
Impact on Mental Well-Being and Resilience of Patients with Multiple Chronic Conditions in Different Periods during the Coronavirus Disease 2019 Outbreak in Taiwan

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection Methods
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics of the Different Periods of the COVID-19 Outbreak in Taiwan
3.2. Variable Correlations
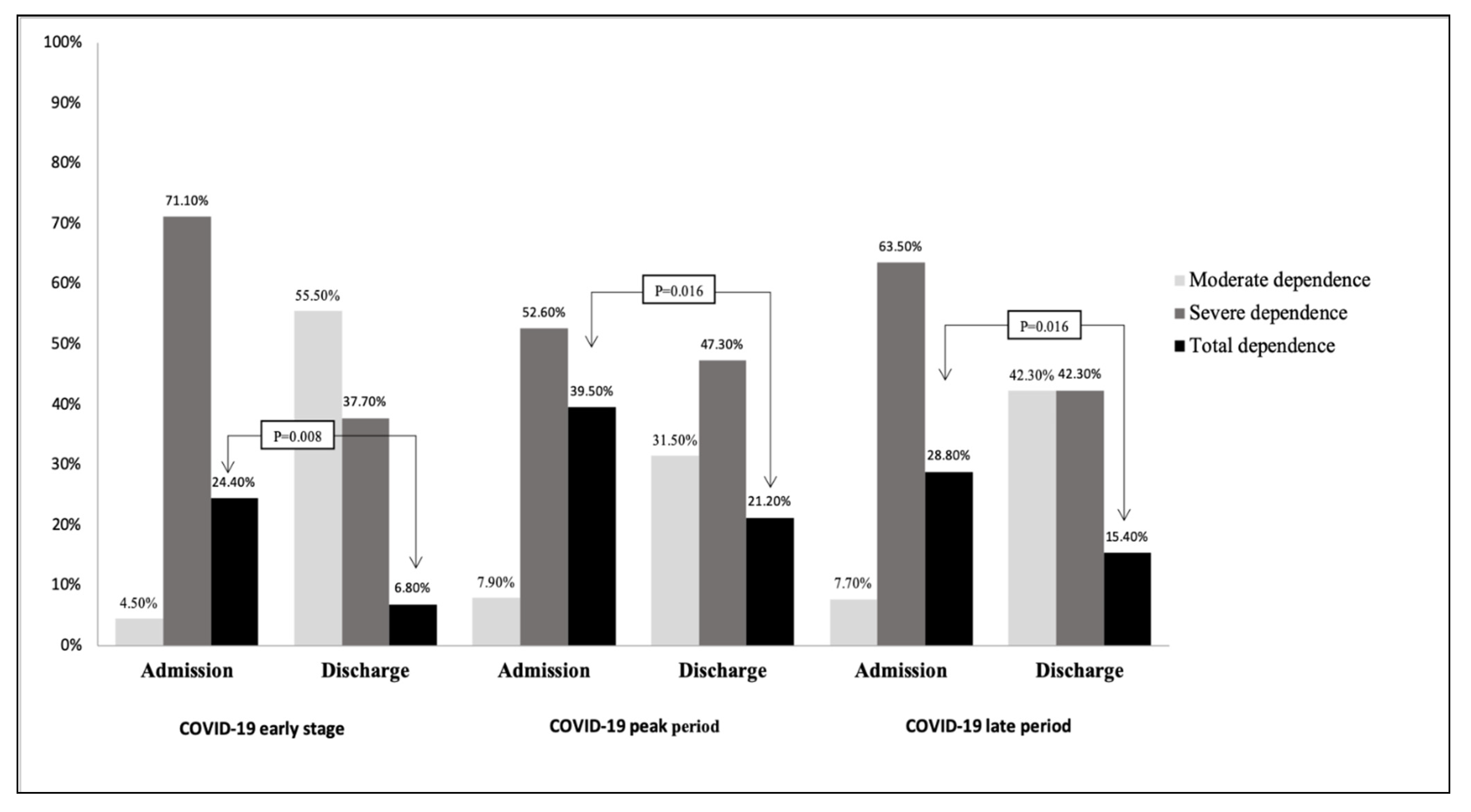
3.3. Activities of Daily Living at Admission and Discharge during the COVID-19 Outbreak in Taiwan
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loeffler-Wirth, H.; Schmidt, M.; Binder, H. Covid-19 transmission trajectories–monitoring the pandemic in the worldwide context. Viruses 2020, 12, 777. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fang, X.; Cai, Z.; Wu, X.; Gao, X.; Min, J.; Wang, F. Comorbid chronic diseases and acute organ injuries are strongly correlated with disease severity and mortality among COVID-19 patients: A systemic review and meta-analysis. Research 2020, 2020, 2402961. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Su, S.-F.; Han, Y.-Y. How Taiwan, a non-WHO member, takes actions in response to COVID-19. J. Glob. Health 2020, 10, 010380. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-P.; Yen, C.-F.; Wu, C.-F.; Wang, P.-W. Nonattendance at Scheduled Appointments in Outpatient Clinics Due to COVID-19 and Related Factors in Taiwan: A Health Belief Model Approach. Int. J. Environ. Res. Public Health 2021, 18, 4445. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.A.; Cahir, C.; Tecklenborg, S.; Byrne, C.; Culbertson, M.A.; Bennett, K.E. The association between medication non-adherence and adverse health outcomes in ageing populations: A systematic review and meta-analysis. Br. J. Clin. Pharmacol 2019, 85, 2464–2478. [Google Scholar] [CrossRef]
- Xue, Q.L.; Bandeen-Roche, K.; Tian, J.; Kasper, J.D.; Fried, L.P. Progression of Physical Frailty and the Risk of All-Cause Mortality: Is There a Point of No Return? J. Am. Geriatr. Soc. 2021, 69, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Casten, K.; Collins, S.; Hassan, H.; García-Hermoso, A.; Faul, J. Muscle weakness is a prognostic indicator of disability and chronic disease multimorbidity. Exp. Gerontol. 2021, 152, 111462. [Google Scholar] [CrossRef]
