
Personalized Use of an Adjustable Movement-Controlled Video Game in Obstetric Brachial Plexus Palsy during Physiotherapy Sessions at School: A Case Report

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Information
2.2. Clinical Findings
2.3. Environment of the Study
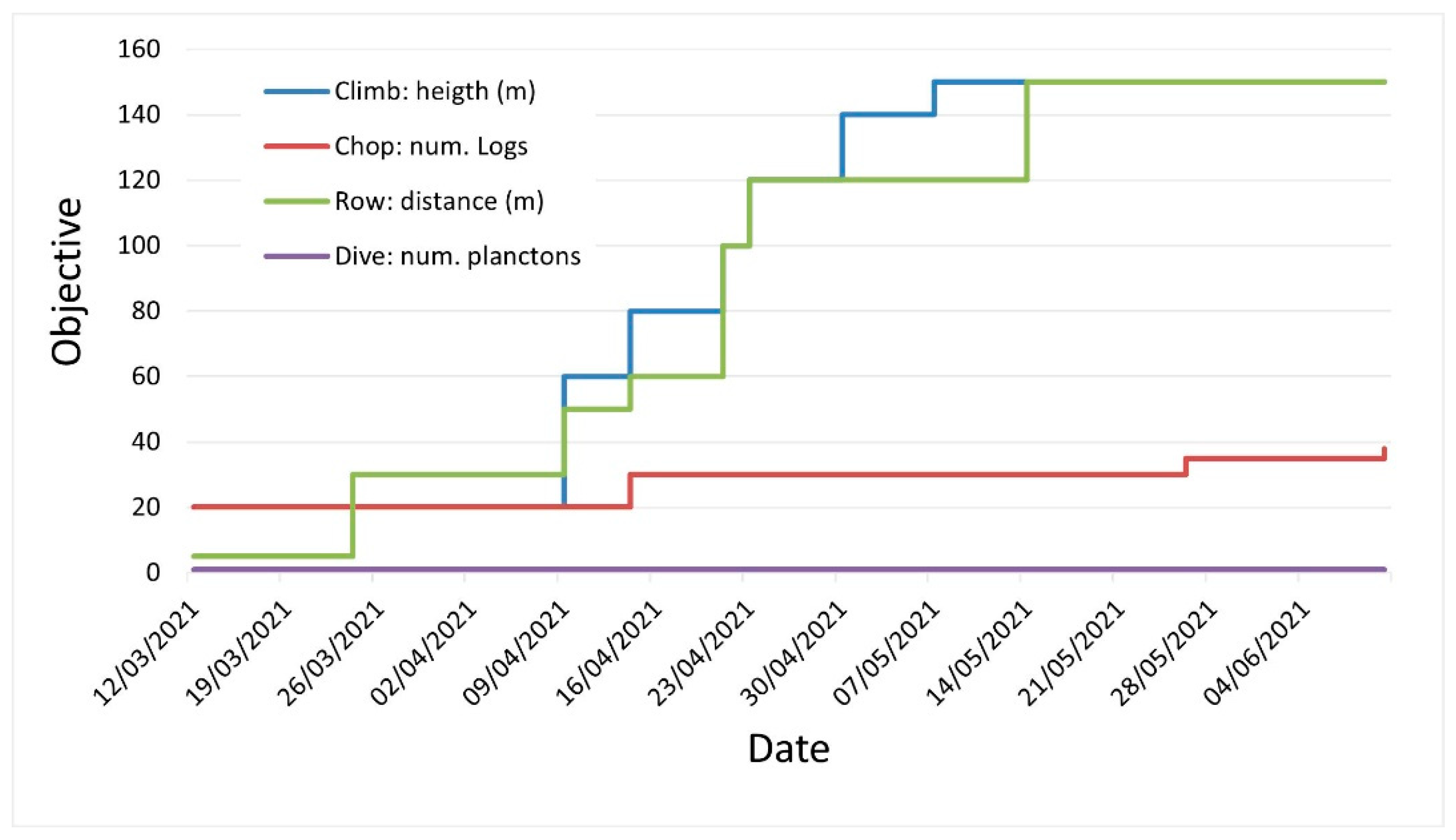
- Chop: This includes raising and lowering the affected arm, requiring maximum shoulder flexion, posture stability to keep the axe raised until it is loaded, and a certain speed to lower the arm. The time limit and number of logs to be cut can be adjusted.
