Anticipated Social and Healthcare Economic Burden of People with Alzheimer’s Disease in Two Selected Regions of the Czech Republic

 , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Theoretical Background
3. Methodology
3.1. Study Design
- A population model for predicting the number of people with AD between 2020 and 2070;
- A cost model for calculating the economic burden between 2020 and 2070 based on the predicted number of people with AD from the population model.
3.2. Population Model and Data Sources
3.3. Cost Model and Data Sources
- Outpatient care—outpatient procedures administered by primary care medical doctors and specialists;
- Costs of medicines in outpatient clinics and hospitals (residential facility);
- Costs of hospital services;
- Hospitalisation—emergency care as well as other care.
- People in the mild stage are mostly at home and are cared for by informal caregivers;
- Moderate-stage patients are also predominantly at home and use outpatient and domiciliary social services more often but there is a capacity problem, meaning many of them are unable to use these services;
- Patients suffering from the severe stage could be in residential social care facilities, but there is a capacity problem, meaning many of them cannot use these social services.
4. Results
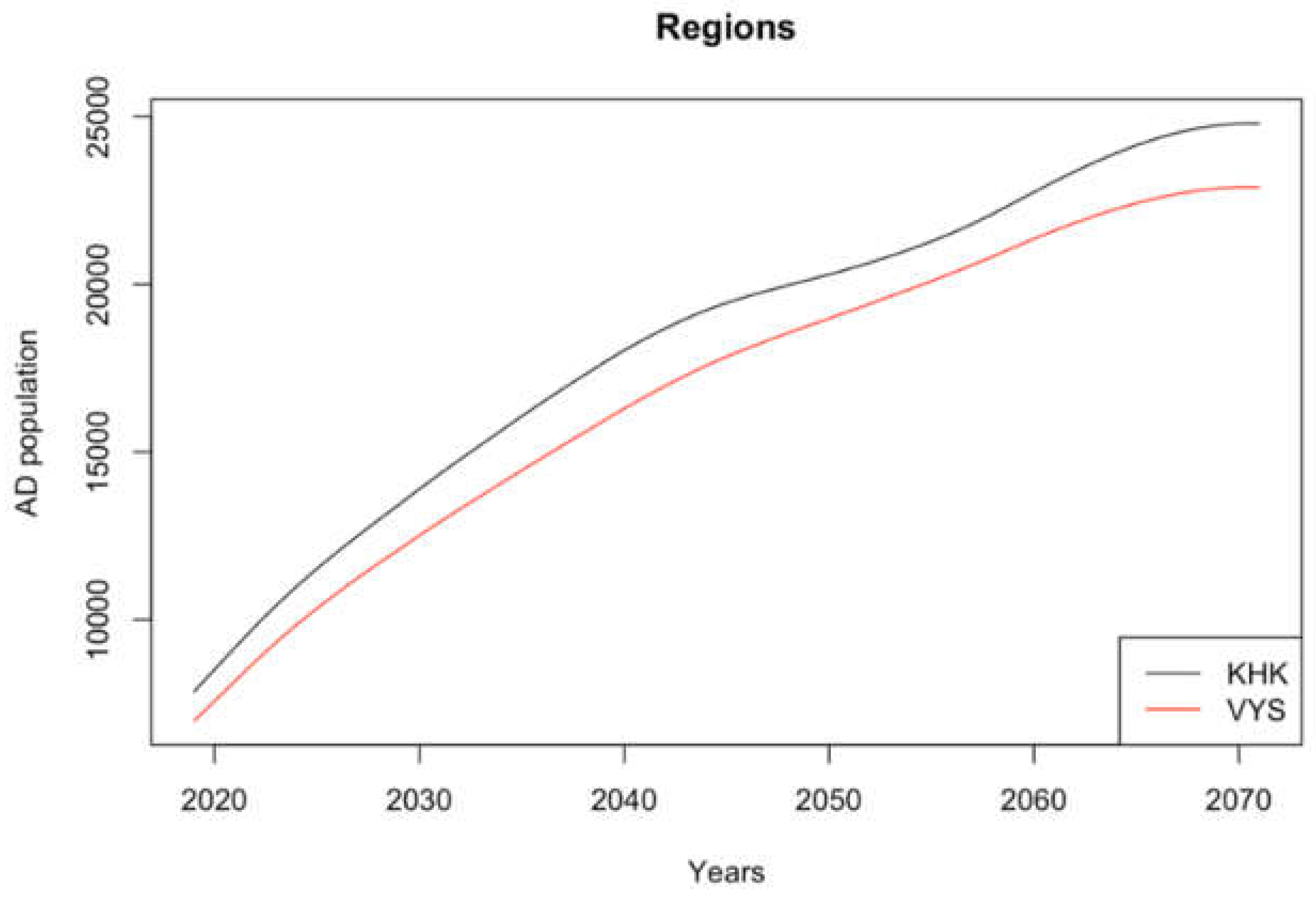
4.1. Population of People with AD
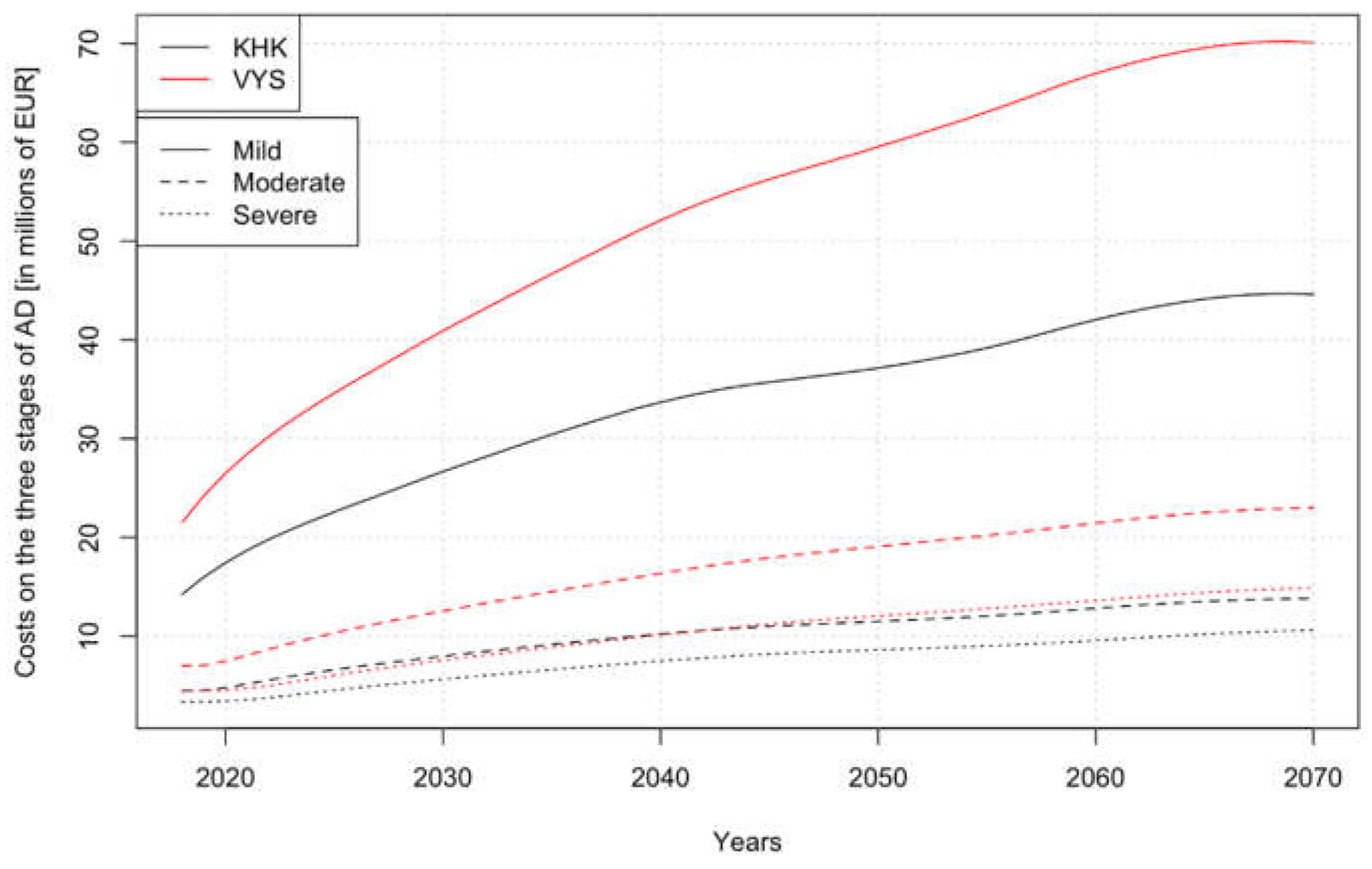
4.2. Direct Costs
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sidlo, L.; Sprocha, B.; Klapkova, M. Regional differences in population aging in Europe viewed through prospective indicators. Erdkunde 2019, 225–240. [Google Scholar] [CrossRef]
- Age Structure of the Population—2019. Available online: https://www.czso.cz/csu/czso/vekove-slozeni-obyvatelstva-2019 (accessed on 29 August 2020).
- Czech Statistical Office. Age Distribution on 31st December 2101, Czech Republic. Available online: https://www.czso.cz/staticke/animgraf/projekce_1950_2101/index.html?lang=en (accessed on 29 August 2020).
