
Mobile Health Interventions to Improve Health Behaviors and Healthcare Services among Vietnamese Individuals: A Systematic Review
Abstract
:1. Introduction
2. Materials and Methods
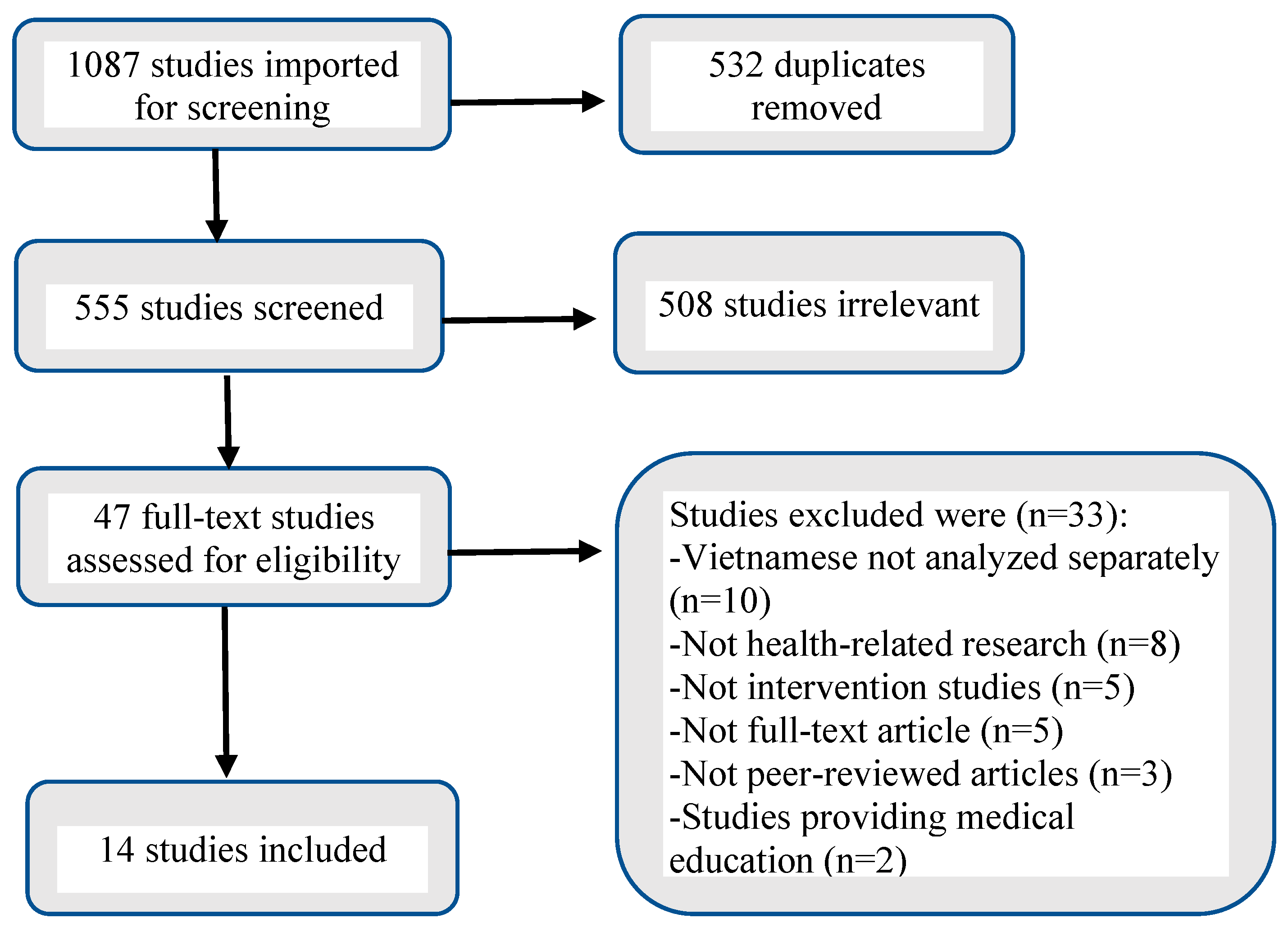
2.1. Data Sources and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Data Synthesis
3. Results
3.1. Study Characteristics and Quality

{kind=link}
| Author (Year) | Study Design (Participants) | Device—mHealth Intervention | Study Outcomes | Findings | ||
|---|---|---|---|---|---|---|
| Feasibility | Acceptability | Efficacy | ||||
| McBride, B. et al. (2018) [8] | Qualitative—document review; observations; focus group discussions; in-depth interviews (n = 60) | Mobile phone— SMS | Improve access to maternal, newborn, and child health services and health equity utilizing mHealth intervention. | Not measured. | Participants reported satisfaction with SMS and willingness to pay a fee for service. | Increased knowledge, effective behavior change, communication, husband involvement, and strengthened relationships between participants and community health workers. |
| Vu, L. T. H. et al. (2016) [9] | Prospective cohort (mixed methods) (n = 411 for baseline survey; n = 482 for post-intervention survey) | Telephone— Hotline, SMS, and map of health services providers | Impact of the 12-month mHealth intervention on changes in knowledge and practices related to sexual and reproductive health among female migrants. | Ability to recruit and retain 411 participants with various backgrounds and demographics. | Participants rated SMS service as useful (64.9%, n = 288) and very useful (20.3%, n = 90). | Women’s knowledge of sexual and reproductive health increased by 70.3%, and sexual and reproductive health practices were improved by 85.5%. |
| Nguyen, N. T. et al. (2017) [10] | Prospective cohort (pre- and post- uncontrolled study) (n = 11,449) | Mobile phone— SMS | Impact of SMS reminders to improve the immunization program by increasing vaccination rate. | SMS reminders have been shown to improve immunization coverage and timeliness of vaccination. | 93.3% (111/120) of interviewees were willing to pay for SMS reminders for immunization schedule. | Immunization rate of children under one year old increased significantly from 75.4% in 2013 to 81.7% in 2014 and to 99.2% in 2015. |
| Ngo, C. Q. et al. (2019) [11] | Randomized, cross-sectional study (n = 469) | Telephone—SMS, phone calls/counseling | Impact of national telephone counselling for smoking cessation (self-report quit rate at baseline, 7-day, and 6-month abstinence) and factors associated with the Quitline use. | Response rate of 28.4% (469/1648) after excluding callers who did not set counseling appointments. | 88.5% of participants were satisfied with program. Satisfaction and engagement were factors associated with increased Quitline use. | Most participants felt more confident about quitting (74.3%) and took early action via their first quit attempt (81.7%); 18.3% reported more than 7-day abstinence period. |
| Jiang, N. et al. (2021) [12] | RCT (2 arms) (n = 100) | Mobile phone— SMS | Feasibility, acceptability, and preliminary efficacy of a fully automated bidirectional SMS smoking cessation 6-week intervention. | Recruitment rate of 99% (100/101) enrolled in program and completed 12-week follow-up survey. In-depth interviews were also conducted to evaluate feasibility. | 98% of participants in the intervention arm reported being satisfied with the program versus 82% in the control arm. | Biochemically verified abstinence was higher in the intervention arm at 6 weeks (20% vs. 2%), but the effect was not significant at 12 weeks (12% vs. 6%). |
