
Stringent Nonpharmaceutical Interventions Are Crucial for Curbing COVID-19 Transmission in the Course of Vaccination: A Case Study of South and Southeast Asian Countries

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Model
2.3. Parameter Estimation
2.4. Design of Experiments
3. Results and Analysis
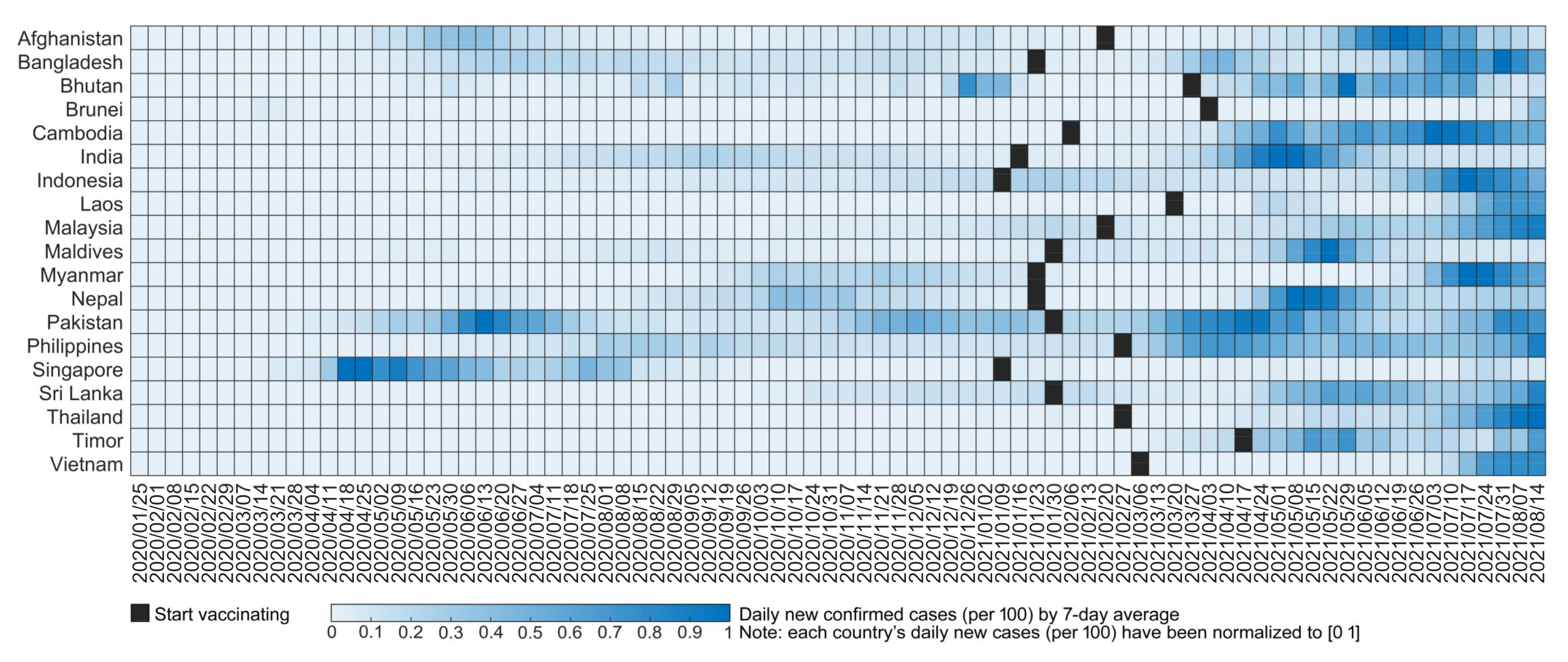
3.1. Retrospective Analysis of the Impact of Intervention Measures on Daily New Cases
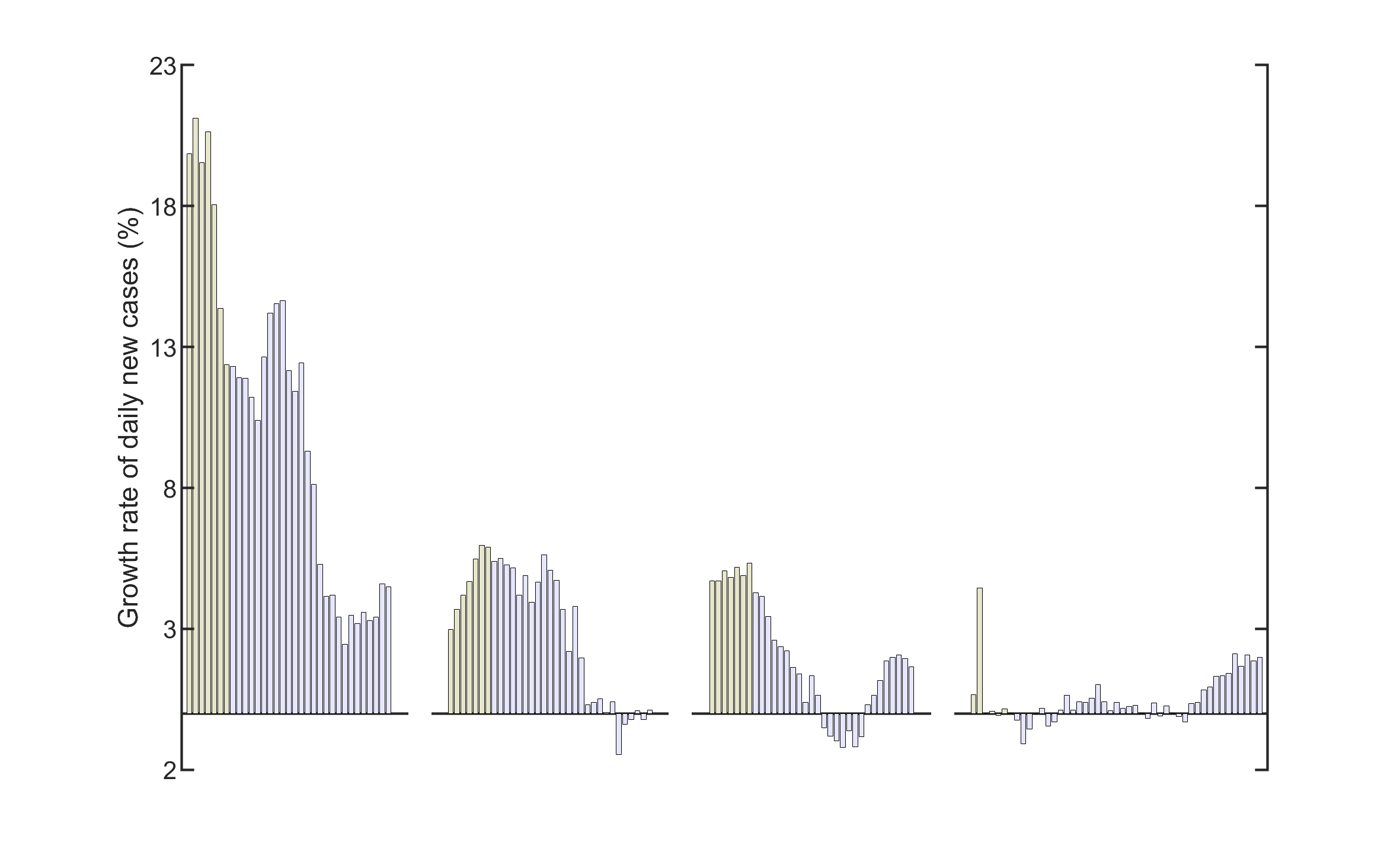
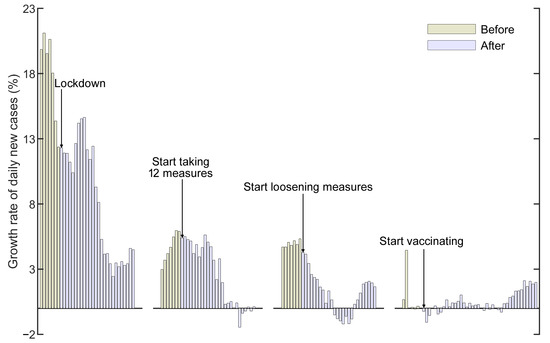
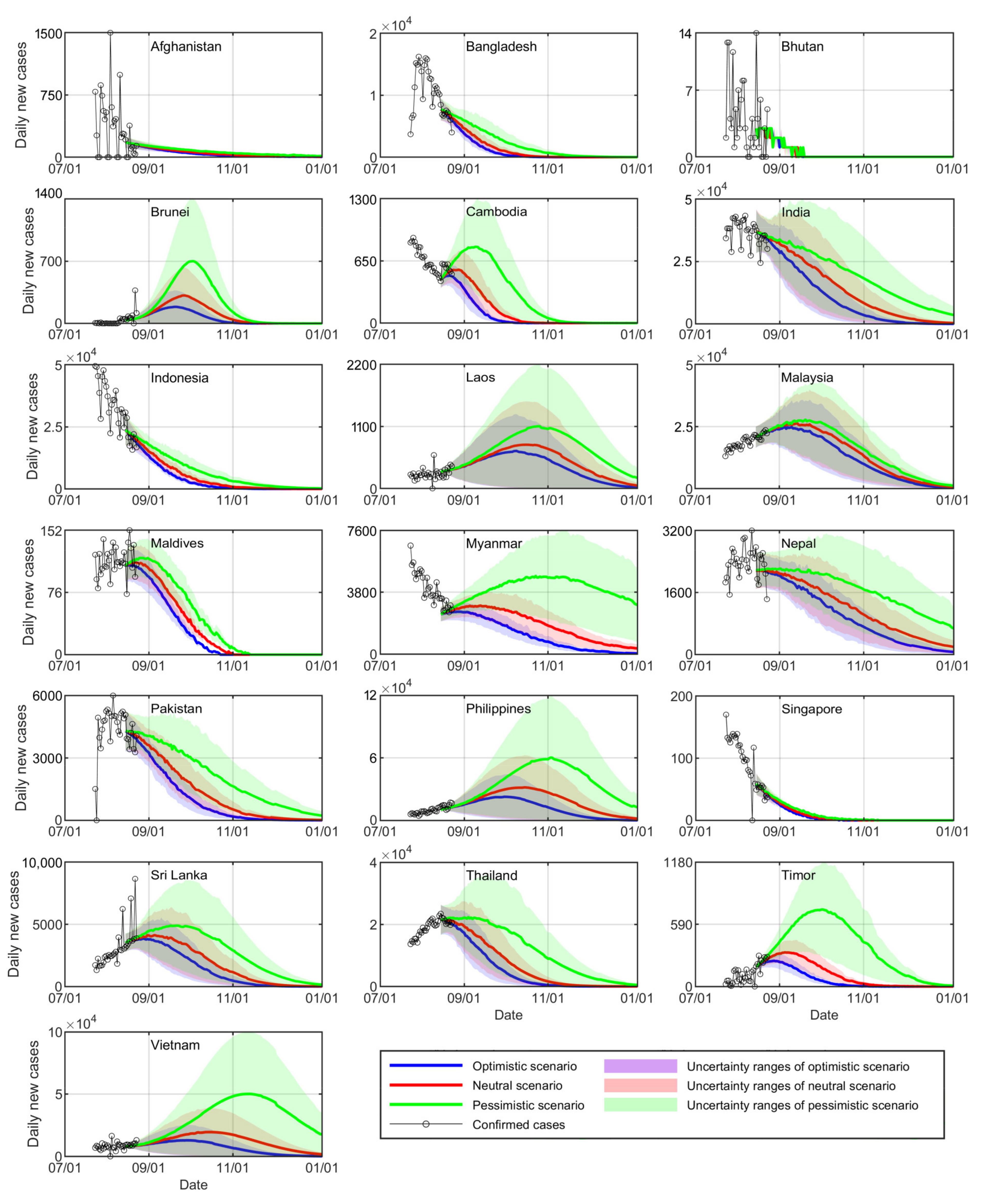
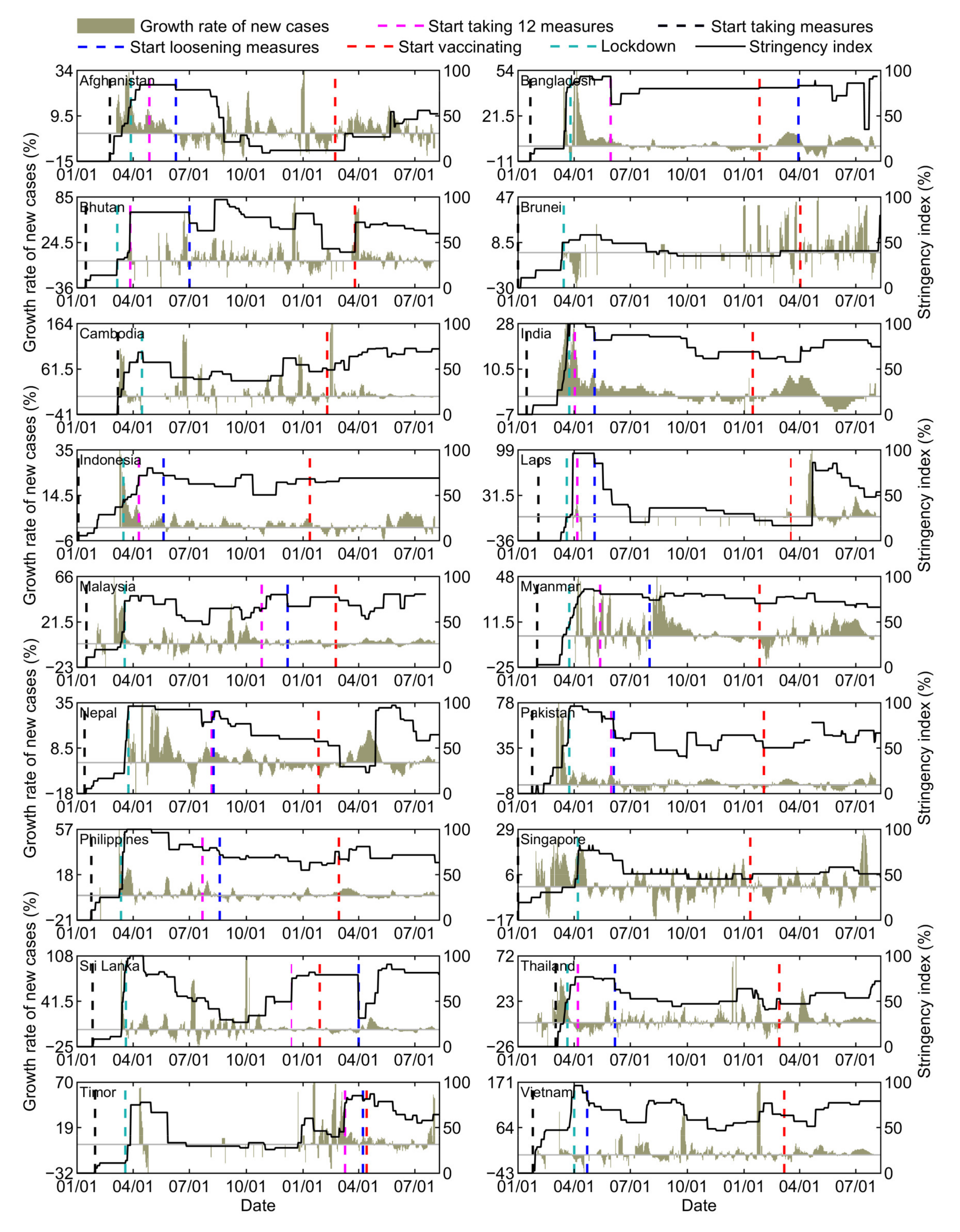
3.2. Retrospective Analysis of the Growth Rate for Daily New Cases
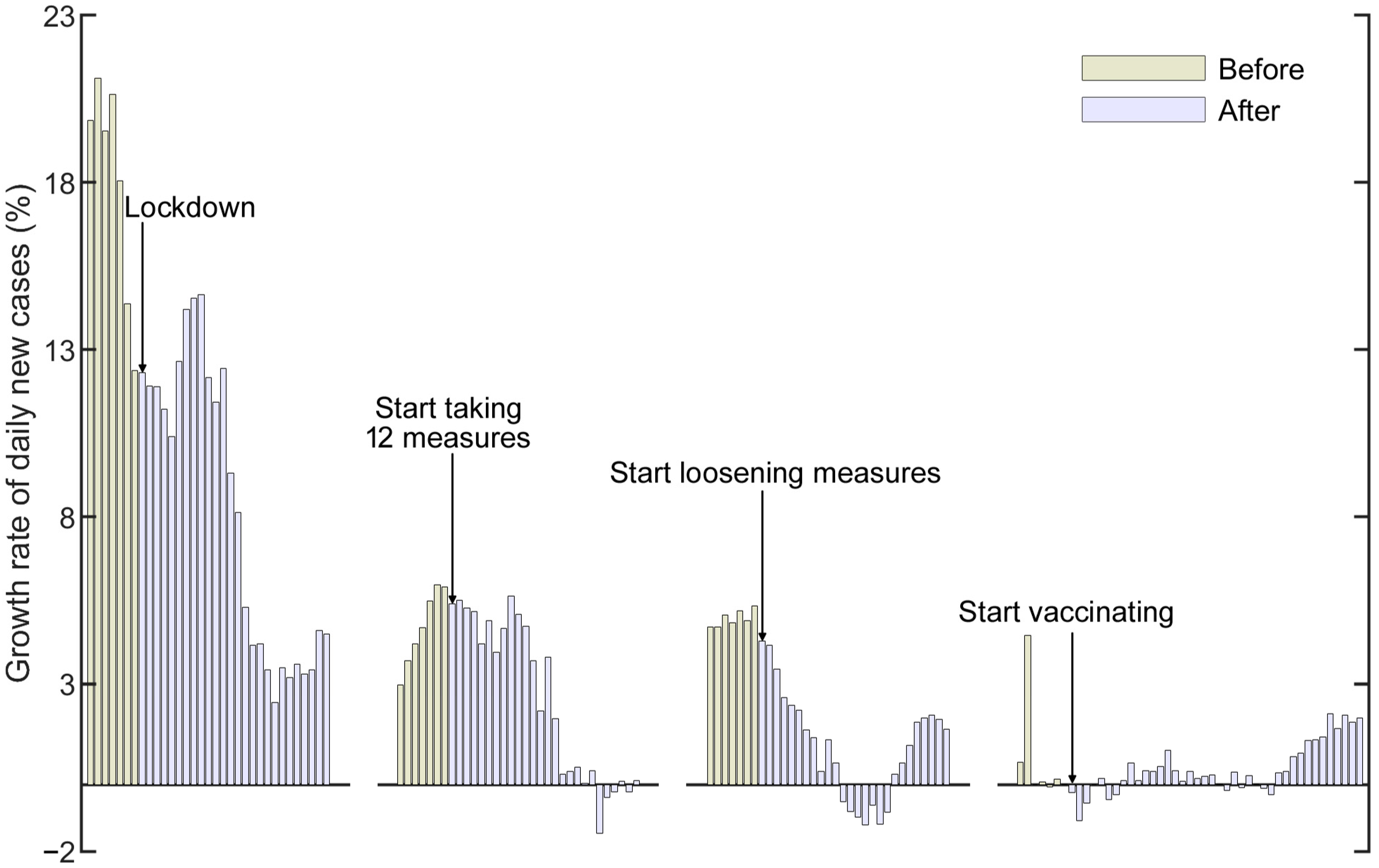
3.3. Prediction of the Spread of COVID-19 in South and Southeast Asia
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B
References
- Uzoh, B.C. Socio-economic effects of COVID-19 pandemic on the Nigeria working class. Soc. J. Soc. Sci. Humanit. 2020, 5, 40–54. [Google Scholar]
