Association between Risk Communication Format and Perceived Risk of Adverse Events after COVID-19 Vaccination among US Adults

 , ,
, ,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
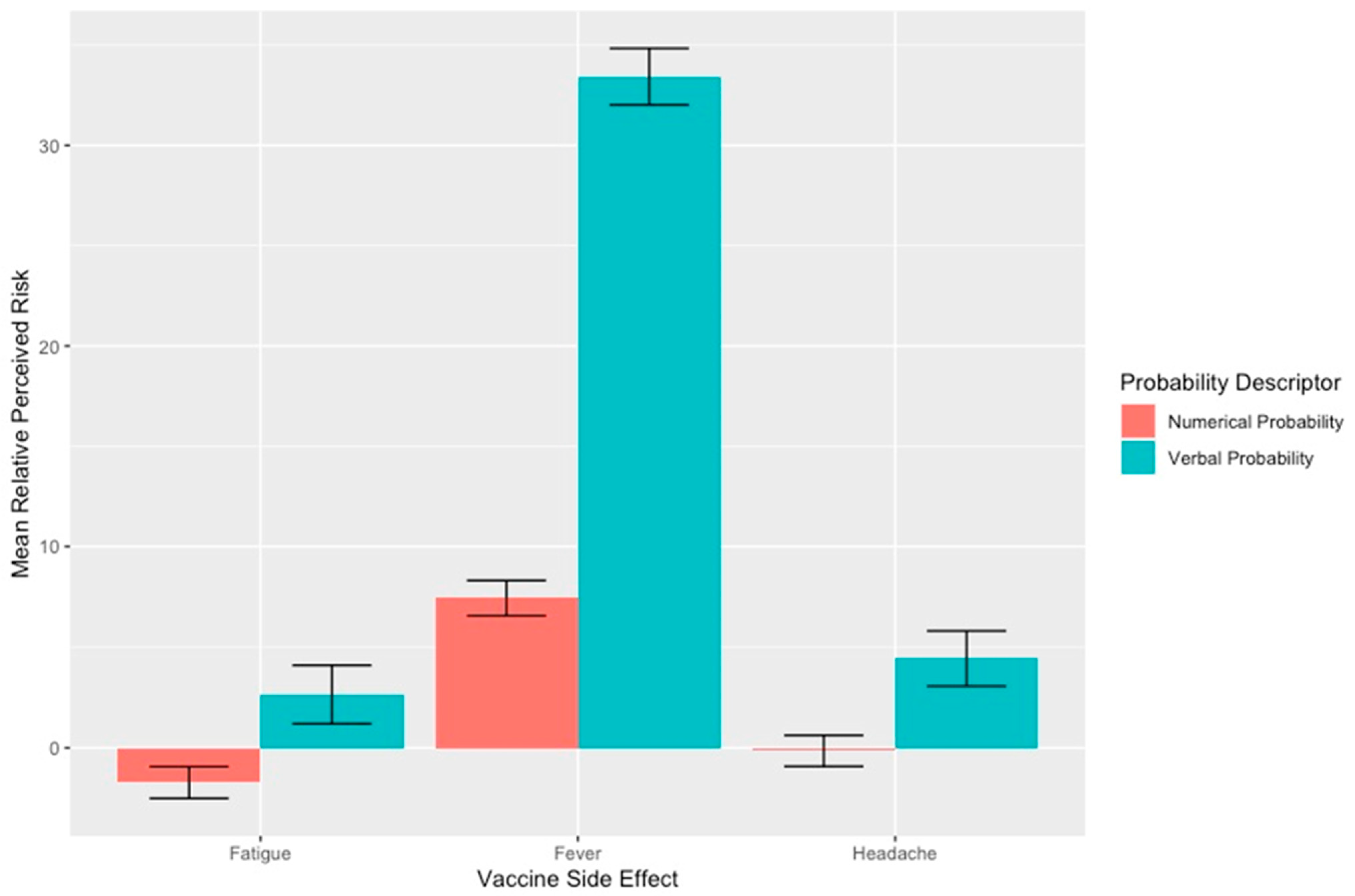
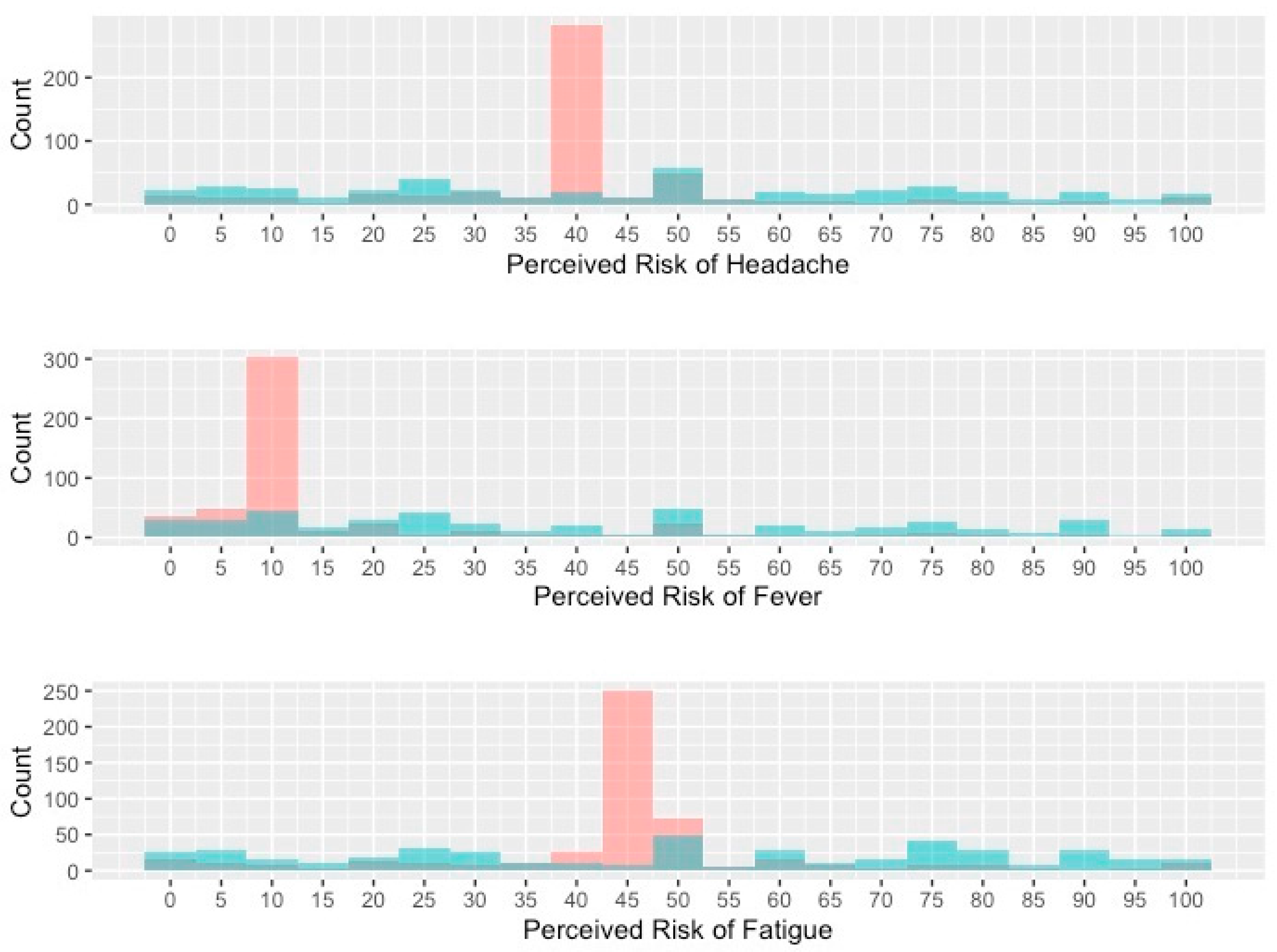
3.1. Headache, Fever and Fatigue
3.2. Myocarditis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center for Disease Control and Prevention. Safety of COVID-19 Vaccines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/safety-of-vaccines.html (accessed on 31 October 2021).
