
Association of Platelets and White Blood Cells Subtypes with Trauma Patients’ Mortality Outcome in the Intensive Care Unit

 and
and
Abstract
:1. Introduction
2. Materials and Methods
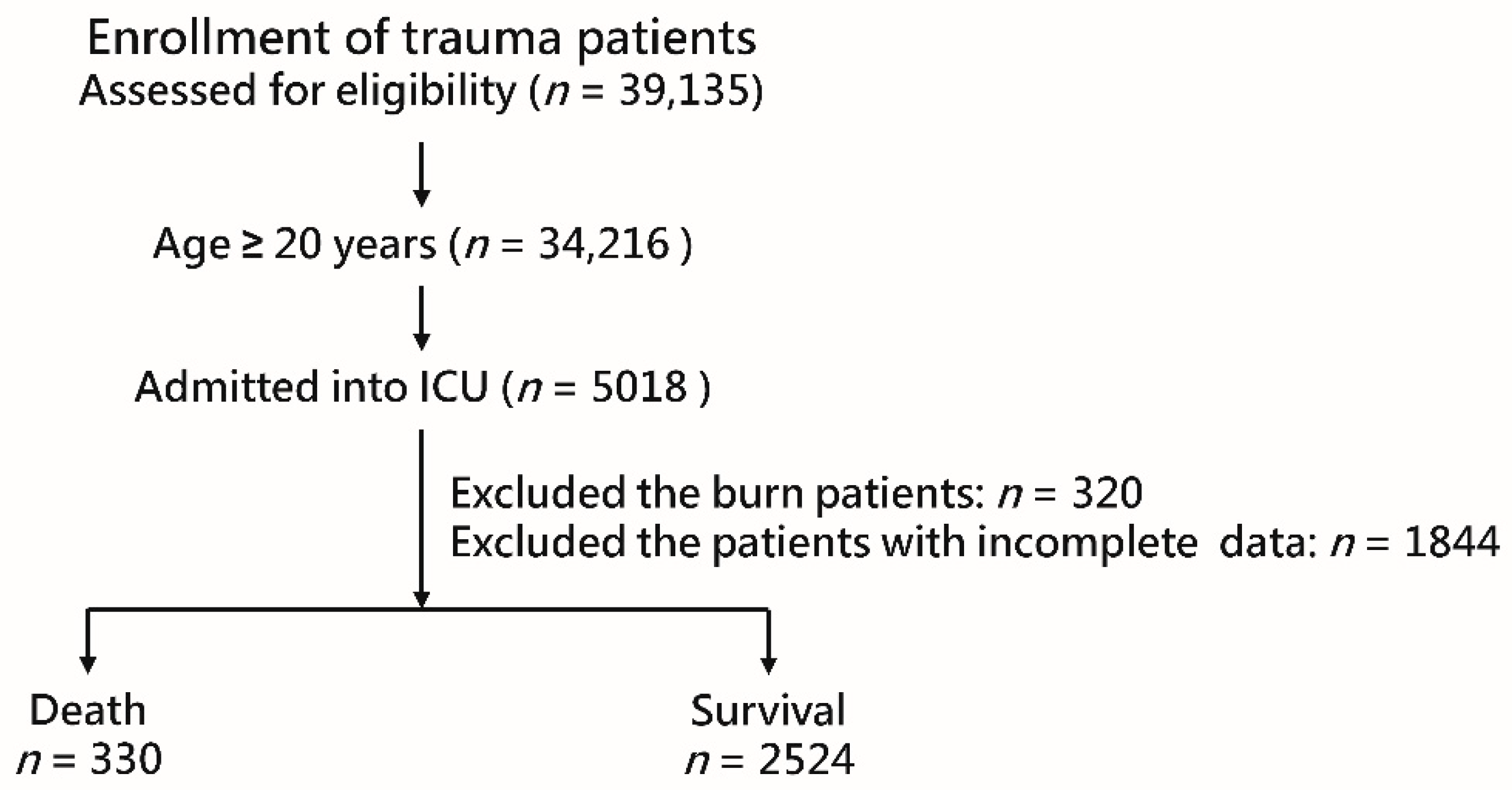
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Risk Factors for Mortality
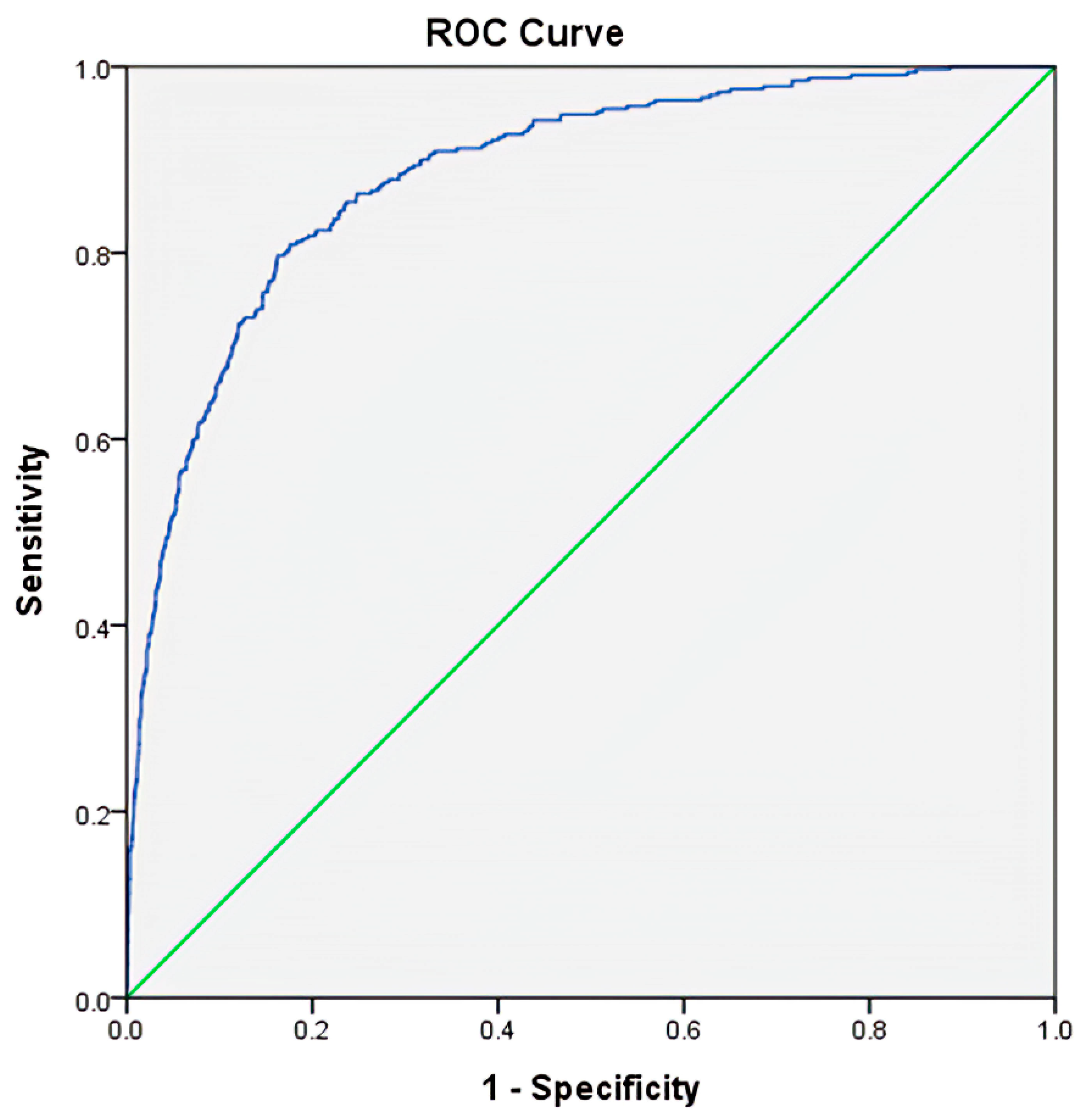
3.3. Prediction for Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| Aptt | activated partial thromboplastin time |
| AST | aspartate aminotransferase |
| BUN | blood urea nitrogen |
| CAD | coronary artery disease |
| CBC | complete blood count |
| CHF | congestive heart failure |
| CI | confidence interval |
| Cr | creatinine |
| CVA | cerebrovascular accident |
| DM | diabetes mellitus |
| ESRD | end-stage renal disease |
| GCS | Glasgow Coma Scale |
| HTN | hypertension |
| ICU | intensive care unit |
| INR | international normalized ratio |
| IQR | interquartile range |
| ISS | Injury Severity Score |
| MLR | monocyte-to-lymphocyte ratio |
| NLR | neutrophil-to-lymphocyte ratio |
| PLR | platelet-to-lymphocyte ratio |
| PT | prothrombin time |
| RBCs | red blood cells |
| WBCs | white blood cells |
References
- Liao, P.H.; Kao, C.C.; How, C.K.; Yang, Y.S.; Chen, M.C.; Hung-Tsang Yen, D.; Lee, Y.T. Initial white blood cell count and revised Baux score predict subsequent bloodstream infection in burn patients: A retrospective analysis of severe burn patients from the Formosa color dust explosion of 2015. J. Formos. Med. Assoc. 2020. [Google Scholar] [CrossRef]
- Bilen, M.A.; Martini, D.J.; Liu, Y.; Lewis, C.; Collins, H.H.; Shabto, J.M.; Akce, M.; Kissick, H.T.; Carthon, B.C.; Shaib, W.L.; et al. The prognostic and predictive impact of inflammatory biomarkers in patients who have advanced-stage cancer treated with immunotherapy. Cancer 2019, 125, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Wang, K.; Lu, H.; Xue, D.; Fan, M.; Zhuang, Q.; Yin, S.; He, X.; Xu, R. Systemic inflammation response index predicts prognosis in patients with clear cell renal cell carcinoma: A propensity score-matched analysis. Cancer Manag. Res. 2019, 11, 909–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dettori, P.; Paliogiannis, P.; Pascale, R.M.; Zinellu, A.; Mangoni, A.A.; Pintus, G. Blood cell count indexes of systemic inflammation in carotid artery disease: Current evidence and future perspectives. Curr. Pharm. Des. 2020. [Google Scholar] [CrossRef]
