
A Brief Cognitive-Behavioral Psycho-Education (B-CBE) Program for Managing Stress and Anxiety of Main Family Caregivers of Patients in the Intensive Care Unit

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Theoretical Framework and the B-CBE
2.2. Instruments
2.2.1. Demographic Data Sheet
2.2.2. Depression Anxiety Stress Scale-Chinese (C-DASS)
2.2.3. Critical Care Family Need Inventory-Chinese (C-CCFNI)
2.2.4. Automatic Thoughts Questionnaire-Chinese (C-ATQ)
2.3. Setting and Sampling
2.4. Procedures
2.5. Data Analysis
3. Results
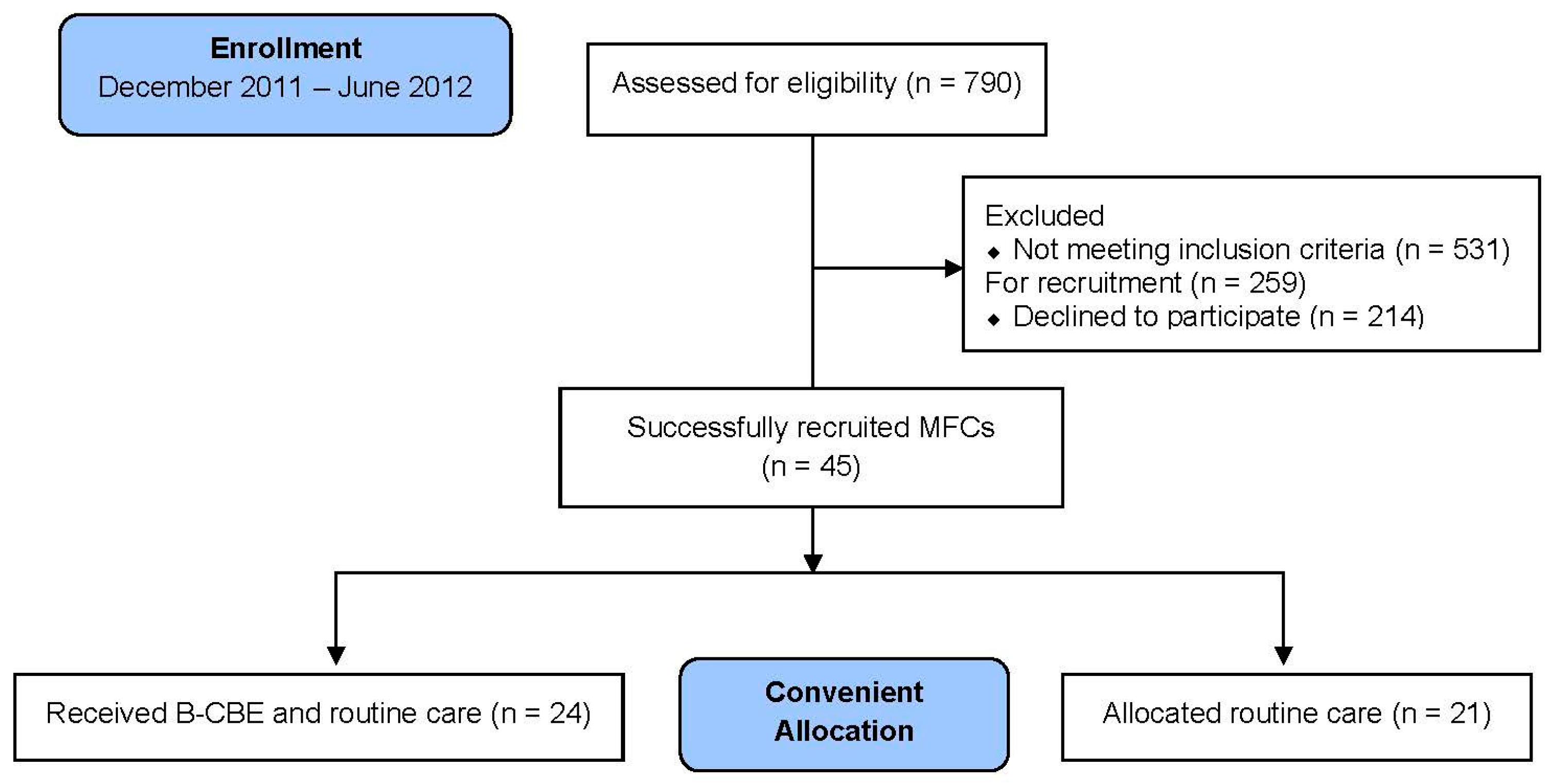
3.1. Enrollment of Participants
3.2. Comparison between the B-CBE and Routine Care Groups at T0
3.3. Split-Plot ANOVA Analysis on the Pre-Post Measurements
4. Discussion
4.1. Recruitment Process, Feasibility, and the Need of Family Caregivers
4.2. Pre-Post Measurements Comparison
4.3. The Difference of Patients’ Health Conditions between the Two Groups
4.4. Other Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| APACHE | Acute physiology and chronic health evaluation |
| AT | Automatic thoughts |
| B-CBE | Brief cognitive-behavioral psycho-education program |
| CB | Cognitive-behavioral |
| C-DASS | Depression anxiety stress scale—Chinese |
| C-CCFNI | Critical care family need inventory—Chinese |
| C-ATQ | Automatic thoughts questionnaire—Chinese |
| FSEM | Five steps of emotion management |
| ICU | Intensive care unit |
| MFC | Main family caregiver |
| RCT | Randomized control trail |
References
- Chiang, V.C. Surviving a critical illness through mutually being there with each other: A grounded theory study. Intensive Crit. Care Nurs. 2011, 27, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Van Horn, E.; Tesh, A. The effect of critical care hospitalization on family members: Stress and responses. Dimens. Crit. Care Nurs. 2000, 19, 40–49. [Google Scholar] [CrossRef] [PubMed]
