
Medical Hydrogeology of Asian Deltas: Status of Groundwater Toxicants and Nutrients, and Implications for Human Health

Abstract
:
1. Introduction
2. Hydrogeology and Health
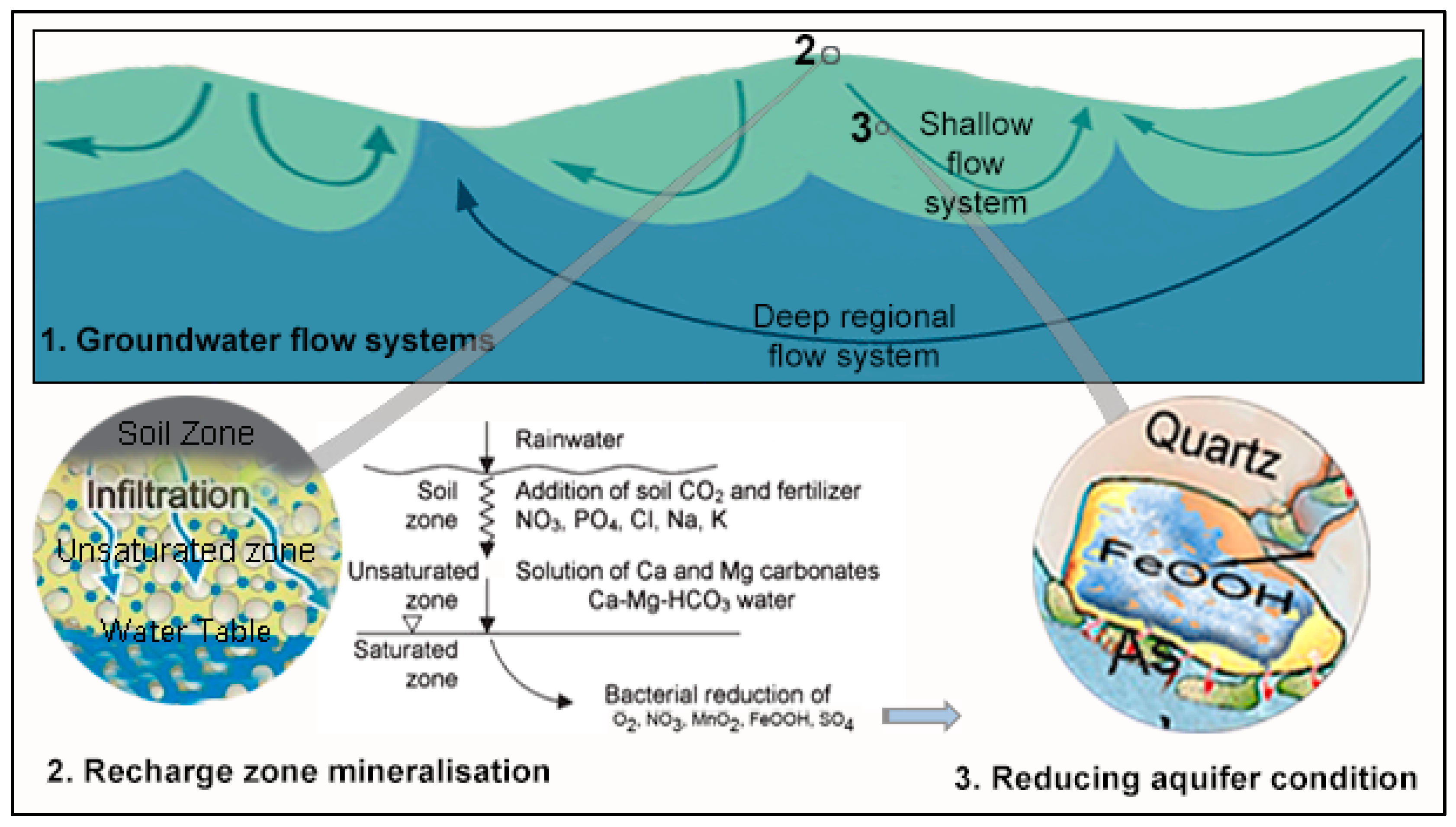
2.1. Hydrogeological Settings
2.2. Groundwater and Health Impact

3. Methods and Materials
3.1. Data
3.2. Data Treatment and Assumptions
3.3. Groundwater Nutrients and Health—Bangladesh Case Study
