Effect of Dysphagia Rehabilitation Using Kinesiology Taping on Oropharyngeal Muscle Hypertrophy in Post-Stroke Patients: A Double Blind Randomized Placebo-Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
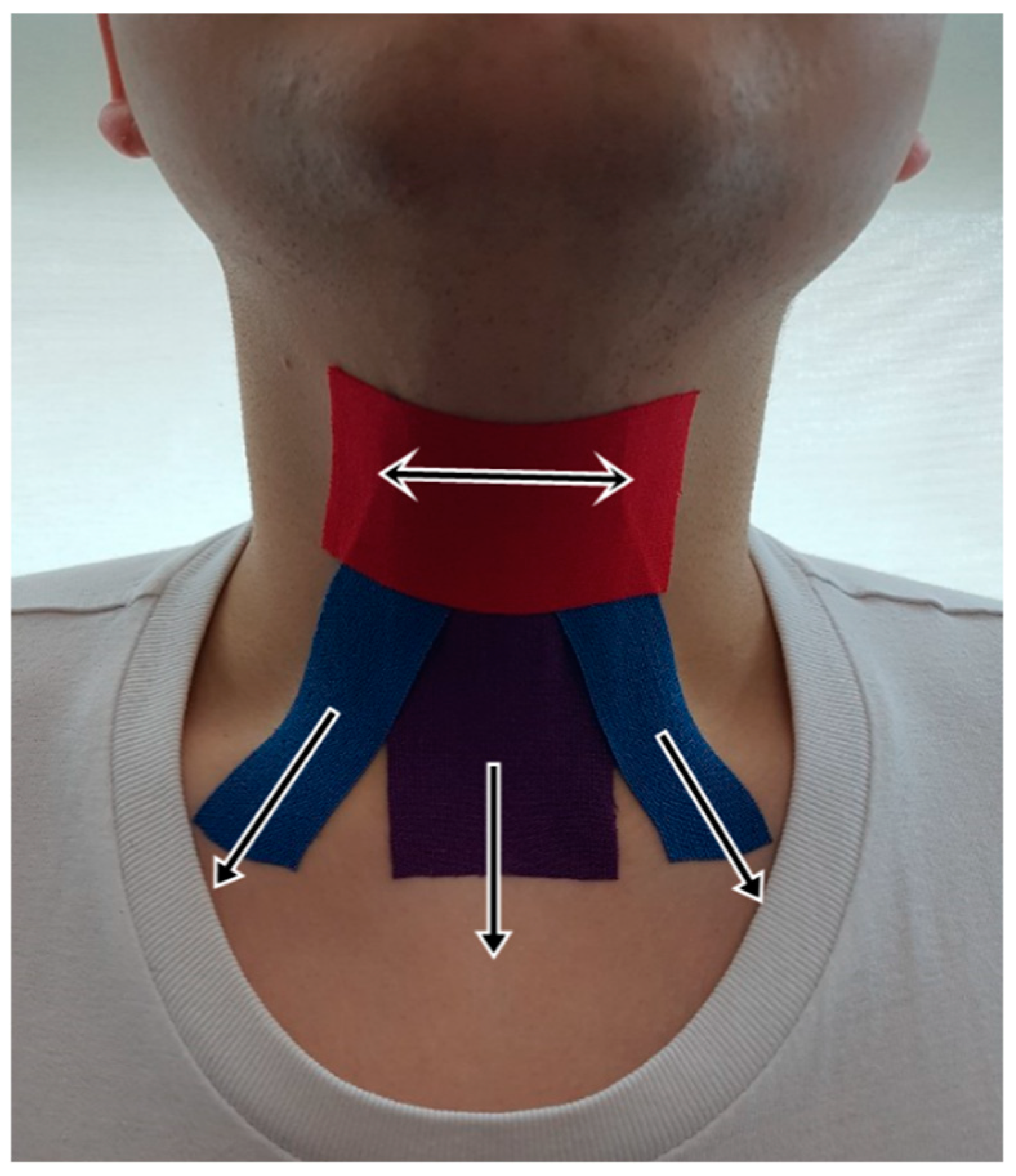
2.2. Procedures
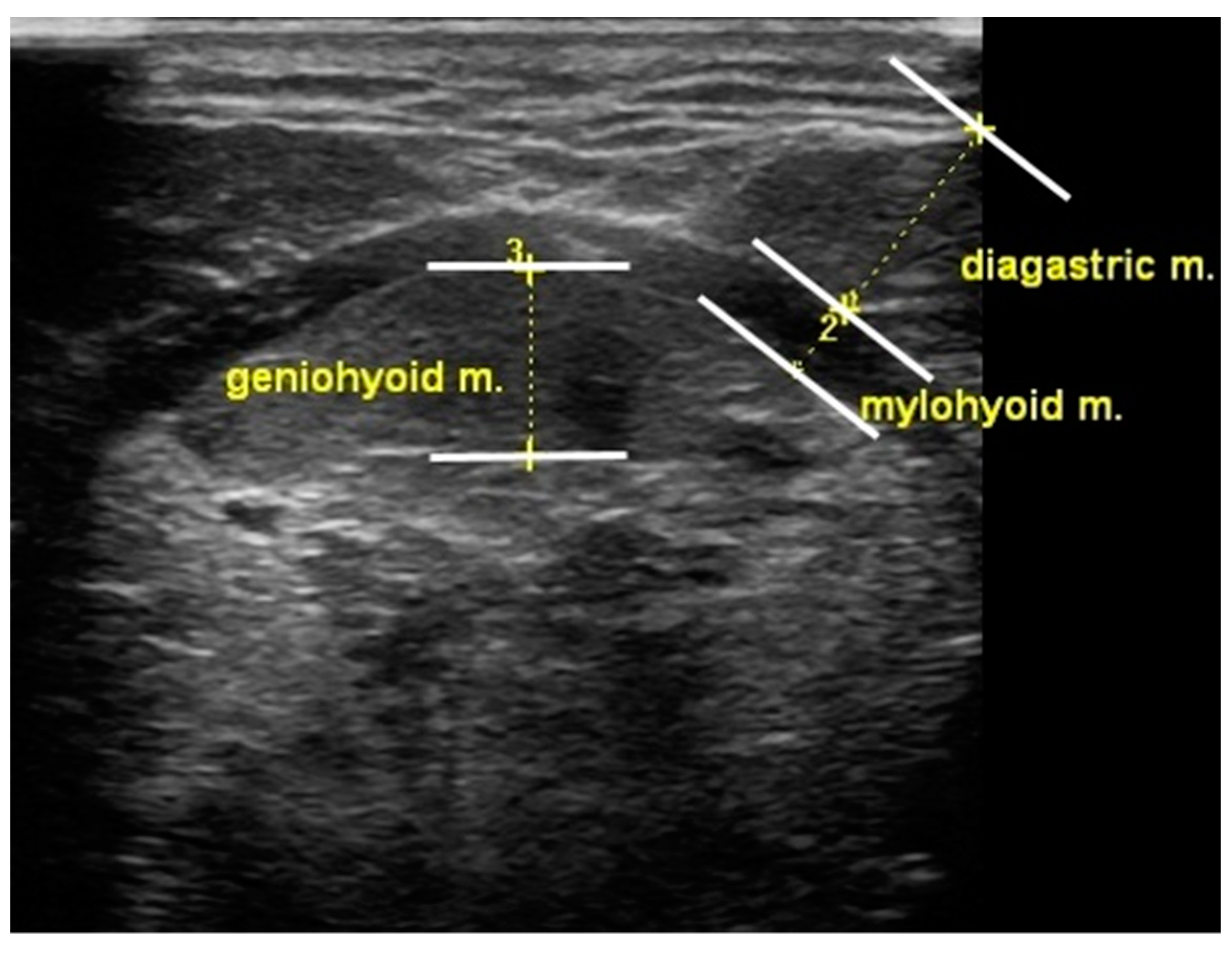
2.3. Outcome Measurement
2.4. Statistical Analysis
3. Results
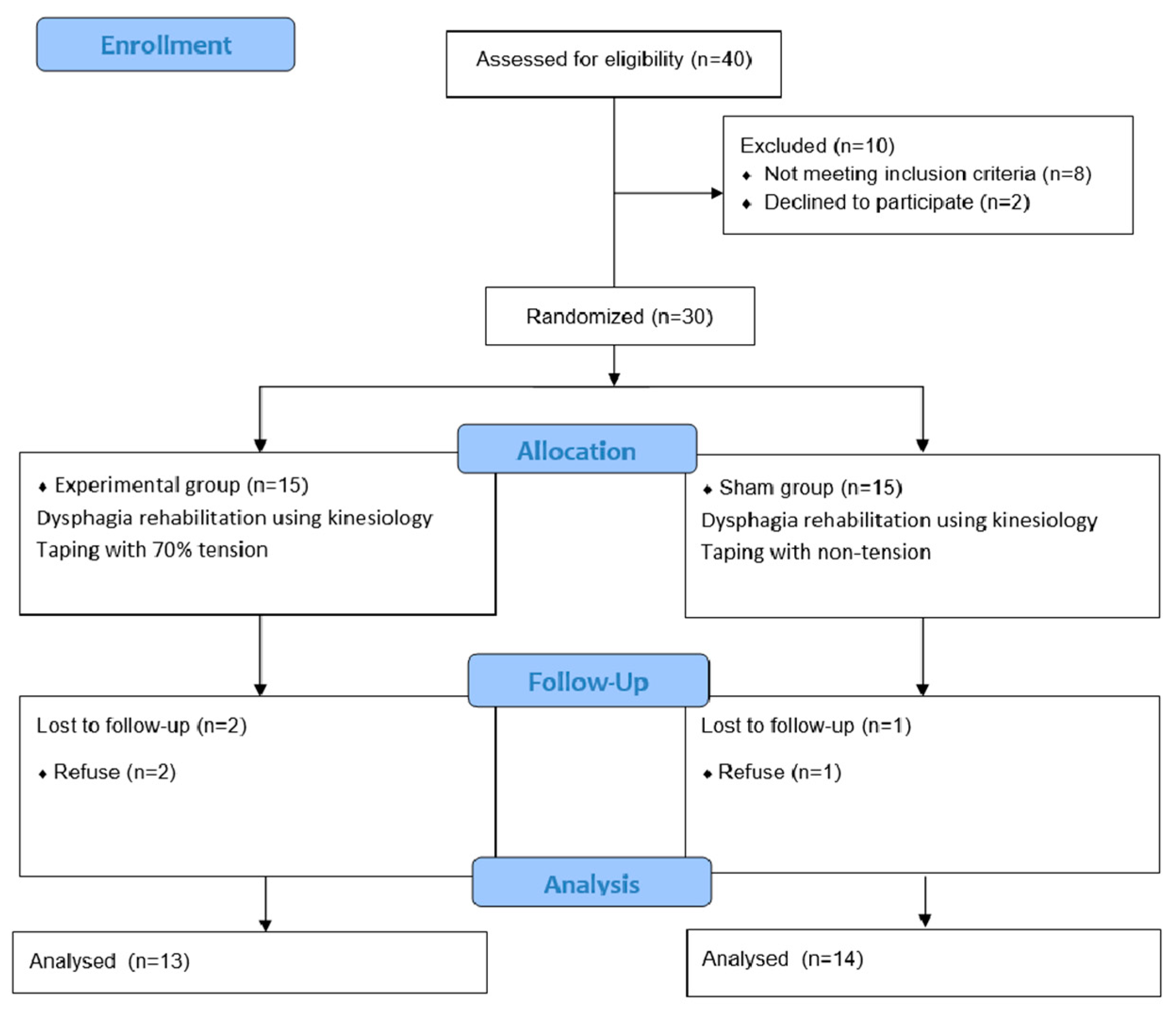
3.1. Participants
3.2. Tongue Muscle Thickness
3.3. Suprahyoid Muscle Thickness
3.4. Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Martino, R.; Foley, N.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia after stroke: Incidence, diagnosis and pulmonary complications. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef] [Green Version]
- Perry, L.; Love, C.P. Screening for Dysphagia and Aspiration in Acute Stroke: A Systematic Review. Dysphagia 2001, 16, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Reber, E.; Gomes, F.; Dähn, I.A.; Vasiloglou, M.F.; Stanga, Z.G. Management of Dehydration in Patients Suffering Swallowing Difficulties. J. Clin. Med. 2019, 8, 1923. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-S.; Hwang, N.K.; Oh, D.H.; Chang, M. Effect of head lift exercise on kinematic motion of the hyolaryngeal complex and aspiration in patients with dysphagic stroke. J. Oral Rehabil. 2017, 44, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R. A Systematic Review of the Prevalence of Oropharyngeal Dysphagia in Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, and Pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Silbergleit, A.K.; Schultz, L.; Jacobson, B.H.; Beardsley, T.; Johnson, A.F. The Dysphagia Handicap Index: Development and Validation. Dysphagia 2011, 27, 46–52. [Google Scholar] [CrossRef]