- Climb: This includes asymmetric movement in abduction of the arms and shoulder flexion, requiring an alternating movement of abduction. The time limit and height of the tree in meters (one meter is equivalent to one arm movement) can be adjusted.
- Row: This includes symmetrical movement of the upper limbs. of the time limit and width of the river in meters (one meter is equivalent to one back and forth arm movement) can be adjusted.
- Dive: This includes control and stability of the trunk. The time limit and number of plankton balls to be caught can be adjusted.
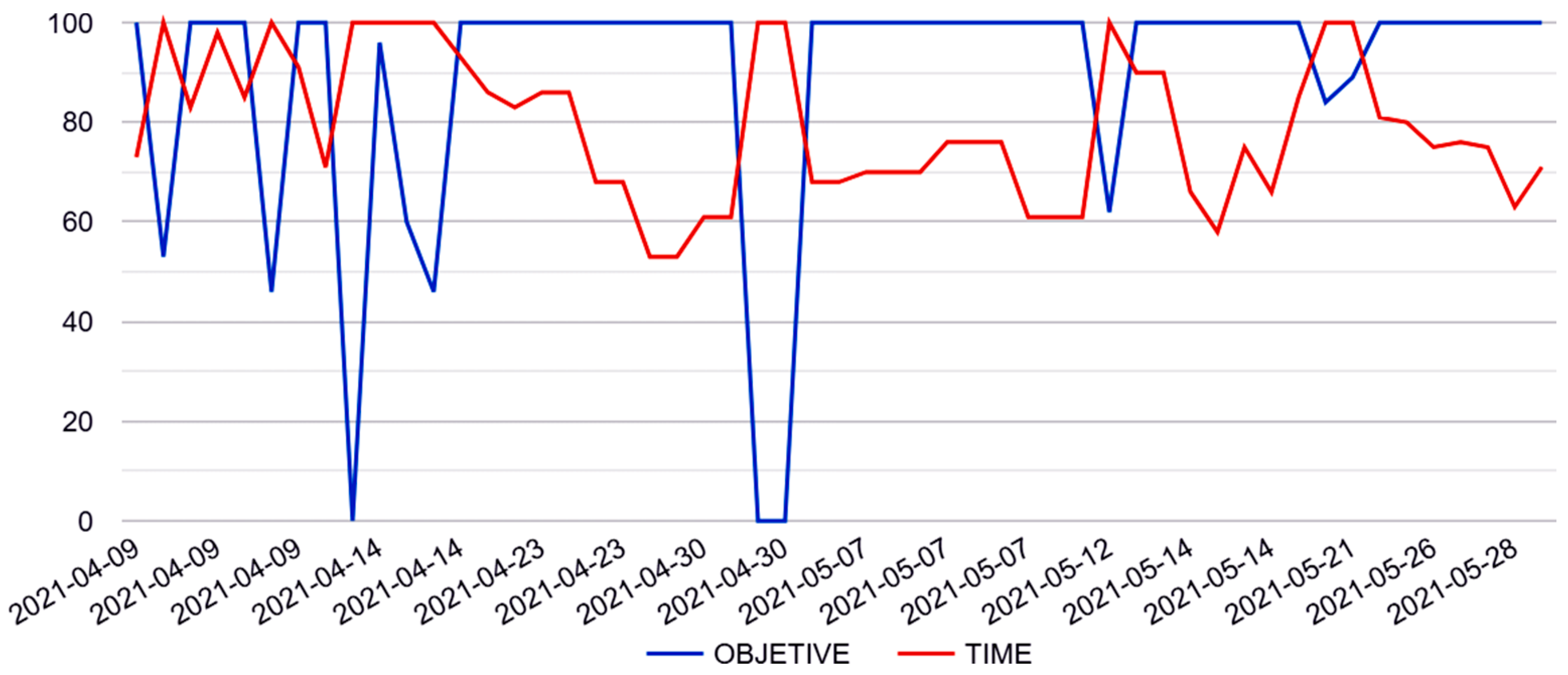
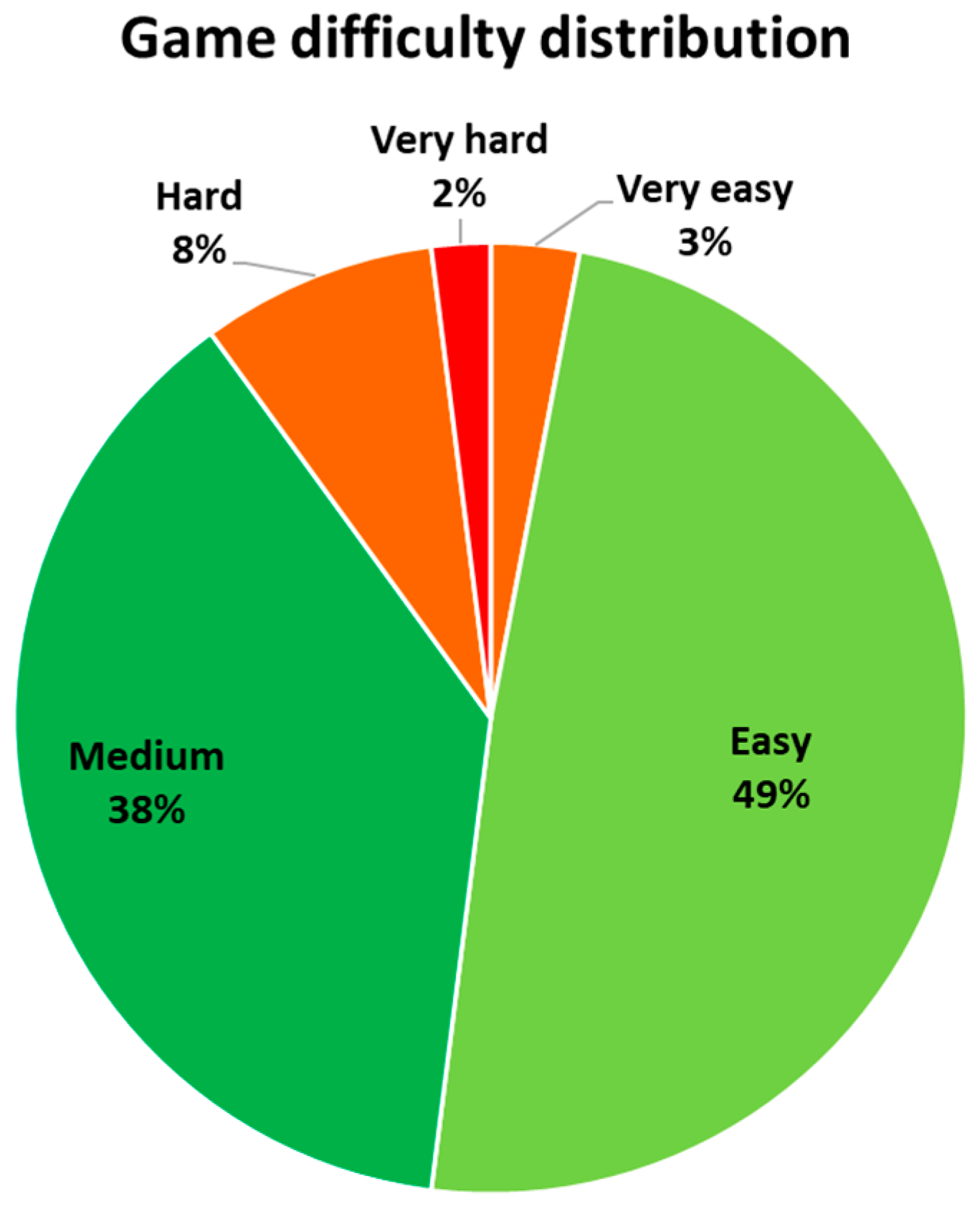
- Very easy: ≤30% of the time limit used to achieve the objective.
- Easy: 30–70% of the time limit used to achieve the objective.
- Medium: 70–100% of the time limit used; 70–100% of the objective achieved.
- Hard: time limit reached; 30–70% of the objective achieved.
- Very hard: time limit reached; ≤30% of the objective achieved.