- Burlando, C.; Cusano, I. Growing Old and Keep Mobile in Italy. Active Ageing and the Importance of Urban Mobility Planning Strategies. Tema. J. Land Use Mobil. Environ. 2018, 43–52. [Google Scholar] [CrossRef]
- Health 2020: A European Policy Framework and Strategy for the 21st Century. Available online: https://www.euro.who.int/__data/assets/pdf_file/0011/199532/Health2020-Long.pdf?ua=1 (accessed on 5 October 2020).
- G8 Dementia Summit: Global Action against Dementia—11 December 2013. Available online: https://www.gov.uk/government/publications/g8-dementia-summit-global-action-against-dementia/g8-dementia-summit-global-action-against-dementia-11-december-2013 (accessed on 5 October 2020).
- Greve, B. Long-term care: What is about? In Long-Term Care for the Elderly in Europe: Development and Prospects; Routledge: New York, NY, USA, 2017; pp. 1–7. [Google Scholar]
- Langhamrova, J.; Simkova, M.; Sixta, J. Macroeconomic Impacts of the Expansion of Social Services for Ageing Population of the Czech Republic. Polit. Ekon. 2018, 2018, 240–259. [Google Scholar] [CrossRef] [Green Version]
- Soucasna Struktura Sluzeb Dlouhodobe Pece a Prognoza Potrebnosti Socialnich Sluzeb 2019–2050 [The Current Structure of Long-Term Care Services and the Forecast of the Need for Social Services 2019–2050]. Available online: http://www.apsscr.cz/cz/nabizime/Soucasna-struktura-sluzeb-dlouhodobe-pece-a-prognoza-potrebnosti-socialnich-sluzeb-2019%E2%80%932050 (accessed on 9 September 2020).
- Position of Caregivers in the Czech Republic. Analysis of the Concept and Implementation of Social Policy in the Czech Republic with Focus on Care for Seniors. Available online: http://praha.vupsv.cz/fulltext/ul_1963.pdf (accessed on 5 October 2020).
- Zprava o Stavu Demence 2016. Kolik Zaplatite za Peci? [Dementia Report 2016. How much do you Pay for Care?]. Available online: http://www.alzheimer.cz/res/archive/004/000480.pdf?seek=1492589048 (accessed on 29 August 2020).
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Bertens, D.; Vos, S.; Kehoe, P.; Wolf, H.; Nobili, F.; Mendonça, A.; van Rossum, I.; Hort, J.; Molinuevo, J.L.; Heneka, M.; et al. Use of mild cognitive impairment and prodromal AD/MCI due to AD in clinical care: A European survey. Alzheimers Res. Ther. 2019, 11, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinklarova, L.; Schmidt, M.; Benek, O.; Kuca, K.; Gunn-Moore, F.; Musilek, K. Friend or enemy? Review of 17β-HSD10 and its role in human health or disease. J. Neurochem. 2020, 155, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Ellison, J.M. What’s New in the Alzheimer’s Treatment Pipeline? 2020. Available online: https://www.brightfocus.org/alzheimers/article/whats-new-alzheimers-treatment-pipeline (accessed on 9 September 2020).
- Czech Republic: Number of People Suffering from Dementia has Doubled in 30 Years. Available online: https://kafkadesk.org/2019/11/22/czech-republic-number-of-people-suffering-from-dementia-has-doubled-in-30-years/ (accessed on 5 October 2020).
- Czech Republic: Country Health Profile 2017, State of Health in the EU. Available online: https://ec.europa.eu/health/sites/health/files/state/docs/chp_cs_english.pdf (accessed on 5 October 2020).
- Czech Republic: National Dementia Strategies. Available online: https://www.alzheimer-europe.org/Policy/National-Dementia-Strategies/Czech-Republic (accessed on 5 October 2020).
- Ministerstvo Zdravotnictvi a NUDZ Pripravily Narodni Akcni Plan pro Alzheimerovu Nemoc [The Ministry of Health and NUDZ have Prepared a National Action Plan for Alzheimer’s Disease]. Available online: https://www.mzcr.cz/tiskove-centrum-mz/ministerstvo-zdravotnictvi-a-nudz-pripravily-narodni-akcni-plan-pro-alzheimerovu-nemoc/ (accessed on 5 October 2020).
- Alzheimer’s Association. Coronavirus (COVID-19): Tips for Dementia Caregivers. Available online: https://www.alz.org/help-support/caregiving/coronavirus-(covid-19)-tips-for-dementia-care (accessed on 5 October 2020).
- Alzheimer Europe. Alzheimer Europe Position Regarding the Allocation of Scarce Medical Resources for Intensive Care Services during the COVID-19 Pandemic. 2020. Available online: https://www.alzheimer-europe.org/Policy/Our-opinion-on/Triage-decisions-during-COVID-19-pandemic (accessed on 5 October 2020).