- McAdam, J.L.; Fontaine, D.K.; White, D.B.; Dracup, K.A.; Puntillo, K.A. Psychological symptoms of family members of high-risk intensive care unit patients. Am. J. Crit. Care 2012, 21, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Bench, S.; Day, T. The user experience of critical care discharge: A meta-synthesis of qualitative research. Int. J. Nurs. Stud. 2010, 47, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.T.; Chiu, Y.L.; Lam, L.W.; Ip, W.Y. Effects of a needs-based education programme for family carers with a relative in an intensive care unit: A quasi-experimental study. Int. J. Nurs. Stud. 2006, 43, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Skirrow, P.; Griffiths, R.D.; Humphris, G.; Ingleby, S.; Eddleston, J.; Waldmann, C.; Gager, M. Post-traumatic stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Med. 2004, 30, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Lautrette, A.; Darmon, M.; Megarbane, B.; Joly, L.M.; Chevret, S.; Adrie, C.; Barnoud, D.; Bleichner, G.; Bruel, C.; Choukroun, G.; et al. A communication strategy and brochure for relatives of patients dying in the ICU. N. Engl. J. Med. 2007, 356, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders; Penguin: Middlesex, UK, 1989. [Google Scholar]
- Ellis, A. Reason and Emotion in Psychotherapy: A Comprehensive Method of Treating Human Disturbances, Revised and Updated ed.; Carol Publishing Group: Secaucus, NJ, USA, 1994. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Wong, D. Getting Out of the Abyss of Depression: A Cognitive Therapy Self Help Manual; Joint Publishing Co.: Hong Kong, China, 2005. [Google Scholar]
- Leung, S.; Mak, Y.; Chiang, V.; Chui, Y.; Sun, S.; Wong, D. Brief cognitive-behavioral intervention for teachers’ work-related stress: A discussion paper on recruitment and engagement issues. Hong Kong J. Ment. Health 2008, 34, 43–50. [Google Scholar]
- Leung, S.S.; Chiang, V.C.; Chui, Y.Y.; Mak, Y.W.; Wong, D.F. A brief cognitive-behavioral stress management program for secondary school teachers. J. Occup. Health 2011, 53, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scale; Psychology Foundation Sydney: Sydney, Australia, 1995. [Google Scholar]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Andrew, M.J.; Baker, R.A.; Kneebone, A.C.; Knight, J.L. Mood state as a predictor of neuropsychological deficits following cardiac surgery. J. Psychosom. Res. 2000, 48, 537–546. [Google Scholar] [CrossRef]