4. Results
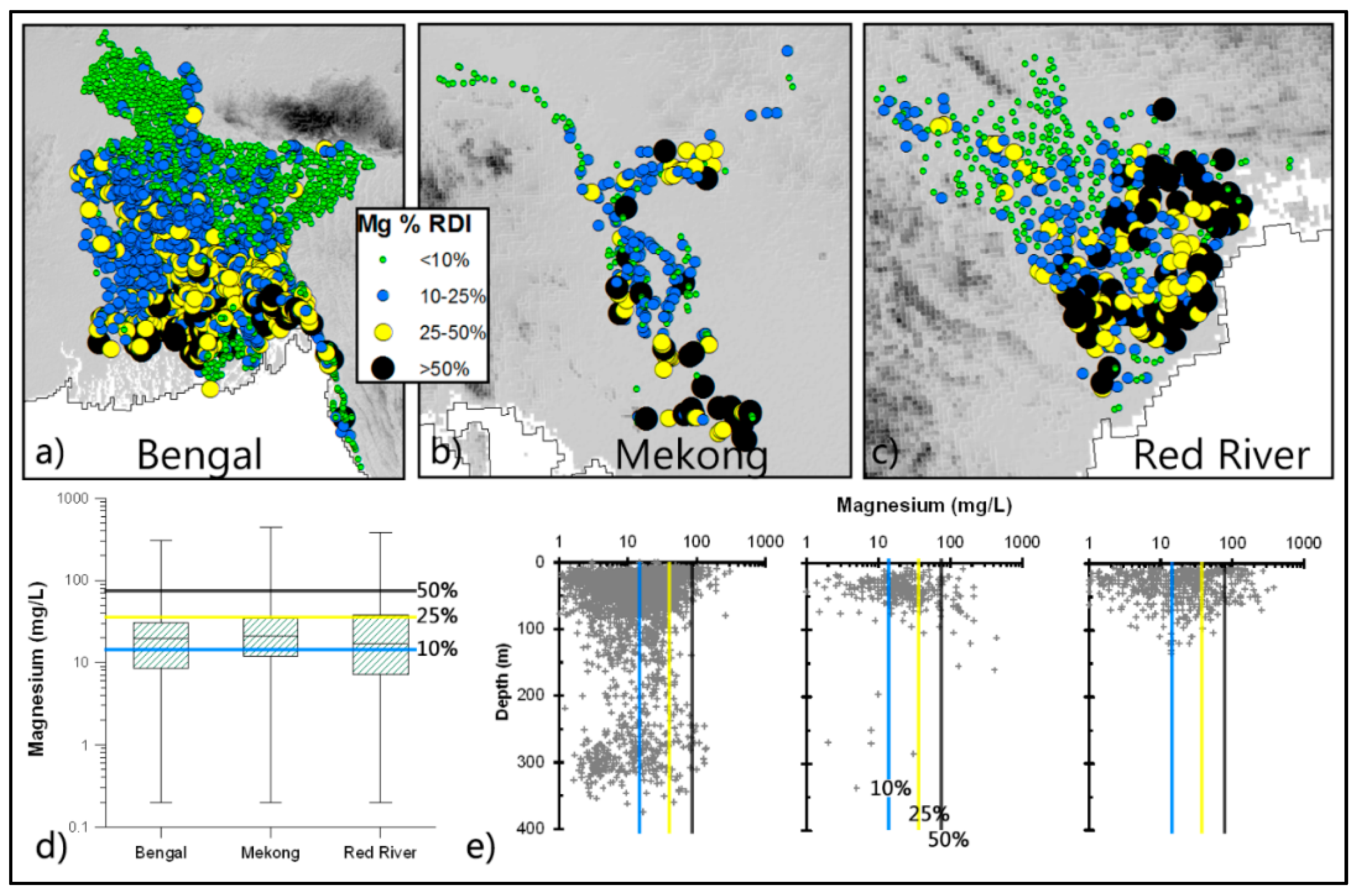
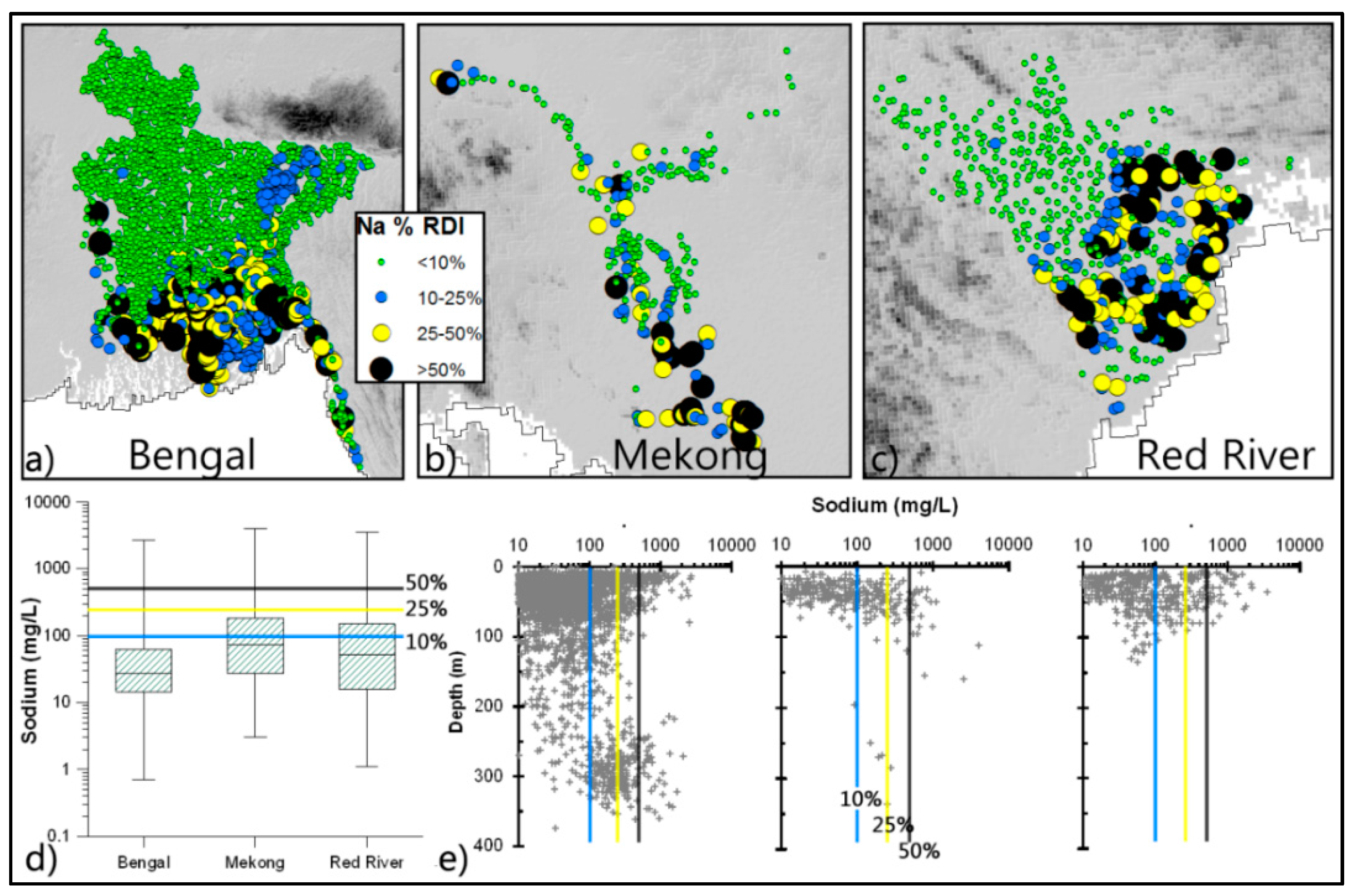
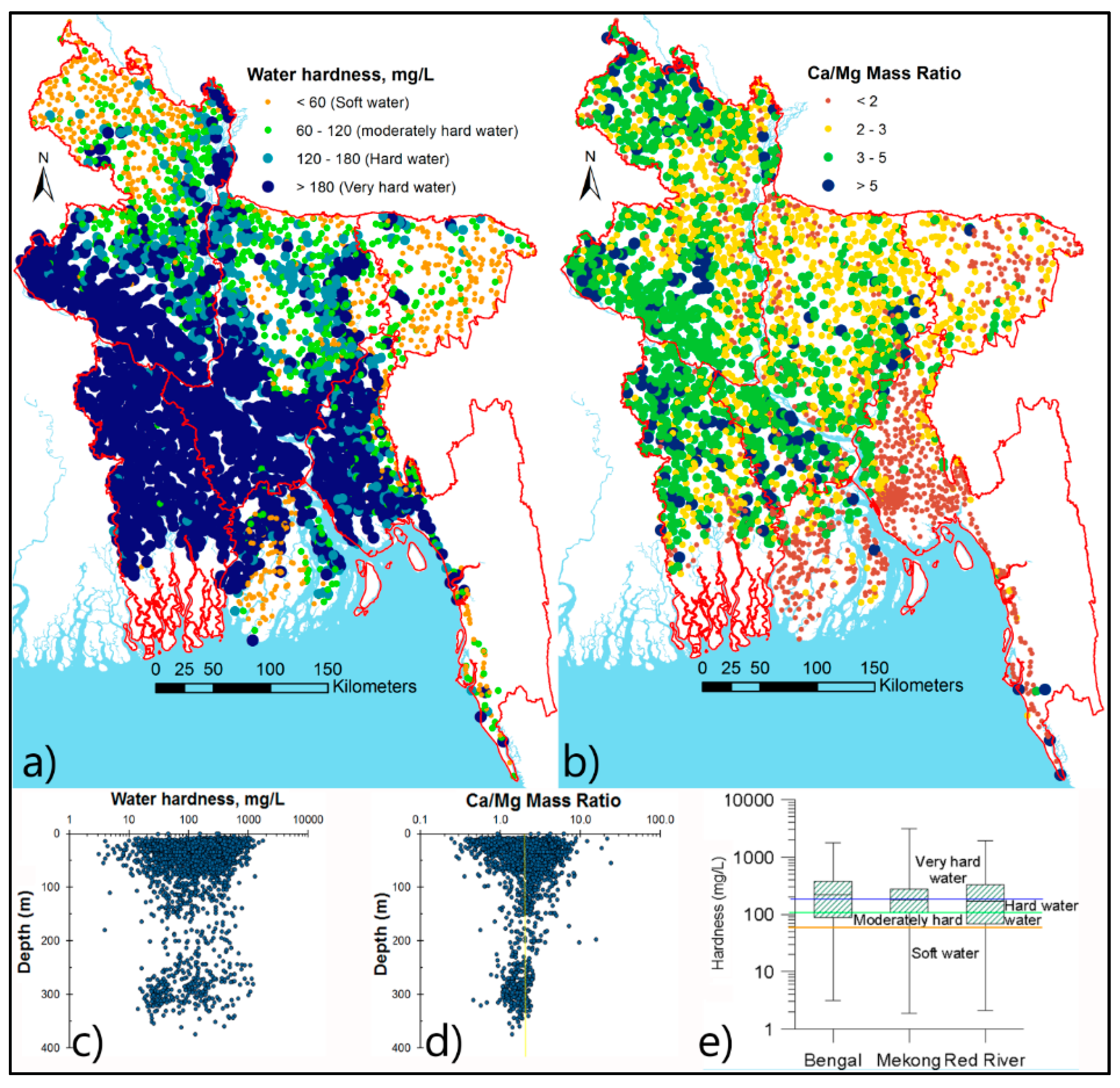
4.1. Status of Macro-Minerals




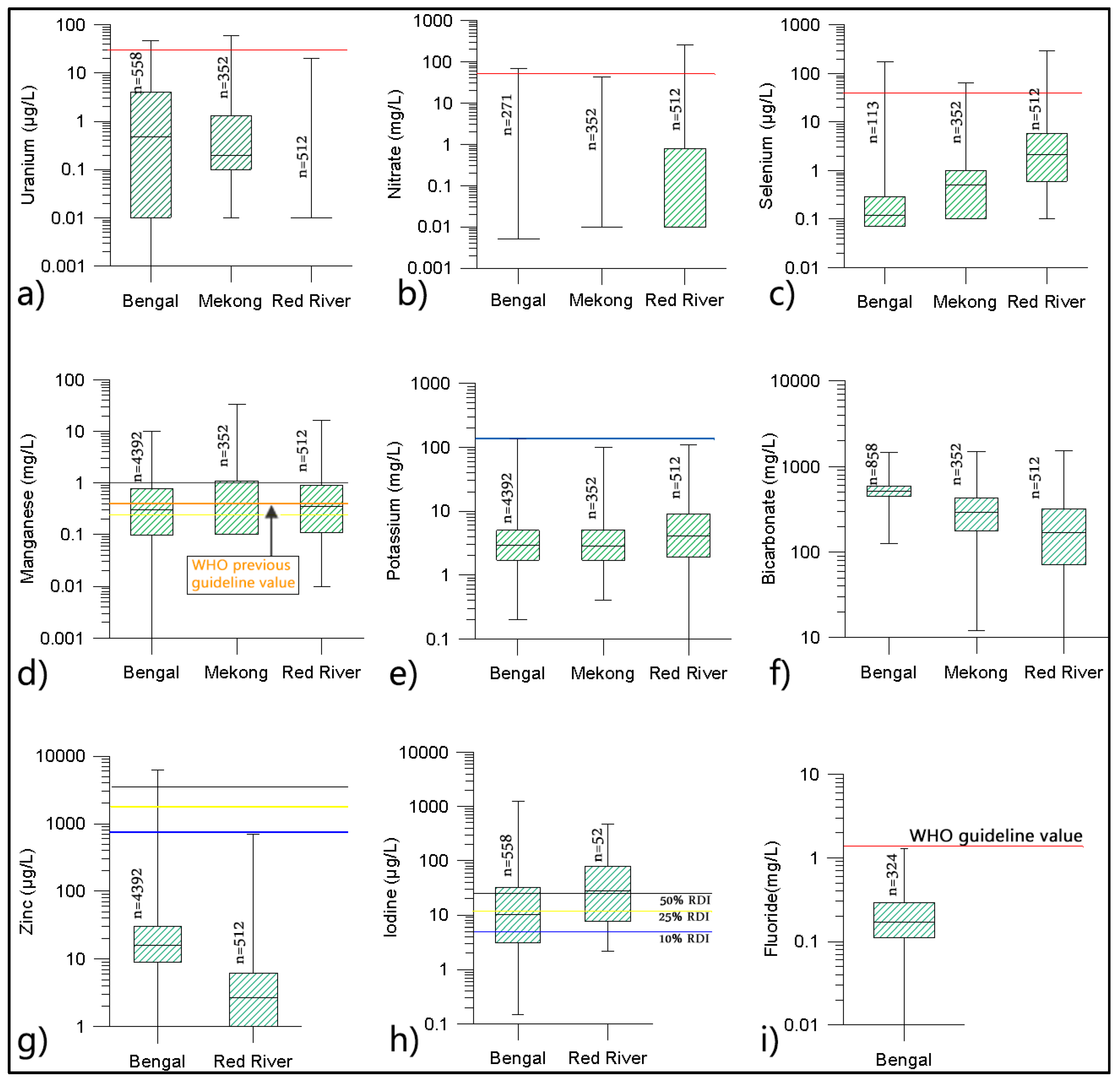
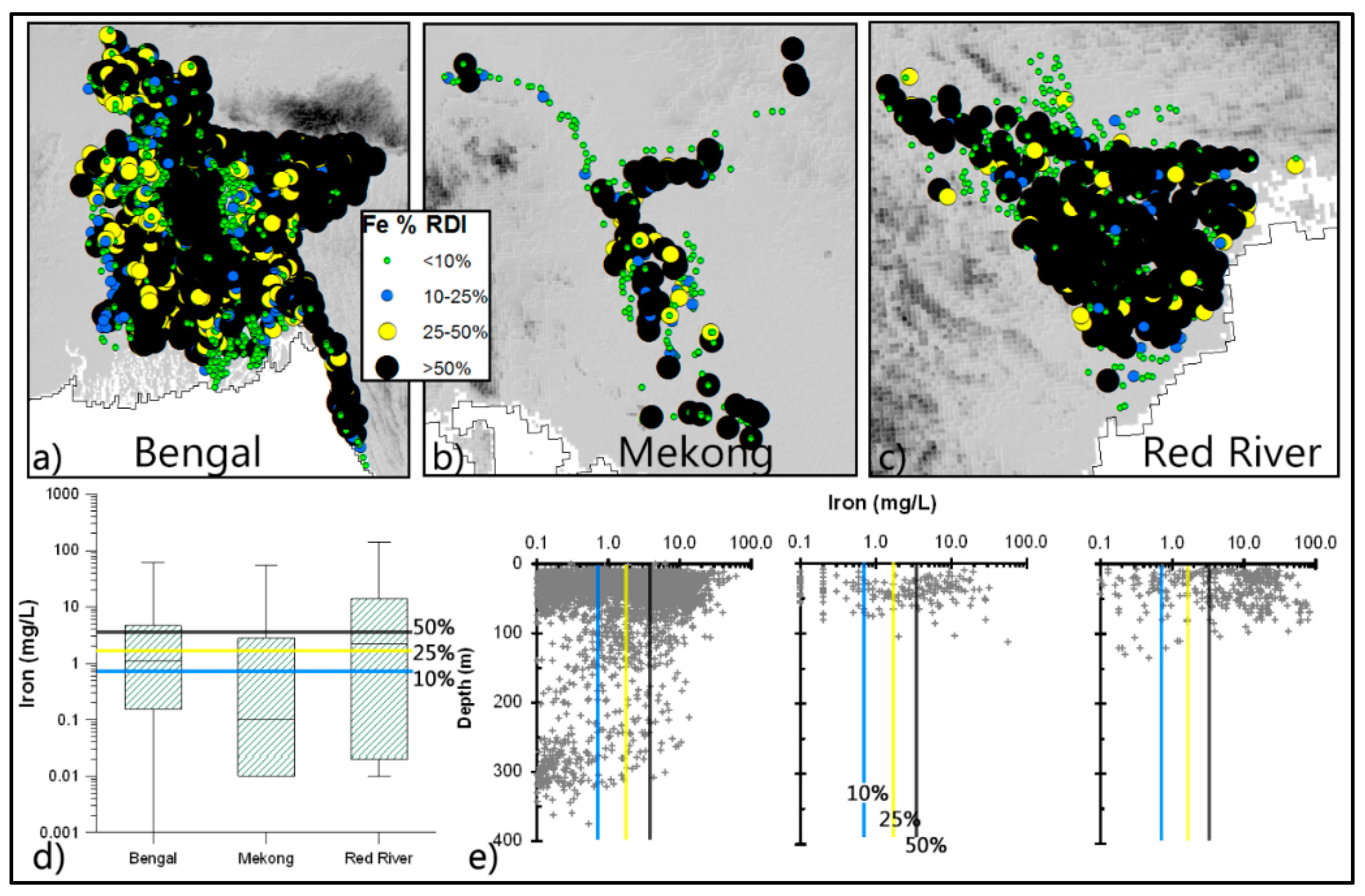
4.2. Status of Micro-Minerals and Toxicants

4.3. Others

4.4. Potential Hydrogeologically Related Health Impacts (Bangladesh Case Study)