| Nguyen, T.A. et al. (2017) [13] | Prospective cohort (uncontrolled feasibility study) (n = 40) | Smartphone—SMS, participants record themselves taking treatment and upload video to online server | Feasibility of using asynchronous Video Directly Observed Therapy (VDOT) to support treatment adherence among patients with pulmonary tuberculosis for 12 months. | 51% (40/78) participated and rated the VDOT as feasible and interface highly, despite facing some initial technical difficulties. | 87.5% (n = 35) found that VDOT was easy to use and stated they would recommend this service to others. | 71.1% (n = 27) of participants took all required doses. A median of 88.4% of doses were correctly recorded and uploaded. 85% (n = 34) of participants missed <4 video uploads during the follow-up period. |
| Tran, B. X. & Houston, S. (2012) [14] | Cross-sectional survey (n = 1016) | Mobile phone— SMS, direct phone calls, and automatic voice calls | Feasibility of using mobile phone to support antiretroviral treatment adherence for patients with HIV/AIDS. | Expressed preferences for SMS (41.8%), direct calls (35.4%), direct counseling (43.1%), automated pill taking reminders (29.1%), regular information messages (21.3%), and clinic visits booking (16.5%). | 63.5% of participants were willing to use services and willing to pay a fee for SMS adherence support service. | Majority of participants (78.6%) considered using mobile phone could be an effective adherence support. |
| Imamura, K. et al. (2021) [15] | Randomized controlled trial (RCT) (3 arms) (n = 951) | Smartphone—Smartphone application | Effect of a 10-week smartphone-based internet cognitive behavioral therapy stress management program to improve depression and anxiety among nurses. | Recruitment rate of 75.8% (962/1269) participated in baseline survey; 90% completed 7-month follow up for all 3 groups. | Completion rates (84%), satisfaction (>82%), and usefulness (>80%) in both intervention groups. | Depression and anxiety average scores decreased at 3 months from baseline but increased again at 7 months from baseline in both intervention groups. |
| Huang, W.-C. et al. (2022) [16] | Prospective cohort (uncontrolled feasibility single-arm study) (n = 221) | Mobile phone— Telephone calls, short message service (SMS) | Feasibility of a 12-month smoking cessation intervention that integrates follow-up counseling phone calls and scheduled text messages with brief advice from physicians. | Of 431 who were eligible, 221 (51.3%) agreed to participate in program. | 141 (63.8%) participated in all 4 phone calls; 117 (52.9%) participated in all 8 phone calls in first 30 days. | 90 (40.7%) self-reported abstinence from smoking in previous 30 days. Overall, 5.9% of all participants achieved verified smoking cessation for more than 30 days 12 months after enrollment. |
| Tran, B. X. et al. (2018) [17] | Cross-sectional study (n = 429) | Smartphone— application for vaccination management | Efficacy, adoption, and feasibility of implementing an mHealth application to educate and deliver information about vaccination and immunization. | Ability to recruit 429 participants with different levels of socio-demographic background. | Participants reported willingness to use (90.1%) and willingness to pay for the app 79.1%). | 69.6% of participants believed that the app was necessary. Those who thought the app was unnecessary also felt there was sufficient vaccination information available online. |