- Barrett, P.; Shortt, A.; Healy, L. Do parent and child behaviours differentiate families whose children have obsessive-compulsive disorder from other clinic and non-clinic families? J. Child Psychol. Psychiatry 2002, 43, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.J. Depression anxiety and stress scales (Dass-21): Psychometric analysis across four racial groups. Anxiety Stress Coping 2007, 20, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Leske, J.S. Needs of relatives of critically ill patients: A follow-up. Heart Lung 1986, 15, 189–193. [Google Scholar] [PubMed]
- Chien, W.T.; Ip, W.Y.; Lee, I.Y.M. Psychometric properties of a Chinese version of Critical Care Family Needs Inventory. Res. Nurs. Health 2005, 28, 474–487. [Google Scholar] [CrossRef] [PubMed]
- Leske, J.S. Internal psychometric properties of the critical care family needs inventory. Heart Lung 1991, 20, 236–244. [Google Scholar] [PubMed]
- Leung, K.K.; Chien, W.T.; Mackenzie, A.E. Needs of Chinese families of critically ill patients. West J. Nurs. Res. 2000, 22, 826–840. [Google Scholar] [CrossRef] [PubMed]
- Hollon, S.D.; Kendall, P.C. Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cognit. Ther. Res. 1980, 4, 383–395. [Google Scholar] [CrossRef]
- Wong, D.F.; Chau, P.; Kwok, A.; Kwan, J. Cognitive-behavioral treatment groups for people with chronic physical illness in Hong Kong: Reflections on a culturally attuned model. Int. J. Group Psychother. 2007, 57, 367–385. [Google Scholar] [CrossRef] [PubMed]
- Roemer, L.; Orsillo, S.M.; Salters-Pedneault, K. Efficacy of an acceptance-based behavior therapy for generalized anxiety disorder: Evaluation in a randomized controlled trial. J. Consult. Clin. Psychol. 2008, 76, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Lenth, R.V. Java Applets for Power and Sample Size (Computer Software). 2006. Available online: http://www.stat.uiowa.edu/~rlenth/Power (accessed on 11 August 2011).
- Tse, M.W.D. Palliative Care in Intensive Care. Presented at Autumn Respiratory Seminar, Hong Kong Thoracic Society, Hong Kong Convention Centre, Hong Kong, China. 25 November 2007. Available online: http://www.fmshk.org/database/articles/palliativecareinintensivecaretsedmwhkspmnewsletter.pdf (accessed on 10 August 2011).