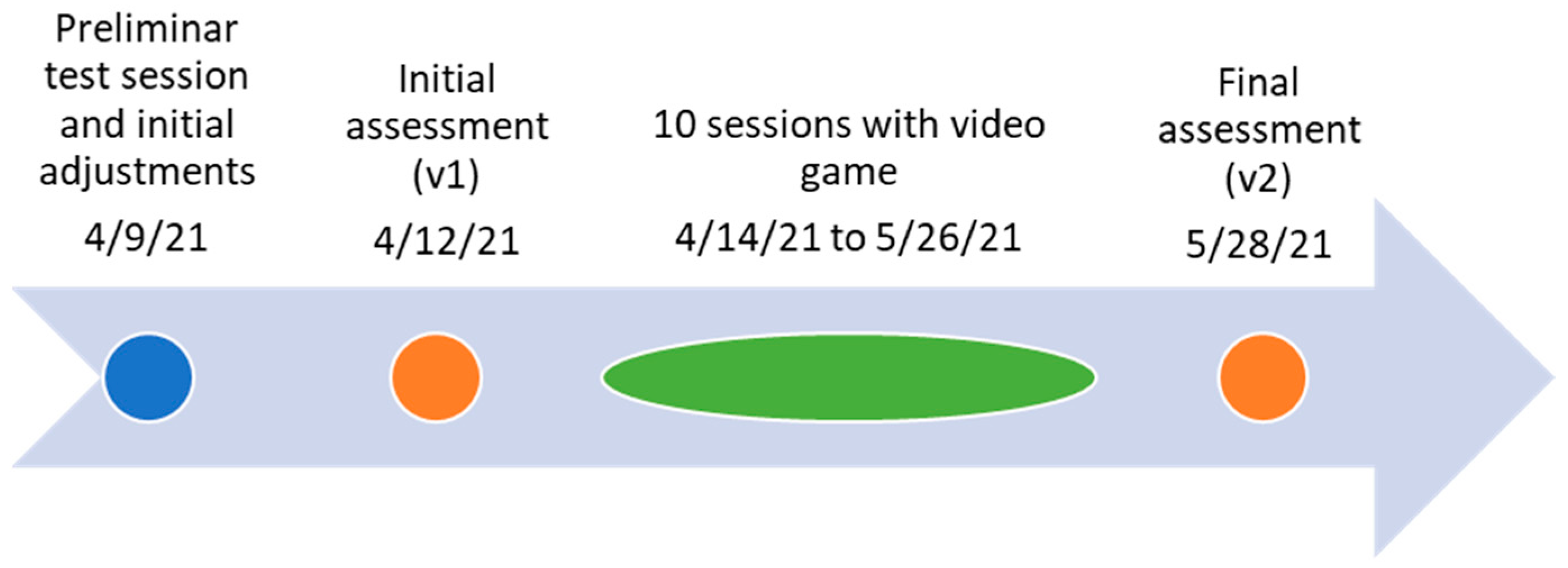
2.4. Therapeutic Intervention
- Chop: 20 logs of wood
- Climb: 60 m (=60 alternate arm movements)
- Row: 30 m (=30 symmetric arm movements)
- Dive: 1 plankton
2.5. Assessment
- Jebsen Taylor Hand Function Test (JTHFT): Improvement in this test is reflected by a decrease in the time used to complete each activity [33].
- Box and Block Test (BBT): Improvement is reflected in a greater number of blocks moved from one side of the box to the other [34].
- The strength of analytical movements of the affected limb’s (right arm) shoulder was measured using a Sauter model FA20 dynamometer.
- How tired do you feel?
- Is something hurting? Where? How much?
- How much did you enjoy the game today?
- Do you want to play again next week?