- Czech Statistical Office. Regional Statistics. Available online: https://www.czso.cz/csu/czso/regiony_mesta_obce_souhrn (accessed on 5 October 2020).
- Allegri, R.F.; Butman, J.; Arizaga, R.L.; Machnicki, G.; Serrano, C.; Taragano, F.E.; Sarasola, D.; Lon, L. Economic impact of dementia in developing countries: An evaluation of costs of Alzheimer-type dementia in Argentina. Int. Psychogeriatr. 2007, 19, 705–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brookmeyer, R.; Johnson, E.; Ziegler-Graham, K.; Arrighi, H.M. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007, 3, 186–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavallo, M.C.; Fattore, G. The economic and social burden of Alzheimer disease on families in the Lombardy region of Italy. Alzheimer Dis. Assoc. Disord. 1997, 11, 184–190. [Google Scholar]
- Maresova, P.; Kuca, K. Missing Uniform Costs Classification for Alzheimer’s Disease Treatment and Care. Curr. Alzheimer Res. 2018, 15, 1297–1303. [Google Scholar] [CrossRef]
- Schwarzkopf, L.; Menn, P.; Kunz, S.; Holle, R.; Lauterberg, J.; Marx, P.; Mehlig, H.; Wunder, S.; Leidl, R.; Donath, C.; et al. Costs of care for dementia patients in community setting: An analysis for mild and moderate disease stage. Value Health 2011, 14, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reese, J.P.; Hessmann, P.; Seeberg, G.; Henkel, D.; Hirzmann, P.; Rieke, J.; Baum, E.; Dannhoff, F.; Müller, M.J.; Jessen, F.; et al. Cost and care of patients with Alzheimer’s disease: Clinical predictors in German health care settings. J. Alzheimers Dis. 2011, 27, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Michalowsky, B.; Kaczynski, A.; Hoffmann, W. Ökonomische und gesellschaftliche Herausforderungen der Demenz in Deutschland–Eine Metaanalyse [Economic and social challenges of dementia in Germany—A meta-analysis]. Bundesgesundheitsbl 2019, 62, 981–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodel, R.; Belger, M.; Reed, C.; Wimo, A.; Jones, R.W.; Happich, M.; Argimon, J.M.; Bruno, G.; Vellas, B.; Haro, J.M. Determinants of societal costs in Alzheimer’s disease: GERAS study baseline results. Alzheimers Dement. 2015, 11, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Reed, C.C.; Dodel, R.; Belger, M.; Jones, R.W.; Happich, M.; Argimon, J.M.; Bruno, G.; Novick, D.; Vellas, B.; et al. The GERAS Study: A prospective observational study of costs and resource use in community dwellers with Alzheimer’s disease in three European countries--study design and baseline findings. J. Alzheimers Dis. 2013, 36, 385–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Alzheimer Report 2015, The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf (accessed on 29 August 2020).
- Maresova, P.; Mohelska, H.; Kuca, K. Social and family load of Alzheimer’s disease. Appl. Econ. 2016, 48, 1936–1948. [Google Scholar] [CrossRef]
- Broulikova, H.M.; Sladek, V.; Arltova, M.; Cerny, J. The Potential Impact of Alzheimer’s Disease Early Treatment on Societal Costs of Care in Czechia: A Simulation Approach. J. Ment. Health Policy Econ. 2018, 21, 147–161. [Google Scholar]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. 2013, 9, 63–75.e2. [Google Scholar] [CrossRef]
- Keogh-Brown, M.R.; Jensen, H.T.; Arrighi, H.M.; Smith, R.D. The Impact of Alzheimer’s Disease on the Chinese Economy. EBioMedicine 2016, 4, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, G.-H. Modeling the Cost-Effectiveness of Galantamine for Mild to Moderately Severe Alzheimer’s Disease in Korea. Value Health 2009, 12, S49–S54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimler, R.; Tomaskova, H.; Kuhnova, J.; Dolezal, O.; Pscheidl, P.; Kuca, K. Numeric, Agent-based or System Dynamics Model? Which Modeling Approach is the Best for Vast Population Simulation? Curr. Alzheimer Res. 2018, 15, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Population Projection in the Regions of the Czech Republic—Until 2070. Available online: https://www.czso.cz/csu/czso/projekce-obyvatelstva-v-krajich-cr-do-roku-2070 (accessed on 29 August 2020).
- Eurostat. Available online: https://ec.europa.eu/eurostat (accessed on 25 December 2018).