| Khanh, T. Q. et al. (2020) [18] | Prospective cohort (uncontrolled pilot single-arm study) (n = 279) | Smartphone— Mobile app, SMS | Improve glycemic control and user satisfaction of incorporating a 12-week digital diabetes care system that monitor patient data and adjust therapy through digital contact. | Recruitment rate of 93% (279/300) participation. At week 12 and during the 20-day follow-up period, 81% remained engaged with the system and maintained glucose monitoring. | Both patients and healthcare professionals completed questionnaires at the final visit and reported overall satisfaction with system. | 79% of participants had decreased average glucose levels, 36.9% of participants had decreased fasting glucose in first 2 weeks and last 2 weeks, and 45% of participants had HbA1c decreased from baseline at 12-week follow up. |
| Nguyet, T.T. et al. (2021) [19] | Quasi-experimental with a nonequivalent control group design (n = 52) | Smartphone, tablet, personal computers—SMS, viewings of educational content | Effect of a 4-week newborn care education program on breastfeeding rate and maternal role confidence of first-time mothers. | 69% (70/101) agreed to participate with an attrition rate of 72% in the control group and 78% in the experimental group. | Not measured | At 4 weeks postpartum, the experimental group showed a significantly higher level of breastfeeding rate (p < 0.05) and mean maternal role confidence (p < 0.05) than the control group. |
| Ngoc, N. T. N. et al. (2014) [20] | RCT (n = 1433) | Telephone— Phone follow-up calls | Feasibility, acceptability, and efficacy of a service delivery protocol that replaces the routine clinic visit after medical abortion. | Phone follow-up offers a feasible approach to review pregnancy test result and checklist responses with the participants. | Most participants (88.3% [606/686]) indicated preference to have phone call follow-up from a healthcare provider. | Phone call follow-ups enable 85% of women to avoid a routine clinic visit without any decrease in safety. |
| Shapiro, L. M. et al. (2021) [21] | Prospective cluster (uncontrolled feasibility pilot study) (n = 8) | Mobile phone— SMS reminders and follow-up data collection | Feasibility of a 12-week SMS follow-up to obtain patient-reported outcome measures after hand surgery. | 100% (8/8) were eligible and agreed to participate with 100% attrition. | Majority (>75%) of patients completed follow-up questionnaires at all data collection points. | SMS may serve as an effective method for follow-up to ensure safety and quality healthcare in low-resource settings. |
3.2. Feasibility of mHealth Interventions
3.3. Acceptability of mHealth Interventions
3.4. Efficacy of mHealth Interventions
4. Discussion
Strengths and Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Telecommunication Union. ICT Facts and Figures; International Telecommunication Union: Geneva, Switzerland, 2020. [Google Scholar]
- MHealth Use of Appropriate Digital Technologies for Public Health Report by the Director-General; 2018. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_20-en.pdf (accessed on 9 February 2023).