- Ekberg, O.; Hamdy, S.; Woisard, V.; Wuttge-Hannig, A.; Ortega, P. Social and Psychological Burden of Dysphagia: Its Impact on Diagnosis and Treatment. Dysphagia 2002, 17, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Hamdy, S. Dysphagia in stroke patients. Postgrad. Med. J. 2006, 82, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falsetti, P.; Acciai, C.; Palilla, R.; Bosi, M.; Carpinteri, F.; Zingarelli, A.; Pedace, C.; Lenzi, L. Oropharyngeal Dysphagia after Stroke: Incidence, Diagnosis, and Clinical Predictors in Patients Admitted to a Neurorehabilitation Unit. J. Stroke Cerebrovasc. Dis. 2009, 18, 329–335. [Google Scholar] [CrossRef]
- González-Fernández, M.; Ottenstein, L.; Atanelov, L.; Christian, A.B. Dysphagia after stroke: An overview. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 187–196. [Google Scholar] [CrossRef]
- Martino, R.; Pron, G.; Diamant, N. Screening for Oropharyngeal Dysphagia in Stroke: Insufficient Evidence for Guidelines. Dysphagia 2000, 15, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Yano, J.; Yamamoto-Shimizu, S.; Yokoyama, T.; Kumakura, I.; Hanayama, K.; Tsubahara, A. Effects of Tongue-Strengthening Exercise on the Geniohyoid Muscle in Young Healthy Adults. Dysphagia 2020, 35, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Pearson, W.G., Jr.; Langmore, S.E.; Yu, L.B.; Zumwalt, A.C. Structural Analysis of Muscles Elevating the Hyolaryngeal Complex. Dysphagia 2012, 27, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Pearson, W.G., Jr.; Hindson, D.F.; Langmore, S.E.; Zumwalt, A.C. Evaluating Swallowing Muscles Essential for Hyolaryngeal Elevation by Using Muscle Functional Magnetic Resonance Imaging. Int. J. Radiat. Oncol. 2013, 85, 735–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-S.; Oh, D.-H.; Hwang, N.-K.; Lee, J.-H. Effects of neuromuscular electrical stimulation combined with effortful swallowing on post-stroke oropharyngeal dysphagia: A randomised controlled trial. J. Oral Rehabil. 2016, 43, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Jacob, P.; Kahrilas, P.; Logemann, J.; Shah, V.; Ha, T. Upper esophageal sphincter opening and modulation during swallowing. Gastroenterology 1989, 97, 1469–1478. [Google Scholar] [CrossRef]