- Jiao, N.; Chen, F.; Hou, Z. Combating climate change in a post-COVID-19 era. Sci. Bull. 2020, 65, 1958–1960. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, J.; Meadows, M.E.; Liu, Y.; Hua, T.; Fu, B. A systematic approach is needed to contain COVID-19 globally. Sci. Bull. 2020, 65, 876–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasul, G.; Nepal, A.K.; Hussain, A.; Maharjan, A.; Joshi, S.; Lama, A.; Gurung, P.; Ahmad, F.; Mishra, A.; Sharma, E. Socio-Economic Implications of COVID-19 Pandemic in South Asia: Emerging Risks and Growing Challenges. Front. Sociol. 2021, 6, 629693. [Google Scholar] [CrossRef]
- Burzynska, K.; Contreras, G. Gendered effects of school closures during the COVID-19 pandemic. Lancet 2020, 395, 1968. [Google Scholar] [CrossRef]
- Gabster, B.P.; van Daalen, K.; Dhatt, R.; Barry, M. Challenges for the female academic during the COVID-19 pandemic. Lancet 2020, 395, 1968–1970. [Google Scholar] [CrossRef]
- Romero-Brufau, S.; Chopra, A.; Ryu, A.J.; Gel, E.; Raskar, R.; Kremers, W.; Anderson, K.S.; Subramanian, J.; Krishnamurthy, B.; Singh, A. Public health impact of delaying second dose of BNT162b2 or mRNA-1273 COVID-19 vaccine: Simulation agent based modeling study. BMJ 2021, 373, n1087. [Google Scholar] [CrossRef]
- Kuppalli, K.; Gala, P.; Cherabuddi, K.; Kalantri, S.; Mohanan, M.; Mukherjee, B.; Pinto, L.; Prakash, M.; Pramesh, C.; Rathi, S. India’s COVID-19 crisis: A call for international action. Lancet 2021, 397, 2132–2135. [Google Scholar] [CrossRef]
- Sohn, A.H.; Phanuphak, N.; Baral, S.; Kamarulzaman, A. Know your epidemic, know your response: Understanding and responding to the heterogeneity of the COVID-19 epidemics across Southeast Asia. J. Int. AIDS Soc. 2020, 23, e25557. [Google Scholar] [CrossRef]
- Chalise, H.N. South Asia is more vulnerable to COVID-19 pandemic. Arch. Psychiatr. Ment. Health 2020, 4, 46–47. [Google Scholar]