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 9th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Lucasey, B. Quasi-experimental design. Orthop. Nurs. 2002, 21, 56–57. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 301. Repeated measurement analysis. Singap. Med. J. 2004, 45, 354–368. [Google Scholar]
- Halm, M.A. Effects of support groups on anxiety of family members during critical illness. Heart Lung 1990, 19, 62–71. [Google Scholar] [PubMed]
- Curley, M.A. Patient-nurse synergy: Optimizing patients’ outcomes. Am. J. Crit. Care 1998, 7, 64–72. [Google Scholar] [PubMed]
- Insel, T.R.; Fenton, W.S. Psychiatric epidemiology: It’s not just about counting anymore. Arch. Gen. Psychiatry 2005, 62, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Zhao, S.; Katz, S.J.; Kouzis, A.C.; Frank, R.G.; Edlund, M.; Leaf, P. Past-year use of outpatient services for psychiatric problems in the national comorbidity survey. Am. J. Psychiatry 1999, 156, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Berglund, P.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Failure and delay in initial treatment contact after first onset of mental disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Demler, O.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Changing profiles of service sectors used for mental health care in the united states. Am. J. Psychiatry 2006, 163, 1187–1198. [Google Scholar] [CrossRef] [PubMed]
- Pochard, F.; Darmon, M.; Fassier, T.; Bollaert, P.E.; Cheval, C.; Coloigner, M.; Merouani, A.; Moulront, S.; Pigne, E.; Pingat, J.; et al. Symptoms of anxiety and depression in family members of intensive care unit patients before discharge or death. A prospective multicenter study. J. Crit. Care 2005, 20, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Seligman, M.E.; Schulman, P.; DeRubeis, R.J.; Hollon, S.D. The prevention of depression and anxiety. Prev. Treat. 1999. [Google Scholar] [CrossRef]
- Salzberg, A.J. Removable selection bias in quasi-experiments. Am. Stat. 1999, 53, 103–107. [Google Scholar]



{kind=link}
{kind=link}
| Time (min) | Purpose and Focus | Topic | Format/Activities/Materials |
|---|---|---|---|
| 20 | Stress Awareness
|
|
|