- Logemann, J.A.; Kahrilas, P.J.; Cheng, J.; Pauloski, B.R.; Gibbons, P.J.; Rademaker, A.W.; Lin, S. Closure mechanisms of laryngeal vestibule during swallow. Am. J. Physiol. Liver Physiol. 1992, 262, G338–G344. [Google Scholar] [CrossRef]
- Steele, C.M. Exercise-based approaches to dysphagia rehabilitation. Nestle Nutr. Inst. Workshop Ser. 2012, 72, 109–117. [Google Scholar]
- Krekeler, B.N.; Rowe, L.M.; Connor, N.P. Dose in Exercise-Based Dysphagia Therapies: A Scoping Review. Dysphagia 2020. [Google Scholar] [CrossRef]
- Mishra, A.; Rajappa, A.; Tipton, E.; Malandraki, G.A. The Recline Exercise: Comparisons with the Head Lift Exercise in Healthy Adults. Dysphagia 2015, 30, 730–737. [Google Scholar] [CrossRef]
- Park, J.-S.; Lee, S.-H.; Jung, S.-H.; Choi, J.-B.; Jung, Y.-J. Tongue strengthening exercise is effective in improving the oropharyngeal muscles associated with swallowing in community-dwelling older adults in South Korea. Medicine 2019, 98, e17304. [Google Scholar] [CrossRef] [PubMed]
- Steen, L.V.D.; Vanderwegen, J.; Guns, C.; Elen, R.; De Bodt, M.; Van Nuffelen, G. Tongue-Strengthening Exercises in Healthy Older Adults: Does Exercise Load Matter? A Randomized Controlled Trial. Dysphagia 2019, 34, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Oh, D.H.; Chang, M.Y.; Kim, K.M. Effects of expiratory muscle strength training on oropharyngeal dysphagia in subacute stroke patients: A randomised controlled trial. J. Oral Rehabil. 2016, 43, 364–372. [Google Scholar] [CrossRef]
- Wheeler, K.M.; Chiara, T.; Sapienza, C.M. Surface Electromyographic Activity of the Submental Muscles During Swallow and Expiratory Pressure Threshold Training Tasks. Dysphagia 2007, 22, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-S.; Oh, D.-H.; Yoon, T.; Park, J.-S. Effect of effortful swallowing training on tongue strength and oropharyngeal swallowing function in stroke patients with dysphagia: A double-blind, randomized controlled trial. Int. J. Lang. Commun. Disord. 2019, 54, 479–484. [Google Scholar] [CrossRef]