4.4.1. Drinking Water and Diet in Bangladesh
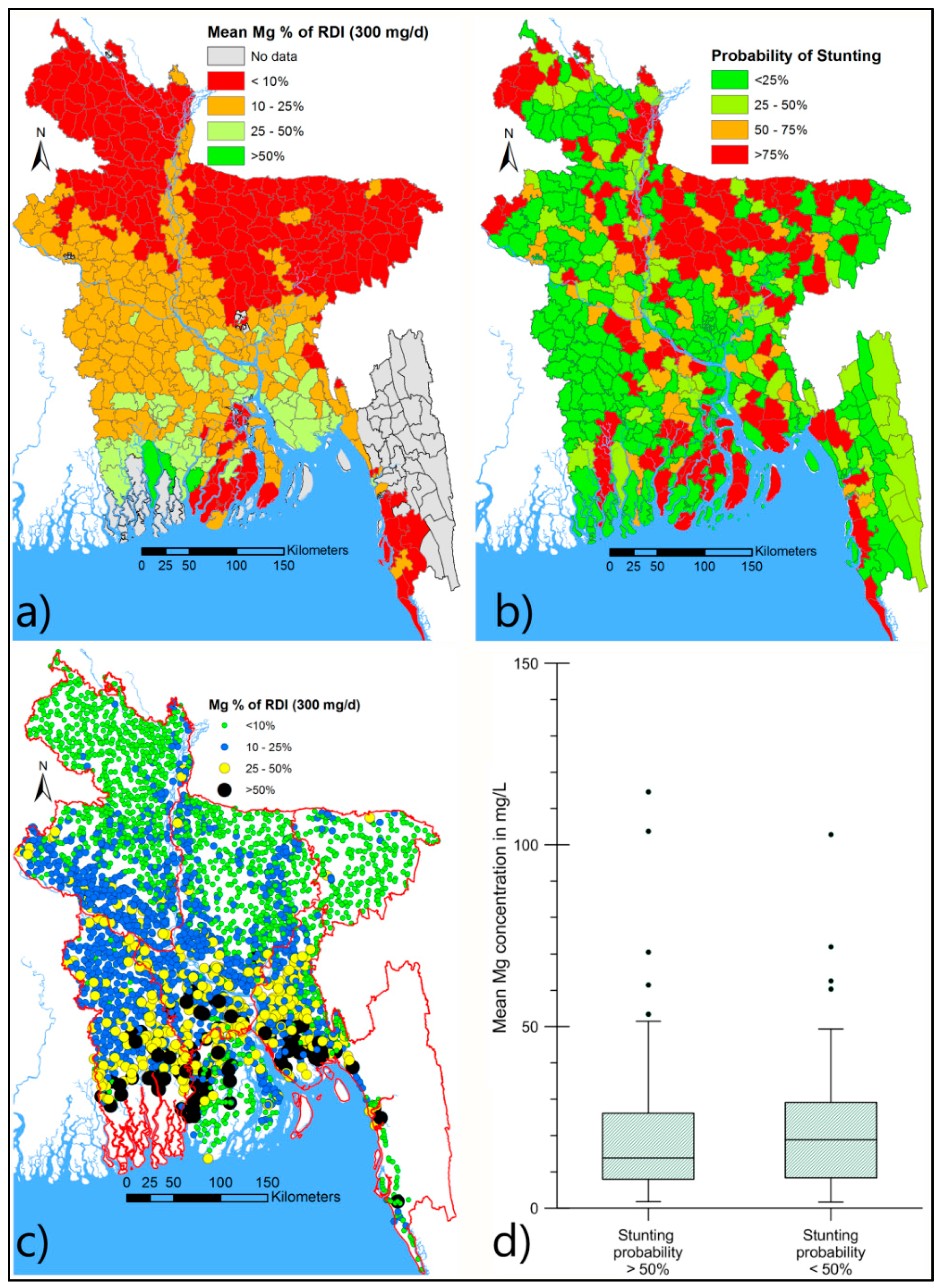
4.4.2. Possible Link between Mg and Low Birth-Weight and Diabetes
4.4.3. Possible Role of Ca in Bone Health, and Joint Role of Ca and Mg in Blood Pressure Regulation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
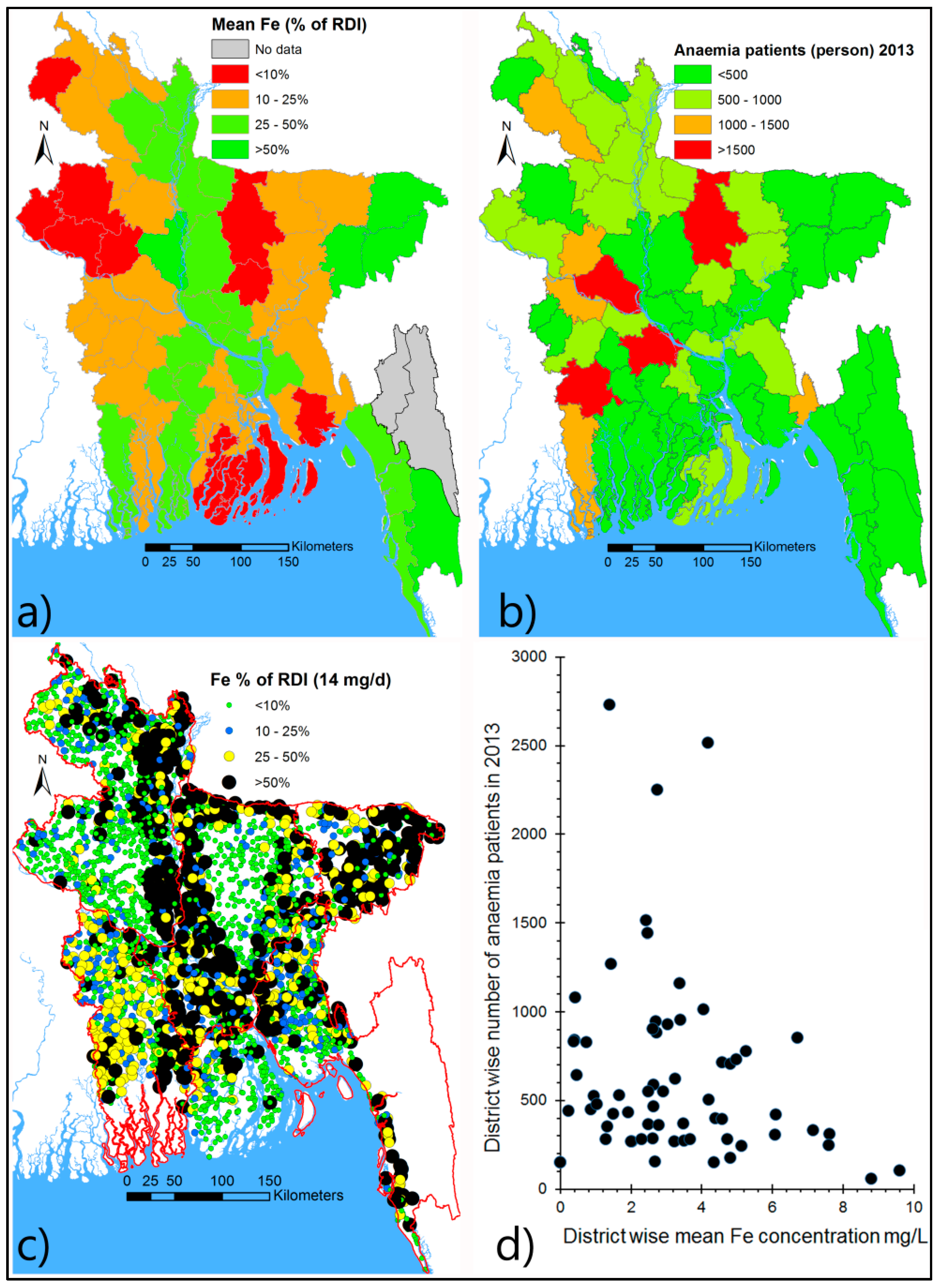
