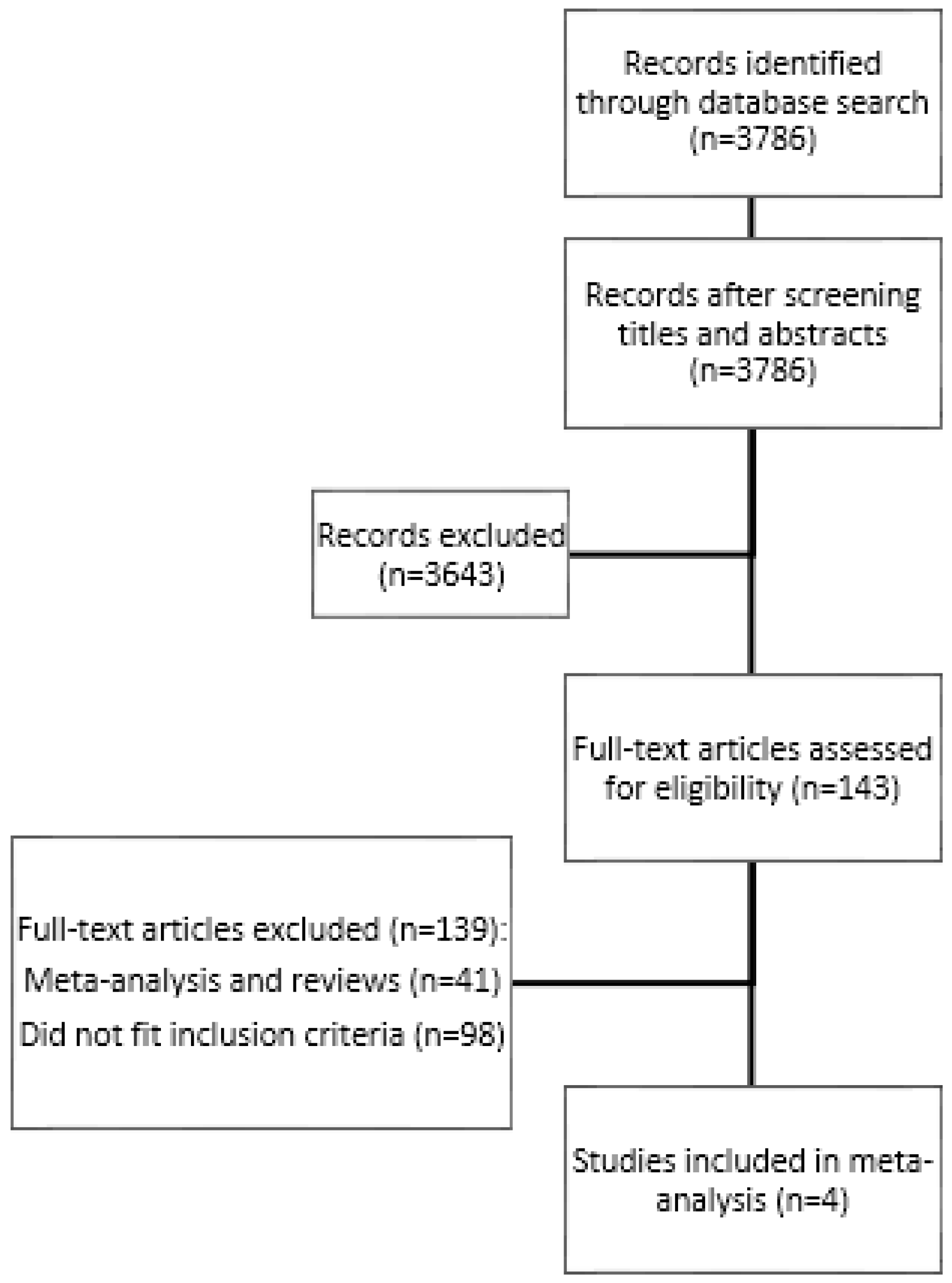
2. Methods
2.1. Sample of Studies
2.2. Data Extraction
2.3. Statistical Analyses
3. Results
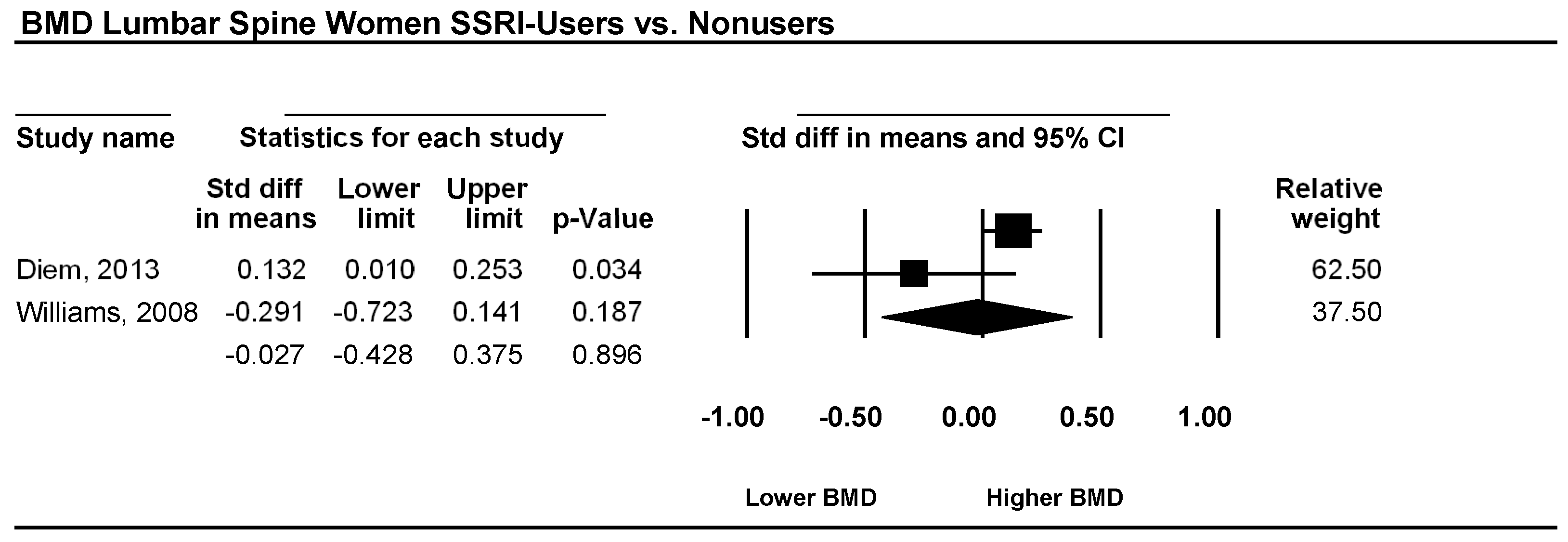
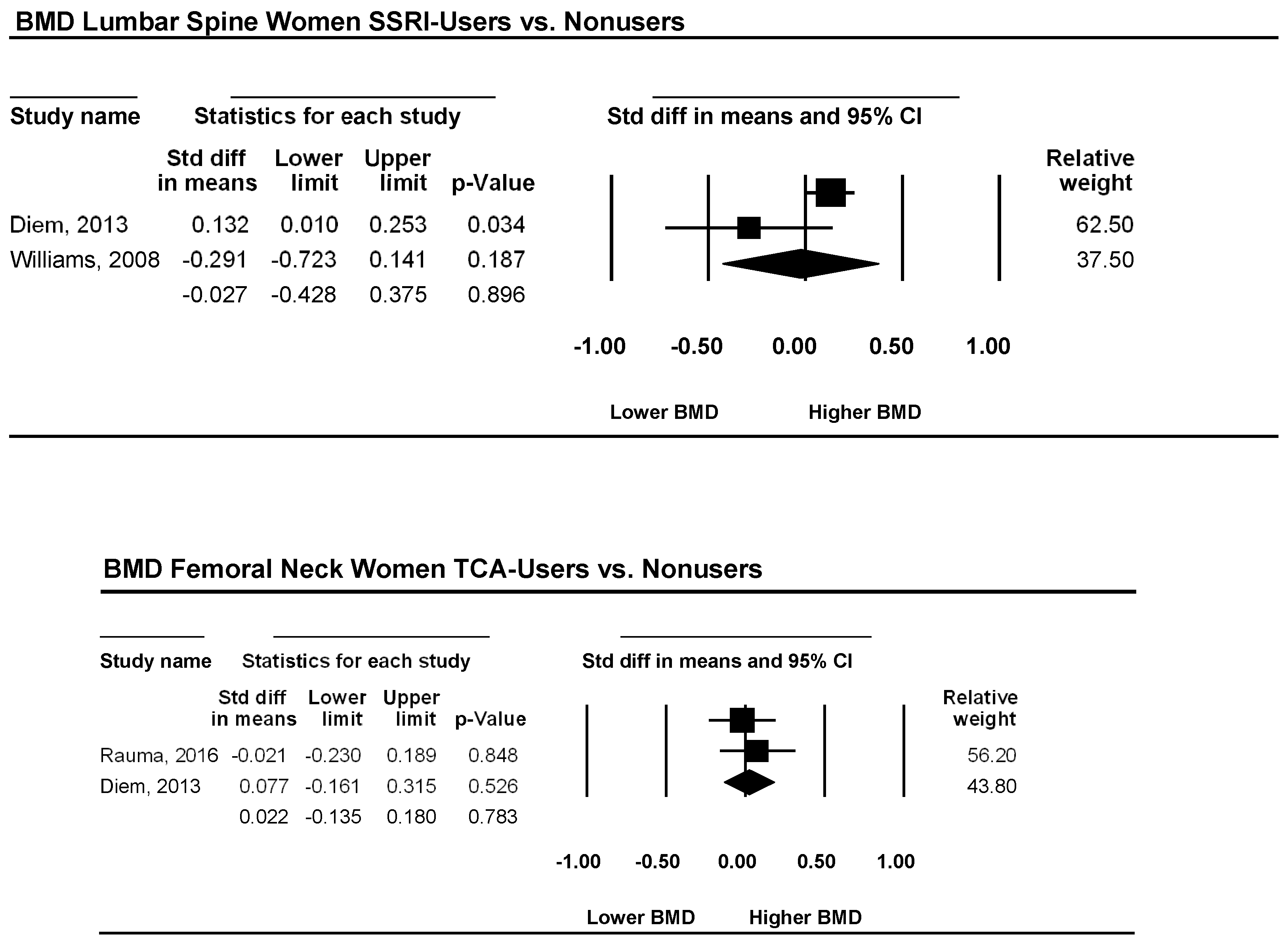
3.1. Lumbar Spine
3.2. Femoral Neck
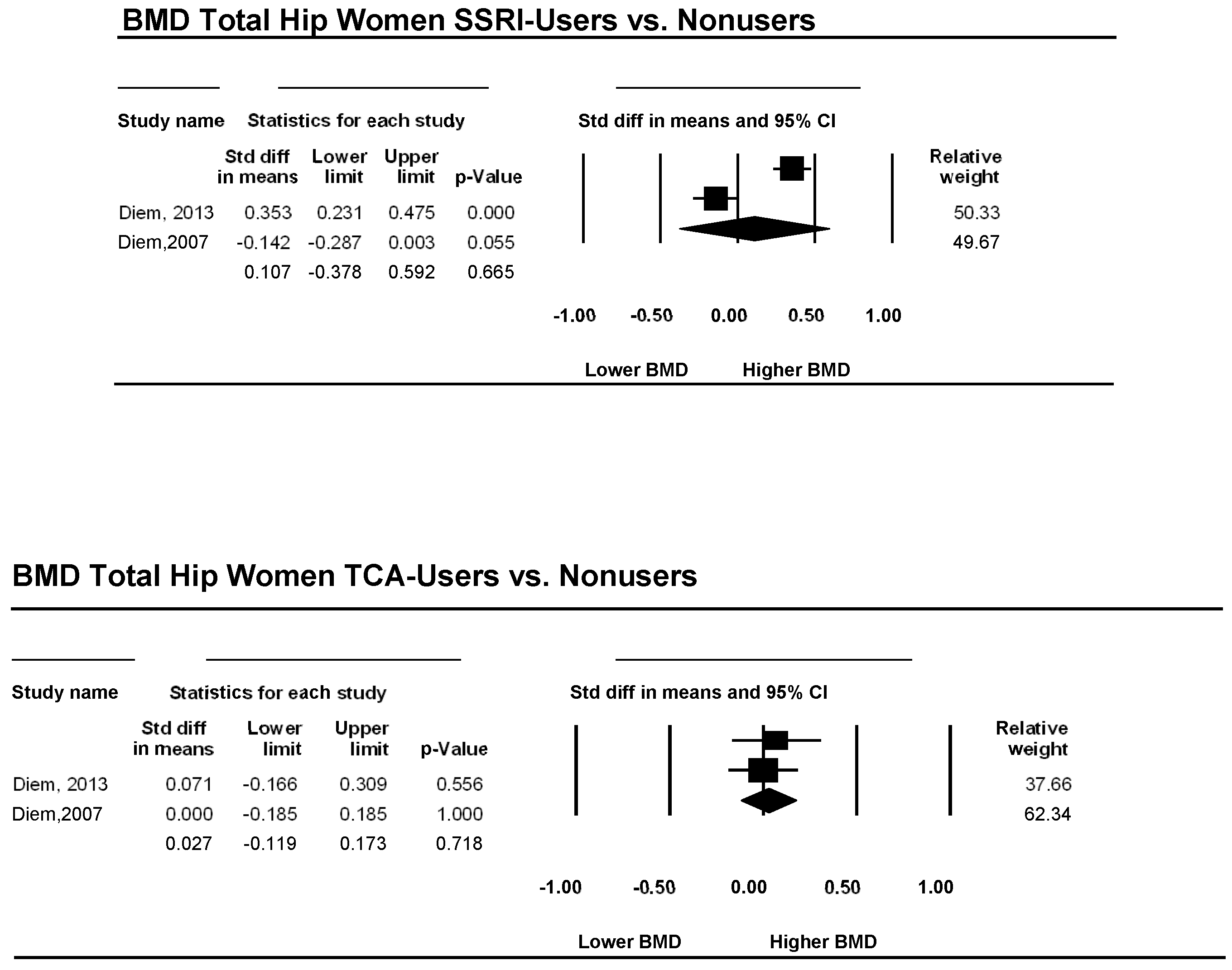
3.3. Total Hip
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Aitken, M.; Kleinrock, M.; Lyle, J.; Nass, D.; Caskey, L. Medicines Use and Spending Shifts: A Review of the Use of Medicines in the US in 2014; IMS Institute for Healthcare Informatics: Parsippany, NJ, USA, 2015. [Google Scholar]
- Olfson, M.; Marcus, S.C. National patterns in antidepressant medication treatment. Arch. Gen. Psychiatry 2009, 66, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Noordam, R.; Aarts, N.; Verhamme, K.M.; Sturkenboom, M.C.; Stricker, B.H.; Visser, L.E. Prescription and indication trends of antidepressant drugs in the netherlands between 1996 and 2012: A dynamic population-based study. Eur. J. Clin. Pharmacol. 2015, 71, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Lewer, D.; O’Reilly, C.; Mojtabai, R.; Evans-Lacko, S. Antidepressant use in 27 european countries: Associations with sociodemographic, cultural and economic factors. Br. J. Psychiatry 2015, 207, 221–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, G.E.; Stewart, C.; Beck, A.; Ahmedani, B.K.; Coleman, K.J.; Whitebird, R.R.; Lynch, F.; Owen-Smith, A.A.; Waitzfelder, B.E.; Soumerai, S.B.; et al. National prevalence of receipt of antidepressant prescriptions by persons without a psychiatric diagnosis. Psychiatr. Serv. 2014, 65, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Wade, S.W.; Strader, C.; Fitzpatrick, L.A.; Anthony, M.S.; O’Malley, C.D. Estimating prevalence of osteoporosis: Examples from industrialized countries. Arch. Osteoporos. 