- Castellana, F.; Lampignano, L.; Bortone, I.; Zupo, R.; Lozupone, M.; Griseta, C.; Daniele, A.; De Pergola, G.; Giannelli, G.; Sardone, R. Physical frailty, multimorbidity, and all-cause mortality in an older population from southern italy: Results from the salus in apulia study. J. Am. Geriatr. Soc. 2021, 22, 598–605. [Google Scholar] [CrossRef]
- Chen, L.-K. Older adults and COVID-19 pandemic: Resilience matters. Arch. Gerontol. Geriatr. 2020, 89, 104124. [Google Scholar] [CrossRef]
- Han, B.H. Aging, multimorbidity, and substance use disorders: The growing case for integrating the principles of geriatric care and harm reduction. Int. J. Drug Policy 2018, 58, 135–136. [Google Scholar] [CrossRef]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110207. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.; Wood, A.M. Integrating positive and clinical psychology: Viewing human functioning as continua from positive to negative can benefit clinical assessment, interventions and understandings of resilience. Cognit. Ther. Res. 2017, 41, 335–349. [Google Scholar] [CrossRef] [Green Version]
- Papathanasiou, I.V.; Fradelos, E.C.; Mantzaris, D.; Rammogianni, A.; Malli, F.; Papagiannis, D.; Gourgoulianis, K.I. Multimorbidity, Trauma Exposure, and Frailty of Older Adults in the Community. Front. Genet. 2021, 12, 430. [Google Scholar] [CrossRef]
- Lara, R.; Vázquez, M.; Ogallar, A.; Godoy-Izquierdo, D. Psychosocial resources for hedonic balance, life satisfaction and happiness in the elderly: A path analysis. Int. J. Environ. Res. Public Health 2020, 17, 5684. [Google Scholar] [CrossRef]
- D’Hoore, W.; Bouckaert, A.; Tilquin, C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J. Clin. Epidemiol. 1996, 49, 1429–1433. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems; 10th Revision; World Health Organization: Geneva, Switzerland, 1992; Volume 341. [Google Scholar]
- Mahoney, F.I. Functional evaluation: The Barthel index. Md. Med. J. 1965, 14, 61–65. [Google Scholar]
- Wagnild, G.M.; Young, H.M. Development and psychometric. J. Nurs. Meas. 1993, 1, 165–17847. [Google Scholar]
- Dupuy, H.; McDowell, I.; Newell, C. The General Well-Being Schedule. Measuring Health: A Guide to Rating Scales and Questionnaires; Oxford University Press: Oxford, UK, 1977; pp. 206–213. [Google Scholar]