- Mazza, M.G.; Lucchi, S.; Rossetti, A.; Clerici, M. Neutrophil-lymphocyte ratio, monocyte-lymphocyte ratio and platelet-lymphocyte ratio in non-affective psychosis: A meta-analysis and systematic review. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2020, 21, 326–338. [Google Scholar] [CrossRef]
- Shao, Y.; Li, W.; Wang, D.; Wu, B. Prognostic value of preoperative lymphocyte-related systemic inflammatory biomarkers in upper tract urothelial carcinoma patients treated with radical nephroureterectomy: A systematic review and meta-analysis. World J. Surg. Oncol. 2020, 18, 273. [Google Scholar] [CrossRef]
- Gao, K.; Zhu, W.; Liu, W.; Ma, D.; Li, H.; Yu, W.; Li, Q.; Cao, Y. The predictive role of monocyte-to-lymphocyte ratio in osteoporosis patient. Medicine 2019, 98, e16793. [Google Scholar] [CrossRef]
- Jonska-Gmyrek, J.; Gmyrek, L.; Zolciak-Siwinska, A.; Kowalska, M.; Fuksiewicz, M.; Kotowicz, B. Pretreatment neutrophil to lymphocyte and platelet to lymphocyte ratios as predictive factors for the survival of cervical adenocarcinoma patients. Cancer Manag. Res. 2018, 10, 6029–6038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Duan, W.C.; Zhao, H.B.; Wang, L.; Wang, W.W.; Zhan, Y.B.; Sun, T.; Zhang, F.J.; Yu, B.; Bai, Y.H.; et al. Preoperative Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio are Associated with the Prognosis of Group 3 and Group 4 Medulloblastoma. Sci. Rep. 2019, 9, 13239. [Google Scholar] [CrossRef] [Green Version]
- Vijenthira, A.; Chiu, N.; Jacobson, D.; Freedman, Z.; Cheung, M.C.; Goddard, S.; Fowler, R.; Buckstein, R. Predictors of intensive care unit admission in patients with hematologic malignancy. Sci. Rep. 2020, 10, 21145. [Google Scholar] [CrossRef]
- Emektar, E.; Corbacioglu, S.K.; Dagar, S.; Uzunosmanoglu, H.; Safak, T.; Cevik, Y. Prognostic Value of the Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Predicting One-Year Mortality in Patients with Hip Fractures and Aged Over 60 Years. Eurasian J. Emerg. Med. 2017, 16, 165–170. [Google Scholar] [CrossRef]
- Djordjevic, D.; Pejovic, J.; Surbatovic, M.; Jevdjic, J.; Radakovic, S.; Veljovic, M.; Peric, A.; Andjelic, T.; Popovic, N. Prognostic Value and Daily Trend of Interleukin-6, Neutrophil CD64 Expression, C-Reactive Protein and Lipopolysaccharide-Binding Protein in Critically Ill Patients: Reliable Predictors of Outcome or Not? J. Med. Biochem. 2015, 34, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Surbatovic, M.; Veljovic, M.; Jevdjic, J.; Popovic, N.; Djordjevic, D.; Radakovic, S. Immunoinflammatory response in critically ill patients: Severe sepsis and/or trauma. Mediat. Inflamm. 2013, 2013, 362793. [Google Scholar] [CrossRef]