- Chookajorn, T.; Kochakarn, T.; Wilasang, C.; Kotanan, N.; Modchang, C. Southeast Asia is an emerging hotspot for COVID-19. Nat. Med. 2021, 27, 1495–1496. [Google Scholar] [CrossRef]
- Fauzi, M.A.; Paiman, N. COVID-19 pandemic in Southeast Asia: Intervention and mitigation efforts. Asian Educ. Dev. Stud. 2020, 10, 176–184. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, X.; Zhao, Z.; Ma, C.; Nie, X. Return to normal pre-COVID-19 life is delayed by inequitable vaccine allocation and SARS-CoV-2 variants. J. Infect Public Health 2021. submitted for publication. [Google Scholar]
- Gumel, A.B.; Iboi, E.A.; Ngonghala, C.N.; Ngwa, G.A. Towards achieving a vaccine-derived herd immunity threshold for COVID-19 in the US. Front. Public Health 2021, 9, 709369. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Britton, T.; Ball, F.; Trapman, P. A mathematical model reveals the influence of population heterogeneity on herd immunity to SARS-CoV-2. Science 2020, 369, 846–849. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G. Effectiveness of COVID-19 vaccines against the B. 1.617. 2 (Delta) variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- De Deyn, M.L.Z.Q.; Ng, Q.X.; Loke, W.; Yeo, W.S. A tale of two cities: A comparison of Hong Kong and Singapore’s early strategies for the Coronavirus Disease 2019 (COVID-19). J. Infect. 2020, 81, e51–e52. [Google Scholar] [CrossRef]
- Lyu, W.; Wehby, G.L. Community Use Of Face Masks And COVID-19: Evidence From A Natural Experiment Of State Mandates In The US: Study examines impact on COVID-19 growth rates associated with state government mandates requiring face mask use in public. Health Aff. 2020, 39, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- An, B.Y.; Porcher, S.; Tang, S.-Y.; Kim, E.E. Policy Design for COVID-19: Worldwide Evidence on the Efficacies of Early Mask Mandates and Other Policy Interventions. Available online: https://www.imf.org/en/Topics/imf-and-COVID19/Policy-Responses-to-COVID-19 (accessed on 2 July 2021).