4.4.4. Anaemia and the Tubewell Fe Content in Bangladesh
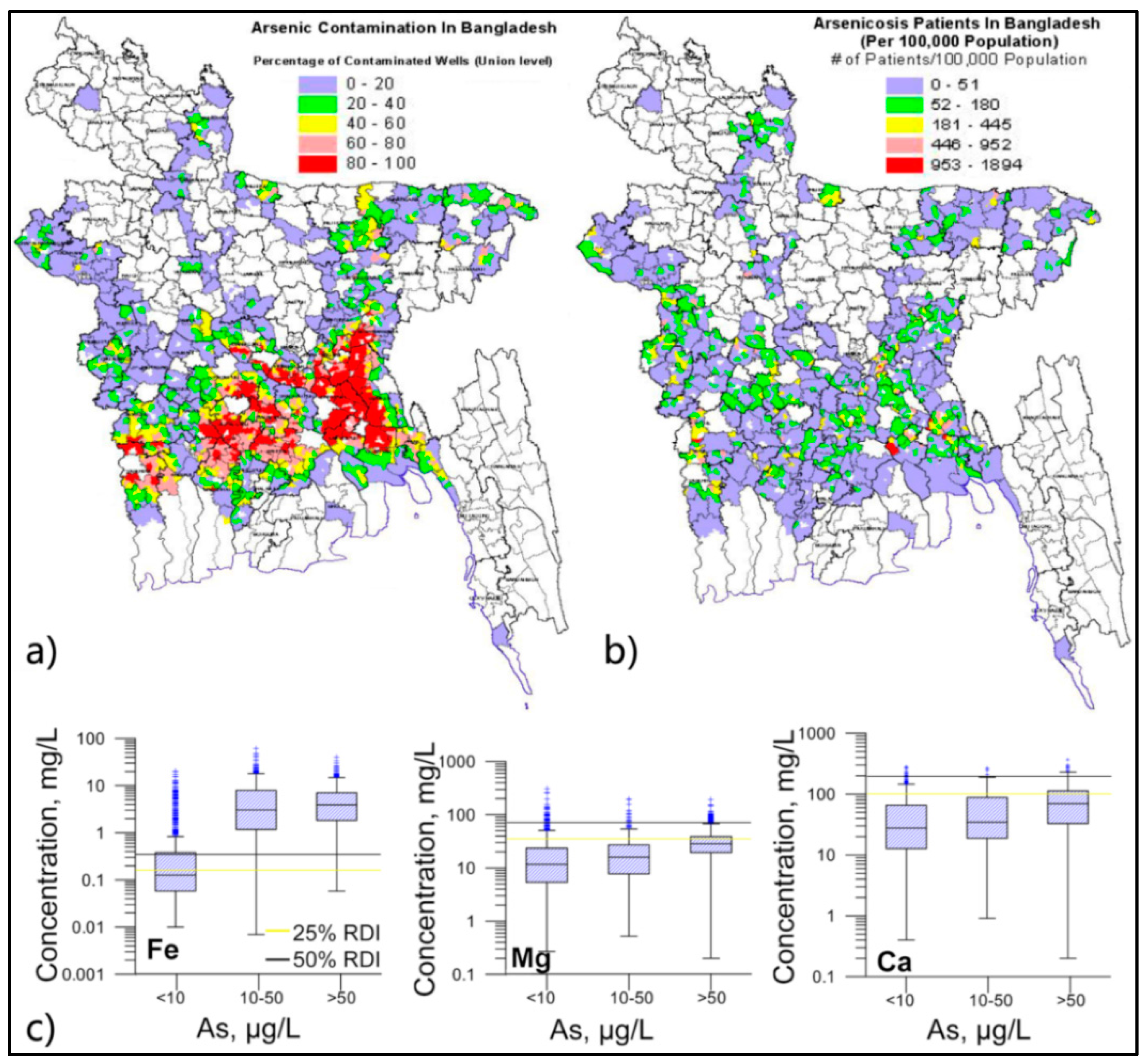
4.4.5. Spatial Distribution of As and Arsenicosis in Bangladesh

5. Discussion
5.1. Coexistence of Nutrients and Toxicants in Groundwater


5.2. Medical Hydrogeology: Controls on Groundwater Nutrients and Toxicants
5.3. Health Benefit in Resource Poor Settings and Food Frequency Questionnaire
6. Conclusions
- Drinking groundwater may supply substantial amounts of nutrients beneficial to human health, even though their adsorption by the body and overall health benefits are yet to be fully determined.
- In addition, groundwater may also contain toxicants and therefore coupling or decoupling the toxicity with other constituents present in the water needs to be studied in an holistic manner.
