
Overview of Multi-Modal Brain Tumor MR Image Segmentation


1
School of Information Science and Engineering, Linyi University, Linyi 276000, China
2
Shandong Provincial Key Laboratory of Network Based Intelligent Computing, Jinan 250022, China
3
School of Control Science and Engineering, Shandong University, Jinan 250061, China
4
School of Computer and Communication Engineering, University of Science and Technology Beijing, Beijing 100083, China
*
Author to whom correspondence should be addressed.
Healthcare 2021, 9(8), 1051; https://doi.org/10.3390/healthcare9081051
Submission received: 23 June 2021
/
Revised: 8 August 2021
/
Accepted: 10 August 2021
/
Published: 16 August 2021
(This article belongs to the Special Issue Artificial Intelligence (AI) and Machine Learning (ML) in Human Health and Healthcare)
Abstract
:The precise segmentation of brain tumor images is a vital step towards accurate diagnosis and effective treatment of brain tumors. Magnetic Resonance Imaging (MRI) can generate brain images without tissue damage or skull artifacts, providing important discriminant information for clinicians in the study of brain tumors and other brain diseases. In this paper, we survey the field of brain tumor MRI images segmentation. Firstly, we present the commonly used databases. Then, we summarize multi-modal brain tumor MRI image segmentation methods, which are divided into three categories: conventional segmentation methods, segmentation methods based on classical machine learning methods, and segmentation methods based on deep learning methods. The principles, structures, advantages and disadvantages of typical algorithms in each method are summarized. Finally, we analyze the challenges, and suggest a prospect for future development trends.
1. Introduction
Brain tumors can grow in cerebral vessels, nerves, brain appendages and other intracranial tissues, which seriously threaten the life and health of patients. MRI plays an important role in the diagnosis and treatment of brain tumors. It is the most widely used imaging method in brain tumor detection and clinical treatment. MRI has no radiation, no injury, and no bone artifact in the human body [1]. As a multi-parameter imaging method, MRI has high resolution in soft tissue [2]. Through the acquisition of brain image detail information, we can accurately judge the pathological and histomorphological changes to optimize the segmentation results, which is helpful to the extraction of lesions and the treatment of tumors [3]. In MRI, images of different modes can be obtained according to the difference of transverse relaxation time and longitudinal relaxation time, and images of different modes have specificity in the image information. For example, T1-weighted imaging sequence (T1) can better display the anatomical structure of various brain tissues. T1-weighted Contrast-enhanced (T1C) imaging sequence can observe the boundary information of brain tumors more clearly. T2-weighted imaging sequences (T2) enhance the lesion area and are often used to identify lesions and determine tumor type. Fluid Attenuated Inversion Recovery (FLAIR) inhibited intracranial cerebrospinal fluid and was able to better detect high signal information in the lesion area [4]. In the process of diagnosis and treatment of brain tumors, accurate segmentation of brain tumor MR images is particularly important. According to different degrees of human intervention, it can be divided into artificial segmentation, semi-automatic segmentation and automatic segmentation. Traditionally artificial segmentation has high accuracy, but it is time-consuming and laborious, and subject to the subjective judgment of doctors. In addition, this method also requires experts to have both related brain tumor image knowledge and other professional knowledge of anatomy [5]. Therefore, researchers have done tremendous work on how to improve the accuracy and efficiency of brain tumor MR image segmentation by using semi-automatic segmentation and automatic segmentation. In brain images, the amount of information that can be expressed by single-mode MR images is limited, which cannot give accurate auxiliary information to doctors. The combination of different modal images can achieve complementary information between images [6] to obtain the morphological and pathological information of brain tumors. The result of the algorithm segmentation needs to be compared with the result drawn by the doctor manually, so it is at most the same as the result of the doctor’s manual segmentation. This not only saves doctors a lot of time, but also provides them with important reference information, which can assist in the diagnosis and treatment of brain tumors. Generally, the tumor segmentation process is shown in Figure 1.
This paper attempts to summarize the existing methods of brain tumor MR image segmentation. Firstly, this paper briefly introduces the database of brain tumor segmentation commonly used in brain tumor segmentation. Then, we introduce the basic ideas, network architecture, representative solutions, advantages and disadvantages of different methods. In addition, this paper compares the segmentation results of typical methods on BraTs database and clinical data. Finally, this paper analyzes the challenges faced by brain tumor MR image segmentation, and suggests prospects for development and direction.
2. Databases and Evaluation Measures
In the segmentation of brain tumor MR images, most research is based on public databases, and a smaller part on clinical data. After researchers obtain the results of image segmentation, they need to evaluate them. The evaluation of segmentation results can be divided into subjective evaluation and objective evaluation. Subjective evaluation needs to invest a lot of human and material resources, the evaluators rely on experience, and there is no standard answer. The subjective evaluation results of different people are generally different, and those of the same person at different times are also different. Therefore, objective evaluation measures that can be recognized by most people are particularly important in the study of brain tumor MR image segmentation.
2.1. Evaluation Measures Commonly Used
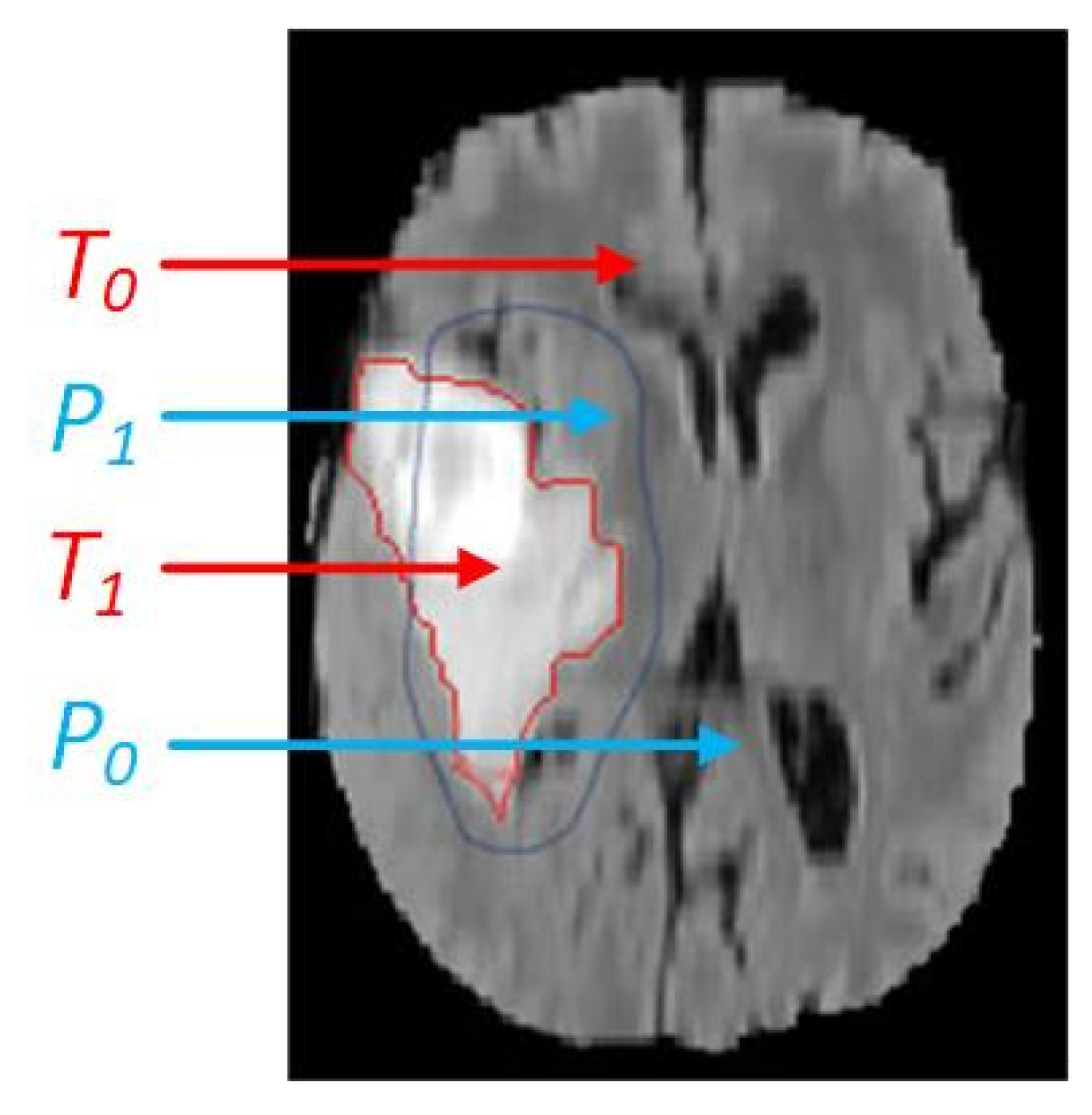
After continuous development and improvement, commonly used segmentation evaluation indicators are as follows: Dice Similarity Coefficient (DSC) [7], Jaccard Similarity (JS) [8], True Positive Rate (TPR) [9], Positive Predictive Value (PPV) [10] and Hausdorff Distance (HD) [11]. In order to obtain the evaluation measures introduced, we need to use the ground truths and actual segmentation results for calculation. The ground truth is an image formed by medical experts directly delineating the boundary of the relevant area of the lesion [12], and it is a standard that is unanimously recognized by researchers. The actual segmentation is the result of algorithm segmentation. Figure 2 shows the comparison between ground truth and the actual segmentation.
In the Figure 2, T1 and T0 represent the tumor area and background area of the ground truth, and P1 and P0 represent the tumor region and background region of the actual segmentation result.
The value of DSC is between [0, 1]. When DSC is equal to 0, the segmentation result is the worst. On the contrary, when DSC is equal to 1, the segmentation result is the most accurate [7], and DSC [13] is computed as follows:
JS value is obtained by the intersection of the actual segmentation result and the ground truth and the ratio of their union, and the definition [14] is as follows:
TPR is obtained from the segmentation result of the algorithm and the ratio of the overlap part of ground truth to ground truth [9]. The definition of true positive rate [15] is as follows:
Positive Predictive Value (PPV) is also called Precision. The Positive Predictive Value is obtained by the ratio of the result correctly segmented by the algorithm to the result segmented by the algorithm. The definition [10] is as follows:
The definition of Hausdorff Distance (HD) is as follows:
can be obtained from set A and set B, is the one-way Hausdorff distance from set A to set B, means the i-th point in set A, means the j-th point in set B, and means the distance between the point and [11].
2.2. Databases Commonly Used
The database commonly used for brain tumor segmentation is the BraTs (Brain Tumor Segmentation) database, and a small number of studies are based on clinical databases. This paper mainly introduces the BraTs2013, BraTs2015, BraTs2017, BraTs2018, BraTs2019, BraTs2020 and some clinical databases. The relevant data information involved in this paper are shown in Table 1.
From Table 1, we can see that BraTs database contains four modes: T1, T1C, T2 and Flair. All image sizes are 240 mm × 240 mm × 155 mm. Before 2018, BraTs database had training data and test data, which could be tested offline. However, since 2018, there is no test data in the database and online testing is required.