| 15 | Cognitive awareness | Identifying automatic thoughts (AT), and irrational beliefs (“thought traps“) |
|
| 25 | Cognitive recognition and intervention | Table of the physio-psycho-cognitive self-analysis (to learn recognizing and differentiating physiological, emotional, cognitive and behavioral responses) |
|
| 20 | Cognitive Restructuring (get away from “thought traps“) | “Five steps to emotion management“ (FSEM) |
|
| 5 | Break | ||
| 25 | Questions & Answers | Individual needs and difficult care giving situations |
|
| 10 | Behavioral interventions |
|
|
| 5 | Feedback | “a person a say“ (sharing of feedback about the program) | |
| Demographic Variable | Intervention (n = 24) | Control (n = 21) | χ2 | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | Male | 8 | 33.3 | 3 | 14.3 | 2.20 |
| Female | 16 | 66.7 | 18 | 85.7 | ||
| Marital Status | Single | 9 | 39.1 | 6 | 28.6 | 0.55 |
| Married | 14 | 60.9 | 15 | 71.4 | ||
| Education level | High school or below | 6 | 25 | 9 | 42.9 | 1.61 |
| High school graduate or above | 18 | 75 | 12 | 57.1 | ||
| History of depression | Yes | 1 | 4.2 | 2 | 9.5 | 0.52 |
| No | 23 | 95.8 | 19 | 90.5 | ||
| Instrument | mean | SD | mean | SD | Z | |
| DASS | Stress | 16.17 | 10.53 | 13.05 | 8.73 | −1.00 |
| Anxiety | 8.83 | 7.98 | 7.62 | 6.15 | −0.23 | |
| Depression | 10.25 | 9.05 | 5.43 | 5.07 | −2.06 * | |
| C-CCFNI | Support | 40.50 | 4.18 | 39.57 | 6.79 | −0.51 |
| Comfort | 16.79 | 2.15 | 16.00 | 3.66 | −0.12 | |
| Proximity | 26.92 | 2.67 | 26.14 | 4.76 | −0.73 | |
| Assurance | 21.67 | 2.65 | 22.00 | 3.41 | −0.58 | |
| Information | 25.67 | 4.63 | 27.19 | 5.06 | −0.89 | |
| Automatic thoughts | 48.17 | 18.66 | 36.00 | 6.12 | −2.50 * | |
| Instrument | B-CBE (n = 24) | Routine Care (n = 21) | Overall (n = 45) | F-Statistics | η2 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | T0 | T1 | Main Effect | Inter-Action Effect | |||
| Mean (SD) | Mean (SD) | Mean (SD) | ||||||||
| DASS | Stress | 16.17 (10.53) | 13.67 (10.28) | 13.05 (8.73) | 9.81 (8.02) | 14.71 (9.75) | 11.87 (9.39) | 10.39 ** | 0.17 | 0.20 |
| Anxiety | 8.83 (7.98) | 8.25 (7.49) | 7.62 (6.15) | 4.86 (5.00) | 8.27 (7.13) | 6.67 (6.61) | 9.63 ** | 4.08 | 0.18 | |
| Depression | 10.25 (9.05) | 9.50 (9.03) | 5.43 (5.07) | 3.24 (4.36) | 8.00 (7.77) | 6.58 (7.82) | 6.37 * | 1.53 | 0.13 | |