2014, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Golob, A.L.; Laya, M.B. Osteoporosis: Screening, prevention, and management. Med. Clin. N. Am. 2015, 99, 587–606. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.B.; Baggesen, L.M.; Ehrenstein, V.; Pedersen, L.; Lasgaard, M.; Mikkelsen, E.M. Perceived stress and risk of any osteoporotic fracture. Osteoporos. Int. 2016, 27, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Von Friesendorff, M.; McGuigan, F.E.; Wizert, A.; Rogmark, C.; Holmberg, A.H.; Woolf, A.D.; Akesson, K. Hip fracture, mortality risk, and cause of death over two decades. Osteoporos. Int. 2016, 27, 2945–2953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisani, P.; Renna, M.D.; Conversano, F.; Casciaro, E.; Di Paola, M.; Quarta, E.; Muratore, M.; Casciaro, S. Major osteoporotic fragility fractures: Risk factor updates and societal impact. World J. Orthop. 2016, 7, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Pratt, L.A.; Brody, D.J. Depression in the U.S. Household population, 2009–2012. NCHS Data Brief 2014, 172, 1–8. [Google Scholar]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 386, 743–800. [Google Scholar]
- Kessler, R.C.; Bromet, E.J. The epidemiology of depression across cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, J.U.; Schweiger, U.; Hüppe, M.; Kahl, K.G.; Greggersen, W.; Fassbinder, E. Bone density and depressive disorder: A meta-analysis. Brain Behav. 2016, 6, e00489. [Google Scholar] [CrossRef] [PubMed]