- Lee, Y.-J.; Hung, W.-L. The relationship between exercise participation and well-being of the retired elderly. Aging Ment. Health 2011, 15, 873–881. [Google Scholar] [CrossRef]
- Gluckman, T.J.; Wilson, M.A.; Chiu, S.-T.; Penny, B.W.; Chepuri, V.B.; Waggoner, J.W.; Spinelli, K.J. Case rates, treatment approaches, and outcomes in acute myocardial infarction during the coronavirus disease 2019 pandemic. JAMA Cardiol. 2020, 5, 1419–1424. [Google Scholar] [CrossRef]
- Motterle, G.; Morlacco, A.; Iafrate, M.; Bianco, M.; Federa, G.; Xhafka, O.; Zattoni, F.; Prayer-Galetti, T. The impact of COVID-19 pandemic on urological emergencies: A single-center experience. World J. Urol. 2021, 39, 1985–1989. [Google Scholar] [CrossRef] [PubMed]
- Son, J.S.; Nimrod, G.; West, S.T.; Janke, M.C.; Liechty, T.; Naar, J.J. Promoting older adults’ physical activity and social well-being during COVID-19. Leis. Sci. 2021, 43, 287–294. [Google Scholar] [CrossRef]
- Wongtanasarasin, W.; Srisawang, T.; Yothiya, W.; Phinyo, P. Impact of national lockdown towards emergency department visits and admission rates during the COVID-19 pandemic in Thailand: A hospital-based study. Emerg. Med. Australas. 2021, 33, 316–323. [Google Scholar] [CrossRef]
- Kimmel, S.D.; Bazzi, A.R.; Barocas, J.A. Integrating harm reduction and clinical care: Lessons from Covid-19 respite and recuperation facilities. J. Subst. Abuse Treat. 2020, 118, 108103. [Google Scholar] [CrossRef] [PubMed]
- Amieva, H.; Avila-Funes, J.-A.; Caillot-Ranjeva, S.; Dartigues, J.-F.; Koleck, M.; Letenneur, L.; Pech, M.; Peres, K.; Raoux, N.; Rascle, N.; et al. Older People Facing the Crisis of COVID-19: Between Fragility and Resilience. J. Frailty Aging 2021, 10, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.G.; Carr, D. Psychological resilience and health among older adults: A comparison of personal resources. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 1241–1250. [Google Scholar] [CrossRef]
- Grossman, E.S.; Hoffman, Y.S.; Palgi, Y.; Shrira, A. COVID-19 related loneliness and sleep problems in older adults: Worries and resilience as potential moderators. Pers. Individ. Differ. 2021, 168, 110371. [Google Scholar] [CrossRef]