- Jang, H.J.; Leigh, J.H.; Gil Seo, H.; Han, T.R.; Oh, B.-M. Effortful swallow enhances vertical hyolaryngeal movement and prolongs duration after maximal excursion. J. Oral Rehabil. 2015, 42, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Yoon, W.L.; Khoo, J.K.P.; Liow, S.J.R. Chin Tuck Against Resistance (CTAR): New Method for Enhancing Suprahyoid Muscle Activity Using a Shaker-type Exercise. Dysphagia 2014, 29, 243–248. [Google Scholar] [CrossRef]
- Kılınç, H.E.; Arslan, S.S.; Demir, N.; Karaduman, A. The Effects of Different Exercise Trainings on Suprahyoid Muscle Activation, Tongue Pressure Force and Dysphagia Limit in Healthy Subjects. Dysphagia 2019, 35, 717–724. [Google Scholar] [CrossRef]
- Balasubramanium, R.K.; Krishnamurthy, R.; Rajan, A.; K, S. Forehead against Resistance (FAR): Preliminary Findings from A Clinical Alternative to Shaker’s Type of Exercise. Gastroenterol. Res. Pract. 2019. [Google Scholar] [CrossRef]
- Hughes, T.; Watts, C.R. Effects of 2 Resistive Exercises on Electrophysiological Measures of Submandibular Muscle Activity. Arch. Phys. Med. Rehabil. 2016, 97, 1552–1557. [Google Scholar] [CrossRef]
- Inamoto, Y.; Saitoh, E.; Ito, Y.; Kagaya, H.; Aoyagi, Y.; Shibata, S.; Ota, K.; Fujii, N.; Palmer, J.B. The Mendelsohn Maneuver and its Effects on Swallowing: Kinematic Analysis in Three Dimensions Using Dynamic Area Detector CT. Dysphagia 2018, 33, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, T.; Ono, T.; Hori, K.; Tamine, K.-I.; Nozaki, S.; Shimada, K.; Yamamoto, N.; Fukuda, Y.; Domen, K. Effect of the Effortful Swallow and the Mendelsohn Maneuver on Tongue Pressure Production against the Hard Palate. Dysphagia 2013, 28, 539–547. [Google Scholar] [CrossRef]