2.2.1. BraTs Database
BraTs database is provided by MICCAI (Medical Image Computing and Computer Assisted Intervention) conference. This is the official database for the brain tumor MR image segmentation challenge held by the conference, and is also widely used by researchers engaged in brain tumor MR image segmentation. Since the challenge was held in 2012, the BraTs database has been updated every year. The URL of BraTs database mentioned in this paper is as follows:
- BraTs2013 (Retrieved 21 May 2021 from https://www.smir.ch/BRATS/Start2013),
- BraTs2015 (Retrieved 21 May 2021 from https://www.smir.ch/BRATS/Start2015),
- BraTs2017 (Retrieved 21 May 2021 from https://www.med.upenn.edu/sbia/brats2017/data.html),
- BraTs2018 (Retrieved 21 May 2021 from https://www.med.upenn.edu/sbia/brats2018/data.html),
- BraTs2019 (Retrieved 21 May 2021 from https://www.med.upenn.edu/cbica/brats2019/data.html),
- BraTs2020 (Retrieved 21 May 2021 from https://www.med.upenn.edu/cbica/brats2020/data.html).
In recent years, there have been a large number of studies on BraTs series databases. Table 2 shows some of these research results.
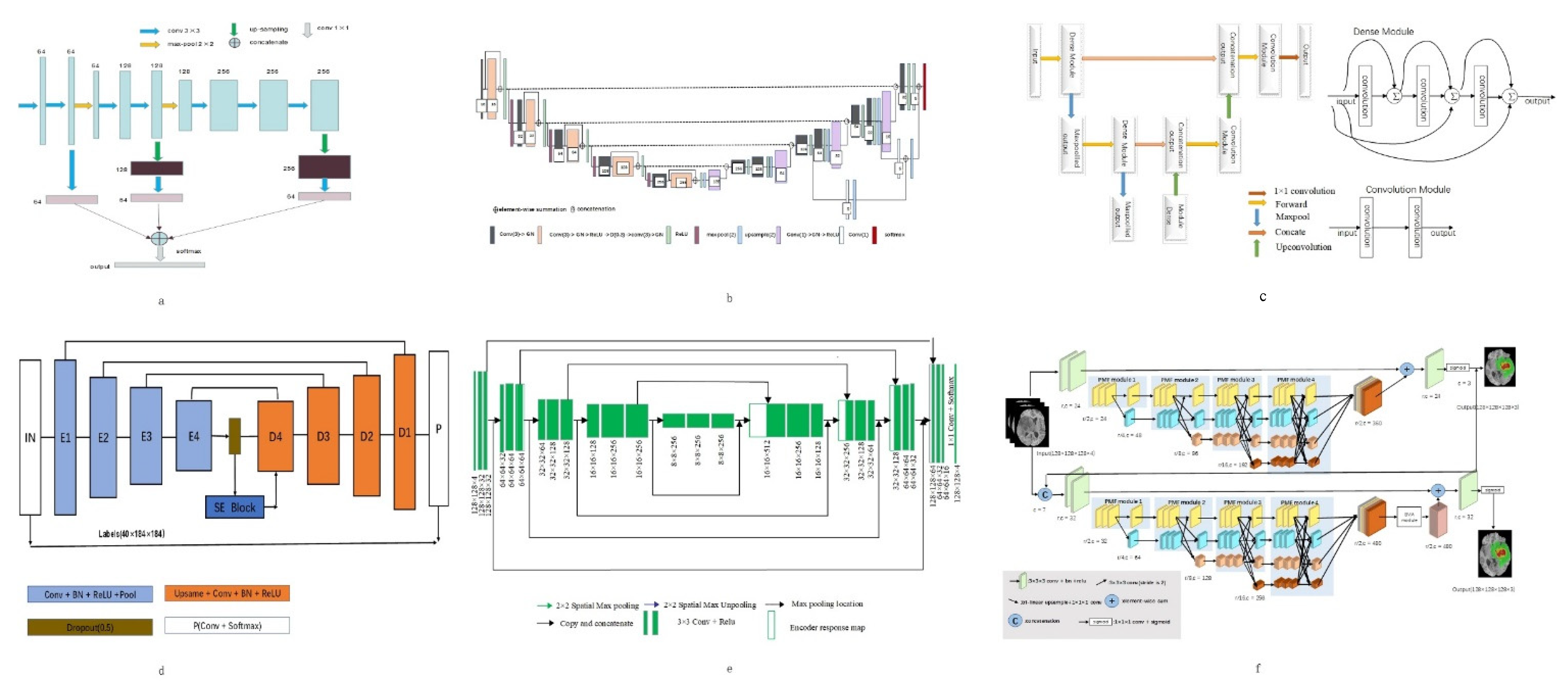
Among the work based on BraTs2013 database, Shen et al. [19] obtained good results in the segmentation of the whole tumor and its sub-regions by using the proposed structure of one subsample and three up-samples to extract stratified features. (The network diagram is shown in Figure 3a). Zhou Z et al. [12] proposed a 3D convolution pyramid module, which is a 3D dense connection architecture that can fuse multi-scale context information. This method performs well in whole tumor segmentation.
In the work based on BraTs2015 database, Iqbal et al. [27] added jump connection and interpolation operation on the basis of Segnet (the network diagram is shown in Figure 3d), which enhanced the segmentation effect of core tumor and enhanced tumor. In the whole tumor segmentation, Casamitjana et al. [23] proposed a method that uses two paths to collect low-resolution and high-resolution features from the input image, and the segmentation effect is better than with other methods.
In the research work based on BraTs2017 database, Po et al. [26] proposed a 3D U-Net model combined with prior knowledge of lesions. Using the original image to generate a group of patients with lesion heat map, then the generated map is employed to locate the target area. (The network diagram is shown in Figure 3b). Experiments show that this method is more effective than other methods in tumor overall segmentation and enhancement segmentation.
In the research work based on BraTs2018 database, Subhashis B et al. [35] proposed a multi-plane convolution neural network for brain tumor MR image segmentation from different anatomical planes (The network diagram is shown in Figure 3e), which showed good performance in the segmentation of whole tumor, core tumor and enhanced tumor.
In the research work based on BraTs2019 database, the method of adding dense connection to encoder part of three-layer codec architecture (The network diagram is shown in Figure 3c) proposed by R Agrava et al. [44], which has the highest precision in the segmentation of whole tumor and core tumor. In the segmentation of enhanced tumor, the deep convolution neural network improved by Zhao Y et al. [43] has the best segmentation effect.
In the research work based on BraTs2020 database, the Hybrid High-resolution and Non-local Feature Network (H2NF-Net) proposed by Jia H et al. [52] uses a single and cascaded HNF-Net to segment different brain tumor regions. Combine the prediction results as the final segmentation result. (The network diagram is shown in Figure 3f). This method works well in whole tumor and core tumor segmentation tasks. In enhanced tumor segmentation, a tumor region segmentation model that combines a two-stage codec with regularization and attention mechanism proposed by Lyu C et al. [53] works well.
2.2.2. Clinical Database
Clinical data of MR brain tumor images are collected by the hospital with the permission of the patients during their treatment. The collected MR brain images are used by doctors to judge the condition of patients and propose reasonable and effective treatment plans. Because of patient privacy and ethical issues, researchers are not allowed to use such data for research without permission from patients and hospitals. In recent years, the comparison of segmentation results based on clinical database is shown in Table 3.
Because the clinical data of each hospital is collected in different stages from different patients, and the equipment conditions used to collect the data are also different, it is impractical to compare the segmentation performance of these works. From the experimental results alone, the improved 3D U-Net scheme proposed by U Baid et al. [44] has higher segmentation accuracy in whole tumor, core tumor and enhanced tumor. The model consists of contraction path and expansion path. The shrinking path mainly captures the context, and the expanding path realizes the target location. The loss function, activation function and data enhancement are also considered. Therefore, each segmentation measure is increased.
3. Methods of Brain Tumor MR Image Segmentation
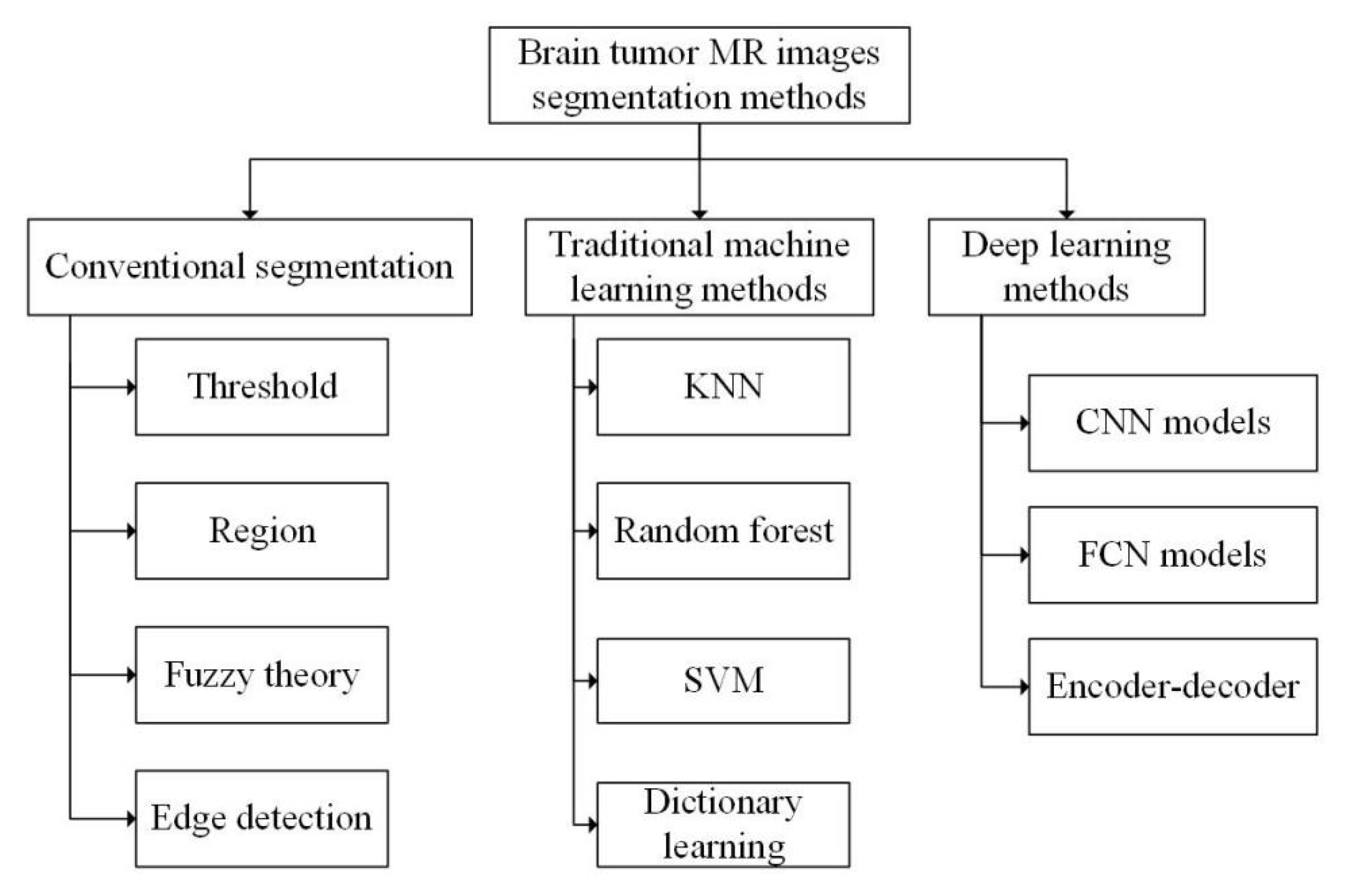
Segmentation methods of brain tumor MR image are mainly divided into three categories according to different segmentation principles: traditional segmentation methods, traditional machine learning-based segmentation methods and deep learning-based segmentation methods. Each category includes a variety of specific segmentation algorithms, as shown in Figure 4.