- Zhang, K.; Zhang, W.; Wu, B.; Liu, S. Anxiety about aging, resilience and health status among Chinese older adults: Findings from Honolulu and Wuhan. Arch. Gerontol. Geriatr. 2020, 88, 104015. [Google Scholar] [CrossRef]
- Sabatini, S.; Silarova, B.; Martyr, A.; Collins, R.; Ballard, C.; Anstey, K.J.; Kim, S.; Clare, L. Associations of awareness of age-related change with emotional and physical well-being: A systematic review and meta-analysis. Gerontologist 2020, 60, e477–e490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giebel, C.; Ivan, B.; Ddumba, I. COVID-19 Public Health Restrictions and Older Adults’ Well-being in Uganda: Psychological Impacts and Coping Mechanisms. Clin. Gerontol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Güler, A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Pers. Individ. Differ. 2021, 168, 110347. [Google Scholar] [CrossRef]
- Dini, M.; Poletti, B.; Tagini, S.; Reitano, M.R.; Allocco, E.; Mazzocco, K.; Pravettoni, G.; Dell’Osso, B.; Monforte, A.D.A.; Centanni, S.; et al. Resilience, Psychological Well-Being and Daily Functioning Following Hospitalization for Respiratory Distress Due to SARS-CoV-2 Infection. Healthcare 2021, 9, 1161. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.-H.; Lin, C.-Y.; Hung, C.-T.; He, J.-J.; Lu, P.-L. The impact of universal face masking and enhanced hand hygiene for COVID-19 disease prevention on the incidence of hospital-acquired infections in a Taiwanese hospital. Int. J. Infect. Dis. 2021, 104, 15–18. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, in press. [Google Scholar] [CrossRef]
- Wang, W.; Tang, J.; Wei, F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J. Med. Virol. 2020, 92, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Paredes, M.R.; Apaolaza, V.; Fernandez-Robin, C.; Hartmann, P.; Yañez-Martinez, D. The impact of the COVID-19 pandemic on subjective mental well-being: The interplay of perceived threat, future anxiety and resilience. Pers. Individ. Differ. 2021, 170, 110455. [Google Scholar] [CrossRef]
- Kendzerska, T.; Zhu, D.T.; Gershon, A.S.; Edwards, J.D.; Peixoto, C.; Robillard, R.; Kendall, C.E. The effects of the health system response to the COVID-19 pandemic on chronic disease management: A narrative review. Risk Manag. Healthc. Policy 2021, 14, 575. [Google Scholar] [CrossRef]