- Tomaskova, H.; Kuhnova, J.; Cimler, R.; Dolezal, O.; Kuca, K. Prediction of population with Alzheimer’s disease in the European Union using a system dynamics model. Neuropsychiatr. Dis. Treat. 2016, 12, 1589–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spackman, D.E.; Kadiyala, S.; Neumann, P.J.; Veenstra, D.L.; Sullivan, S.D. Measuring Alzheimer disease progression with transition probabilities: Estimates from NACC-UDS. Curr. Alzheimer Res. 2012, 9, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Arizaga, R.L. Epidemiology of dementia. In Dementia: A Multidisciplinary Approach, 2nd ed.; Mangone, C.A., Allegri, R.F., Arizaga, R.L., Ollari, J.A., Eds.; Polemos: Buenos Aires, Argentina, 2005; pp. 7–17. [Google Scholar]
- Hanzalova, M.; Pazitny, P.; Kandilaki, D. Prevalence of Alzheimer’s Disease in Retirement Homes and Homes with a Special Regime in the Czech Republic. In Proceedings of the International Scientific Conference Hradec Economic Days 2020, Hradec Kralove, Czech Republic, 2–3 April 2020; Faculty of Informatics and Management, University of Hradec Kralove: Hradec Kralove, Czech Republic, 2020; pp. 228–234. [Google Scholar] [CrossRef]
- Pazitny, P.; Kandilaki, D.; Komarkova, L. Current capacity gap in dementia/AD in the Czech Republic. In Proceedings of the 13th International Scientific Conference INPROFORUM, 100 Years of the Koruna, Ceske Budejovice, Czech Republic, 7–8 November 2019; Faculty of Economics, University of South Bohemia: Ceske Budejovice, Czech Republic, 2019; pp. 251–258. [Google Scholar]
- Holmerova, I.; Hort, J.; Rusina, R.; Wimo, A.; Steffl, M. Costs of dementia in the Czech Republic. Eur. J. Health Econ. 2017, 18, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Handels, R.L.H.; Wolfs, C.A.G.; Aalten, P.; Verhey, F.R.J.; Severens, J.L. Determinants of Care Costs of Patients with Dementia or Cognitive Impairment. Alzheimer Dis. Assoc. Disord. 2013, 27, 30–36. [Google Scholar] [CrossRef] [PubMed]