- WHO Guideline Recommendations on Digital Interventions for Health System Strengthening. Available online: http://apps.who.int/iris/bitstream/handle/10665/311941/9789241550505-eng.pdf (accessed on 9 February 2023).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Medical Devices and eHealth Solutions: Compendium of Innovative Health Technologies for Low-Resource Settings 2011–2012; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McBride, B.; O’Neil, J.D.; Hue, T.T.; Eni, R.; Nguyen, C.V.; Nguyen, L.T. Improving health equity for ethnic minority women in Thai Nguyen, Vietnam: Qualitative results from an mHealth intervention targeting maternal and infant health service access. J. Public Health 2018, 40 (Suppl. S2), ii32–ii41. [Google Scholar] [CrossRef] [PubMed]
- Vu, L.T.H.; Nguyen, N.T.K.; Tran, H.T.D.; Muhajarine, N. mHealth information for migrants: An e-health intervention for internal migrants in Vietnam. Reprod Health 2016, 13, 55. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Vu, H.M.; Dao, S.D.; Tran, H.T.; Nguyen, T.X.C. Digital immunization registry: Evidence for the impact of mHealth on enhancing the immunization system and improving immunization coverage for children under one year old in Vietnam. mHealth 2017, 3, 26. [Google Scholar] [CrossRef]
- Ngo, C.Q.; Phan, P.T.; Van Vu, G.; Le Pham, Q.T.; Chu, H.T.; Pham, K.T.H.; Tran, B.X.; Do, H.P.; Nguyen, C.T.; Tran, T.T.; et al. Impact of a smoking cessation quitline in Vietnam: Evidence base and future directions. Int. J. Environ. Res. Public Health 2019, 16, 2538. [Google Scholar] [CrossRef]
- Jiang, N.; Nguyen, N.; Siman, N.; Cleland, C.M.; Nguyen, T.; Doan, H.T.; Abroms, L.C.; Shelley, D.R. Adaptation and assessment of a text messaging smoking cessation intervention in Vietnam: Pilot randomized controlled trial. JMIR mHealth uHealth 2021, 9, e27478. [Google Scholar] [CrossRef]
- Nguyen, T.A.; Pham, M.T.; Nguyen, T.L.; Nguyen, V.N.; Pham, D.C.; Nguyen, B.H.; Fox, G.J. Video directly observed therapy to support adherence with treatment for tuberculosis in Vietnam: A prospective cohort study. Int. J. Infect. Dis. 2017, 65, 85–89. [Google Scholar] [CrossRef]
- Tran, B.X.; Houston, S. Mobile phone-based antiretroviral adherence support in Vietnam: Feasibility, patient’s preference, and willingness-to-pay. AIDS Behav. 2012, 16, 1988–1992. [Google Scholar] [CrossRef]
- Imamura, K.; Tran, T.T.T.; Nguyen, H.T.; Sasaki, N.; Kuribayashi, K.; Sakuraya, A.; Bui, T.M.; Nguyen, A.Q.; Nguyen, Q.T.; Nguyen, N.T.; et al. Effect of smartphone-based stress management programs on depression and anxiety of hospital nurses in Vietnam: A three-arm randomized controlled trial. Sci. Rep. 2021, 11, 11353. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.-C.; Marks, G.B.; Pham, N.Y.; Nguyen, T.A.; Vu, V.G.; Nguyen, V.N.; Jan, S.; Negin, J.; Ngo, Q.C.; Fox, G.J. A smoking quitline integrated with clinician counselling at outpatient health facilities in Vietnam: A single-arm prospective cohort study. BMC Public Health 2022, 22, 739. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.X.; Nguyen, Q.N.; Dang, A.K.; Vu, G.T.; Hoang, V.Q.; La, P.V.; Hoang, D.A.; Van Dam, N.; Vuong, T.T.; Nguyen, L.H.; et al. Acceptability of and willingness to pay for using a smartphone-based vaccination application in a Vietnamese cohort. Patient Prefer. Adherence 2018, 12, 2583–2591. [Google Scholar] [CrossRef]
- Khanh, T.Q.; Hao, P.N.; Roitman, E.; Raz, I.; Marganitt, B.; Cahn, A. Digital diabetes care system observations from a pilot evaluation study in Vietnam. Int. J. Environ. Res. Public Health 2020, 17, 937. [Google Scholar] [CrossRef]