- An understanding of the association of non-communicable disease and poor nutrition cannot be developed, particularly in areas with high levels of dissolved solids in water sources, without considering the contribution of drinking water to nutrient and mineral supply.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Whelton, A.J.; Dietrich, A.M.; Burlingame, G.A.; Schechs, M.; Duncan, S.E. Minerals in drinking water: Impacts on taste and importance to consumer health. Water Sci. Technol. 2007, 55, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Flaten, T.P.; Bolviken, B. Geographical associations between drinking water chemistry and the mortality and morbidity of cancer and some other diseases in Norway. Sci. Total Environ. 1991, 102, 75–100. [Google Scholar] [CrossRef]
- Komatina, M. Medical Geology: Effects of Geological Environments on Human Health; Elsevier B.V.: Amsterdam, The Netherlands, 2004; Volume 2. [Google Scholar]
- Selinus, O.; Finkelman, R.B.; Centeno, J.A. Medical Geology: A Regional Synthesis; Springer: New York, NY, USA, 2010; p. 392. [Google Scholar]
- Selinus, O. Essentials of Medical Geology; Springer: New York, NY, USA, 2013; p. 824. [Google Scholar]
- Ekambaram, P.; Paul, V. Calcium preventing locomotor behavioral and dental toxicities of fluoride by decreasing serum fluoride level in rats. Environ. Toxicol. Pharmacol. 2001, 9, 141–146. [Google Scholar] [CrossRef]
- Jacks, G.; Bhattacharya, P.; Chaudhary, V.; Singh, K.P. Controls on the genesis of some high-fluoride groundwaters in India. Appl. Geochem. 2005, 20, 221–228. [Google Scholar] [CrossRef]
- Ramakrishnan, U. Prevalence of micronutrient malnutrition worldwide. Nutr. Rev. 2002, 60, 46–52. [Google Scholar] [CrossRef]
- Lee, T.-Y.; Lawver, L.A. Cenozoic plate reconstruction of southeast Asia. Tectonophysics 1995, 251, 85–138. [Google Scholar] [CrossRef]
- Saito, Y.; Chaimanee, N.; Jarupongsakul, T.; Syvitski, J.P.M. Shrinking megadeltas in Asia: Sea-level rise and sediment reduction impacts from case study of the Chao Phraya Delta. INPRINT Newsletter 2007, 2, 3–9. [Google Scholar]
- Voris, H.K. Maps of pleistocene sea levels in Southeast Asia: Shorelines, river systems and time durations. J. Biogeogr. 2000, 27, 1153–1167. [Google Scholar] [CrossRef]
- Goodbred, S.L., Jr.; Kuehl, S.A. The significance of large sediment supply, active tectonism, and eustasy on margin sequence development: Late quaternary stratigraphy and evolution of the ganges-brahmaputra delta. Sediment. Geol. 2000, 133, 227–248. [Google Scholar] [CrossRef]
- Tanabe, S.; Saito, Y.; Lan Vu, Q.; Hanebuth, T.J.J.; Lan Ngo, Q.; Kitamura, A. Holocene evolution of the Song Hong (Red River) delta system, northern Vietnam. Sediment. Geol. 2006, 187, 29–61. [Google Scholar] [CrossRef]
- Ta, T.K.O.; Nguyen, V.L.; Tateishi, M.; Kobayashi, I.; Tanabe, S.; Saito, Y. Holocene delta evolution and sediment discharge of the mekong river, southern Vietnam. Quat. Sci. Rev. 2002, 21, 1807–1819. [Google Scholar] [CrossRef]
- Burgess, W.G.; Hoque, M.A.; Michael, H.A.; Voss, C.I.; Breit, G.N.; Ahmed, K.M. Vulnerability of deep groundwater in the Bengal aquifer system to contamination by arsenic. Nat. Geosci. 2010, 3, 83–87. [Google Scholar] [CrossRef]
- Hoque, M.A.; McArthur, J.M.; Sikdar, P.K. Sources of low-arsenic groundwater in the Bengal Basin: Investigating the influence of the last glacial maximum palaeosol using a 115-km traverse across Bangladesh. Hydrogeol. J. 2014, 22, 1535–1547. [Google Scholar] [CrossRef]
- McArthur, J.M.; Ravenscroft, P.; Banerjee, D.M.; Milsom, J.; Hudson-Edwards, K.A.; Sengupta, S.; Bristow, C.; Sarkar, A.; Tonkin, S.; Purohit, R. How paleosols influence groundwater flow and arsenic pollution: A model from the Bengal Basin and its worldwide implication. Water Resour. Res. 2008, 44, W11411. [Google Scholar] [CrossRef]
- Benner, S.G.; Polizzotto, M.L.; Kocar, B.D.; Ganguly, S.; Phan, K.; Ouch, K.; Sampson, M.; Fendorf, S. Groundwater flow in an arsenic-contaminated aquifer, Mekong Delta, Cambodia. Appl. Geochem. 2008, 23, 3072–3087. [Google Scholar] [CrossRef]
- Winkel, L.H.E.; Trang, P.T.K.; Lan, V.M.; Stengel, C.; Amini, M.; Ha, N.T.; Viet, P.H.; Berg, M. Arsenic pollution of groundwater in Vietnam exacerbated by deep aquifer exploitation for more than a century. Proc. Natl. Acad. Sci. USA 2011, 108, 1246–1251. [Google Scholar] [CrossRef] [PubMed]
- McArthur, J.M.; Banerjee, D.M.; Hudson-Edwards, K.A.; Mishra, R.; Purohit, R.; Ravenscroft, P.; Cronin, A.; Howarth, R.J.; Chatterjee, A.; Talkdar, T.; et al. Natural organic matter in sedimentary basins and its relation to arsenic in anoxic groundwater: The example of West Bengal and its worldwide implications. Appl. Geochem. 2004, 19, 1255–1293. [Google Scholar] [CrossRef]
- Ravenscroft, P.; Burgess, W.G.; Ahmed, K.M.; Burren, M.; Perrin, J. Arsenic in groundwater of the bengal basin, bangladesh: Distribution, field relations, and hydrogeological setting. Hydrogeol. J. 2005, 13, 727–751. [Google Scholar] [CrossRef]
- BGS/DPHE. Arsenic Contamination of Groundwater in Bangladesh; Department of Public Health Engineering (DPHE) of Government of Bangladesh and British Geological Survey (BGS) Keyworth: Dhaka, Bangladesh, 2001; p. 267.
- Fendorf, S.; Michael, H.A.; van Geen, A. Spatial and temporal variations of groundwater arsenic in south and southeast Asia. Science 2010, 328, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Van Weert, F.; van der Gun, J.; Reckman, J. Global Overview of Saline Groundwater Occurrence and Genesis; GP 2009–1; International Groundwater Resources Assessment Centre (IGRAC): The Hague Area, The Netherlands, 2009; p. 104. [Google Scholar]
- Delta Alliance. Vietnam-Netherlands Mekong Delta Masterplan Project Report (Mekong Delta Water Resources Assessment Studies). Available online: http://nguyenthanhmy.com/courses/GOOD-Mekong-Water-Resource-2011.pdf (accessed on 21 December 2015).