- El-Hayek, Y.H.; Wiley, R.E.; Khoury, C.P.; Daya, R.P.; Ballard, C.; Evans, A.R.; Karran, M.; Molinuevo, J.L.; Norton, M.; Atri, A. Tip of the Iceberg: Assessing the Global Socioeconomic Costs of Alzheimer’s Disease and Related Dementias and Strategic Implications for Stakeholders. JAD 2019, 70, 323–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexa, J.; Recka, L.; Votapkova, J.; van Ginneken, E.; Spranger, A.; Wittenbecher, F. Czech Republic: Health system review. Health Syst. Transit. 2015, 17, 1–165. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/280706/Czech-HiT.pdf (accessed on 6 October 2020). [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Number of 65+ | Percentage of 65+ | ||||||
|---|---|---|---|---|---|---|---|---|
| 2020 | 2030 | 2050 | 2070 | 2020 | 2030 | 2050 | 2070 | |
| KHK | 119,380 | 132,425 | 158,148 | 141,309 | 21.7 | 24.4 | 31.0 | 29.9 |
| VYS | 104,649 | 120,262 | 147,689 | 130,291 | 20.5 | 24.3 | 31.9 | 30.6 |
| Variable | Structure | Input Data | Initial Phase Description |
|---|---|---|---|
| Population size | Matrix 96 × 53 (96 age cohorts: 0–95+; 53 years: 2019–2071) | [40] | Population for regions from 2019 (the Czech Statistical Office data). For each region, there is a specific dataset with the same structure. |
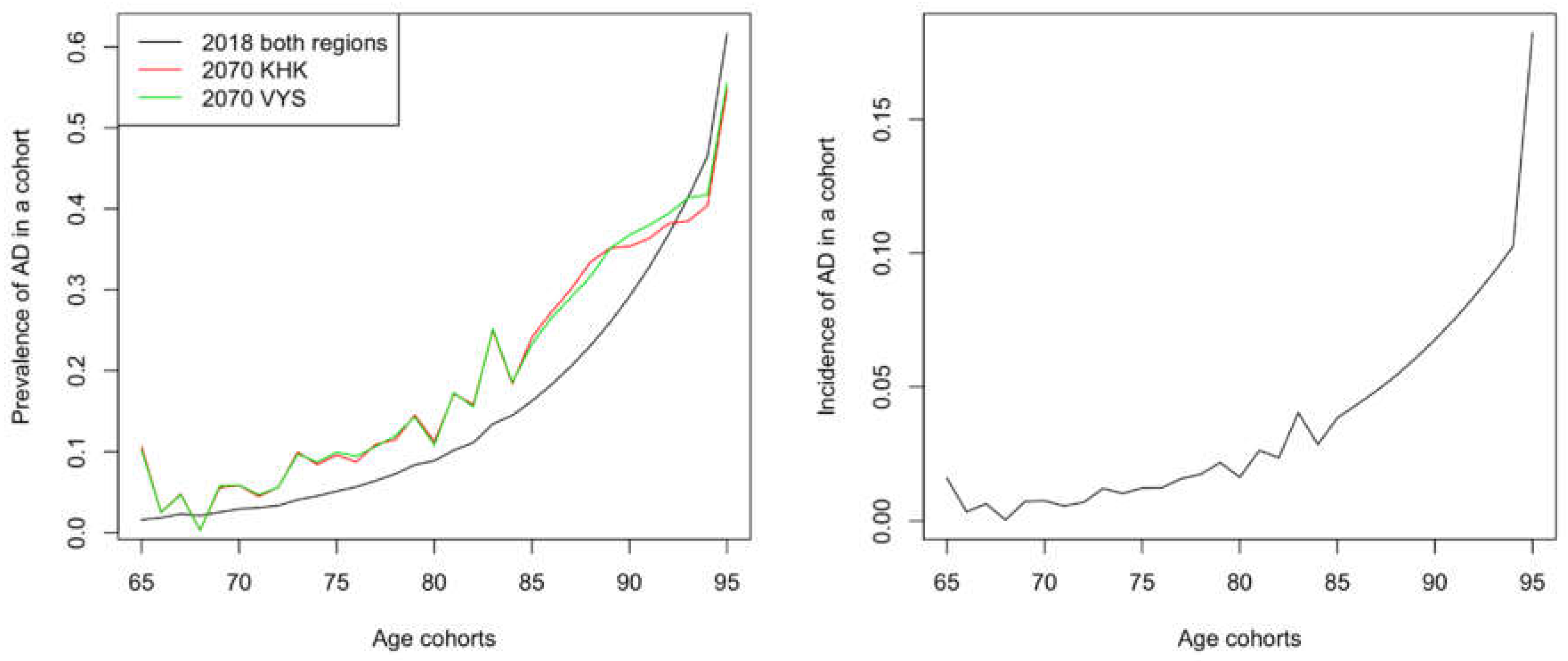
| Prevalence AD | 31 values (from 65 to 95+) | [42,44] | Based on the values for the EU, see Figure 1. |
| Incidence AD | 31 values (from 65 to 95+) | [39] | Derived from AD prevalence, see Figure 1. |
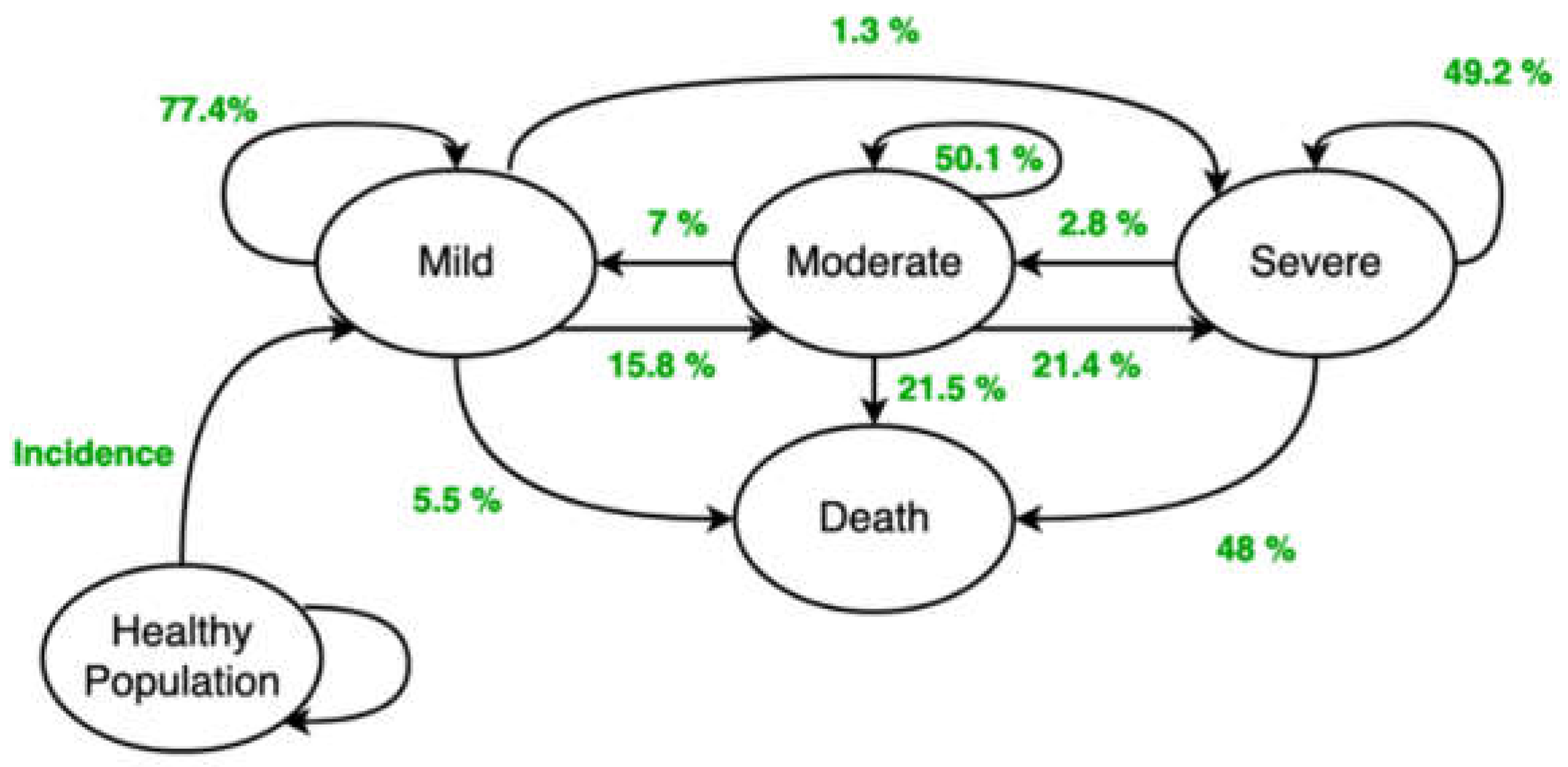
| Transition probabilities | Matrix 4 × 4 (3 stages and death) | [43] | The transition probabilities between the disease stages (Figure 2). |
| Individual stage proportions | 3 values (mild, moderate, severe) | Limit Distribution | Initial division of patients into individual stages. |
| Costs | Data Source | Stage Identification | Year(s) |
|---|---|---|---|
| Medical | Institute of Health Information and Statistics of the Czech Republic | According to Mini Mental State Exam (MMSE) within age cohorts | 2017 |
| Non-medical | Webpages of the regional governments | Based on expert estimates from personal meetings | 2019–2020 |
| Questionnaire [45] for social service providers | 2019 |
| KHK | Outpatient | Inpatient | |||||
|---|---|---|---|---|---|---|---|
| Stage | Age Cohort | “Point” System | Other Services | Medicines | “Point” System | Acute Care | Other Care |
| Mild | 65–69 | 435.77 | 31.77 | 72.00 | 0.00 | 243.42 | 442.54 |