3. Results and Outcome
3.1. Influence of the Game Difficulty Parameters
3.2. Assessment Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Activity | v1 [s] | v2 [s] | v1–v2 [s] | Variation |
|---|---|---|---|---|
| Simulated feeding | 22.64 | 11.35 | 11.29 | 50% |
| Lifting light objects | 8.42 | 5.97 | 2.45 | 29% |
| Stack tokens | 9.74 | 7.32 | 2.42 | 25% |
| Lifting heavy objects | 11.26 | 8.5 | 2.76 | 25% |
| Turn pages | 11.37 | 8.8 | 2.57 | 23% |
| Writing | 80.0 | 69.96 | 10.04 | 13% |
| Lifting small objects | 9.35 | 9.1 | 0.25 | 3% |
4. Discussion
4.1. Influence of the Game Difficulty Parameters
4.2. Assessment Results
4.3. Strengths and Limitations
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galbiatti, J.A.; Cardoso, F.L.; Galbiatti, M.G.P. Obstetric Paralysis: Who Is to Blame? A Systematic Literature Review. Rev. Bras. Ortop. 2020, 55, 139–146. [Google Scholar] [CrossRef]
- Pérez, M.V.; Poblete, L.J.A. Mecanismos Patogénicos de la Parálisis Braquial Congénita. Rev. Chil. Obstet. Ginecol. 2010, 75, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Vaquero, G.; Ramos, A.; Martínez, J.C.; Valero, P.; Núñez Enamorado, N.; Simón de las Heras, R.; Camacho Salas, A. Parálisis braquial obstétrica: Incidencia, seguimiento evolutivo y factores pronósticos. Rev. Neurol. 2017, 65, 19. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.; Watt, J.; Olson, J.; Van Aerde, J. Perinatal Brachial Plexus Palsy. Paediatr. Child. Health 2006, 11, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Bahm, J.; Ocampo-Pavez, C.; Disselhorst-Klug, C.; Sellhaus, B.; Weis, J. Obstetric Brachial Plexus Palsy. Dtsch. Arztebl. Int. 2009, 106, 83–90. [Google Scholar] [CrossRef]
- Olofsson, P.N.; Chu, A.; McGrath, A.M. The Pathogenesis of Glenohumeral Deformity and Contracture Formation in Obstetric Brachial Plexus Palsy-A Review. J. Brachial Plex Peripher. Nerve Inj. 2019, 14, e24–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basit, H.; Ali, C.D.M.; Madhani, N.B. Erb Palsy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Pons, C.; Sheehan, F.T.; Im, H.S.; Brochard, S.; Alter, K.E. Shoulder Muscle Atrophy and Its Relation to Strength Loss in Obstetrical Brachial Plexus Palsy. Clin. Biomech. 2017, 48, 80–87. [Google Scholar] [CrossRef]
- Marrero Riverón, L.O.; Cabrera Viltres, N.; Rodríguez-Triana Orue, J.A.; Navarro González, A.; Castro Soto Del Valle, A.; Tarragona Reinoso, R.; Hernández Gutiérrez, R. Diagnóstico y Tratamiento de La Parálisis Braquial Obstétrica. Rev. Cuba. Ortop. Traumatol. 1998, 12, 28–39. [Google Scholar]
- Rodríguez Díaz, M.; Amigo Castañeda, P. Una Mirada a La Parálisis Braquial Obstétrica. Rev. Médica Electrónica 2011, 33, 509–522. [Google Scholar]