- Savioli, G.; Ceresa, I.F.; Caneva, L.; Gerosa, S.; Ricevuti, G. Trauma-Induced Coagulopathy: Overview of an Emerging Medical Problem from Pathophysiology to Outcomes. Medicines 2021, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, M.E.; Redick, B.J.; McCreery, R.C.; Crane, I.M.; Greenberg, M.D.; Cachola, L.M.; Nelson, M.F.; Cohen, M.J. Characterization of platelet dysfunction after trauma. J. Trauma Acute Care Surg. 2012, 73, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cap, A.; Hunt, B.J. The pathogenesis of traumatic coagulopathy. Anaesthesia 2015, 70 (Suppl. 1), 96–101. [Google Scholar] [CrossRef]
- Johansson, P.I.; Ostrowski, S.R.; Secher, N.H. Management of major blood loss: An update. Acta Anaesthesiol. Scand. 2010, 54, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.I.; Stensballe, J.; Ostrowski, S.R. Current management of massive hemorrhage in trauma. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tekin, Y.K. Are Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios Associated with Mortality in Pediatric Trauma Patients? A Retrospective Study. Rambam Maimonides Med. J. 2019, 10. [Google Scholar] [CrossRef]
- Li, Y.; Chopp, M. Marrow stromal cell transplantation in stroke and traumatic brain injury. Neurosci. Lett. 2009, 456, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Chien, P.C. Defining polytrauma by abbreviated injury scale >/= 3 for a least two body regions is insufficient in terms of short-term outcome: A cross-sectional study at a level I trauma center. Biomed. J. 2018, 41, 321–327. [Google Scholar] [CrossRef] [PubMed]
- van Helmond, N.; Johnson, B.D.; Curry, T.B.; Cap, A.P.; Convertino, V.A.; Joyner, M.J. White blood cell concentrations during lower body negative pressure and blood loss in humans. Exp. Physiol. 2016, 101, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Sørbye, H.; Svanes, K. The role of blood flow in gastric mucosal defence, damage and healing. Dig. Dis 1994, 12, 305–317. [Google Scholar] [CrossRef]