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef]
- An, B.Y.; Tang, S.-Y. Lessons from COVID-19 responses in East Asia: Institutional infrastructure and enduring policy instruments. Am. Rev. Public Adm. 2020, 50, 790–800. [Google Scholar] [CrossRef]
- Cheng, C.; Barceló, J.; Hartnett, A.S.; Kubinec, R.; Messerschmidt, L. COVID-19 government response event dataset (CoronaNet v. 1.0). Nat. Hum. Behav. 2020, 4, 756–768. [Google Scholar] [CrossRef]
- Porcher, S. Response2COVID19, a dataset of governments’ responses to COVID-19 all around the world. Sci. Data 2020, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Porcher, S.; Renault, T. Social distancing beliefs and human mobility: Evidence from Twitter. PLoS ONE 2021, 16, e0246949. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Wang, J.; Cai, J.; Yao, S.; Chan, P.K.S.; Tam, T.H.-W.; Hong, Y.-Y.; Ruktanonchai, C.W.; Carioli, A.; Floyd, J.R. Integrated vaccination and physical distancing interventions to prevent future COVID-19 waves in Chinese cities. Nat. Hum. Behav. 2021, 5, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Liao, S.-H.; Lai, C.-C.; Paci, E.; Chuang, S.-Y. Effectiveness of Non-Pharmaceutical Interventions and Vaccine for Containing the Spread of COVID-19: Three Illustrations Before and After Vaccination Periods. J. Formos. Med. Assoc. 2021, 120, S46–S56. [Google Scholar] [CrossRef]
- Castillo, J.C.; Ahuja, A.; Athey, S.; Baker, A.; Budish, E.; Chipty, T.; Glennerster, R.; Kominers, S.D.; Kremer, M.; Larson, G. Market design to accelerate COVID-19 vaccine supply. Science 2021, 371, 1107–1109. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Hale, T.; Petherick, A.; Phillips, T.; Webster, S. Variation in Government Responses to COVID-19; Blavatnik School of Government, University of Oxford: Oxford, UK, 2020. [Google Scholar]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Zeng, Z.; Wang, K.; Wong, S.-S.; Liang, W.; Zanin, M.; Liu, P.; Cao, X.; Gao, Z.; Mai, Z. Modified SEIR and AI prediction of the epidemics trend of COVID-19 in China under public health interventions. J. Thorac. Dis. 2020, 12, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Liu, Y.; Li, Y.; Wu, C.-H.; Chen, B.; Kraemer, M.U.; Li, B.; Cai, J.; Xu, B.; Yang, Q. An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science 2020, 368, 638–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Li, X.; Liu, F.; Zhu, G.; Ma, C.; Wang, L. Prediction of the COVID-19 spread in African countries and implications for prevention and control: A case study in South Africa, Egypt, Algeria, Nigeria, Senegal and Kenya. Sci. Total Environ. 2020, 729, 138959. [Google Scholar] [CrossRef]
- Gao, S.; Teng, Z.; Nieto, J.J.; Torres, A. Analysis of an SIR epidemic model with pulse vaccination and distributed time delay. J. Biomed. Biotechnol. 2007, 2007, 064870. [Google Scholar] [CrossRef]
- Schlickeiser, R.; Kröger, M. Analytical Modeling of the Temporal Evolution of Epidemics Outbreaks Accounting for Vaccinations. Physics 2021, 3, 386–426. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: Novavax Vaccine Efficacy Is 86% against UK variant and 60% against South African Variant. BMJ. 2021, 372, n296. [Google Scholar] [CrossRef]
- Salzman, S. Johnson & Johnson Single-Shot Vaccine 85% Effective against Severe COVID-19 Disease. ABC News 2021. Available online: https://abcnews.go.com/Health/johnson-johnson-single-shot-vaccine-85-effective-severe/story?id=75557358 (accessed on 29 January 2021).