3.1. Traditional Brain Tumor Segmentation Methods
According to the different theories and emphases, the traditional segmentation methods can be generally divided into four categories: threshold based segmentation, region-based segmentation, fuzzy theory based segmentation and edge detection based segmentation [56].
3.1.1. Segmentation Methods Based on Threshold
Threshold-based segmentation is the simplest method. First, it is assumed that the pixels within a range belong to the same category [57]. Brain tumor images can be divided into target region and background region by setting an appropriate threshold. Different thresholds can also be set to divide the tumor into multiple regions. After continuous research and development, the accuracy of threshold segmentation has been greatly improved. Wang Y P et al. proposed an improved threshold segmentation algorithm. The method improves the noise sensitivity in threshold segmentation by using local information of pixel neighborhood [58]. Foladivanda et al. proposed an adaptive threshold segmentation method. The method can effectively overcome the problem of uneven gray, and enhance the contrast of images, and effectively improve the DSC and JS measure of MR image segmentation of the brain tumor [59].
The segmentation method based on threshold is relatively simple, and the quality of segmentation results almost entirely depends on the size of threshold, so the selection of threshold is very important. Moreover, the threshold segmentation method can only segment simple images, and it is difficult to deal with complex images.
3.1.2. Segmentation Methods Based on Region
Common region-based segmentation methods include watershed algorithm and region-growing algorithm.
Watershed algorithm is a segmentation method based on mathematical morphology. In this algorithm, the image to be processed is compared to the terrain in geography, and the elevation of terrain is represented by the gray value of the pixel. The local minimum and its adjacent area are called the ponding basin. It is assumed that there are water permeable holes at each local minimum. With the increase of infiltration water, the ponding basin will be gradually submerged. Blocking the flow of water from a stagnant basin to a nearby basin is called a dam. When the water level reaches the peak, the infiltration process ends. These dams are called watersheds. Kaleem et al. [60] proposed a watershed segmentation method guided by setting internal or external markers to calculate the morphological gradient of the input image and internal and external markers of the original image. Then they use watershed transform to obtain the segmentation results. Rajini N et al. [61] proposed a method combining threshold segmentation and watershed. First, the image was segmented by threshold method, and then the segmented image was segmented by watershed algorithm. The experiment proved that the segmentation results obtained by this method were more accurate than those obtained by one of the two methods alone, with the average TPR measure higher than 90%.
The segmentation algorithm based on watershed can obtain a complete closed curve and provide contour information for subsequent processing, whereas the watershed algorithm is influenced by noise and easy to over segment.
The region growing algorithm draws all the pixel points conforming to the criterion into the same region via formulating a criterion, so as to achieve pixel segmentation. This kind of segmentation method has the following characteristics: (1) Each pixel must be in a certain region, and the pixels in the region must be connected, and must meet certain similar conditions; (2) different regions are disjoint, and two different regions cannot have the same property. Qusay et al. [62] proposed an automatic seed region growth method, which can automatically set the initial value of seeds, avoid the defects of manual interaction, and improve the efficiency of image segmentation.
The region-based segmentation method has the characteristics of simple calculation and high accuracy, which can extract better regional features and is more suitable for segmentation of small targets. However, it is sensitive to noise and easy to make holes in the extracted region.
3.1.3. Segmentation Methods Based on Fuzzy Theory
The segmentation methods based on fuzzy theory have also been highly valued. In brain tumor MR image segmentation, the most widely used Fuzzy theory algorithm is Fuzzy C-means clustering (FCM) [63]. Muneer K et al. [64] obtained the K-FCM method through the combination of FCM algorithm and K-means algorithm. The experiment proved that, compared with FCM, K-FCM showed higher accuracy in brain tumor MR image segmentation and could reduce the computational complexity. Guo Y et al. [65] proposed a Neutrosophic C-Means (NCM) algorithm based on fuzzy C-means and neutral set framework. The algorithm introduced distance constraint into the objective function to solve the problem of insufficient prior knowledge and achieved satisfactory segmentation results. On the basis of Super-pixel fuzzy clustering and the lattice Boltzmann method, Asieh et al. [66] proposed a level set method that can automatically segment brain tumors, which has strong robustness to image intensity and noise.
The segmentation method based on fuzzy theory can effectively solve the problem of incomplete image information, imprecision, and so on. It has strong compatibility and can be used in combination with other methods, but it is difficult to deal with large-scale data due to its large amount of computation and high time complexity.
3.1.4. Segmentation Methods Based on Edge Detection
The segmentation principle based on edge detection and target contour achieves segmentation by obtaining the edge of the target region and then obtaining the contour of the target region. Common detection operators for edge detection include Roberts operator, Sobel operator, Canny operator and Prewitt operator [67]. Jayanthi et al. [68] integrated FCM into the active contour model. The initial contour of the model is automatically selected by FCM, which reduces the human–computer interaction. Moreover, the problem of the unclear edge contour and uneven intensity in MR images was improved. The average DSC measure of segmentation by this method reached 81%.
Compared with other traditional segmentation methods, the segmentation method based on edge detection pays attention to the edge information of the image and links the edges into contours, and the anti-noise performance is stronger. But the anti-noise performance is negatively correlated with accuracy, that is, the better the anti-noise performance, the lower the accuracy. On the contrary, improved accuracy will reduce the anti-noise performance.
3.2. Segmentation Methods of Brain Tumor MR Images Based on Traditional Machine Learning
Brain tumor segmentation methods based on traditional machine learning use predefined features to train the classification model. Generally, they are divided into two levels: organizational level and pixel level. At the organizational level, the classifier needs to determine which kind of organizational structure each feature belongs to, and at the pixel level the classifier needs to determine which category each pixel belongs to. Traditional Machine Learning algorithms mainly include K-Nearest Neighbors (KNN) [69], Support Vector Machine (SVM) [70], Random Forest (RF) [71], Dictionary Learning (DL) [72], etc.
Havaei et al. [69] regarded each brain as a separate database and used the KNN algorithm for segmentation. They obtained very accurate results, and the segmentation time of each brain image is only one minute, which improves the efficiency of segmentation. Llner F et al. [70] used SVM to segment brain tumors, taking into account the changing characteristics of signal intensity and other features of brain tumor MR images. The TPR measure of this method for LGG reached 83%, and the accuracy measure for HGG reached 91%. Sher et al. [73] first segmented the image by the Otsu method and K-means clustering, then extracted the features by discrete wavelet transformation, and finally reduced the feature dimension by the PCA algorithm to obtain the best features for SVM classification. The experimental results show that the sensitivity and specificity of the scheme can reach more than 90%. Vaishnavee et al. [74] used a proximal support vector machine (PSVM). The method uses equation constraints to solve the primary linear equations, which simplifies the original problem of solving convex quadratic programming. The experiment shows that PSVM is more accurate than SVM in MR image segmentation of brain tumor. Wu et al. [75] proposed a method to first segment the image into super-voxels, then segment the tumor using MRF, estimate the likelihood function at the same time, and extract the features using a multistage wavelet filter. Nabizadeh et al. [76] proposed an automatic segmentation algorithm based on texture and contour. Firstly, the initial points were determined and the machine learning classifier was trained by the initial points. Mahmood et al. [71] proposed an automatic segmentation algorithm based on RF. This algorithm uses several important features such as image intensity, gradient and entropy to generate multiple classifiers, and classifies pixels in multispectral brain MR images by combining the results to obtain segmentation results. Selvathi et al. [77] increased the weight of the wrongly classified samples and decreased the weight of the correctly classified samples in the training process. Then the classifier gives new weights to the samples to ensure that the weights of all decision trees are positively correlated with their classification ability. Finally, the input of the improved RF consists of two parts: the image intensity feature and the original image feature extracted by curve and wavelet transformation. Experimental results show that the accuracy of the improved RF scheme is 3% higher than that of the original RF algorithm. Reza et al. [78] studied the correlation of image minimization features from the perspective of image features, effectively selected features, and finally classified features in multimodal MR images through RF. Compared with the RF algorithm alone, the proposed method can improve the DSC, PPV and TPR measure simultaneously. Meier et al. [79] trained a specific random forest classifier by semi-supervised learning. It takes image segmentation as a classification task and effectively combines the preoperative and postoperative MR image information to improve the postoperative brain tumor segmentation. The PPV and ME measure obtained by this method were 93% and 2.4%, respectively. Dictionary learning is a kind of learning method for simulating dictionary lookup. The dictionary itself is set as dictionary matrix, and the method used is sparse matrix. The process of dictionary lookup is obtained by multiplying the sparse matrix and dictionary matrix, and then the dictionary matrix and sparse matrix are optimized to minimize the error between the value searched and the original data. Chen et al. [72] transformed the super-pixel feature into a high-dimensional feature space. According to the different error values of different regions when the dictionary was modeling brain tumors, the segmentation of brain tumor MR images was realized and the segmentation accuracy was improved. Li [80] proposed a multi dictionary fuzzy learning algorithm based on dictionary learning. This algorithm effectively combines dictionary learning with fuzzy algorithm, and fully considers the differences between the target region and the background, as well as the consistency within the target region. This method can describe the gray and texture information of different regions of the image, and segment the image quickly and accurately.
The traditional machine learning algorithm is better than many traditional segmentation algorithms in algorithmic performance, but there are many shortcomings when it is used in brain tumor MR image segmentation. For example, the KNN algorithm is simple to implement, and the prediction accuracy of the brain tumor region is relatively high, but the calculation is relatively large [69]. The support vector machine has strong theory, and the final result is determined by several support vectors. The calculation is relatively simple and the generalization ability is strong, but it has higher requirements concerning the selection of parameters and kernel function [70]. Random forest can solve the problem of over-segmentation well, process multiple types of data, and has good anti-noise performance. It can parallel operation and shorten the operation time, but it has a poor effect on low-dimensional tumor data processing [71]. The algorithm based on dictionary learning is similar to the idea of dimensionality reduction, both of which reduce the computing complexity and speed up the computing speed, but also have higher requirements for tumor data [72].
3.3. Segmentation Methods of Brain Tumor MR Images Based on Deep Learning
According to different network frameworks, the brain MR image segmentation method is based on deep learning and can be divided into that based on Convolutional Neural network (Convolutional Neural Networks, CNN) of the brain MR image segmentation method, and that based on the Convolutional Neural network (Fully Convolutional Networks, FCN) MR image segmentation method of brain tumors and the brain MR image segmentation method, based on the encoder and decoder.