- Dembiński, A.; Warzecha, Z.; Ceranowicz, P.; Brzozowski, T.; Dembiński, M.; Konturek, S.J.; Pawlik, W.W. Role of capsaicin-sensitive nerves and histamine H1, H2, and H3 receptors in the gastroprotective effect of histamine against stress ulcers in rats. Eur. J. Pharmacol. 2005, 508, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Warzecha, Z.; Dembiński, A.; Brzozowski, T.; Ceranowicz, P.; Pajdo, R.; Niemiec, J.; Drozdowicz, D.; Mitis-Musioł, M.; Konturek, S.J. Gastroprotective effect of histamine and acid secretion on ammonia-induced gastric lesions in rats. Scand. J. Gastroenterol. 2000, 35, 916–924. [Google Scholar] [CrossRef]
- Warzecha, Z.; Dembiński, A.; Brzozowski, T.; Ceranowicz, P.; Dembiński, M.; Stachura, J.; Konturek, S.J. Histamine in stress ulcer prophylaxis in rats. J. Physiol. Pharmacol. 2001, 52, 407–421. [Google Scholar]
- Warzecha, Z.; Ceranowicz, P.; Dembinski, M.; Cieszkowski, J.; Ginter, G.; Ptak-Belowska, A.; Dembinski, A. Involvement of cyclooxygenase-1 and cyclooxygenase-2 activity in the therapeutic effect of ghrelin in the course of ethanol-induced gastric ulcers in rats. J. Physiol. Pharmacol. 2014, 65, 95–106. [Google Scholar]
- Ceranowicz, P.; Warzecha, Z.; Dembinski, A.; Sendur, R.; Cieszkowski, J.; Ceranowicz, D.; Pawlik, W.W.; Kuwahara, A.; Kato, I.; Konturek, P.C. Treatment with ghrelin accelerates the healing of acetic acid-induced gastric and duodenal ulcers in rats. J. Physiol. Pharmacol. 2009, 60, 87–98. [Google Scholar]
- Maduzia, D.; Matuszyk, A.; Ceranowicz, D.; Warzecha, Z.; Ceranowicz, P.; Fyderek, K.; Galazka, K.; Dembinski, A. The influence of pretreatment with ghrelin on the development of acetic-acid-induced colitis in rats. J. Physiol. Pharmacol. 2015, 66, 875–885. [Google Scholar]
- Maduzia, D.; Ceranowicz, P.; Cieszkowski, J.; Gałązka, K.; Kuśnierz-Cabala, B.; Warzecha, Z. Pretreatment with Warfarin Attenuates the Development of Ischemia/Reperfusion-Induced Acute Pancreatitis in Rats. Molecules 2020, 25, 2493. [Google Scholar] [CrossRef] [PubMed]
- Gullo, L.; Cavicchi, L.; Tomassetti, P.; Spagnolo, C.; Freyrie, A.; D’Addato, M. Effects of ischemia on the human pancreas. Gastroenterology 1996, 111, 1033–1038. [Google Scholar] [CrossRef]
- Warshaw, A.L.; O’Hara, P.J. Susceptibility of the pancreas to ischemic injury in shock. Ann. Surg. 1978, 188, 197–201. [Google Scholar] [CrossRef]
- Piton, G.; Capellier, G. Biomarkers of gut barrier failure in the ICU. Curr. Opin. Crit. Care 2016, 22, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Harrois, A.; Libert, N.; Duranteau, J. Acute kidney injury in trauma patients. Curr. Opin. Crit. Care 2017, 23, 447–456. [Google Scholar] [CrossRef]