- Brooks-Pollock, E.; Christensen, H.; Trickey, A.; Hemani, G.; Nixon, E.; Thomas, A.C.; Turner, K.; Finn, A.; Hickman, M.; Relton, C.; et al. High COVID-19 transmission potential associated with re-opening universities can be mitigated with layered interventions. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Peng, Y.; Sun, K. SEIR modeling of the COVID-19 and its dynamics. Nonlinear Dyn. 2020, 101, 1667–1680. [Google Scholar] [CrossRef] [PubMed]
- Roda, W.C.; Varughese, M.B.; Han, D.; Li, M.Y. Why is it difficult to accurately predict the COVID-19 epidemic? Infect. Dis. Model. 2020, 5, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Li, X.; Zhao, Z.; Liu, F.; Zhang, K.; Wu, A. Understanding the dynamics of pandemic models to support predictions of COVID-19 transmission: Parameter sensitivity analysis of the SIR-type model. Appl. Math. Model. 2021. submitted for publication. [Google Scholar]
- King, A.A.; Ionides, E.L.; Pascual, M.; Bouma, M.J. Inapparent infections and cholera dynamics. Nature 2008, 454, 877–880. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Z.; Liu, F. Big data assimilation to improve the predictability of COVID-19. Geogr. Sustain. 2020, 1, 317–320. [Google Scholar]
- Liu, F.; Li, X.; Zhu, G. Using the contact network model and Metropolis-Hastings sampling to reconstruct the COVID-19 spread on the “Diamond Princess”. Sci. Bull. 2020, 65, 1297–1305. [Google Scholar] [CrossRef]
- Zhu, G.; Li, X.; Su, Y.; Zhang, K.; Bai, Y.; Ma, J.; Li, C.; Hu, X.; He, J. Simultaneous parameterization of the two-source evapotranspiration model by Bayesian approach: Application to spring maize in an arid region of northwest China. Geosci. Model Dev. 2014, 7, 741–775. [Google Scholar] [CrossRef] [Green Version]
- Zhu, G.; Li, X.; Ma, J.; Wang, Y.; Liu, S.; Huang, C.; Zhang, K.; Hu, X. A new moving strategy for the sequential Monte Carlo approach in optimizing the hydrological model parameters. Adv. Water Resour. 2018, 114, 164–179. [Google Scholar] [CrossRef]
- Hilley, G.; Young, J. Deducing Paleoearthquake Timing and Recurrence from Paleoseismic Data, Part I: Evaluation of New Bayesian Markov-Chain Monte Carlo Simulation Methods Applied to Excavations with Continuous Peat GrowthDeducing Paleoearthquake Timing and Recurrence from Paleoseismic Data, Part I. Bull. Seismol. Soc. Am. 2008, 98, 383–406. [Google Scholar]
- Giordano, G.; Colaneri, M.; Di Filippo, A.; Blanchini, F.; Bolzern, P.; De Nicolao, G.; Sacchi, P.; Colaneri, P.; Bruno, R. Modeling vaccination rollouts, SARS-CoV-2 variants and the requirement for non-pharmaceutical interventions in Italy. Nat. Med. 2021, 27, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Cheng, G.; Wang, L.; Wang, J.; Ran, Y.; Che, T.; Li, G.; He, H.; Zhang, Q.; Jiang, X.; et al. Boosting geoscience data sharing in China. Nat. Geosci. 2021, 14, 541–542. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prevention and Control Measures | Detailed Measures (Identity Code) | Corresponding Measures (Intensity) |
|---|---|---|
| Closures and containment measures | School closures (C1) | Complete closure (3), partial suspension (2), suggested closure (1), no measures (0) |
| Workplace closures (C2) | Closure of all nonessential workplaces (3), closure of several workplaces (2), suggested closure (1), no measures (0) | |
| Public event cancellations (C3) | Mandatory cancellation (2), suggested cancellation (1), no measures (0) | |
| Restrictions on gatherings (C4) | No more than 10 people (4), no more than 100 people (3), no more than 1000 people (2), limits only on major events (1), no measures (0) | |
| Public transport closures (C5) | Complete closure (2), suggested closure (1), no measures (0) | |
| Stay at home requirements (C6) | Home except for special events (3), home except for daily activities (2), no measures (0) | |
| Restrictions on internal movement (C7) | Regional/local movement restrictions (2), interregional movement restrictions (1), no measures (0) | |