3.3.1. Segmentation Methods of Brain Tumor MR Images Based on CNN
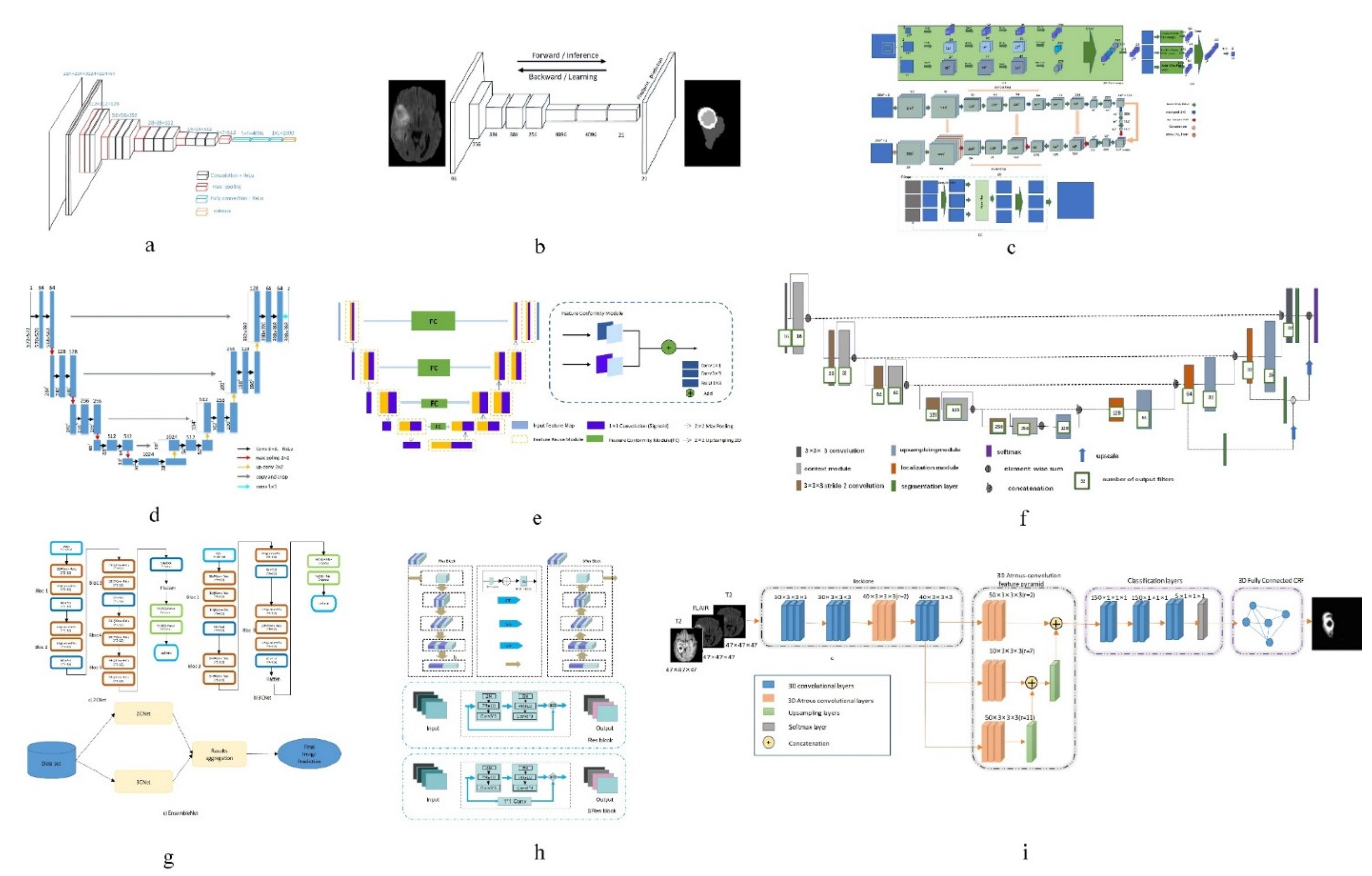
Convolutional neural network belongs to the category of neural network, and its weight sharing mechanism greatly reduces the model complexity. Convolutional neural network (the network diagram is shown in Figure 5a) can directly take the image as the input, automatically extract the features, and has a high degree of invariance to the image translation, scaling and other changes. In recent years, a series of Network models based on convolutional neural Network [81], such as Network in Network [82], VGG [83], Google-Net [84], Res-Net [85], etc., have been widely used in medical image segmentation. Among them, the VGG network has a strong ability to extract features and can guarantee the convergence in the case of fewer training times. However, as the deepening of the network will cause gradient explosion and gradient disappearance, the optimization effect will start to deteriorate when the network depth exceeds a certain range.
In order to solve the problem of network degradation, He et al. [85] proposed deep Residual Network (ResNet), which achieved good results in the segmentation task [86]; Anand et al. [50] combined the 3D convolutional neural network with dense connection, pre-trained the model, and then initialized the model with the weight obtained. This method improved the DSC measure in the segmentation task of brain tumor MR images. Havaei et al. [18] constructed a cascaded dual path CNN, which took the output characteristic graph of CNN in the first stage as the additional input of CNN in the second stage. This method can effectively obtain rich background information and get better segmentation results. Lai et al. [87] reduced the tail of the original image by 98% firstly, corrected the bias field by using n4itk, then pre-segmented it by multi classification CNN, and finally obtained the final segmentation result by median filtering. The algorithm improves the DSC and PPV of segmentation significantly. Salehi et al. [6] proposed a convolutional neural network technology based on automatic context (Auto-Nets) to indirectly learn 3D image information by means of 2D convolution. This method uses 2D convolution in axial, coronal and sagittal MR images respectively to avoid complex 3D convolution operations in segmentation (The network diagram is shown in Figure 5c). Hussain et al. [88] established a correlation architecture composed of a parallel CNN layer and a linear CNN layer by adding an induction structure. This structure has achieved good results in brain tumor MR image segmentation, especially in enhancing the DSC measure to 90%. Kamnitsas et al. [24] trained 3D brain tumor images and then carried out conditional random field post-processing to obtain smoother results. Saouli et al. [89] designed a sequential CNN architecture and proposed that an end-to-end incremental network can simultaneously develop and train CNN models (the network diagram is shown in Figure 5g). The average DSC measure obtained by this method is 88%. Hu K et al. [22] proposed a more hierarchical convolution based Neural Network (Multi-Cascaded Convolutional Neural Network, MCCNN) and fully connected conditional random fields (CRFs), combined with the brain tumor segmentation method, Firstly, the brain tumor is roughly segmented by multi classification convolution neural network, and then fine segmented by fully connected random field according to the rough segmentation results, so as to achieve the effect of batch segmentation and improve the accuracy. The segmentation algorithm based on CNN can automatically extract features and process high-dimensional data, but it is easy to lose information in the process of pooling, and its interpretability is poor.
3.3.2. Segmentation Methods of Brain Tumor MR Images Based on FCN
Compared with pixel-level classification, image-level classification and regression tasks are more suitable for using the CNN structure, because they both expect to obtain a probable value for image classification. For semantic segmentation of images, FCN works better. FCN has no requirement on the size of the input image, and there will be an up sampling process at the last convolution layer. This process can get the same result as the input image size, predicting each pixel while retaining the spatial information in the input image, so as to achieve the pixel classification. In simple terms, FCN is a method to classify and segment images at the pixel level. Therefore, the semantic segmentation model based on FCN is more in line with the requirements of medical image segmentation. Zhao et al. [20] proposed a combination of FCN with CRF for brain tumor segmentation. The method trains two-dimensional slices in axial, coronal and sagittal directions respectively, and then uses fusion strategy to combine segmented brain tumor images. Compared with the traditional segmentation methods, the segmentation speed is faster and the efficiency is higher. Xue et al. [90] proposed a fully convolutional neural network with feature reuse module and feature integration module (f2fcn). It reuses the features of different layers, and uses the feature integration module to eliminate the possible noise and enhance the fusion between different layers (the network diagram is shown in Figure 5e). The DSC and PPV obtained by this method are high. Zhou et al. [91] proposed a 3D atomic convolution feature pyramid to enhance the discrimination ability of the model, which is used to segment tumors of different sizes. Then, an improvement is made on the original basis [12], a 3D dense connection architecture is proposed, and a new feature pyramid module is designed by using 3D convolution (the network diagram is shown in Figure 5i). This module is used to fuse multi-scale context to improve the accuracy of segmentation. Liu et al. [26] proposed a Dilated Convolution optimization structure (DCR) based on Resnet-50, which can effectively extract local and global features, and this method can improve the segmentation PPV measure to 92%. The segmentation algorithm based on FCN can predict the category of each pixel, transform the image classification level to the semantic level, retain the position information in the original image, and obtain a result with the same size as the input image. However, the algorithm has low computational efficiency, takes up a lot of memory space, and the receptive field is relatively small.
3.3.3. Segmentation Methods of Brain Tumor MR Images Based on Encoder-Decoder Structure
The encoder-decoder structure is generally composed of an encoder and a decoder. The encoder trains and learns the input image through a neural network to obtain its characteristic map. The function of the decoder is to mark the category of each pixel after the encoder provides the feature map, so as to achieve the segmentation effect. In the segmentation tasks based on encoder-decoder structure, the structure of encoders is generally similar, mostly derived from the network structure of classification tasks, such as VGG, etc. The purpose of doing this is to obtain the weight parameters of network training through the training of a large database. Therefore, the difference of the decoder reflects the difference of the whole network to a large extent, and is also the key factor affecting the segmentation effect.