- Messerer, D.A.C.; Halbgebauer, R.; Nilsson, B.; Pavenstädt, H.; Radermacher, P.; Huber-Lang, M. Immunopathophysiology of trauma-related acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 91–111. [Google Scholar] [CrossRef]
- Ronco, C. N-GAL: Diagnosing AKI as soon as possible. Crit. Care 2007, 11, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sporek, M.; Dumnicka, P.; Gala-Bladzinska, A.; Ceranowicz, P.; Warzecha, Z.; Dembinski, A.; Stepien, E.; Walocha, J.; Drozdz, R.; Kuzniewski, M.; et al. Angiopoietin-2 Is an Early Indicator of Acute Pancreatic-Renal Syndrome in Patients with Acute Pancreatitis. Mediat. Inflamm. 2016, 2016, 5780903. [Google Scholar] [CrossRef] [Green Version]
- Araújo, C.B.; de Oliveira Neves, F.M.; de Freitas, D.F.; Arruda, B.F.T.; de Macêdo Filho, L.J.M.; Salles, V.B.; Meneses, G.C.; Martins, A.M.C.; Libório, A.B. Angiopoietin-2 as a predictor of acute kidney injury in critically ill patients and association with ARDS. Respirology 2019, 24, 345–351. [Google Scholar] [CrossRef]
- Doi, K.; Nishida, O.; Shigematsu, T.; Sadahiro, T.; Itami, N.; Iseki, K.; Yuzawa, Y.; Okada, H.; Koya, D.; Kiyomoto, H.; et al. The Japanese clinical practice guideline for acute kidney injury 2016. Clin. Exp. Nephrol. 2018, 22, 985–1045. [Google Scholar] [CrossRef] [Green Version]
- Pidcoke, H.F.; Isbell, C.L.; Herzig, M.C.; Fedyk, C.G.; Schaffer, B.S.; Chung, K.K.; White, C.E.; Wolf, S.E.; Wade, C.E.; Cap, A.P. Acute blood loss during burn and soft tissue excisions: An observational study of blood product resuscitation practices and focused review. J. Trauma Acute Care Surg. 2015, 78, S39–S47. [Google Scholar] [CrossRef] [Green Version]
- Søvik, S.; Isachsen, M.S.; Nordhuus, K.M.; Tveiten, C.K.; Eken, T.; Sunde, K.; Brurberg, K.G.; Beitland, S. Acute kidney injury in trauma patients admitted to the ICU: A systematic review and meta-analysis. Intensive Care Med. 2019, 45, 407–419. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Tian, S.; Zhao, K.; Zhang, R.; Yin, Y.; Zhu, Y.; Hou, Z.; Zhang, Y. Neutrophil to lymphocyte ratio and fracture severity in young and middle-aged patients with tibial plateau fractures. Int. Orthop. 2020, 44, 2769–2777. [Google Scholar] [CrossRef] [PubMed]