- Brochard, S.; Alter, K.; Damiano, D. Shoulder Strength Profiles in Children with and without Brachial PLEXUS PALSY. Muscle Nerve 2014, 50, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Frade, F.; Gómez-Salgado, J.; Jacobsohn, L.; Florindo-Silva, F. Rehabilitation of Neonatal Brachial Plexus Palsy: Integrative Literature Review. J. Clin. Med. 2019, 8, 980. [Google Scholar] [CrossRef] [Green Version]
- Palomo, R.; Sánchez, R. Physiotherapy applied to the upper extremity in 0 to 10-year-old children with obstetric brachial palsy: A systematic review. Rev. Neurol. 2020, 71, 29. [Google Scholar] [CrossRef]
- El-Shamy, S.; Alsharif, R. Effect of Virtual Reality versus Conventional Physiotherapy on Upper Extremity Function in Children with Obstetric Brachial Plexus Injury. J. Musculoskelet. Neuronal Interact. 2017, 17, 319–326. [Google Scholar] [PubMed]
- Karas, H.E.; Atıcı, E.; Aydın, G.; Demirsöz, M. The Effects of Virtual Reality on Upper Extremity in Patients with Obstetric Brachial Plexus Injury. J. Pediatric Neurol. 2022, 20, 028–036. [Google Scholar] [CrossRef]
- Chen, Y.; Fanchiang, H.D.; Howard, A. Effectiveness of Virtual Reality in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys. Ther. 2018, 98, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Johansen, T.; Strøm, V.; Simic, J.; Rike, P.-O. Effectiveness of Training with Motion-Controlled Commercial Video Games on Hand and Arm Function in Young People with Cerebral Palsy: A Systematic Review and Meta-Analysis. J. Rehabil. Med. 2019, 52, jrm00012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knippenberg, E.; Verbrugghe, J.; Lamers, I.; Palmaers, S.; Timmermans, A.; Spooren, A. Markerless Motion Capture Systems as Training Device in Neurological Rehabilitation: A Systematic Review of Their Use, Application, Target Population and Efficacy. J. Neuroeng. Rehabil. 2017, 14, 61. [Google Scholar] [CrossRef]
- Lopes, S.; Magalhães, P.; Pereira, A.; Martins, J.; Magalhães, C.; Chaleta, E.; Rosário, P. Games Used with Serious Purposes: A Systematic Review of Interventions in Patients with Cerebral Palsy. Front. Psychol 2018, 9, 1712. [Google Scholar] [CrossRef] [Green Version]
- Massetti, T.; da Silva, T.D.; Crocetta, T.B.; Guarnieri, R.; de Freitas, B.L.; Bianchi Lopes, P.; Watson, S.; Tonks, J.; de Mello Monteiro, C.B. The Clinical Utility of Virtual Reality in Neurorehabilitation: A Systematic Review. J. Cent. Nerv. Syst. Dis. 2018, 10, 1179573518813541. [Google Scholar] [CrossRef] [Green Version]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Eckert, M.; Gómez-Martinho, I.; Meneses, J.; Martínez, J.-F. New Approaches to Exciting Exergame-Experiences for People with Motor Function Impairments. Sensors 2017, 17, 354. [Google Scholar] [CrossRef] [Green Version]