- Omboni, S.; Ballatore, T.; Rizzi, F.; Tomassini, F.; Panzeri, E.; Campolo, L. Telehealth at scale can improve chronic disease management in the community during a pandemic: An experience at the time of COVID-19. PLoS ONE 2021, 16, e0258015. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.G.; Marques, G.; Barrachina, I.; Garcia-Zapirain, B.; Arambarri, J.; Salvador, J.C.; de la Torre Díez, I. Telemedicine and e-Health research solutions in literature for combatting COVID-19: A systematic review. Health Technol. 2021, 11, 257–266. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | COVID-19 Early Stage | COVID-19 Peak Period | COVID-19 Late Period | F | p |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
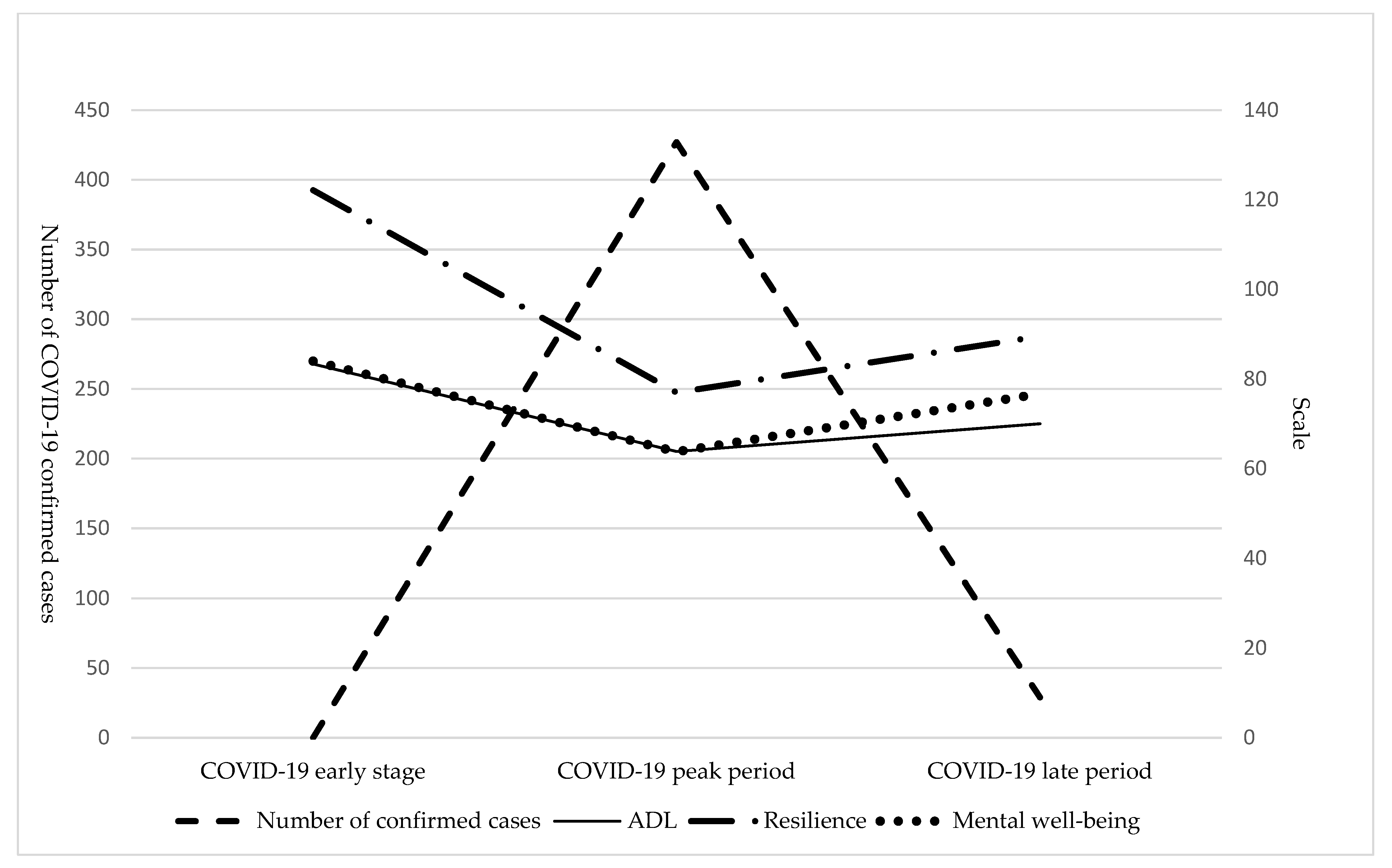
| Number of COVID-19 cases | 0 | 428 | 29 | ||
| n/N | 45/263 (17.1) | 38/224 (16.9) | 52/312 (17.0) | 0.822 | 0.442 |
| Age, mean ± SD, years | 61.27 ± 16.37 | 64.74 ± 17.48 | 58.75 ± 19.33 | 1.233 | 0.295 |
| Visits per month | |||||
| OPD | 184,294 | 147,457 | 168,312 | 4.530 | <0.001 |
| ED | 9861 | 8888 | 9482 | 1.246 | <0.001 |
| Sex | 0.552 | 0.577 | |||
| Male | 31 (68.9) | 22 (57.9) | 34 (65.4) | ||
| Female | 14 (31.1) | 16 (42.1) | 18 (34.6) | ||
| Marital status | 1.961 | 0.145 | |||
| Single | 7 (15.6) | 4 (10.5) | 12 (23.1) | ||
| Married/cohabitating | 37 (82.2) | 30 (78.9) | 37 (71.2) | ||
| Divorced/widowed | 1 (2.2) | 4 (7.9) | 3 (5.7) | ||
| Education level | 0.837 | 0.435 | |||
| Above college | 7 (15.6) | 5 (13.2) | 7 (13.5) | ||
| Senior or junior high school | 20 (44.4) | 15 (39.5) | 30 (57.7) | ||
| Below elementary school | 18 (40.0) | 18 (47.4) | 15 (28.8) | ||
| Employed | 0.252 | 0.777 | |||
| No | 28 (62.2) | 26 (68.4) | 32 (61.5) | ||
| Yes | 17 (37.8) | 12 (31.6) | 20 (38.5) | ||
| Religion | 0.777 | 0.462 | |||
| Yes | 30 (66.7) | 30 (78.9) | 38 (73.1) | ||
| No | 15 (33.3) | 8 (21.1) | 14 (26.9) | ||
| Acute diseases at admission | 0.892 | 0.412 | |||
| Certain infectious diseases | 19 (42.2) | 21 (55.3) | 26 (50.0) | ||
| Diseases of the circulatory system | 3 (6.7) | 3 (7.9) | 3 (5.8) | ||
| Diseases of the digestive system | 13 (28.9) | 5 (13.2) | 15 (28.8) | ||
| Diseases of the genitourinary system | 1 (2.2) | 4 (10.5) | 4 (7.7) | ||
| Diseases of the nervous system | 9 (20.0) | 5 (13.1) | 4 (7.7) | ||