- Matsubara, M.; Tohara, H.; Hara, K.; Shinozaki, H.; Yamazaki, Y.; Susa, C.; Nakane, A.; Wakasugi, Y.; Minakuchi, S. High-speed jaw-opening exercise in training suprahyoid fast-twitch muscle fibers. Clin. Interv. Aging 2018, 13, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-S.; An, D.-H.; Kam, K.-Y.; Yoon, T.; Kim, T.; Chang, M.-Y. Effects of resistive jaw opening exercise in stroke patients with dysphagia: A double- blind, randomized controlled study. J. Back Musculoskelet. Rehabil. 2020, 33, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Sayaca, C.; Serel-Arslan, S.; Sayaca, N.; Demir, N.; Somay, G.; Kaya, D.; Karaduman, A. Is the proprioceptive neuromuscular facilitation technique superior to Shaker exercises in swallowing rehabilitation? Eur. Arch. Otorhinolaryngol. 2020, 277, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.-C. Effect of partial head extension swallowing exercise on the strength of the suprahyoid and tongue muscles in healthy subjects: A feasibility study. J. Oral Rehabil. 2018, 46, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.-C. Effect of the head extension swallowing exercise on suprahyoid muscle activity in elderly individuals. Exp. Gerontol. 2018, 110, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Shaker, R.; Sanvanson, P.; Balasubramanian, G.; Kern, M.K.; Wuerl, A.; Hyngstrom, A.S. Effects of laryngeal restriction on pharyngeal peristalsis and biomechanics: Clinical implications. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 310, G1036–G1043. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, D.; Kern, M.; Edeani, F.; Balasubramanian, G.; Hyngstrom, A.; Sanvanson, P.; Shaker, R. Swallow strength training exercise for elderly: A health maintenance need. Neurogastroenterol. Motil. 2018, 30, e13382. [Google Scholar] [CrossRef]
- Karsten, R.T.; Ter Beek, L.C.; Jasperse, B.; Van Alphen, M.J.A.; Peeters, J.M.; Van Der Molen, L.; Hilgers, F.J.M.; Stuiver, M.M.; Smeele, L.E. MRI Assessment of Swallow Muscle Activation with the Swallow Exercise Aid and with Conventional Exercises in Healthy Volunteers: An Explorative Biomechanical Study. Dysphagia 2020. [Google Scholar] [CrossRef]