- Eckert, M.; Aglio, A.; Martín-Ruiz, M.-L.; Osma-Ruiz, V. A New Architecture for Customizable Exergames: User Evaluation for Different Neuromuscular Disorders. Healthcare 2022, 10, 2115. [Google Scholar] [CrossRef]
- Eckert, M.; Domingo Soria, B.; Terroso Gil, N. Finding Effective Adjustment Levels for Upper Limb Exergames: Focus Group Study with Children with Physical Disabilities. JMIR Serious Games 2023, 11, e36110. [Google Scholar] [CrossRef]
- Sevick, M.; Eklund, E.; Mensch, A.; Foreman, M.; Standeven, J.; Engsberg, J. Using Free Internet Videogames in Upper Extremity Motor Training for Children with Cerebral Palsy. Behav. Sci. 2016, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Hung, J.-W.; Chang, Y.-J.; Chou, C.-X.; Wu, W.-C.; Howell, S.; Lu, W.-P. Developing a Suite of Motion-Controlled Games for Upper Extremity Training in Children with Cerebral Palsy: A Proof-of-Concept Study. Games Health J. 2018, 7, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.; Lewthwaite, R. Optimizing Performance through Intrinsic Motivation and Attention for Learning: The OPTIMAL Theory of Motor Learning. Psychon. Bull. Rev. 2016, 23, 1382–1414. [Google Scholar] [CrossRef] [PubMed]
- Radtka, S.; Hone, R.; Brown, C.; Mastick, J.; Melnick, M.E.; Dowling, G.A. Feasibility of Computer-Based Videogame Therapy for Children with Cerebral Palsy. Games Health J. 2013, 2, 222–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staiano, A.E.; Flynn, R. Therapeutic Uses of Active Videogames: A Systematic Review. Games Health J. 2014, 3, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siu, K.; Al-Harbi, S.; Clark, H.; Thabane, L.; Cheng, J.; Tarnopolsky, M.; Meaney, B.; Choong, K. Feasibility and Reliability of Muscle Strength Testing in Critically Ill Children. J. Pediatr. Intensive Care 2015, 4, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Al-Qattan, M.; El-Sayed, A. Obstetric Brachial Plexus Palsy: The Mallet Grading System for Shoulder Function—Revisited. BioMed Res. Int. 2014, 2014, 398121. [Google Scholar] [CrossRef] [Green Version]
- Eckert, M.; Gomez-Martinho, I.; Esteban, C.; Peláez, Y.; Jiménez, M.; Martín-Ruiz, M.-L.; Manzano, M.; Aglio, A.; Osma, V.; Meneses, J.; et al. The Blexer System—Adaptive Full Play Therapeutic Exergames with Web-Based Supervision for People with Motor Dysfunctionalities. EAI Endorsed Trans. Game-Based Learn. 2018, 5, 155085. [Google Scholar] [CrossRef]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; Howard, L.A. An Objective and Standardized Test of Hand Function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar] [PubMed]
- Mulcahey, M.J.; Kozin, S.; Merenda, L.; Gaughan, J.; Tian, F.; Gogola, G.; James, M.A.; Ni, P. Evaluation of the Box and Blocks Test, Stereognosis and Item Banks of Activity and Upper Extremity Function in Youths with Brachial Plexus Birth Palsy. J. Pediatr. Orthop. 2012, 32 (Suppl. 2), S114–S122. [Google Scholar] [CrossRef]