- Yirmiya, R.; Bab, I. Major depression is a risk factor for low bone mineral density: A meta-analysis. Biol. Psychiatry 2009, 66, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Mezuk, B.; Eaton, W.W.; Golden, S.H. Depression and osteoporosis: Epidemiology and potential mediating pathways. Osteoporos. Int. 2008, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cizza, G.; Primma, S.; Coyle, M.; Gourgiotis, L.; Csako, G. Depression and osteoporosis: A research synthesis with meta-analysis. Horm. Metab. Res. 2010, 42, 467–482. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Magnus, J.H.; Liu, J.; Bencaz, A.F.; Hentz, J.G. Depression and low bone mineral density: A meta-analysis of epidemiologic studies. Osteoporos. Int. 2009, 20, 1309–1320. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.L.; Lin, C.C. Advances in biomarkers of major depressive disorder. Adv. Clin. Chem. 2015, 68, 177–204. [Google Scholar] [PubMed]
- Osella, G.; Ventura, M.; Ardito, A.; Allasino, B.; Termine, A.; Saba, L.; Vitetta, R.; Terzolo, M.; Angeli, A. Cortisol secretion, bone health, and bone loss: A cross-sectional and prospective study in normal non-osteoporotic women in the early postmenopausal period. Eur. J. Endocrinol. 2012, 166, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Young, J.J.; Bruno, D.; Pomara, N. A review of the relationship between proinflammatory cytokines and major depressive disorder. J. Affect. Disord. 2014, 169, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.M.; Kim, K.W.; Yang, C.W.; Park, S.H.; Ju, J.H. Cytokine-mediated bone destruction in rheumatoid arthritis. J. Immunol. Res. 2014, 2014, 263625. [Google Scholar] [CrossRef] [PubMed]
- Villareal, D.T.; Fontana, L.; Das, S.K.; Redman, L.; Smith, S.R.; Saltzman, E.; Bales, C.; Rochon, J.; Pieper, C.; Huang, M.; et al. Effect of two-year caloric restriction on bone metabolism and bone mineral density in non-obese younger adults: A randomized clinical