- Kraaijenga, S.A.C.; Van Der Molen, L.; Stuiver, M.M.; Teertstra, H.J.; Hilgers, F.J.M.; van den Brekel, M.W. Effects of Strengthening Exercises on Swallowing Musculature and Function in Senior Healthy Subjects: A Prospective Effectiveness and Feasibility Study. Dysphagia 2015, 30, 392–403. [Google Scholar] [CrossRef]
- Park, J.-S.; Jung, Y.-J.; Kim, H.-H.; Lee, G. A Novel Method Using Kinesiology Taping for the Activation of Suprahyoid Muscles in Healthy Adults: A Preliminary Research. Dysphagia 2020, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Park, T.; Kim, Y. Effects of tongue pressing effortful swallow in older healthy individuals. Arch. Gerontol. Geriatr. 2016, 66, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG: An update. J. Appl. Physiol. 2014, 117, 1215–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh, H.T.; Cho, S.-Y.; So, W.-Y. A Cross-Sectional Study Evaluating the Effects of Resistance Exercise on Inflammation and Neurotrophic Factors in Elderly Women with Obesity. J. Clin. Med. 2020, 9, 842. [Google Scholar] [CrossRef] [Green Version]
- Fry, A.C. The Role of Resistance Exercise Intensity on Muscle Fibre Adaptations. Sports Med. 2004, 34, 663–679. [Google Scholar] [CrossRef]
- Androulakis-Korakakis, P.; Fisher, J.P.; Steele, J. The Minimum Effective Training Dose Required to Increase 1RM Strength in Resistance-Trained Men: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 751–765. [Google Scholar] [CrossRef]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of Resistance Training Frequency on Gains in Muscular Strength: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Experimental Group | Sham Group | |
|---|---|---|
| Number of subjects | 13 | 14 |
| Gender (male/female) | 5/8 | 6/8 |
| Age (year) | 71.3 ± 6.5 | 70.5 ± 8.2 |