Badrinarayanan et al. [92] proposed the SegNet model. Compared with other models, this model has a deeper layer and has better performance in semantic segmentation of pixels. The encoder part of the model consists of a 13 layer vgg-16 network, and can remember the position information of the largest pixel in the encoding phase. In the decoder, the low resolution input features are up sampled to get the segmentation results. The U-Net model based on FCN is a kind of widely used brain tumor segmentation model, in which the network structure is also made up of an encoder and a decoder, and a U-Net network jump connection will code paths, used to get the characteristics of the figure to the decoding path to the corresponding position, in order to get the characteristics of the direct sampling under the coding phase into the decoding stage, thus learning more detailed characteristics. Chen et al. [93] proposed a multi-level deep network, which can obtain image multi-level information by adding auxiliary classifiers on Multi-Level Deep Medical (MLDM) and U-Net, so as to realize image segmentation. The results of DSC, PPV and TPR were 83%, 73% and 85%, respectively. In order to reduce the semantic gap between the feature mapping of encoder and decoder networks, Zhou et al. [94] proposed a variety of nested dense connection methods to connect the encoder and decoder networks. Alom et al. [95] proposed a recursive neural network and a recursive residual convolutional neural network based on U-Net. The experimental results show that the performance of the two kinds of network segmentation combined with U-Net is better than that of U-Net alone. Zhang et al. [38] introduced the attention mechanism and residual network into the traditional U-Net network and proposed an attention residual U-Net (the network diagram is shown in Figure 5h), which improved the segmentation performance of brain tumor MR images. Milletari et al. [96] proposed the V-Net model on the basis of the 3D U-Net model, which extended the original U-Net model by using a 3D convolution check. Hua et al. [37] cascaded V-Net and used the method of segmentation of the whole tumor first into sub-regions of the tumor; the accuracy of segmentation is higher than that of direct V-Net segmentation. Cicek et al. [97] proposed a 3D U-Net model to learn the features of sparse annotated volume images. On the basis of 3D U-Net, Heet et al. [98] added a Hybrid Dilated Convolution (HDC) module to increase the sensory field of neurons, overcoming the restriction that multi-scale feature extraction requires deep neural networks. Using shallow neural networks can reduce the number of model parameters and reduce the computational complexity. Tsenget et al. [25] proposed one with the depth of the layer cross-modal convolution encoder/decoder structure, in combination with MR image data of different modalities, and at the same time using the weighted and multi-stage training methods to solve the problem of unbalanced data; compared with the traditional U-Net structure, the methods of DSC, TPR and PPV measure are improved. Isensee et al. [31] improved the U-Net network model and designed a robust neural network algorithm, which prevented overfitting by expanding the amount of data (the network diagram is shown in Figure 5f). This algorithm improved the TPR measure to 91%; Haichun et al. [28] cleverly applied the improved full convolutional neural network structure to the U-Net model and proposed a novel end-to-end brain tumor segmentation method. In this method, an up-hop connection structure was designed between the encoding path and decoding path to enhance the information flow. Jia et al. [99] constructed a HNF network based on the parallel multi-scale fusion (PMF) module, and proposed a three-dimensional high-resolution and non-local feature network (HNF-NET) for multi parameter MR imaging, which can generate strong high-resolution feature representation and aggregate multi-scale context information. The expectation maximization attention (EMA) module is introduced to extract more relevant features and reduce redundant features. The DSC and HD of the whole tumor are 91.1% and 4.13%, respectively. The segmentation algorithm based on encoder-decoder can combine high-resolution and low-resolution information, and can recognize features from multiple scales, but there is only a short connection between the encoding process and the decoding process, and the connection between the two is obviously insufficient.
3.4. Summary and Analysis
This paper summarizes the existing traditional machine learning based and deep learning based brain tumor MR image segmentation methods and reviews the researchers’ work in the field. It is not difficult to find that deep learning methods and techniques gradually occupy a dominant position in the field of brain tumor MR image segmentation. In the past few years, an end-to-end CNNS method and a U-Net network with codec function for brain tumor MR image segmentation have been most widely used. However, even if similar network architectures are used, the results are not identical [100,101], because data preprocessing can increase the segmentation accuracy without changing the network architecture, and can enhance the generalization ability of the network. Therefore, almost all the research has carried out data preprocessing. By comparing the segmentation performance of various methods, this paper finds that each type of method can solve some of the problems in segmentation. However, there are deficiencies in generalization. For example, brain tumor segmentation based on traditional methods is mostly simple and easy to implement, but it is difficult to process complex images, and the segmentation accuracy is generally low. Segmentation methods based on traditional machine learning are theoretically easy to understand, but it is difficult to process big data. Segmentation methods based on deep learning can extract the deep information from the image, but their interpretability is poor. The advantages and disadvantages of the brain tumor MR image segmentation method described in this paper are shown in Table 4.
In recent years, there has been more and more research into brain tumor MR image segmentation. However, the DSC measure of brain tumor segmentation is only about 0.9, which due to the complexity of the brain tumor MR image and the limitation of the segmentation algorithm. In addition, there are many other challenges in the research field of brain tumor MR image segmentation, such as the generalization ability of segmentation algorithms. Most of the existing segmentation algorithms are for a single lesion, and it is difficult to generalize these to brain tumors with different conditions or even other lesions. The proportion of brain tumor background in the MR image is too large, and the proportion of tumor target region (especially the subregion of brain tumor) is too small, so it is difficult to locate accurately and effectively in the segmentation process. MR images of brain tumors are multimodal data. If the multimodal information is not handled properly, the information between images will be confused, which can lead to no improvement, or even a reduction in segmentation accuracy. Currently, many studies on brain tumor MR image segmentation are only at the theoretical stage, unable to meet the needs of medical staff and difficult to be applied in clinical practice. Deep learning has gradually become the mainstream method in brain tumor MR image segmentation. However, as a supervised learning method, deep learning relies too much on ground truth, but manual labeling is extremely difficult.
4. Future Research Directions
Through studying and summarizing the existing segmentation methods, this paper looks forward to future research directions from four aspects: data acquisition and processing, feature extraction, calculation methods and clinical application.
In recent years, with the continuous development of medical imaging, MR images of brain tumors are playing an increasingly important role in the diagnosis and treatment of brain tumors. Traditional research is mostly based on the calculation and analysis of unit point and small sample data. If the data of different institutions can be integrated and utilized, the accuracy of tumor segmentation will be greatly improved [102]. However, it is still a great challenge to find a general method to deal with all changes of brain MR images from different institutions and MRI scanners. Therefore, how to make full use of multi-site and multi center data [103] will become an area worthy of attention.
Deep learning has an ability to learn features, high efficiency in extracting features, can set the number of network layers, can be mapped to any function in theory, and can solve more complex problems. As long as there are enough brain tumor MR image data, we can obtain ideal results and good portability, which can be used in Tensorflow, Pytorch and other frameworks. Therefore, deep learning based methods will continue to be active in brain tumor MR image segmentation. However, how to improve the feature expression ability of the network is the key problem in improving the performance of the segmentation network.
With the development of artificial intelligence theories and methods, there are many efficient network architectures in the field of computer vision. How to reasonably migrate these architectures to brain tumor MR image segmentation tasks, such as using mask RCNN network [104] in image retrieval and blendmark network [105] in the instance segmentation task, to improve the detection and location ability of brain tumor and its sub regions, is a direction worth exploring.
At present, the mainstream supervised brain tumor MR image segmentation methods have limited databases and are highly dependent on ground truth, while manual labeling is extremely complex. Therefore, how to segment brain tumor MR images accurately through unsupervised learning without labels, and weakly supervised learning with a small number of labels or coarse-grained labels, or to ensure that supervised methods have unsupervised learning ability, will become a hot research direction.
With the proposal of the issue of “combining scientific research with practical problems”, as well as continuous interdisciplinary collision and integration, cooperation between clinicians and computer scientists in the field of medical imaging is becoming more and more important, i.e., scientific research should meet the clinical needs of the hospital. Therefore, in the research into brain tumor MR image segmentation, how to combine clinical information, such as the deep fusion of brain tumor pathology, disease symptoms and MR image at the feature level, etc., will be an important research direction.
Author Contributions