- Ravenscroft, P.; McArthur, J.M.; Hoque, M.A. Stable groundwater quality in deep aquifers of Southern Bangladesh: The case against sustainable abstraction. Sci. Total Environ. 2013, 454–455, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, B.K.; Caldwell, J.C.; Mitra, S.N.; Smith, W. Tubewells and arsenic in Bangladesh: Challenging a public health success story. Int. J. Popul. Geogr. 2003, 9, 23–38. [Google Scholar] [CrossRef]
- Zwane, A.P.; Kremer, M. What works in fighting diarrheal diseases in developing countries? A critical review. World Bank Res. Obs. 2007, 22, 1–24. [Google Scholar] [CrossRef]
- Aziz, K.M.A.; Hoque, B.A.; Hasan, K.Z.; Patwary, M.Y.; Huttly, S.R.A.; Rahaman, M.M.; Feachem, R.G. Reduction in diarrhoeal diseases in children in rural Bangladesh by environmental and behavioural modifications. Trans. R. Soc. Trop. Med. Hyg. 1990, 84, 433–438. [Google Scholar] [CrossRef]
- Smith, A.H.; Lingas, E.O.; Rahman, M. Contamination of drinking water by arsenic in Bangladesh: A public health emergency. Bull. World Health Organ. 2000, 78, 1093–1103. [Google Scholar] [PubMed]
- Argos, M.; Kalra, T.; Rathouz, P.J.; Chen, Y.; Pierce, B.; Parvez, F.; Islam, T.; Ahmed, A.; Rakibuz-Zaman, M.; Hasan, R.; et al. Arsenic exposure from drinking water, and all-cause and chronic-disease mortalities in Bangladesh (HEALS): A prospective cohort study. Lancet 2010, 376, 252–258. [Google Scholar] [CrossRef]
- Wasserman, G.A.; Liu, X.; Parvez, F.; Ahsan, H.; Levy, D.; Factor-Litvak, P.; Kline, J.; van Geen, A.; Slavkovich, V.; LoIacono, N.J.; et al. Water manganese exposure and children's intellectual function in Araihazar, Bangladesh. Environ. Health Perspect. 2006, 114, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.E.; Ireson, A.; Kovats, S.; Mojumder, S.K.; Khusru, A.; Rahman, A.; Vineis, P. Drinking water salinity and maternal health in coastal Bangladesh: Implications of climate change. Environ. Health Perspect. 2011, 119, 1328–1332. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.E.; Scheelbeek, P.F.D.; Shilpi, A.B.; Chan, Q.; Mojumder, S.K.; Rahman, A.; Haines, A.; Vineis, P. Salinity in drinking water and the risk of (pre)Eclampsia and gestational hypertension in coastal Bangladesh: A case-control study. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Buschmann, J.; Berg, M.; Stengel, C.; Winkel, L.; Sampson, M.L.; Trang, P.T.K.; Viet, P.H. Contamination of drinking water resources in the mekong delta floodplains: Arsenic and other trace metals pose serious health risks to population. Environ. Int. 2008, 34, 756–764. [Google Scholar] [CrossRef] [PubMed]
- McArthur, J.M.; Sikdar, P.K.; Nath, B.; Grassineau, N.; Marshall, J.D.; Banerjee, D.M. Sedimentological control on Mn, and other trace elements, in groundwater of the Bengal Delta. Environ. Sci. Technol. 2012, 46, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Fryar, A.E. Deeper groundwater chemistry and geochemical modeling of the arsenic affected western Bengal Basin, West Bengal, India. Appl. Geochem. 2008, 23, 863–894. [Google Scholar] [CrossRef]
- EROS. Shuttle Radar Topography Mission (SRTM) Elevation Data Set—National Aeronautics and Space Administration (NASA), German Aerospace Center (DLR), Italian Space Agency (ASI). The National Center for Earth Resources Observations and Science (EROS); United State Geological Survey (USGS) Sioux Falls: Garretson, SD, USA, 2002. [Google Scholar]
- FAO; WHO. Human Vitamin and Mineral Requirements, Report of a Joint FAO/WHO Expert Consultation Bangkok, Thailand; Food and Agriculture Organization (FAO) of the United Nations, and World Health Organization (WHO): New York, NY, USA, 2001; p. 286. [Google Scholar]
- Islam, M.A.; Sakakibara, H.; Sekine, M.; Karim, M.R. Rural water consumption behavior: A case study in southwest coastal area, Bangladesh. World Environ. Water Resour. Congr. 2011. [Google Scholar] [CrossRef]
- Rahman, M.M.; Asaduzzaman, M.; Naidu, R. Consumption of arsenic and other elements from vegetables and drinking water from an arsenic-contaminated area of Bangladesh. J. Hazard. Mater. 2013, 262, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- WHO. Nutrients in Drinking Water; World Health Organization (WHO): Geneva, Switzerland, 2005; p. 186. [Google Scholar]
- UNICEF. Strengthening National Wash MIS/GIS System: Nation-Wide Water Point Mapping; UNICEF: Dhaka, Bangladesh, 2014; p. 2. [Google Scholar]
- WHO. Guidelines for Drinking-Water Quality, 4th ed.; World Health Organization, Ed.; World Health Organization: Geneva, Swizerland, 2011. [Google Scholar]
- Berg, M.; Tran, H.C.; Nguyen, T.C.; Pham, H.V.; Schertenleib, R.; Giger, W. Arsenic contamination of groundwater and drinking water in Vietnam: A human health threat. Environ. Sci. Technol. 2001, 35, 2621–2626. [Google Scholar] [CrossRef] [PubMed]
- Ravenscroft, P.; Brammer, H.; Richards, K.S. Arsenic Pollution: A Global Synthesis, 1st ed.; Wiley-Blackwell: London, UK, 2009; p. 616. [Google Scholar]
- van Geen, A.; Zheng, Y.; Versteeg, R.; Stute, M.; Horneman, A.; Dhar, R.; Steckler, M.; Gelman, A.; Small, C.; Ahsan, H.; et al. Spatial variability of arsenic in 6000 tube wells in a 25 km2 area of Bangladesh. Water Resour. Res. 2003, 39, 1140–1155. [Google Scholar] [CrossRef]
- Nickson, R.; McArthur, J.M.; Burgess, W.G.; Ahmed, K.M.; Ravenscroft, P.; Rahman, M. Arsenic poisoning in Bangladesh groundwater. Nature 1998. [Google Scholar] [CrossRef] [PubMed]
- Rylander, R. Drinking water constituents and disease. J. Nutr. 2008, 138, 423–425. [Google Scholar]
- Razowska-Jaworek, L. Calcium and Magnesium in Groundwater: Occurrence and Significance for Human Health; Taylor & Francis Group: London, UK, 2014; p. 236. [Google Scholar]
- Halder, S.; Urey, I.; Barua, P. Patterns and Trends in Food Consumption in Poor Urban and Rural Households in Bangladesh: The Field Survey Results; Research and Evaluation Division, Bangladesh Rural Advancement Committee (BRAC): Dhaka, Bangladesh, 2003; p. 84. [Google Scholar]
- World Bank. Maintaining Momentum to 2015? An Impact Evaluation of Interventions to Improve Maternal and Child Health and Nutrition in Bangladesh; The World Bank: Washington, DC, USA, 2005; p. 248. [Google Scholar]
- Hels, O.; Kidmose, U.; Larsen, T.; Hassan, N.; Tetens, I.; Thilsted, S.H. Estimated nutrient intakes and adequacies in Bangladesh change when newer values for vitamin A, iron and calcium in commonly consumed foods are applied. Int. J. Food Sci. Nutr. 2003, 54, 457–465. [Google Scholar] [CrossRef] [PubMed]
- WFP. Nutrition Strategy 2012–2016; World Food Programme (WFP) Bangladesh: Dhaka, Bangladesh, 2012; p. 24. [Google Scholar]