| Stroke onset (weeks) | 16.2 ± 5.2 | 15.1 ± 6.4 |
| Stroke type | ||
| Hemorrhage | 7 | 5 |
| Infarction | 6 | 9 |
| Site of stroke lesion | ||
| Middle cerebral artery | 12 | 13 |
| Pontine | 1 | 1 |
| Paretic side (Left/Right) | 6/7 | 8/5 |
| Taping tension | 70% tension | Non-tension |
| Experimental Group | Sham Group | Intergroup p-Values | |||||
|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | p-Value in Group | Pre-Intervention | Post-Intervention | p-Value in Group | ||
| TM | 41.09 ± 3.19 | 42.86 ± 2.86 | <0.001 * | 39.64 ± 2.50 | 39.80 ± 2.53 | 0.182 | 0.007 † |
| MHM | 0.76 ± 0.11 | 0.88 ± 0.07 | <0.001 * | 0.73 ± 0.08 | 0.75 ± 0.10 | 0.231 | 0.002 † |
| ADM | 6.34 ± 0.36 | 6.67 ± 0.38 | <0.001 * | 6.09 ± 0.22 | 6.10 ± 0.21 | 0.198 | 0.001 † |
| Experimental Group | Sham Group | p-Value | |
|---|---|---|---|
| TM | 1.77 ± 1.03 | 0.15 ± 0.35 | <0.001 † |
| MHM | 0.11 ± 0.08 | 0.01 ± 0.04 | <0.001 † |
| ADM | 0.34 ± 0.21 | 0.01 ± 0.03 | <0.001 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.-J.; Kim, H.-J.; Choi, J.-B.; Park, J.-S.; Hwang, N.-K. Effect of Dysphagia Rehabilitation Using Kinesiology Taping on Oropharyngeal Muscle Hypertrophy in Post-Stroke Patients: A Double Blind Randomized Placebo-Controlled Trial. Healthcare 2020, 8, 411. https://doi.org/10.3390/healthcare8040411
Jung Y-J, Kim H-J, Choi J-B, Park J-S, Hwang N-K. Effect of Dysphagia Rehabilitation Using Kinesiology Taping on Oropharyngeal Muscle Hypertrophy in Post-Stroke Patients: A Double Blind Randomized Placebo-Controlled Trial. Healthcare. 2020; 8(4):411. https://doi.org/10.3390/healthcare8040411
Chicago/Turabian StyleJung, Young-Jin, Hee-Jeong Kim, Jong-Bae Choi, Ji-Su Park, and Na-Kyoung Hwang. 2020. "Effect of Dysphagia Rehabilitation Using Kinesiology Taping on Oropharyngeal Muscle Hypertrophy in Post-Stroke Patients: A Double Blind Randomized Placebo-Controlled Trial" Healthcare 8, no. 4: 411. https://doi.org/10.3390/healthcare8040411