trial. J. Bone Miner. Res. 2015, 31, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Dorn, L.D.; Pabst, S.; Sontag, L.M.; Kalkwarf, H.J.; Hillman, J.B.; Susman, E.J. Bone mass, depressive, and anxiety symptoms in adolescent girls: Variation by smoking and alcohol use. J. Adolesc. Health 2011, 49, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Brot, C.; Jorgensen, N.R.; Sorensen, O.H. The influence of smoking on vitamin d status and calcium metabolism. Eur. J. Clin. Nutr. 1999, 53, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; van Wijngaarden, J.P. The role of B-vitamins in bone health and disease in older adults. Curr. Osteoporos. Rep. 2015, 13, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Cohn, A.M.; Cobb, C.; Hagman, B.T.; Cameron, A.; Ehlke, S.; Mitchell, J.N. Implicit alcohol cognitions in risky drinking nicotine users with and without co-morbid major depressive disorder. Addict. Behav. 2014, 39, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghadir, A.H.; Gabr, S.A.; Al-Eisa, E. Physical activity and lifestyle effects on bone mineral density among young adults: Sociodemographic and biochemical analysis. J. Phys. Ther. Sci. 2015, 27, 2261–2270. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Nakamura, T.; Kikuchi, H.; Yoshiuchi, K.; Sasaki, T.; Yamamoto, Y. Covariation of depressive mood and spontaneous physical activity in major depressive disorder: Toward continuous monitoring of depressive mood. IEEE J. Biomed. Health Inform. 2015, 19, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Sheu, Y.H.; Lanteigne, A.; Sturmer, T.; Pate, V.; Azrael, D.; Miller, M. SSRI use and risk of fractures among perimenopausal women without mental disorders. Inj. Prev. 2015, 21, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Quiros-Gonzalez, I.; Yadav, V.K. Central genes, pathways and modules that regulate bone mass. Arch. Biochem. Biophys. 