| Income quartiles | 1.248 | 0.290 | |||
| 1 (Poorest) | 8 (17.8) | 3 (7.9) | 4 (7.7) | ||
| 2 (Poorer) | 11 (24.4) | 10 (26.3) | 14 (26.9) | ||
| 3 (Middle) | 23 (51.1) | 19 (50.0) | 29 (55.8) | ||
| 4 (Wealthiest) | 3 (6.7) | 6 (15.8) | 5 (9.6) |
| Variable | COVID-19 Early Stage | COVID-19 Peak Period | COVID-19 Late Period | F | p |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| CCI | 4.13 ± 1.79 | 4.53 ± 2.05 | 3.69 ± 2.08 | 1.977 | 0.143 |
| ADL | 83.33 ± 26.37 | 63.82 ± 35.27 | 70.00 ± 32.30 | 4.304 | 0.015 |
| Resilience scale | 122.11 ± 21.14 | 76.97 ± 20.46 | 89.52 ± 35.48 | 30.912 | <0.001 |
| Mental well-being scale | 83.98 ± 12.32 | 63.76 ± 11.37 | 76.71 ± 18.93 | 18.961 | <0.001 |
| Variable | COVID-19 | CCI | OPD | ED | ADL | Resilience Scale | Mental Well-Being Scale | |
|---|---|---|---|---|---|---|---|---|
| COVID-19 | r | 1 | 0.176 | −0.764 | −0.023 | −0.257 | −0.390 | −0.475 |
| p | 0.041 | <0.001 | 0.788 | 0.003 | <0.001 | <0.001 | ||
| CCI | r | 1 | −0.080 | 0.094 | −0.535 | −0.240 | −0.257 | |
| p | 0.358 | 0.278 | <0.001 | 0.005 | 0.003 | |||
| OPD | r | 1 | 0.455 | 0.268 | 0.553 | 0.439 | ||
| p | <0.001 | 0.002 | <0.001 | <0.001 | ||||
| ED | r | 1 | 0.209 | 0.346 | 0.172 | |||
| p | 0.015 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, Y.-Y.; Chen, Y.-C.; Hsu, T.-W.; Zhong, H.-R.; Cheng, B.-C.; Lee, C.-T.; Lee, C.-H. Impact on Mental Well-Being and Resilience of Patients with Multiple Chronic Conditions in Different Periods during the Coronavirus Disease 2019 Outbreak in Taiwan. Healthcare 2021, 9, 1457. https://doi.org/10.3390/healthcare9111457
Kao Y-Y, Chen Y-C, Hsu T-W, Zhong H-R, Cheng B-C, Lee C-T, Lee C-H. Impact on Mental Well-Being and Resilience of Patients with Multiple Chronic Conditions in Different Periods during the Coronavirus Disease 2019 Outbreak in Taiwan. Healthcare. 2021; 9(11):1457. https://doi.org/10.3390/healthcare9111457
Chicago/Turabian StyleKao, Yu-Yin, Yi-Chun Chen, Tsuen-Wei Hsu, Hua-Rong Zhong, Ben-Chung Cheng, Chien-Te Lee, and Chen-Hsiang Lee. 2021. "Impact on Mental Well-Being and Resilience of Patients with Multiple Chronic Conditions in Different Periods during the Coronavirus Disease 2019 Outbreak in Taiwan" Healthcare 9, no. 11: 1457. https://doi.org/10.3390/healthcare9111457