| 70–79 | 268.15 | 34.35 | 22.35 | 0.00 | 236.88 | 489.04 | |
| 80–89 | 187.77 | 15.23 | 33.35 | 0.00 | 264.69 | 574.23 | |
| 90+ | 164.85 | 6.27 | 3.35 | 0.00 | 263.15 | 976.08 | |
| Moderate | 65–69 | 227.35 | 23.46 | 77.27 | 0.00 | 166.77 | 557.00 |
| 70–79 | 212.31 | 24.12 | 9.46 | 0.00 | 291.65 | 772.62 | |
| 80–89 | 182.96 | 13.08 | 50.15 | 0.15 | 242.38 | 506.92 | |
| 90+ | 154.69 | 10.19 | 5.54 | 0.00 | 125.00 | 0.00 | |
| Severe | 65–69 | 188.42 | 52.58 | 25.58 | 0.00 | 170.04 | 356.77 |
| 70–79 | 213.77 | 21.85 | 294.54 | 0.00 | 307.88 | 685.92 | |
| 80–89 | 161.15 | 11.81 | 9.00 | 0.00 | 298.85 | 715.96 | |
| 90+ | 120.42 | 8.35 | 7.65 | 0.00 | 224.54 | 891.38 | |
| VYS | Outpatient | Inpatient | |||||
|---|---|---|---|---|---|---|---|
| Stage | Age Cohort | “Point” System | Other Services | Medicines | “Point” System | Acute Care | Other Care |
| Mild | 65–69 | 244.69 | 30.85 | 454.62 | 0.00 | 316.85 | 586.85 |
| 70–79 | 232.23 | 19.54 | 75.58 | 0.00 | 194.00 | 453.85 | |
| 80–89 | 251.15 | 12.00 | 14.19 | 0.00 | 260.92 | 711.69 | |
| 90+ | 157.42 | 6.54 | 7.08 | 0.00 | 308.73 | 668.38 | |
| Moderate | 65–69 | 194.35 | 24.38 | 1.85 | 0.00 | 107.42 | 761.92 |
| 70–79 | 202.00 | 19.12 | 5.92 | 0.00 | 167.58 | 708.12 | |
| 80–89 | 201.35 | 8.65 | 3.92 | 0.00 | 193.62 | 722.12 | |
| 90+ | 187.04 | 13.50 | 4.54 | 0.00 | 263.73 | 868.12 | |
| Severe | 65–69 | 185.35 | 25.23 | 2.73 | 0.00 | 187.19 | 647.42 |
| 70–79 | 210.12 | 18.42 | 41.81 | 0.00 | 215.08 | 531.62 | |
| 80–89 | 261.31 | 9.08 | 12.58 | 0.00 | 257.73 | 832.12 | |
| 90+ | 157.92 | 3.23 | 19.58 | 0.00 | 276.35 | 987.19 | |
| Region | KHK | VYS | ||||
|---|---|---|---|---|---|---|
| Residential Services | Capacity (beds) | For AD (%) | Unit Cost (EUR) | Capacity (beds) | For AD (%) | Unit Cost (EUR) |
| Respite Care | 67 | 78 | 44.65 | 39 | 78 | 71.15 |
| Week Care Centres | 9 | 47 | 45.58 | 0 | 47 | 76.92 |
| Homes for the Elderly | 2019 | 17 | 39.77 | 1977 | 20 | 51.92 |
| Special Regime Homes | 447 | 90 | 44.73 | 812 | 80 | 53.85 |
| Health Care Facilities | 34 | 47 | 23.77 | 57 | 47 | 33.08 |
| Region | KHK | VYS | ||||
|---|---|---|---|---|---|---|
| Outpatient & Domiciliary Services | Capacity (FTE) | For AD (%) | Unit Cost (EUR) | Capacity (FTE) | For AD (%) | Unit Cost (EUR) |