- Dilektasli, E.; Inaba, K.; Haltmeier, T.; Wong, M.D.; Clark, D.; Benjamin, E.R.; Lam, L.; Demetriades, D. The prognostic value of neutrophil-to-lymphocyte ratio on mortality in critically ill trauma patients. J. Trauma Acute Care Surg. 2016, 81, 882–888. [Google Scholar] [CrossRef]
- Fisher, A.; Srikusalanukul, W.; Fisher, L.; Smith, P. The neutrophil to lymphocyte ratio on admission and short-term outcomes in orthogeriatric patients. Int. J. Med. Sci. 2016, 13, 588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djordjevic, D.; Rondovic, G.; Surbatovic, M.; Stanojevic, I.; Udovicic, I.; Andjelic, T.; Zeba, S.; Milosavljevic, S.; Stankovic, N.; Abazovic, D.; et al. Neutrophil-to-Lymphocyte Ratio, Monocyte-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Mean Platelet Volume-to-Platelet Count Ratio as Biomarkers in Critically Ill and Injured Patients: Which Ratio to Choose to Predict Outcome and Nature of Bacteremia? Mediat. Inflamm. 2018, 2018, 3758068. [Google Scholar] [CrossRef] [Green Version]
- Peralta, R.; Vijay, A.; El-Menyar, A.; Consunji, R.; Afifi, I.; Mahmood, I.; Asim, M.; Latifi, R.; Al-Thani, H. Early high ratio platelet transfusion in trauma resuscitation and its outcomes. Int. J. Crit. Ill. Inj. Sci. 2016, 6, 188–193. [Google Scholar] [CrossRef] [Green Version]
- Kor, D.J.; Gajic, O. Blood product transfusion in the critical care setting. Curr. Opin. Crit. Care 2010, 16, 309–316. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Cameron, P.A.; Wolfe, R. TRISS: Does it get better than this? Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2004, 11, 181–186. [Google Scholar] [CrossRef]
- Glance, L.G.; Osler, T. Beyond the major trauma outcome study: Benchmarking performance using a national contemporary, population-based trauma registry. J. Trauma 2001, 51, 725–727. [Google Scholar] [CrossRef] [PubMed]
- de Munter, L.; Polinder, S.; Lansink, K.W.; Cnossen, M.C.; Steyerberg, E.W.; de Jongh, M.A. Mortality prediction models in the general trauma population: A systematic review. Injury 2017, 48, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Rau, C.S.; Wu, S.C.; Chuang, J.F.; Huang, C.Y.; Liu, H.T.; Chien, P.C.; Hsieh, C.H. Machine Learning Models of Survival Prediction in Trauma Patients. J. Clin. Med. 2019, 8, 799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.C.; Chou, S.E.; Liu, H.T.; Hsieh, T.M.; Su, W.T.; Chien, P.C.; Hsieh, C.H. Performance of Prognostic Scoring Systems in Trauma Patients in the Intensive Care Unit of a Trauma Center. Int. J. Environ. Res. Public Health 2020, 17, 7226. [Google Scholar] [CrossRef] [PubMed]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The TRISS method. Trauma Score and the Injury Severity Score. J. Trauma 1987, 27, 370–378. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Death n = 330 | Survival n = 2524 | OR (95% CI) | p | |||
|---|---|---|---|---|---|---|---|
| Sex | 0.031 | ||||||
| Male, n (%) | 229 | (69.4) | 1599 | (63.4) | 1.31 | (1.02–1.68) | |
| Female, n (%) | 101 | (30.6) | 925 | (36.6) | 0.76 | (0.60–0.98) | |
| Age (years) | 63.3 | ±18.4 | 56.6 | ±19.2 | — | <0.001 | |
| Comorbidities | |||||||
| CVA, n (%) | 20 | (6.1) | 134 | (5.3) | 1.15 | (0.71–1.87) | 0.570 |
| HTN, n (%) | 147 | (44.5) | 873 | (34.6) | 1.52 | (1.21–1.92) | <0.001 |
| CAD, n (%) | 44 | (13.3) | 166 | (6.6) | 2.19 | (1.53–3.11) | <0.001 |
| CHF, n (%) | 3 | (0.9) | 13 | (0.5) | 1.77 | (0.50–6.25) | 0.367 |
| DM, n (%) | 72 | (21.8) | 479 | (19.0) | 1.19 | (0.90–1.58) | 0.219 |
| ESRD, n (%) | 32 | (9.7) | 55 | (2.2) | 4.82 | (3.07–7.58) | <0.001 |
| GCS, median (IQR) | 5 | (3–12) | 15 | (11–15) | — | <0.001 | |
| 3–8, n (%) | 222 | (67.3) | 468 | (18.5) | 9.03 | (7.03–11.61) | <0.001 |
| 9–12, n (%) | 26 | (7.9) | 319 | (12.6) | 0.59 | (0.39–0.90) | 0.013 |
| 13–15, n (%) | 82 | (24.8) | 1737 | (68.8) | 0.15 | (0.12–0.20) | <0.001 |
| ISS, median (IQR) | 25 | (25–29) | 17 | (16–24) | — | <0.001 | |
| 1–15, n (%) | 22 | (6.7) | 509 | (20.2) | 0.28 | (0.18–0.44) | <0.001 |
| 16–24, n (%) | 58 | (17.6) | 1426 | (56.5) | 0.16 | (0.12–0.22) | <0.001 |
| ≥25, n (%) | 250 | (75.8) | 589 | (23.3) | 10.27 | (7.85–13.42) | <0.001 |
| RBCs (millions/μL) | 3.9 | ±0.9 | 4.3 | ±0.8 | <0.001 | ||
| Monocytes (count/μL) | 631 | ±450 | 626 | ±415 | — | 0.834 | |
| Neutrophils (count/μL) | 9725 | ±5550 | 10,198 | ±53,932 | — | 0.136 | |
| Platelets (count/μL) | 175,842 | ±61,713 | 206,890 | ±69,006 | — | <0.001 | |
| Lymphocytes (count/μL) | 2458 | ±1940 | 1971 | ±1453 | — | <0.001 | |
| MLR | 0.4 | ±0.5 | 0.5 | ±0.5 | — | 0.605 | |
| NLR | 7.6 | ±8.5 | 8.2 | ±7.8 | — | 0.211 | |
| PLR | 124.3 | ±110.3 | 150.6 | ±106.5 | — | <0.001 | |
| PT (s) | 13.3 | ±6.3 | 11.2 | ±3.1 | — | <0.001 | |
| aPTT (s) | 33.0 | ±13.5 | 26.9 | ±4.8 | — | <0.001 | |
| INR | 1.3 | ±0.6 | 1.1 | ±0.2 | — | <0.001 | |
| AST (U/L) | 87.8 | ±152.2 | 79.8 | ±170.6 | — | 0.418 | |