2014, 561, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Karg, K.; Burmeister, M.; Shedden, K.; Sen, S. The serotonin transporter promoter variant (5-HTTLPR), stress, and depression meta-analysis revisited: Evidence of genetic moderation. Arch. Gen. Psychiatry 2011, 68, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Bliziotes, M. Update in serotonin and bone. J. Clin. Endocrinol. Metab. 2010, 95, 4124–4132. [Google Scholar] [CrossRef] [PubMed]
- Warden, S.J.; Robling, A.G.; Haney, E.M.; Turner, C.H.; Bliziotes, M.M. The emerging role of serotonin (5-hydroxytryptamine) in the skeleton and its mediation of the skeletal effects of low-density lipoprotein receptor-related protein 5 (LRP5). Bone 2010, 46, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: Chichester, UK, 2009. [Google Scholar]
- Williams, L.J.; Henry, M.J.; Berk, M.; Dodd, S.; Jacka, F.N.; Kotowicz, M.A.; Nicholson, G.C.; Pasco, J.A. Selective serotonin reuptake inhibitor use and bone mineral density in women with a history of depression. Int. Clin. Psychopharmacol. 2008, 23, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Diem, S.J.; Ruppert, K.; Cauley, J.A.; Lian, Y.; Bromberger, J.T.; Finkelstein, J.S.; Greendale, G.A.; Solomon, D.H. Rates of bone loss among women initiating antidepressant medication use in midlife. J. Clin. Endocrinol. Metab. 2013, 98, 4355–4363. [Google Scholar] [CrossRef] [PubMed]