| CCFNI | Support | 40.50 (4.18) | 39.29 (5.69) | 39.57 (6.79) | 37.67 (8.40) | 40.07 (5.51) | 38.53 (7.05) | 6.28 * | 0.31 | 0.13 |
| Comfort | 16.79 (2.15) | 16.50 (2.15) | 16.00 (3.66) | 14.67 (3.71) | 16.42 (2.94) | 15.64 (3.08) | 5.44 * | 2.24 | 0.11 | |
| Proximity | 26.92 (2.67) | 26.54 (3.80) | 26.14 (4.76) | 25.57 (6.00) | 26.56 (3.76) | 26.09 (4.91) | 1.31 | 0.06 | - | |
| Assurance | 21.67 (2.65) | 21.50 (3.70) | 22.00 (3.41) | 21.14 (4.22) | 21.82 (3.00) | 21.33 (3.91) | 1.74 | 0.79 | - | |
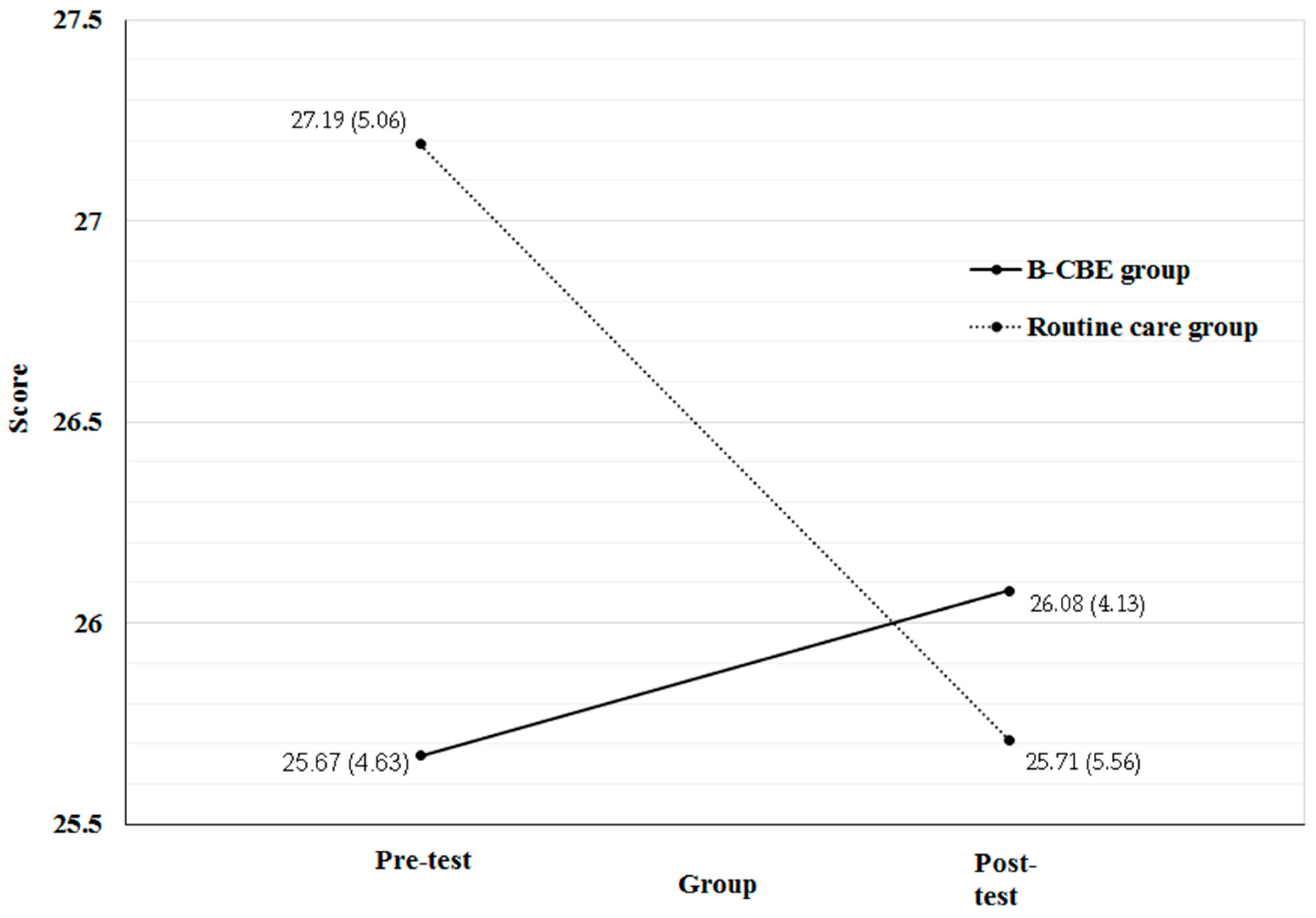
| Information | 25.67 (4.63) | 26.08 (4.13) | 27.19 (5.06) | 25.71 (5.56) | 26.38 (4.84) | 25.91 (4.80) | 1.31 | 4.18 * | 0.09 | |
| Automatic thoughts | 48.17 (18.66) | 47.50 (18.01) | 36.00 (6.12) | 34.62 (4.33) | 42.49 (15.39) | 41.49 (14.84) | 1.49 | 0.18 | - | |
| Instrument | Group | T0 | T1 | Z |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| C-CCFNI (information) | B-CBE | 25.67 (4.63) | 26.08 (4.13) | −0.83 |
| Routine care | 27.19 (5.06) | 25.71 (5.56) | −2.21 * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, V.C.L.; Chien, W.T.; Wong, H.T.; Lee, R.L.P.; Ha, J.; Leung, S.S.K.; Wong, D.F.K. A Brief Cognitive-Behavioral Psycho-Education (B-CBE) Program for Managing Stress and Anxiety of Main Family Caregivers of Patients in the Intensive Care Unit. Int. J. Environ. Res. Public Health 2016, 13, 962. https://doi.org/10.3390/ijerph13100962
Chiang VCL, Chien WT, Wong HT, Lee RLP, Ha J, Leung SSK, Wong DFK. A Brief Cognitive-Behavioral Psycho-Education (B-CBE) Program for Managing Stress and Anxiety of Main Family Caregivers of Patients in the Intensive Care Unit. International Journal of Environmental Research and Public Health. 2016; 13(10):962. https://doi.org/10.3390/ijerph13100962
Chicago/Turabian StyleChiang, Vico Chung Lim, Wai Tong Chien, Ho Ting Wong, Rainbow Lai Ping Lee, Juana Ha, Sharron Shuk Kam Leung, and Daniel Fu Keung Wong. 2016. "A Brief Cognitive-Behavioral Psycho-Education (B-CBE) Program for Managing Stress and Anxiety of Main Family Caregivers of Patients in the Intensive Care Unit" International Journal of Environmental Research and Public Health 13, no. 10: 962. https://doi.org/10.3390/ijerph13100962