- Jesmin, A.; Yamamoto, S.S.; Malik, A.A.; Haque, M.A. Prevalence and determinants of chronic malnutrition among preschool children: A cross-sectional study in Dhaka City, Bangladesh. J. Health Popul. Nutr. 2011, 29, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Takaya, J.; Yamato, F.; Kaneko, K. Possible relationship between low birth weight and magnesium status: From the standpoint of “fetal origin” hypothesis. Magnes Res. 2006, 19, 63–69. [Google Scholar] [PubMed]
- Yang, C.Y.; Chiu, H.F.; Tsai, S.S.; Chang, C.C.; Sung, F.C. Magnesium in drinking water and the risk of delivering a child of very low birth weight. Magnes Res. 2002, 15, 207–213. [Google Scholar] [PubMed]
- Sales, C.H.; Pedrosa, L.D.F.C. Magnesium and diabetes mellitus: Their relation. Clin. Nutr. 2006, 25, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Dai, Q.; He, K. Magnesium intake, insulin resistance, and type 2 diabetes. N. Am. J. Med. Sci. 2013, 6, 9–15. [Google Scholar]
- Akter, S.; Rahman, M.M.; Abe, S.K.; Sultana, P. Prevalence of diabetes and prediabetes and their risk factors among bangladeshi adults: A nationwide survey. Bull. World Health Organ. 2014, 92, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.Z.; Lamberg-Allardt, C.; Karkkainen, M.; Ali, S.M.K. Dietary calcium intake in premenopausal Bangladeshi women: Do socio-economic or physiological factors play a role? Eur. J. Clin. Nutr. 2003, 57, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.; Bhattacharjee, S.C.; Khan, S.S.A.; Rahman, S. Determining the magnesium concentration from some indigenous fruits and vegetables of Chittagong Region, Bangladesh. Int. Food Res. J. 2014, 21, 1413–1417. [Google Scholar]
- Fischer, P.; Rahman, A.; Cimma, J.; Kyaw-Myint, T.; Kabir, A.; Talukder, K.; Hassan, N.; Manaster, B.; Staab, D.; Duxbury, J.; et al. Nutritional rickets without vitamin D deficiency in Bangladesh. J. Trop. Pediatr. 1999, 45, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Helen Keller Worldwide. Rickets in Bangladeshi children: A small focus or a widespread problem? Nutr. Surveill. Proj. Bull. 2001, 4, 1–3. [Google Scholar]
- Briend, A.; Hoque, B.A.; Aziz, K.M. Iron in tubewell water and linear growth in rural Bangladesh. Arch. Dis. Child. 1990, 65, 224–225. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.D.; Shamim, A.A.; Ali, H.; Jahan, N.; Labrique, A.B.; Schulze, K.; Christian, P.; West, K.P., Jr. Iron status of women is associated with the iron concentration of potable groundwater in rural Bangladesh. J. Nutr. 2011, 141, 944–949. [Google Scholar] [CrossRef] [PubMed]
- APSU. The Response to Arsenic Contamination in Bangladesh: A Position Paper; Department of Public Health Engineering (DPHE): Dhaka, Bangladesh, 2005; p. 74. [Google Scholar]
- Rosborg, I. Drinking Water Minerals and Mineral Balance: Importance, Health Significance, Safety Precautions; Springer International Publishing Switzerland: London, UK, 2015; p. 140. [Google Scholar]
- Chen, Y.; Graziano, J.H.; Parvez, F.; Liu, M.; Slavkovich, V.; Kalra, T.; Argos, M.; Islam, T.; Ahmed, A.; Rakibuz-Zaman, M.; et al. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: Prospective cohort study. BMJ 2011. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, D.; Subramanian, R.B.; Madamwar, D.; Flora, S.J. Protective effects of selenium, calcium, and magnesium against arsenic-induced oxidative stress in male rats. Arh. Hig. Rada Toksikol 2010, 61, 153–159. [Google Scholar] [CrossRef] [PubMed]
- ICCIDD. FAQS about Iodine Nutrition, International Council for the Control of Iodine Deficiency Disorders (ICCIDD). Available online: http://ign.org/p142002130.html (accessed on 30 July 2013).
- Hiscock, K. Hydrogeology: Principles and Practice, 1st ed.; Blackwell Science Ltd.: Malden, MA, USA, 2005. [Google Scholar]
- McArthur, J.M.; Ravenscroft, P.; Safiullah, S.; Thirlwall, M.F. Arsenic in groundwater: Testing pollution mechanisms for sedimentary aquifers in Bangladesh. Water Resour. Res. 2001, 37, 109–117. [Google Scholar] [CrossRef]
- Reeburgh, W.S. Rates of biogeochemical processes in anoxic sediments. Annu. Rev. Earth Planet. Sci. 1983, 11, 269–298. [Google Scholar] [CrossRef]
- Zheng, Y.; Stute, M.; van Geen, A.; Gavrieli, I.; Dhar, R.; Simpson, H.J.; Schlosser, P.; Ahmed, K.M. Redox control of arsenic mobilization in Bangladesh groundwater. Appl. Geochem. 2004, 19, 201–214. [Google Scholar] [CrossRef]
- Schoppen, S.; Pérez-Granados, A.M.; Carbajal, Á.; Oubiña, P.; Sánchez-Muniz, F.J.; Gómez-Gerique, J.A.; Vaquero, M.P. A sodium-rich carbonated mineral water reduces cardiovascular risk in postmenopausal women. J. Nutr. 2004, 134, 1058–1063. [Google Scholar] [PubMed]
- Santos, A.; Martins, M.J.; Guimaraes, J.T.; Severo, M.; Azevedo, I. Sodium-rich carbonated natural mineral water ingestion and blood pressure. Rev. Port. Cardiol. 2010, 29, 159–172. [Google Scholar] [PubMed]
- Edmunds, W.M.; Smedley, P.L. Groundwater geochemistry and health: An overview. Geol. Soc. London. Spec. Publ. 1996, 113, 91–105. [Google Scholar] [CrossRef]
- Nickson, R.; McArthur, J.M.; Ravenscroft, P.; Burgess, W.G.; Ahmed, K.M. Mechanism of arsenic release to groundwater, Bangladesh and west bengal. Appl. Geochem. 2000, 15, 403–413. [Google Scholar] [CrossRef]
- Hug, S.J.; Leupin, O.X.; Berg, M. Bangladesh and vietnam: Different groundwater compositions require different approaches to arsenic mitigation. Environ. Sci. Technol. 2008, 42, 6318–6323. [Google Scholar] [CrossRef] [PubMed]
- Ravenscroft, P.; McArthur, J.M. Mechanism of regional scale enrichment of groundwater by boron: The examples of Bangladesh and Michigan, USA. Appl. Geochem. 2004, 19, 1413–1430. [Google Scholar] [CrossRef]
- Hoque, M.A.; Burgess, W.G. 14C dating of deep groundwater in the bengal aquifer system, Bangladesh: Implications for aquifer anisotropy, recharge sources and sustainability. J. Hydrol. 2012, 444–445, 209–220. [Google Scholar] [CrossRef]
- Sharma, S. Development and use of FFQ among adults in diverse settings across the globe. Proc. Nutr. Soc. 2011, 70, 232–251. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoque, M.A.; Butler, A.P. Medical Hydrogeology of Asian Deltas: Status of Groundwater Toxicants and Nutrients, and Implications for Human Health. Int. J. Environ. Res. Public Health 2016, 13, 81. https://doi.org/10.3390/ijerph13010081
Hoque MA, Butler AP. Medical Hydrogeology of Asian Deltas: Status of Groundwater Toxicants and Nutrients, and Implications for Human Health. International Journal of Environmental Research and Public Health. 2016; 13(1):81. https://doi.org/10.3390/ijerph13010081
Chicago/Turabian StyleHoque, Mohammad A., and Adrian P. Butler. 2016. "Medical Hydrogeology of Asian Deltas: Status of Groundwater Toxicants and Nutrients, and Implications for Human Health" International Journal of Environmental Research and Public Health 13, no. 1: 81. https://doi.org/10.3390/ijerph13010081