- Rauma, P.H.; Honkanen, R.J.; Williams, L.J.; Tuppurainen, M.T.; Kroger, H.P.; Koivumaa-Honkanen, H. Effects of antidepressants on postmenopausal bone loss—A 5-year longitudinal study from the ostpre cohort. Bone 2016, 89, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Diem, S.J.; Blackwell, T.L.; Stone, K.L.; Yaffe, K.; Haney, E.M.; Bliziotes, M.M.; Ensrud, K.E. Use of antidepressants and rates of hip bone loss in older women: The study of osteoporotic fractures. Arch. Intern. Med. 2007, 167, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Knorr, U.; Vinberg, M.; Gether, U.; Winkel, P.; Gluud, C.; Wetterslev, J.; Kessing, L.V. The effect of escitalopram versus placebo on perceived stress and salivary cortisol in healthy first-degree relatives of patients with depression—A randomised trial. Psychiatry Res. 2012, 200, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Moura, C.; Bernatsky, S.; Abrahamowicz, M.; Papaioannou, A.; Bessette, L.; Adachi, J.; Goltzman, D.; Prior, J.; Kreiger, N.; Towheed, T.; et al. Antidepressant use and 10-year incident fracture risk: The population-based canadian multicentre osteoporosis study (CaMoS). Osteoporos. Int. 2014, 25, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.B.; Papaioannou, A.; Adachi, J.D.; Joseph, L.; Whitson, H.E.; Prior, J.C.; Goltzman, D. Effect of selective serotonin reuptake inhibitors on the risk of fracture. Arch. Intern. Med. 2007, 167, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Hegeman, J.; van den Bemt, B.; Weerdesteyn, V.; Nienhuis, B.; van Limbeek, J.; Duysens, J. Unraveling the association between SSRI use and falls: An experimental study of risk factors for accidental falls in long-term paroxetine users. Clin. Neuropharmacol. 2011, 34, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Wadhwa, R.; Kothari, P.; Trivedi, R.; Vohora, D. Differential effects of serotonin reuptake inhibitors fluoxetine and escitalopram on bone markers and microarchitecture in Wistar rats. Eur. J. Pharmacol. 