- Nguyet, T.T.; Huy, N.V.Q.; Kim, Y. Effects of a newborn care education program using ubiquitous learning on exclusive breastfeeding and maternal role confidence of first-time mothers in Vietnam: A quasi-experimental study. Korean J. Women Health Nurs. 2021, 27, 278–285. [Google Scholar] [CrossRef]
- Ngoc, N.T.N.; Bracken, H.; Blum, J.; Nga, N.T.B.; Minh, N.H.; Van Nhang, N.; Lynd, K.; Winikoff, B.; Blumenthal, P.D. Acceptability and feasibility of phone follow-up after early medical abortion in Vietnam. Obstet. Gynecol. 2014, 123, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, L.M.; Đình, M.P.; Tran, L.; Fox, P.M.; Richard, M.J.; Kamal, R.N. Short message service-based collection of patient-reported outcome measures on hand surgery global outreach trips: A pilot feasibility study. J. Hand Surg. 2022, 47, 384.e1–384.e5. [Google Scholar] [CrossRef]
- Heijmans, M.; Waverijn, G.; Rademakers, J.; van der Vaart, R.; Rijken, M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ. Couns. 2015, 98, 41–48. [Google Scholar] [CrossRef]
- Carroll, A.E.; DiMeglio, L.A.; Stein, S.; Marrero, D.G. Using a cell phone-based glucose monitoring system for adolescent diabetes management. Diabetes Educ. 2010, 37, 59–66. [Google Scholar] [CrossRef]
- Franklin, V.L.; Greene, A.; Waller, A.; Greene, S.A.; Pagliari, C. Patients’ engagement with “Sweet Talk”—A text messaging support system for young people with diabetes. J. Med. Internet Res. 2008, 10, e20. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The impact of mHealth interventions: Systematic review of systematic reviews. JMIR mHealth uHealth 2018, 6, e23. [Google Scholar] [CrossRef] [PubMed]
- Mulvaney, S.A.; Anders, S.; Smith, A.K.; Pittel, E.J.; Johnson, K.B. A pilot test of a tailored mobile and web-based diabetes messaging system for adolescents. J. Telemed. Telecare 2012, 18, 115–118. [Google Scholar] [CrossRef]
- Mcgregor, S.L.T. Understanding and Evaluating Research: A Critical Guide; Sage: Los Angeles, CA, USA; London, UK; New Delhi, India, 2018. [Google Scholar]
- Venkatesh, V.; Davis, F.D. A model of the antecedents of perceived ease of use: Development and test. Decis. Sci. 1996, 27, 451–481. [Google Scholar] [CrossRef]
- Morris, M.G.; Venkatesh, V. Age differences in technology adoption decisions: Implications for a changing work force. Pers. Psychol. 2000, 53, 375–403. [Google Scholar] [CrossRef]
- Mohr, D.C.; Cuijpers, P.; Lehman, K. Supportive accountability: A model for providing human support to enhance adherence to eHealth interventions. J. Med. Internet Res. 2011, 13, e30. [Google Scholar] [CrossRef] [PubMed]
- Mohr, D.C.; Schueller, S.M.; Montague, E.; Burns, M.N.; Rashidi, P. The behavioral intervention technology model: An integrated conceptual and technological framework for eHealth and mHealth interventions. J. Med. Internet Res. 2014, 16, e3077. [Google Scholar] [CrossRef]
- Shariful, I.M. Theories applied to m-health interventions for behavior change in low-and middle-income countries: A systematic review. Telemed. e-Health 2018, 24, 727–741. [Google Scholar]
- DeLanda, M. A New Philosophy of Society: Assemblage Theory and Social Complexity; Bloomsbury Publishing: London, UK, 2019. [Google Scholar]
- Schneider-Kamp, A.; Fersch, B. Detached co-involvement in interactional care: Transcending temporality and spatiality through mHealth in a social psychiatry out-patient setting. Soc. Sci. Med. 2021, 285, 114297. [Google Scholar] [CrossRef]
- Berker, T.; Hartmann, M.; Punie, Y. Domestication of Media and Technology; McGraw-Hill Education (UK): London, UK, 2005. [Google Scholar]