Conceptualization, W.Z. and Y.W.; Data curation, S.H., L.W. and S.D.; Formal analysis, B.Y. and W.Z.; Funding acquisition, B.Y., W.Z. and S.H.; Investigation, Y.W. and S.D; Methodology, W.Z., Y.W. and L.W.; Project administration, B.Y. and W.Z.; Resources, W.Z.; Supervision, B.Y.; Validation, S.H.; Visualization, L.W. and S.D; Writing—original draft, Y.W. and W.Z.; Writing—review and editing, Y.W. and W.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (61572230, 61173078, 61771230), and the Key R & amp; D plan of Shandong (2017CXZC1206, 2019GNC106027, 2019JZZY010134), and the Youth program of Shandong Natural Science Foundation (ZR2020QF011, ZR2020QF014).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The URL of BraTs database mentioned in this paper is as follows: BraTs2013 (Retrieved 21 May 2021 from https://www.smir.ch/BRATS/Start2013), BraTs2015 (Retrieved 21 May 2021 from https://www.smir.ch/BRATS/Start2015), BraTs2017 (Retrieved 21 May 2021 from https://www.med.upenn.edu/sbia/brats2017/data.html), BraTs2018 (Retrieved 21 May 2021 from https://www.med.upenn.edu/sbia/brats2018/data.html), BraTs2019 (Retrieved 21 May 2021 from https://www.med.upenn.edu/cbica/brats2019/data.html), BraTs2020 (Retrieved 21 May 2021 from https://www.med.upenn.edu/cbica/brats2020/data.html).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lin, W. Principles of Magnetic Resonance Imaging: A Signal Processing Perspective. IEEE Eng. Med. Biol. Mag. 2000, 19, 129–130. [Google Scholar]
- Letteboer, M.; Olsen, O.F. Segmentation of Tumors in Magnetic Resonance Brain Images Using an Interactive Multiscale Watershed Algorithm. Acad. Radiol. 2004, 11, 1125–1138. [Google Scholar] [CrossRef] [PubMed]
- Ge, T.; Mu, N.; Li, L. A Brain Tumor Segmentation Method Based on Softmax Regression and Graph Cut. Chin. J. Electron. 2017, 45, 644–649. [Google Scholar]
- Pham, D.L.; Xu, C.Y.; Prince, J.L. Current Methods in Medical Image Segmentation. Annu. Rev. Biomed. Eng. 2000, 2, 315–337. [Google Scholar] [CrossRef]
- Luo, S.H.; Li, X.; Ourselin, S. A New Deformable Model Using Dynamic Gradient Vector Flow and Adaptive Balloon Forces; APRS Workshop on Digital Computing: Brisbane, Australia, 2003; pp. 9–14. [Google Scholar]
- Salehi, S.; Erdogmus, D.; Gholipour, A. Auto-context Convolutional Neural Network(Auto-Net) for Brain Extraction in Magnetic Resonance Imaging. IEEE Trans. Med. Imaging 2017, 36, 2319–2330. [Google Scholar] [CrossRef] [PubMed]
- Dice, L.R. Measures of the Amount of Ecologic Association between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Jaccard, P. The Distribution of Flora in the Alpine Zone. New Phytol. 1912, 11, 37–50. [Google Scholar] [CrossRef]
- Storey, J.D. The Positive False Discovery Rate: A Bayesian Interpretation and the Q-Value. Ann. Stat. 2003, 3, 2013–2035. [Google Scholar] [CrossRef]
- Fletcher Robert, H.; Suzanne, W. Clinical Epidemiology: The Essentials, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; p. 45. [Google Scholar]
- The Editor-in-Chief of Mathematics Dictionary. Mathematics Dictionary; Southeast University Press: Nanjing, China, 2002; Volume III. [Google Scholar]
- Zhou, Z.X.; He, Z.S.; Shi, M.F.; Du, J.L.; Chen, D.D. 3D Dense Connectivity Network with Atrous Convolutional Feature Pyramid for Brain Tumor Segmentation in Magnetic Resonance Imaging of Human Head. Comput. Biol. Med. 2020, 121, 103766. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.; Hanbury, A. Metrics for Evaluating 3D Medical Image Segmentation: Analysis, Selection, and Tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Vovk, U.; Pernus, F.; Likar, B. A Review of Methods for Correctio of Intensity Inhomogeneity in MRI. IEEE Trans. Med. Imaging 2007, 26, 405–421. [Google Scholar] [CrossRef]
- Bland, A.D.G. Statistics Notes: Diagnostic Tests1: Sensitivity and Specificity. BMJ 1994, 308, 1552. [Google Scholar]
- Tustison, N.J.; Shrinidhi, K.L.; Wintermark, M.; Durst, C.R.; Kandel, B.M.; Gee, J.C.; Grossman, M.C.; Avants, B.B. Optimal Symmetric Multimodal Templates and Concatenated Random Forests for Supervised Brain Tumor Segmentation (Simplified) with ANTsR. Neuro Inform. 2015, 13, 209–225. [Google Scholar] [CrossRef]
- Pereira, S.; Pinto, A.; Correia, H.; Oliveira, J.; Rasteiro, D.M.; Silva, C.A. Brain Tumor Segmentation Based on Extremely Randomized Forest with High-level Features. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC, Milan, Italy, 25–29 August 2015; pp. 3037–3040. [Google Scholar]
- Havaei, M.; Davy, A.; Warde, F.D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.-M.; Larochelle, H. Brain Tumor Segmentation with Deep Neural Networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.C.; Zhang, J.G.; Zheng, W.S. Efficient Symmetry-driven Fully Convolutional Network for Multimodal Brain Tumor Segmentation. In Proceedings of the 2017 IEEE International Conference on Image Processing, Beijing, China, 17–20 September 2017; pp. 3864–3868. [Google Scholar]
- Zhao, X.; Wu, Y.; Song, G.; Li, Z.; Zhang, Y.; Fan, Y. A Deep Learning Model Integrating FCNNs and CRFs for Brain Tumor Segmentation. Med. Image Anal. 2017, 43, 98–111. [Google Scholar] [CrossRef]
- Bhagat, P.K.; Choudhary, P. Multi-class Segmentation of Brain Tumor from MRI Images. Appl. Artif. Intell. Tech. Eng. Adv. Intell. Syst. Comput. 2019, 698, 543–553. [Google Scholar]
- Hu, K.; Deng, S.H. Brain Tumor Segmentation Using Multi-Cascaded Convolutional Neural Networks and Conditional Random Field. IEEE Access 2019, 7, 2615–2629. [Google Scholar] [CrossRef]
- Casamitjana, A.; Puch, S.; Aduriz, A.; Vilaplana, V. 3D Convolutional Neural Networks for Brain Tumor Segmentation: A Comparison of Multi-resolution Architectures. In Proceedings of the 2nd International Brain lesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Athens, Greece, 17–21 October 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 150–161. [Google Scholar]
- Kamnitsas, K.; Ledig, C. Efficient Multi-Scale 3D CNN with Fully Connected CRF for Accurate Brain Lesion Segmentation. Med. Image Anal. 2017, 36, 61–78. [Google Scholar] [CrossRef]
- Tseng, K.L.; Lin, Y.L.; Hsu, W.; Huang, C.Y. Joint Sequence Learning and Cross-modality Convolution for 3D Biomedical Segmentation. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 3739–3746. [Google Scholar]
- Liu, D.; Zhang, H.; Zhao, M.; Yu, X.; Yao, S.; Zhou, W. Brain Tumor Segmentation Based on Dilated Convolution Refine Networks. In Proceedings of the 16th IEEE International Conference on Software Engineering Research, Management and Application, Kunming, China, 13–15 June 2018; pp. 113–120. [Google Scholar]
- Iqbal, S.; Ghani, M.U.; Saba, T.; Rehman, A. Brain Tumor Segmentation in Multi-spectral MRI Using Convolutional Neural Networks(CNN). Microsc. Res. Tech. 2018, 81, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Li, H.C.; Li, A.; Wang, M.H. A Novel End-to-end Brain Tumor Segmentation Method Using Improved Fully Convolutional Networks. Comput. Biol. Med. 2019, 108, 150–160. [Google Scholar] [CrossRef]
- Beers, A.; Chang, K.; Brown, J.; Sartor, E.; Gerstner, E.; Mammen, C.P.; Rosen, B.; Kalpathy, C.J. Sequential 3D U-Nets for Bio-logically-informed Brain Tumor Segmentation. arXiv 2017, arXiv:1709.02967. [Google Scholar]
- Shaikh, M.; Anand, G.; Acharya, G.; Amrutkar, A.; Alex, V.; Krishnamurthi, G. Brain Tumor Segmentation Using Dense Fully Convolutional Neural Network. In Proceedings of the 3rd International Brain Lesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Quebec City, QC, Canada, 10–14 September 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 309–319. [Google Scholar]
- Isensee, F.; Wick, W.; Kickingereder, P.; Bendszus, M.; Maier, H.K. Brain Tumor Segmentation and Radio Mics Survival Prediction: Contribution to the BRATS 2017 Challenge. In Proceedings of the 3rd International Brain lesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Quebec City, QC, Canada, 10–14 September 2017; Springer: Berlin/Heidelberg, Germany, 2018; pp. 287–297. [Google Scholar]
- Zhou, T.X.; Ruan, S.; Hu, H.G.; Canu, S. Deep Learning Model Integrating Dilated Convolution and Deep Supervision for Brain Tumor Segmentation in Multi-parametric MRI. Int. Workshop Mach. Learn. Med. Imaging 2019, 11861, 574–582. [Google Scholar]
- Po, Y.K.; Jefferson, W.; Chen, B.S. Improving 3D U-Net for Brain Tumor Segmentation by Utilizing Lesion Prior. Comput. Sci. Comput. Vis. Pattern Recognit. 2020, 1907, 00281. [Google Scholar]
- Wang, G.; Li, W.; Ourselin, S.; Vercauteren, T. Automatic Brain Tumor Segmentation Based on Cascaded Convolutional Neural Networks with Uncertainty Estimation. Cogn. Syst. Res. 2020, 59, 304–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subhashis, B.; Sushmita, M. Novel Volumetric Sub-region Segmentation in Brain Tumors. Front. Comput. Neurosci. 2020, 14, 3. [Google Scholar]
- Zhou, C.; Ding, C.; Wang, X.; Lu, Z.; Tao, D. One-Pass Multi-Task Networks with Cross-Task Guided Attention for Brain Tumor Segmentation. IEEE Trans. Image Process. 2020, 29, 4516–4529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, R.; Huo, Q.; Gao, Y.; Sui, H.; Zhang, B.; Sun, Y.; Mo, S.; Shi, F. Segmenting Brain Tumor Using Cascaded V-Nets in Multimodal MR Images. Front. Comput. Neurosci. 2020, 14, 9. [Google Scholar] [CrossRef]
- Zhang, J.; Lv, X. Ares U-Net: Attention Residual U-Net for Brain Tumor Segmentation. Symmetry 2020, 12, 721. [Google Scholar] [CrossRef]
- Baid, U.; Talbar, S.; Rane, S.; Gupta, S.; Thakur, M.H.; Moiyadi, A.; Sable, N.; Akolkar, M.; Mahajan, A. A Novel Approach for Fully Automatic Intra-Tumor Segmentation with 3D U-Net Architecture for Gliomas. Front. Comput. Neurosci. 2020, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yogananda, C.; Wagner, B.; Nalawade, S.; Murugesan, G.K.; Pinho, M.C.; Fei, B.; Madhuranthakam, A.J.; Maldjian, J.A. Fully Automated Brain Tumor Segmentation and Survival Prediction of Gliomas Using Deep Learning and MRI. Medical Image Computing and Computer Assisted Intervention, MICCAI; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2020; Volume 11993, pp. 99–112. [Google Scholar]
- Li, X.; Luo, G.; Wang, K. Multi-step Cascaded Networks for Brain Tumor Segmentation. Medical Image Computing and Computer Assisted Intervention, MICCAI; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2020; Volume 11992, pp. 163–173. [Google Scholar]
- Wu, P.; Chang, Q. Brain Tumor Segmentation on Multimodal 3D-MRI Using Deep Learning Method. In Proceedings of the 2020 13th International Congress on Image and Signal Processing, Biomedical Engineering and Informatics, CISP-BMEI, Chengdu, China, 17–19 October 2020; pp. 635–639. [Google Scholar]
- Zhao, Y.; Zhang, Y.; Liu, C. Bag of Tricks for 3D MRI Brain Tumor Segmentation. Med. Image Comput. Comput. Assist. Interv. 2020, 11992, 210–220. [Google Scholar]
- Agravat, R.; Raval, M. Brain Tumor Segmentation and Survival Prediction. arXiv 2020, arXiv:1909.09399V1. [Google Scholar]
- Cheng, G.; Cheng, J.; Luo, M.; He, L.; Tian, Y.; Wang, R. Effective and Efficient Multitask Learning for Brain Tumor Segmentation. J. Real-Time Image Process. 2020, 17, 1951–1960. [Google Scholar] [CrossRef]
- Ieva, A.; Russo, C.; Liu, S.; Jian, A.; Bai, M.Y.; Qian, Y.; Magnussen, J.S. Application of Deep Learning for Automatic Segmentation of Brain Tumors on Magnetic Resonance Imaging: A Heuristic Approach in the Clinical Scenario. Neuroradiology 2021, 63, 1253–1262. [Google Scholar] [CrossRef]
- Lucas, F.; Sebastien, O. Generalized Wasserstein Dice Score, Distributionally Robust Deep Learning, and Ranger for Brain Tumor Segmentation: BraTs2020 Challenge. arXiv 2020, arXiv:2011.01614v2. [Google Scholar]