- Horne-Moyer, H.L.; Moyer, B.H.; Messer, D.C.; Messer, E.C. The Use of Electronic Games in Therapy: A Review with Clinical Implications. Curr. Psychiatry Rep. 2014, 16, 520. [Google Scholar] [CrossRef] [Green Version]
- Zayeni, D.; Raynaud, J.P.; Revet, A. Therapeutic and Preventive Use of Video Games in Child and Adolescent Psychiatry: A Systematic Review. Front. Psychiatry 2020, 11, 36. [Google Scholar] [CrossRef]
- Granic, I.; Lobel, A.; Engels, R.C. The benefits of playing video games. Am. Psychol. 2014, 69, 66–78. [Google Scholar] [CrossRef] [PubMed]





| Activity | v1 [n. Blocks] | v2 [n. Blocks] | v1–v2 [n. Blocks] | Variation |
|---|---|---|---|---|
| Move blocks | 40 | 40 | 0 | 0% |
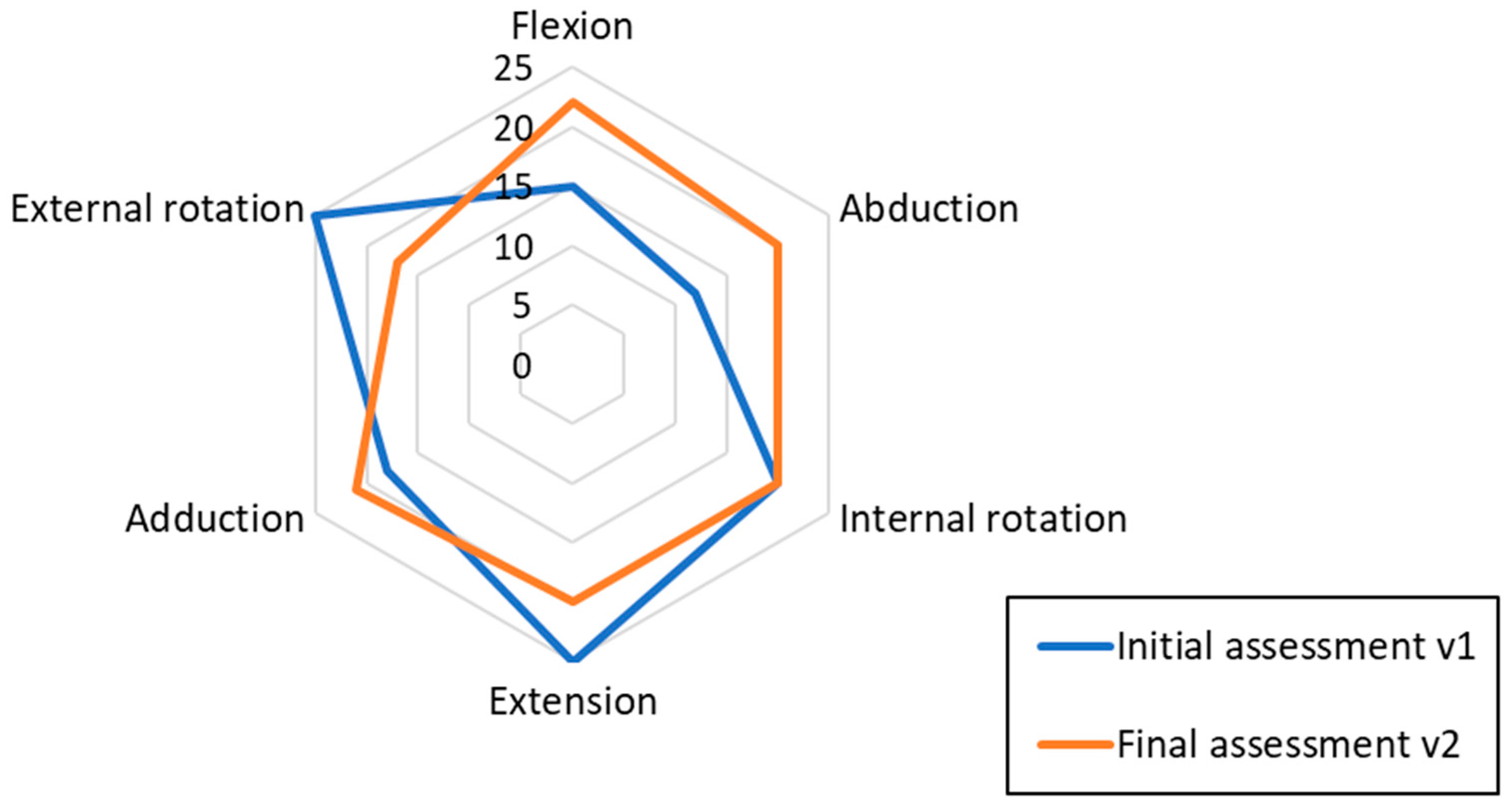
| Movement | v1 [N] | v2 [N] | v1–v2 [N] | Variation |
|---|---|---|---|---|
| Abduction | 12 | 20 | 8 | 67% |
| Adduction | 18 | 21 | 3 | 17% |
| Flexion | 15 | 22 | 7 | 47% |
| Extension | 25 | 20 | −5 | −20% |
| Internal rotation | 20 | 20 | 0 | 0% |
| External rotation | 25 | 17 | −8 | −32% |
| Mean (SD) | 19.17 (5.27) | 20 (1.67) | 0.83 (6.43) | 13% (38%) |
| Date | Fatigue (1–10) | Motivation (1–5) | Play Again? | How Much Pain? (0–10) | Pain Where? 1 |
|---|---|---|---|---|---|
| 9 April 2021 | 2 | 5 | yes | 2 | right abdomen |
| 14 April 2021 | 2 | 5 | yes | 4 | left abdomen |
| 21 April 2021 | 2 | 5 | yes | 4 | abdominals |
| 23 April 2021 | 3 | 5 | yes | 1 | arm-shoulder |
| 27 April 2021 | 5 | 5 | yes | 6 | left rib |
| 30 April 2021 | 4 | 5 | yes | 1 | left rib |
| 7 May 2021 | 1 | 5 | yes | 1 | right arm |
| 12 May 2021 | 1 | 5 | yes | 4 | left arm |
| 14 May 2021 | 2 | 5 | yes | 1 | abdominals |
| 19 May 2021 | 0 | 5 | yes | 2 | ribs |
| Mean | 2.2 | 5 | 2.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domingo, B.; Terroso, N.; Eckert, M. Personalized Use of an Adjustable Movement-Controlled Video Game in Obstetric Brachial Plexus Palsy during Physiotherapy Sessions at School: A Case Report. Healthcare 2023, 11, 2008. https://doi.org/10.3390/healthcare11142008
Domingo B, Terroso N, Eckert M. Personalized Use of an Adjustable Movement-Controlled Video Game in Obstetric Brachial Plexus Palsy during Physiotherapy Sessions at School: A Case Report. Healthcare. 2023; 11(14):2008. https://doi.org/10.3390/healthcare11142008
Chicago/Turabian StyleDomingo, Beatriz, Noelia Terroso, and Martina Eckert. 2023. "Personalized Use of an Adjustable Movement-Controlled Video Game in Obstetric Brachial Plexus Palsy during Physiotherapy Sessions at School: A Case Report" Healthcare 11, no. 14: 2008. https://doi.org/10.3390/healthcare11142008