- Hou, C.; Xu, Q.; Diao, S.; Hewitt, J.; Li, J.; Carter, B. Mobile phone applications and self-management of diabetes: A systematic review with meta-analysis, meta-regression of 21 randomized trials and GRADE. Diabetes Obes. Metab. 2018, 20, 2009–2013. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B.; Oetzel, J.G.; Minkler, M. Community-Based Participatory Research for Health: Advancing Social and Health Equity; Jossey-Bass, A Wiley Brand: San Francisco CA, USA, 2018. [Google Scholar]
- Han, M.; Lee, E. Effectiveness of mobile health application use to improve health behavior changes: A systematic review of randomized controlled trials. Healthc. Inform. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef]
- Abasi, S.; Yazdani, A.; Kiani, S.; Mahmoudzadeh-Sagheb, Z. Effectiveness of mobile health-based self-management application for posttransplant cares: A systematic review. Health Sci. Rep. 2021, 4, e434. [Google Scholar] [CrossRef] [PubMed]
- Buck, C.; Keweloh, C.; Bouras, A.; Simoes, E.J. Efficacy of short message service text messaging interventions for postoperative pain management: Systematic review. JMIR mHealth uHealth 2021, 9, e20199. [Google Scholar] [CrossRef] [PubMed]
- Wickersham, A.; Petrides, P.M.; Williamson, V.; Leightley, D. Efficacy of mobile application interventions for the treatment of post-traumatic stress disorder: A systematic review. Digit. Health 2019, 5, 2055207619842986. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, H.E.; Santos, G.N.; Ferreira Leite, A.; Mesquita, C.R.; de Souza Figueiredo, P.T.; Miron Stefani, C.; de Santos Melo, N. The feasibility of telehealth in the monitoring of head and neck cancer patients: A systematic review on remote technology, user adherence, user satisfaction, and quality of life. Support. Care Cancer 2022, 30, 8391–8404. [Google Scholar] [CrossRef]
- Grist, R.; Porter, J.; Stallard, P. Mental health mobile apps for preadolescents and adolescents: A systematic review. J. Med. Internet Res. 2017, 19, e176. [Google Scholar] [CrossRef]

| Confounding Bias | Selection Bias | Intervention Classification Bias | Deviation in Intervention Bias | Missing Data Bias | Measurement Bias | Selection of Reported Results Bias | Overall Rating | ||
| Nguyen, N.T. et al. (2017) [10] | Green = Low risk of bias Orange = Moderate risk Red = Serious risk Blue = Critical risk Gray = No information | ||||||||
| Ngo, C.Q. et al. (2019) [11] | |||||||||
| Nguyen, T.A. et al. (2017) [13] | |||||||||
| Tran, B.X. & Houston, S. (2012) [14] | |||||||||
| Huang, W-C. et al. (2022) [16] | |||||||||
| Tran, B.X. et al. (2018) [17] | |||||||||
| Khanh, T.Q. et al. (2020) [18] | |||||||||
| Nguyet, T.T. et al. (2021) [19] | |||||||||
| Shapiro, L.M. et al. (2021) [21] |
| Randomization Process Bias | Deviation in Intervention Bias | Missing Data Bias | Measurement Bias | Selection of Reported Results Bias | Overall Rating | ||
| Jiang, N. et al. (2021) [12] | Green = Low risk of bias Orange = Some concerns Red = High risk | ||||||
| Imamura, K. et al. (2021) [15] | |||||||
| Ngoc, N.T.N. et al. (2014) [20] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, A.; Eschiti, V.; Bui, T.C.; Nagykaldi, Z.; Dwyer, K. Mobile Health Interventions to Improve Health Behaviors and Healthcare Services among Vietnamese Individuals: A Systematic Review. Healthcare 2023, 11, 1225. https://doi.org/10.3390/healthcare11091225
Nguyen A, Eschiti V, Bui TC, Nagykaldi Z, Dwyer K. Mobile Health Interventions to Improve Health Behaviors and Healthcare Services among Vietnamese Individuals: A Systematic Review. Healthcare. 2023; 11(9):1225. https://doi.org/10.3390/healthcare11091225
Chicago/Turabian StyleNguyen, Anna, Valerie Eschiti, Thanh C. Bui, Zsolt Nagykaldi, and Kathleen Dwyer. 2023. "Mobile Health Interventions to Improve Health Behaviors and Healthcare Services among Vietnamese Individuals: A Systematic Review" Healthcare 11, no. 9: 1225. https://doi.org/10.3390/healthcare11091225