- Henry, T.; Carre, A.; Lerousseau, M.; Estienne, T.; Robert, C.; Paragios, N.; Deutsch, E. Brain Tumor Segmentation with Self-ensembled, Deeply-supervised 3D U-Net Neural Networks: A BraTs2020 Challenge Solution. arXiv 2020, arXiv:2011.01045. [Google Scholar]
- SilvA, C.; Pinto, A.; Pereira, S.; Lopes, A. Multi-stage Deep Layer Aggregation for Brain Tumor Segmentation. arXiv 2021, arXiv:2101.00490. [Google Scholar]
- Anand, V.K.; Grampurohit, S. Brain Tumor Segmentation and Survival Prediction Using Automatic Hard Mining in 3D CNN Architecture. arXiv 2021, arXiv:2101.01546v1. [Google Scholar]
- Qamar, S.; Ahmad, P.; Shen, L. HI-Net: Hyperdense Inception 3D U_Net for Brain Tumor Segmentation. arXiv 2020, arXiv:2012.06760v1. [Google Scholar]
- Jia, H.; Cai, W.; Huang, H.; Xia, Y. H2NF-Net for Brain Tumor Segmentation Using Multimodal MR Imaging: 2nd Place Solution to BraTs Challenge 2020 Segmentation Task. arXiv 2021, arXiv:2012.15318v1. [Google Scholar]
- Lyu, C.; Shu, H. A Two-Stage Cascade Model with Variational Auto Encoders and Attention Gates for MRI Brain Tumor Segmentation. arXiv 2021, arXiv:2011.02881v2. [Google Scholar]
- Shen, Y.; Gao, M. Brain Tumor Segmentation on MRI with Missing Modalities. Information Processing in Medical Imaging; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2019; Volume 11492, pp. 417–428. [Google Scholar]
- Zhao, Z.R.; Zhao, Z. An Enhanced U-Net for Brain Tumor Segmentation. In Proceedings of the 2019 IEEE International Conference on Robotics and Biomimetics, ROBIO, Dali, China, 6–8 December 2019; pp. 3054–3058. [Google Scholar]
- Tiwari, A.; Srivastava, S.; Pant, M. Brain Tumor Segmentation and Classification from Magnetic Resonance Images: Review of selected methods from 2014 to 2019. Pattern Recognit. Lett. 2019, 131, 244–260. [Google Scholar] [CrossRef]
- Sujan, M.; Alam, N.; Abdullah, S.; Islam, M.J. A Segmentation Based Automated System for Brain Tumor Detection. Comput. Appl. 2016, 153, 41–49. [Google Scholar] [CrossRef]
- Wang, Y.P. Medical Image Processing; Tsinghua University Press: Beijing, China, 2012. [Google Scholar]
- Fooladivanda, A.; Shokouhi, S.B.; Ahmadinejad, N.; Mosavi, M.R. Automatic Segmentation of Breast and Fibro glandular Tissue in Breast MRI Using Local Adaptive Thresholding. In Proceedings of the 2014 21th Iranian Conference on Biomedical Engineering, ICBME, Tehran, Iran, 26–28 November 2014; pp. 195–200. [Google Scholar]
- Kaleem, M.; Sanaullah, M.; Hussain, M.A.; Jaffar, M.A.; Choi, T.S. Segmentation of Brain Tumor Tissue Using Marker Controlled Watershed Transform Method. Commun. Comput. Inf. Sci. 2012, 281, 222–227. [Google Scholar]
- Rajini, N.; Narmatha, T.; Bhavani, R. Automatic Classification of MR Brain Tumor Images Using Decision Tree. In Proceedings of the International Conference on Electronics, Communication and Information Systems, Near Madurai, Tamilnadu, India, 2–3 November 2012; pp. 10–13. [Google Scholar]
- Qusay, A.; Isa, N. Computer-aided Segmentation System for Breast MRI Tumor Using Modified Automatic Seeded Region Growing. BMRI-MASRG. J. Digit. Imaging 2014, 27, 133–144. [Google Scholar]
- Lei, T.; Zhang, X.; Jia, X.H. Research Progress of Image Segmentation Based on Fuzzy Clustering. Chin. J. Electron. 2019, 47, 1776–1791. [Google Scholar]
- Muneer, K.; Joseph, K. Performance Analysis of Combined K-mean and Fuzzy-c-Mean Segmentation of MR Brain Images. Computational Vision and Bio Inspired Computing; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2018; pp. 830–860. [Google Scholar]
- Guo, Y.; Sengur, A. NCM: Neutrosophic C-Means Clustering Algorithm. Pattern Recognit. 2015, 48, 2710–2724. [Google Scholar] [CrossRef]
- Khosravanian, A. Fast Level Set Method for Glioma Brain Tumor Segmentation Based on Super Pixel Fuzzy Clustering and Lattice Boltzmann Method. Comput. Methods Programs Biomed. 2020, 198, 105809. [Google Scholar] [CrossRef] [PubMed]
- Canny, A. Computational Approach to Edge Detection. IEEE Trans. Pattern Anal. Mach. Intell. 1986, 8, 679–698. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, S.; Ranganathan, H.; Palanivelan, M. Segmenting Brain Tumor Regions with Fuzzy Integrated Active Contours. IETE J. Res. 2019. [Google Scholar] [CrossRef]
- Havaei, M.; Jodoin, P.M.; Larochelle, A.H. Efficient Interactive Brain Tumor Segmentation as Within-Brain KNN Classification. In Proceedings of the International Conference on Pattern Recognition, Stockholm, Sweden, 24–28 August 2014; pp. 556–561. [Google Scholar]
- Llner, F.; Emblem, K.; Schad, L. Support Vector Machines in DSC-based Glioma Imaging: Suggestions for Optimal Characterization. Magn. Reson. Med. 2010, 64, 1230–1236. [Google Scholar]
- Mahmood, Q.; Basit, A. Automatic Ischemic Stroke Lesion Segmentation in Multi-Spectral MRI Images Using Random Forests Classifier; Springer: New York, NY, USA, 2015; pp. 266–274. [Google Scholar]
- Chen, X.; Binh, P. Automated Brain Tumor Segmentation Using Kernel Dictionary Learning and Super Pixel-level Features. Syst. Man Cybern. 2016, 10, 1109. [Google Scholar]
- Shil, S.; Polly, F. An Improved Brain Tumor Detection and Classification Mechanism. In Proceedings of the 2017 International Conference on Information and Communication Technology Convergence, ICTC, Jeju, Korea, 18–20 October 2017; pp. 54–57. [Google Scholar]
- Vaishnavee, K.; Amshakala, K. An Automated MRI Brain Image Segmentation and Tumor Detection Using SOM-clustering and Proximal Support Vector Machine Classifier. In Proceedings of the 2015 IEEE International Conference on Engineering and Technology, ICETECH, Coimbatore, India, 20–20 March 2015; pp. 1–6. [Google Scholar]
- Wu, W.; Chen, A. Brain Tumor Detection and Segmentation in A CRF (Conditional Random Fields) Framework with Pixel-pairwise Affinity and Super Pixel-level Features. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 241–253. [Google Scholar] [CrossRef]
- Nabizadeh, N.; Kubat, M. Automatic Tumor Segmentation in Single-spectral MRI Using A Texture-based and Contour-based Algorithm. Expert Syst. Appl. 2017, 77, 1–10. [Google Scholar] [CrossRef]
- Selvathi, D.; Selvaraj, H. Segmentation of Brain Tumor Tissues in MR Images Using Multiresolution Transforms and Random Forest Classifier with Ada Boost Technique. In Proceedings of the 2018 26th International Conference on Systems Engineering, ICSEng, Sydney, Australia, 18–20 December 2018; pp. 1–7. [Google Scholar]
- Reza, S. Multi-fractal Texture Features for Brain Tumor and Edema Segmentation. In Medical Imaging 2014: Computer-Aided Diagnosis; International Society for Optics and Photonics: San Diego, CA, USA, 2014; Volume 9035, p. 903503. [Google Scholar]
- Meier, R.; Bauer, S. Patient-specific Semi-supervised Learning for Postoperative Brain Tumor Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2014; pp. 714–721. [Google Scholar]
- Li, Y.F. A Fuzzy Method for Image Segmentation Based on Multi-dictionary Learning. Chin. J. Electron. 2018, 46, 1700–1709. [Google Scholar]
- Chen, S.H.; Liu, W.X.; Qin, J.; Chen, L.; Bin, G.; Zhou, Y.; Huang, B. Research Progress in Computer-aided Diagnosis of Cancer Based on Deep Learning and Medical Images. J. Biomed. Eng. 2017, 2, 160–165. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Int. Conf. Neural Inf. Process. Syst. 2012, 60, 1066. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large Scale Image Recognition. Comput. Sci. 2014, 6, 1556. [Google Scholar]
- Szegedy, C.; Liu, Y. Going Deeper with Convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.W.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Zhou, T.; Huo, B.Q.; Lu, H.L. Research on Residual Neural Network and Its Application in Medical Image Processing. Chin. J. Electron. 2020, 48, 1436–1447. [Google Scholar]
- Lai, X.B.; Xu, M.S.; Xu, X.M. Multimodal MR Image Segmentation of Glioblastoma Based on Multi-class CNN. Chin. J. Electron. 2019, 47, 140–149. [Google Scholar]
- Hussain, S.; Anwar, S.M. Segmentation of Glioma Tumors in Brain Using Deep Convolutional Neural Network. Neuro Comput. 2018, 282, 248–261. [Google Scholar] [CrossRef] [Green Version]
- Saouli, R.; Akil, M.; Kachouri, R. Fully Automatic Brain Tumor Segmentation Using End-to-end Incremental Deep Neural Networks in MRI Images. Comput. Methods Programs Biomed. 2018, 166, 39–49. [Google Scholar]
- Xue, J.; Hu, J.Y. Hypergraph Membrane System Based F2 Fully Convolutional Neural Network for Brain Tumor Segmentation. Appl. Soft Comput. J. 2020, 94, 106454. [Google Scholar] [CrossRef]
- Zhou, Z.X.; He, Z.S.; Jia, Y.Y. AFP-Net: A 3D Fully Convolutional Neural Network with Atrous-convolution Feature Pyramid for Brain Tumor Segmentation via MRI Images. Neuro Comput. 2020, 402, 03097. [Google Scholar]
- Badrinarayan, V.; Kendall, A. SegNet: A Deep Convolutional Encoder-Decoder Architecture for Image Segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Ding, C.X.; Liu, M.F. Dual-force Convolutional Neural Networks for Accurate Brain Tumor Segmentation. Pattern Recognit. 2019, 88, 90–100. [Google Scholar] [CrossRef]
- Zhou, Z.W.; Siddiquee, M.R. U-Net++: A Nested U-Net Architecture for Medical Image Segmentation. International Workshop on Deep Learning in Medical Image Analysis Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Cham, Switzerland; Berlin/Heidelberg, Germany, 2018; pp. 3–11. [Google Scholar]
- Alom, M.Z.; Hasan, M.; Yakopcic, C.; Taha, T.M.; Asari, K. Recurrent Residual Convolutional Neural Network Based on U-Net (R2U-Net) for Medical Image Segmentation. Comput. Vis. Pattern Recognit. 2018, 5, 06955. [Google Scholar]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the International Conference on 3D Vision, Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Çiçek, Ö. 3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Cambridge, UK, 19–22 September 1999; pp. 424–432. [Google Scholar]
- He, C.E.; Xu, H. Research on Automatic Segmentation Algorithm for Multimodal MRI Brain Tumor Images. Acta Opt. Sin. 2020, 40, 0610001. [Google Scholar]
- Jia, H.Z.; Xia, Y. Learning High-Resolution and Efficient Non-Local Features for Brain Glioma Segmentation in MR Images; Medical Image Computing and Computer Assisted Intervention, MICCAI: Lima, Peru, 2020; pp. 480–490. [Google Scholar]
- Mckinley, A.; Wiest, R.; Reyes, M. Pooling-Free Fully Convolutional Networks with Dense Skip Connections for Semantic Segmentation, with Application to Segmentation of White Matter Lesions. Medical Image Computing and Computer Assisted Intervention; MICCAI: Quebec City, QC, Canada, 2017; pp. 169–177. [Google Scholar]
- Mlynarski, P.; Delingette, H. Deep Learning with Mixed Supervision for Brain Tumor Segmentation. J. Med. Imaging 2019, 6, 034002. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Wei, X. Multi-center Brain Imaging Classification sing A Novel 3D CNN Approach. IEEE Access 2018, 6, 925–934. [Google Scholar] [CrossRef]
- Glocker, B. Machine Learning with Multi-Site Imaging Data: An Empirical Study on the Impact of Scanner Effects. arXiv 2019, arXiv:1910.04597. [Google Scholar]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 2961–2969. [Google Scholar]
- Chen, H.; Sun, K.Y. BlendMask: Top-Down Meets Bottom-Up for Instance Segmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, CVPR, Seattle, WA, USA, 14–19 June 2020; pp. 8573–8581. [Google Scholar]
Figure 1.
The flow chart of tumor segmentation.

Figure 2.
The comparison of actual segmentation and ground truth.

Figure 3.