| Personal Assistance | 82 | 50 | 1605.96 | 83 | 50 | 1961.54 |
| Day Services Centres | 8 | 50 | 2184.31 | 23 | 50 | 2153.85 |
| Daycare Centres | 31 | 50 | 1681.62 | 117 | 50 | 2153.85 |
| Domiciliary Service | 412 | 50 | 1804.54 | 405 | 50 | 1961.54 |
| Respite Care | 0 | 78 | 0.00 | 25 | 78 | 2346.15 |
| Costs/Year | 2020 | 2030 | 2040 | 2050 | 2060 | 2070 |
|---|---|---|---|---|---|---|
| KHK Region | 25.636 | 40.288 | 51.384 | 57.263 | 64.425 | 69.018 |
| Medical | 4.289 | 6.866 | 8.589 | 9.592 | 10.695 | 11.245 |
| Non-medical | 21.347 | 33.422 | 42.795 | 47.671 | 53.730 | 57.773 |
| VYS Region | 38.484 | 61.034 | 78.587 | 90.674 | 102.025 | 107.983 |
| Medical | 3.977 | 6.441 | 8.229 | 9.490 | 10.683 | 11.184 |
| Non-medical | 34.508 | 54.593 | 70.358 | 81.184 | 91.342 | 96.799 |
| Stage | Mild | Moderate | Severe | No Resolution | ||||
|---|---|---|---|---|---|---|---|---|
| Direct Costs | KHK | VYS | KHK | VYS | KHK | VYS | KHK | VYS |
| Medical | 359 | 354 | 298 | 389 | 1624 | 1671 | 482 | 504 |
| Non-medical | 2330 | 4229 | 2330 | 4229 | 2330 | 4229 | 2330 | 4229 |
| Total | 2689 | 4583 | 2628 | 4618 | 3954 | 5900 | 2812 | 4733 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maresova, P.; Komarkova, L.; Kuhnova, J.; Cimler, R.; Pazitny, P.; Kandilaki, D.; Musilek, K.; Truhlarova, Z.; Zemek, F.; Kuca, K. Anticipated Social and Healthcare Economic Burden of People with Alzheimer’s Disease in Two Selected Regions of the Czech Republic. Healthcare 2020, 8, 433. https://doi.org/10.3390/healthcare8040433
Maresova P, Komarkova L, Kuhnova J, Cimler R, Pazitny P, Kandilaki D, Musilek K, Truhlarova Z, Zemek F, Kuca K. Anticipated Social and Healthcare Economic Burden of People with Alzheimer’s Disease in Two Selected Regions of the Czech Republic. Healthcare. 2020; 8(4):433. https://doi.org/10.3390/healthcare8040433
Chicago/Turabian StyleMaresova, Petra, Lenka Komarkova, Jitka Kuhnova, Richard Cimler, Peter Pazitny, Daniela Kandilaki, Kamil Musilek, Zuzana Truhlarova, Filip Zemek, and Kamil Kuca. 2020. "Anticipated Social and Healthcare Economic Burden of People with Alzheimer’s Disease in Two Selected Regions of the Czech Republic" Healthcare 8, no. 4: 433. https://doi.org/10.3390/healthcare8040433