| Restrictions on international travel (C8) | Closure of all borders (4), closure of selective borders (3), high-risk imports quarantined (2), screenings (1), no measures (0) | |
| Economic measures | Income support (E1) | Government subsidizes more than 50% of wages (2), government subsidizes less than 50% of wages (1), no measures (0) |
| Debt/contract relief for households (E2) | Broad relief (2), targeted extensions (1), no measures (0) | |
| Public health measures | Public information campaigns (H1) | Extensive publicity (2), government supervised campaigns (1), no measures (0) |
| Testing policies (H2) | Extensive testing (3), symptomatic testing (2), symptomatic testing under specific criteria (1), no measures (0) | |
| Contact tracing (H3) | Trace all contacts (2), trace limited contacts (1), no measures (0) | |
| Face coverings (H4) | Always (4), in public spaces (3), social distancing when possible (2), recommended (1), no measures (0) | |
| Vaccination policies (H5) | Universal availability (5), key groups (essential workers/clinically vulnerable groups/elderly groups) and broad groups/ages (4), key groups only (3), two-thirds of key groups (2), one-third of key groups (1), no measures (0) |
| Country | Growth Rate of Daily New Cases | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Before Lockdown | After Lockdown | Before Adopting Measures (C1–C8 and H1–H4) | After Adopting Measures (C1–C8 and H1–H4) | Before Loosening Measures | After Loosening Measures | Before Vaccination | After Vaccination I | After Vaccination II | |
| Afghanistan | 20.35% | 6.43% | 6.28% | 6.41% | 0.79% | −1.20% | −3.59% | 3.73% | 6.93% |
| Bangladesh | 21.54% | 15.15% | 3.94% | 1.18% | 8.42% | −4.72% | −3.19% | 0.53% | 5.42% |
| Bhutan | —— | —— | —— | —— | 22.00% | 4.25% | —— | 7.25% | 5.02% |
| Brunei | 4.89% | −18.30% | —— | —— | —— | —— | 16.71% | 19.23% | −1.31% |
| Cambodia | −7.40% | 0.00% | —— | —— | —— | —— | 2.87% | 1.87% | 1.73% |
| India | 20.35% | 6.30% | 18.33% | 4.56% | 5.89% | 4.01% | −1.33% | −0.95% | 2.21% |
| Indonesia | 48.65% | 6.77% | 7.05% | 1.56% | 3.89% | 4.03% | 2.59% | −1.58% | −0.71% |
| Laos | —— | —— | —— | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| Malaysia | 23.35% | −1.75% | 4.46% | 1.82% | −0.88% | 2.42% | −1.54% | −1.13% | −0.44% |
| Myanmar | —— | —— | 8.96% | 16.23% | 5.90% | 29.97% | −2.21% | −6.51% | −0.04% |
| Nepal | —— | —— | 7.15% | 3.24% | 7.65% | 2.69% | −2.87% | −1.08% | −1.32% |
| Pakistan | 36.43% | 7.28% | 5.36% | −3.36% | 5.39% | −4.59% | −2.07% | 1.21% | 5.10% |
| Philippines | 70.11% | 5.52% | 0.77% | 0.07% | 0.07% | 1.40% | 1.90% | 5.30% | 0.95% |
| Singapore | 7.38% | −2.32% | —— | —— | —— | —— | 6.63% | −1.71% | −5.01% |
| Sri Lanka | 66.39% | 1.07% | 1.26% | −0.10% | −2.20% | 14.06% | 1.76% | −4.23% | −2.16% |
| Thailand | 38.47% | −7.90% | −2.28% | −8.85% | 11.61% | 5.17% | −4.79% | 4.24% | 15.43% |
| Timor | —— | —— | —— | 1.29% | 2.15% | 4.14% | 3.62% | 4.93% | 1.36% |
| Vietnam | 4.34% | −29.42% | 4.34% | —— | −25.80% | −0.34% | −3.10% | 12.77% | 3.80% |
| Average | 27.30% | −0.86% | 5.47% | 1.85% | 2.98% | 4.09% | 0.67% | 2.44% | 2.05% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Z.; Li, X.; Liu, F.; Jin, R.; Ma, C.; Huang, B.; Wu, A.; Nie, X. Stringent Nonpharmaceutical Interventions Are Crucial for Curbing COVID-19 Transmission in the Course of Vaccination: A Case Study of South and Southeast Asian Countries. Healthcare 2021, 9, 1292. https://doi.org/10.3390/healthcare9101292
Zhao Z, Li X, Liu F, Jin R, Ma C, Huang B, Wu A, Nie X. Stringent Nonpharmaceutical Interventions Are Crucial for Curbing COVID-19 Transmission in the Course of Vaccination: A Case Study of South and Southeast Asian Countries. Healthcare. 2021; 9(10):1292. https://doi.org/10.3390/healthcare9101292
Chicago/Turabian StyleZhao, Zebin, Xin Li, Feng Liu, Rui Jin, Chunfeng Ma, Bo Huang, Adan Wu, and Xiaowei Nie. 2021. "Stringent Nonpharmaceutical Interventions Are Crucial for Curbing COVID-19 Transmission in the Course of Vaccination: A Case Study of South and Southeast Asian Countries" Healthcare 9, no. 10: 1292. https://doi.org/10.3390/healthcare9101292