Network structure diagrams of better performing methods. (a) is the structure diagram of a sub sample and three up sampling structures proposed by Shen et al. [19]; (b) is the structure diagram of a 3D U-Net model combined with a priori knowledge of lesions proposed by Po et al. [26]; (c) is the structure diagram of the method of adding dense connections to the encoding part of the three tier codec architecture by R Agrava et al. [44]; (d) is the structure diagram of adding jump connection and interpolation operation on the basis of Segnet proposed by Iqbal et al. [27]; (e) is the structure diagram of a multi plane convolutional neural network proposed by Subhashis B et al. [35]; (f) is the structure diagram of hybrid high-resolution and nonlocal feature network (h2nf net) proposed by Jia h et al. [52].
Figure 3.
Network structure diagrams of better performing methods. (a) is the structure diagram of a sub sample and three up sampling structures proposed by Shen et al. [19]; (b) is the structure diagram of a 3D U-Net model combined with a priori knowledge of lesions proposed by Po et al. [26]; (c) is the structure diagram of the method of adding dense connections to the encoding part of the three tier codec architecture by R Agrava et al. [44]; (d) is the structure diagram of adding jump connection and interpolation operation on the basis of Segnet proposed by Iqbal et al. [27]; (e) is the structure diagram of a multi plane convolutional neural network proposed by Subhashis B et al. [35]; (f) is the structure diagram of hybrid high-resolution and nonlocal feature network (h2nf net) proposed by Jia h et al. [52].

Figure 4.
Brain tumor MR image segmentation methods.

Figure 5.
Network structure diagrams of some classical methods and improved methods. (a) is the classic CNN network model; (b) is the classic FCN network model; (c) is the structure diagram of a convolutional neural network technology based on automatic context (Auto-Nets) proposed by Salehi et al. [6]; (d) is the classic Encoder-Decoder network model; (e) is the structure diagram of a fully convolutional neural network with feature reuse module and feature integration module (f2fcn) proposed by Xue et al. [90]; (f) is the structure diagram of a robust neural network algorithm based on u-net proposed by isensee et al. [31]; (g) is the structure diagram of a sequential CNN architecture proposed by saouli et al. [89]; (h) is the structure diagram of attention residual U-net proposed by Zhang et al. [38]; (i) is a structural diagram of 3D dense connection combined with feature pyramid proposed by Zhou et al. [12].
Figure 5.
Network structure diagrams of some classical methods and improved methods. (a) is the classic CNN network model; (b) is the classic FCN network model; (c) is the structure diagram of a convolutional neural network technology based on automatic context (Auto-Nets) proposed by Salehi et al. [6]; (d) is the classic Encoder-Decoder network model; (e) is the structure diagram of a fully convolutional neural network with feature reuse module and feature integration module (f2fcn) proposed by Xue et al. [90]; (f) is the structure diagram of a robust neural network algorithm based on u-net proposed by isensee et al. [31]; (g) is the structure diagram of a sequential CNN architecture proposed by saouli et al. [89]; (h) is the structure diagram of attention residual U-net proposed by Zhang et al. [38]; (i) is a structural diagram of 3D dense connection combined with feature pyramid proposed by Zhou et al. [12].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Commonly used databases.
| Database | Image Information | Number of Training Data | Number of Test Data | With Ground Truth | Testing Method | Data Size (mm3) | |
|---|---|---|---|---|---|---|---|
| Training Data | Test Data | ||||||
| BraTs2013 | T1, T1C, T2, FLAIR | 20 | 10 | Yes | Yes | Offline | 240 × 240 × 155 |
| BraTs2015 | T1, T1C, T2, FLAIR | 285 | 110 | Yes | Yes | Offline | 240 × 240 × 155 |
| BraTs2017 | T1, T1C, T2, FLAIR | 285 | 66 | Yes | Yes | Offline | 240 × 240 × 155 |
| BraTs2018 | T1, T1C, T2, FLAIR | 285 | - | Yes | No | Online | 240 × 240 × 155 |
| BraTs2019 | T1, T1C, T2, FLAIR | 335 | - | Yes | No | Online | 240 × 240 × 155 |
| BraTs2020 | T1, T1C, T2, FLAIR | 369 | - | Yes | No | Online | 240 × 240 × 155 |
| Clinical database | T1, T1C, T2, FLAIR | - | - | Yes | Yes | Offline | - |
Table 2.
Results of studies using BraTs series database in recent years.
| Database | Method | Evaluation Measure: DSC | ||
|---|---|---|---|---|
| Whole Tumor | Core Tumor | Enhance Tumor | ||
| BRATS 2013 | Tustison et al. [16] | 0.871 | 0.781 | 0.741 |
| Pereira et al. [17] | 0.83 | 0.78 | 0.73 | |
| Havaei et al. [18] | 0.86 | 0.77 | 0.73 | |
| Shen et al. [19] | 0.87 | 0.82 | 0.75 | |
| Zhao et al. [20] | 0.81 | 0.65 | 0.61 | |
| P Bhagat et al. [21] | 0.81 | 0.54 | 0.61 | |
| Hu K et al. [22] | 0.86 | 0.77 | 0.70 | |
| Zhou Z et al. [12] | 0.87 | 0.72 | 0.70 | |
| BRATS 2015 | Casamitjana et al. [23] | 0.917 | 0.836 | 0.768 |
| Kamnitsas et al. [24] | 0.901 | 0.754 | 0.728 | |
| Tseng et al. [25] | 0.852 | 0.683 | 0.688 | |
| Liu et al. [26] | 0.87 | 0.62 | 0.68 | |
| Iqbal et al. [27] | 0.87 | 0.86 | 0.79 | |
| Li H et al. [28] | 0.890 | 0.733 | 0.726 | |
| Hu K et al. [22] | 0.87 | 0.76 | 0.75 | |
| BRATS 2017 | Beers et al. [29] | 0.882 | 0.732 | 0.730 |
| Shaikh et al. [30] | 0.89 | 0.84 | 0.78 | |
| Isensee et al. [31] | 0.858 | 0.775 | 0.647 | |
| Zhou T et al. [32] | 0.885 | 0.846 | 0.734 | |
| Po Y K et al. [33] | 0.903 | 0.744 | 0.780 | |
| Wang G et al. [34] | 0.874 | 0.783 | 0.775 | |
| BRATS 2018 | Wang G et al. [34] | 0.908 | 0.869 | 0.807 |
| Subhashis B et al. [35] | 0.902 | 0.872 | 0.824 | |
| Zhou C et al. [36] | 0.908 | 0.858 | 0.811 | |
| HuA R et al. [37] | 0.876 | 0.795 | 0.736 | |
| Zhang J et al. [38] | 0.876 | 0.810 | 0.773 | |
| U Baid et al. [39] | 0.848 | 0.769 | 0.668 | |
| BRATS 2019 | Yogananda C et al. [40] | 0.901 | 0.844 | 0.801 |
| Li X et al. [41] | 0.886 | 0.813 | 0.771 | |
| Wu P et al. [42] | 0.891 | 0.817 | 0.757 | |
| Zhao Y et al. [43] | 0.883 | 0.861 | 0.810 | |
| R Agravat et al. [44] | 0.92 | 0.90 | 0.79 | |
| Cheng G et al. [45] | 0.905 | 0.820 | 0.764 | |
| Ieva A et al. [46] | 0.878 | 0.732 | 0.699 | |
| BRATS 2020 | Lucas F et al. [47] | 0.889 | 0.841 | 0.814 |
| Henry T et al. [48] | 0.89 | 0.84 | 0.79 | |
| Silva C et al. [49] | 0.886 | 0.830 | 0.790 | |
| Anand V et al. [50] | 0.850 | 0.815 | 0.775 | |
| Qamar S et al. [51] | 0.875 | 0.837 | 0.795 | |
| Jia H et al. [52] | 0.913 | 0.855 | 0.788 | |
| Lyu C et al. [53] | 0.873 | 0.836 | 0.821 | |
Table 3.
Comparison of segmentation results based on clinical databases in recent years.
| Method | Data Sources | Data Volume | Evaluation Measure: DSC | ||
|---|---|---|---|---|---|
| Whole Tumor | Core Tumor | Enhance Tumor | |||
| Hua R et al. [37] | Local hospital | 28 patients | 0.864 | 0.804 | 0.722 |
| U Baid et al. [39] | Local hospital | 40 patients | 0.924 | 0.901 | 0.813 |
| Ieva A et al. [46] | Local hospital | 105 patients | 0.87 | 0.71 | 0.68 |
| Shen Y et al. [54] | Local hospital | 105 patients | 0.894 | 0.790 | 0.653 |
| Zhao Z et al. [55] | Local hospital | 184 patients | 0.785 | - | - |
Table 4.
Advantages and disadvantages of various brain tumor MR image segmentation methods.
| Method | Advantage | Disadvantage | |
|---|---|---|---|
| Traditional segmentation methods | Segmentation method based on threshold [57,58] | Easy to implement, Fast in calculation | Low accuracy, Meaningless for small images |
| Segmentation method based on Region [61,62] | Simple calculation, High accuracy, Can operate in parallel | Sensitive to noise, Easy to produce cavity, Volume effect, Easy to oversplit | |
| Segmentation method based on fuzzy theory [63,66] | Low image requirements, Sensitive to parameters, | Lack of theory, Imperfect system, Long time consuming | |
| Segmentation method based on edge monitoring [67,68] | Strong anti noise ability, Fast detection speed | Contradiction between noise, resistance and accuracy | |
| Segmentation method based on traditional machine learning | Segmentation method based on KNN algorithm [69] | Simple, High precision, Effective noise reduction | Data correlation required, Large amount of calculation |
| Segmentation method based on random forest [71,78] | Strong fitting ability, Strong anti noise ability, Fast in calculation, balance data differences | Many features are required, Easy to lose information | |
| Segmentation method based on support vector machine [73,74] | Easy to fit, Strong theoretical, Easy to calculate | Sensitive to kernel function, Low precision in multitasking | |
| Segmentation method based on dictionary learning [72,80] | Fast operation speed, good performance | High requirements for data, | |
| Segmentation method based on deep learning | Segmentation method based on CNN [18,50] | Shared convolution kernel, Automatic feature extraction | Weak interpretability, Easily lost information, Existence of local convergence |
| Segmentation method based on FCN [26,91] | Image size is not required, Classify each pixel | Efficiency is not real-time, Insensitive to details, Lack of spatial consistency | |
| Segmentation method based on encoder and decoder [92,93] | Multiscale feature recognition, Combined with high and low resolution information, Restore pixel position information | Insufficient contact between encoder and decoder, A large number of parameters, Slow computing speed | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhang, W.; Wu, Y.; Yang, B.; Hu, S.; Wu, L.; Dhelim, S. Overview of Multi-Modal Brain Tumor MR Image Segmentation. Healthcare 2021, 9, 1051. https://doi.org/10.3390/healthcare9081051
AMA Style
Zhang W, Wu Y, Yang B, Hu S, Wu L, Dhelim S. Overview of Multi-Modal Brain Tumor MR Image Segmentation. Healthcare. 2021; 9(8):1051. https://doi.org/10.3390/healthcare9081051
Chicago/Turabian StyleZhang, Wenyin, Yong Wu, Bo Yang, Shunbo Hu, Liang Wu, and Sahraoui Dhelim. 2021. "Overview of Multi-Modal Brain Tumor MR Image Segmentation" Healthcare 9, no. 8: 1051. https://doi.org/10.3390/healthcare9081051
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.