| ALT (U/L) | 50.3 | ±91.9 | 53.0 | ±93.8 | — | 0.626 | |
| BUN (mg/dL) | 22.0 | ±18.0 | 16.4 | ±11.2 | — | <0.001 | |
| Cr (mg/dL) | 1.9 | ±2.3 | 1.1 | ±1.5 | — | <0.001 | |
| Hospital stay (days) | 11.1 | ±15.2 | 7.7 | ±9.8 | <0.001 | ||
| Variables | Univariate Analysis | Multivariate Analysis | p | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95% CI) | ||||
| Male | 1.31 | (1.02–1.68) | 0.032 | 1.45 | (1.05–2.01) | 0.024 |
| Age | 1.02 | (1.01–1.03) | <0.001 | 1.03 | (1.02–1.04) | <0.001 |
| HTN | 1.52 | (1.21–1.92) | <0.001 | 1.11 | (0.80–1.54) | 0.538 |
| CAD | 2.19 | (1.53–3.11) | <0.001 | 1.73 | (1.09–2.75) | 0.020 |
| ESRD | 4.82 | (3.07–7.58) | <0.001 | 3.12 | (1.32–7.37) | 0.010 |
| GCS | 0.77 | (0.75–0.79) | <0.001 | 0.79 | (0.76–0.82) | <0.001 |
| ISS | 1.11 | (1.09–1.13) | <0.001 | 1.06 | (1.04–1.08) | <0.001 |
| RBC | 0.53 | (0.46–0.61) | <0.001 | 0.80 | (0.66–0.98) | 0.032 |
| Lymphocytes | 1.19 | (1.12–1.27) | <0.001 | 1.31 | (1.16–1.48) | <0.001 |
| Platelets | 0.48 | (0.40–0.58) | <0.001 | 0.54 | (0.41–0.67) | <0.001 |
| PLR | 0.97 | (0.96–0.98) | <0.001 | 0.98 | (0.98–0.99) | 0.024 |
| PT | 1.11 | (1.08–1.15) | <0.001 | 1.03 | (0.98–1.07) | 0.235 |
| aPTT | 1.11 | (1.08–1.13) | <0.001 | 1.06 | (1.03–1.09) | <0.001 |
| INR | 3.92 | (2.64–5.81) | <0.001 | 1.09 | (0.61–1.95) | 0.779 |
| BUN | 1.03 | (1.02–1.03) | <0.001 | 1.02 | (1.00–1.03) | 0.054 |
| Cr | 1.20 | (1.13–1.27) | <0.001 | 1.02 | (0.91–1.14) | 0.705 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ke, R.-T.; Rau, C.-S.; Hsieh, T.-M.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H.; Liu, H.-T. Association of Platelets and White Blood Cells Subtypes with Trauma Patients’ Mortality Outcome in the Intensive Care Unit. Healthcare 2021, 9, 942. https://doi.org/10.3390/healthcare9080942
Ke R-T, Rau C-S, Hsieh T-M, Chou S-E, Su W-T, Hsu S-Y, Hsieh C-H, Liu H-T. Association of Platelets and White Blood Cells Subtypes with Trauma Patients’ Mortality Outcome in the Intensive Care Unit. Healthcare. 2021; 9(8):942. https://doi.org/10.3390/healthcare9080942
Chicago/Turabian StyleKe, Ruei-Ti, Cheng-Shyuan Rau, Ting-Min Hsieh, Sheng-En Chou, Wei-Ti Su, Shiun-Yuan Hsu, Ching-Hua Hsieh, and Hang-Tsung Liu. 2021. "Association of Platelets and White Blood Cells Subtypes with Trauma Patients’ Mortality Outcome in the Intensive Care Unit" Healthcare 9, no. 8: 942. https://doi.org/10.3390/healthcare9080942