2018, 825, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Manske, S.L.; Zhu, Y.; Sandino, C.; Boyd, S.K. Human trabecular bone microarchitecture can be assessed independently of density with second generation HR-pQCT. Bone 2015, 79, 213–221. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Name | Year | Country | User/Nonuser Subjects (n) | Age (User/Nonuser) | Menopausal Status | Drugs | Bone Site |
|---|---|---|---|---|---|---|---|
| P.H. Rauma et al. | 2016 | Finland | 210/1669 | 63.4/63.7 | Post | SSRI, TCA, Others | Femur |
| S. J. Diem et al. | 2013 | US | 382/1590 | 49.6/49.7 | Pre/Post | SSRI, TCA | Lumbar, Femur, Hip |
| L.J. Williams et al. | 2008 | Australia | 26/102 | 57.5/51 | Pre/Post | SSRI | Lumbar, Femur |
| S. J. Diem et al. | 2007 | US | 316/2406 | 78.4/78.6 | Post | SSRI, TCA | Hip |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweiger, J.U.; Schweiger, U.; Hüppe, M.; Kahl, K.G.; Greggersen, W.; Jauch-Chara, K.; Fassbinder, E. The Use of Antidepressive Agents and Bone Mineral Density in Women: A Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1373. https://doi.org/10.3390/ijerph15071373
Schweiger JU, Schweiger U, Hüppe M, Kahl KG, Greggersen W, Jauch-Chara K, Fassbinder E. The Use of Antidepressive Agents and Bone Mineral Density in Women: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(7):1373. https://doi.org/10.3390/ijerph15071373
Chicago/Turabian StyleSchweiger, Julietta Ursula, Ulrich Schweiger, Michael Hüppe, Kai G. Kahl, Wiebke Greggersen, Kamila Jauch-Chara, and Eva Fassbinder. 2018. "The Use of Antidepressive Agents and Bone Mineral Density in Women: A Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 7: 1373. https://doi.org/10.3390/ijerph15071373