- Barchielli, B.; Cricenti, C.; Gallè, F.; Sabella, E.A.; Liguori, F.; Molin, G.D.; Liguori, G.; Orsi, G.B.; Giannini, A.M.; Ferracuti, S.; et al. Climate Changes, Natural Resources Depletion, COVID-19 Pandemic, and Russian-Ukrainian War: What Is the Impact on Habits Change and Mental Health? Int. J. Environ. Res. Public Health 2022, 19, 11929. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, K.; Chan, E.; Park, M.; Benda, N.C.; Sharma, M.M.; Demetres, M.; Delgado, D.; Sigworth, E.; Chen, Q.; Liu, A.; et al. Imprecision and Preferences in Interpretation of Verbal Probabilities in Health: A Systematic Review. J. Gen. Intern. Med. 2021, 36, 3820–3829. [Google Scholar] [CrossRef] [PubMed]
- Rosen, J.E.; Agrawal, N.; Flum, D.R.; Liao, J.M. Verbal Descriptions of the Probability of Treatment Complications Lead to High Variability in Risk Perceptions: A Survey Study. Ann. Surg. 2021; Publish Ahead of Print. [Google Scholar]
- Mitchell, A.; Liedke, J. About Four-in-Ten Americans Say Social Media Is an Important Way of Following COVID-19 Vaccine News. Available online: https://www.pewresearch.org/fact-tank/2021/08/24/about-four-in-ten-americans-say-social-media-is-an-important-way-of-following-covid-19-vaccine-news/ (accessed on 1 April 2022).
- Wilson, S.L.; Wiysonge, C. Social Media and Vaccine Hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.C.; Hochhauser, M. Verbal Labels Can Triple Perceived Risk in Clinical Trials. Drug Inf. J. 2006, 40, 249–258. [Google Scholar] [CrossRef]
- Berry, D.C.; Raynor, D.K.; Knapp, P.; Bersellini, E. Patients’ Understanding of Risk Associated with Medication Use. Drug Saf. 2003, 26, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.; Rosenzweig, C.; Moss, A.J.; Litman, L. Tapped out or Barely Tapped? Recommendations for How to Harness the Vast and Largely Unused Potential of the Mechanical Turk Participant Pool. PLoS ONE 2019, 14, e0226394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, K.; Hughes, T.L. Comparing Amazon’s Mechanical Turk Platform to Conventional Data Collection Methods in the Health and Medical Research Literature. J. Gen. Intern. Med. 2018, 33, 533–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 18 May 2021).
- Bonner, C.; Trevena, L.J.; Gaissmaier, W.; Han, P.K.J.; Okan, Y.; Ozanne, E.; Peters, E.; Timmermans, D.; Zikmund-Fisher, B.J. Current Best Practice for Presenting Probabilities in Patient Decision Aids: Fundamental Principles. Med. Decis. Mak. 2020, 41, 821–833. [Google Scholar] [CrossRef] [PubMed]
- Windschitl, P.D.; Weber, E.U. The Interpretation of “Likely” Depends on the Context, but “70%” Is 70%—Right? The Influence of Associative Processes on Perceived Certainty. J. Exp. Psychol. Learn. Mem. Cogn. 1999, 25, 1514–1533. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Jungermann, H. Rarely Occurring Headaches and Rarely Occurring Blindness: Is Rarely = Rarely? The Meaning of Verbal Frequentistic Labels in Specific Medical Contexts. J. Behav. Decis. Mak. 1996, 9, 153–172. [Google Scholar] [CrossRef]
- Merz, J.F.; Druzdzel, M.J.; Mazur, D.J. Verbal Expressions of Probability in Informed Consent Litigation. Med. Decis. Mak. 1991, 11, 273–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, M.D.; Duffy, A.; Neill, K. The Numerical Translation of Verbal Probability Expressions by Patients and Clinicians in the Context of Peri-operative Risk Communication. Anaesthesia 2020, 75, e39–e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skafle, I.; Nordahl-Hansen, A.; Quintana, D.S.; Wynn, R.; Gabarron, E. Misinformation about COVID-19 Vaccines on Social Media: Rapid Review. J. Med. Internet Res. 2022, 24, e37367. [Google Scholar] [CrossRef] [PubMed]
- McCredie, M.N.; Morey, L.C. Who Are the Turkers? A Characterization of MTurk Workers Using the Personality Assessment Inventory. Assessment 2019, 26, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Walters, K.; Christakis, D.A.; Wright, D.R. Are Mechanical Turk Worker Samples Representative of Health Status and Health Behaviors in the U.S.? PLoS ONE 2018, 13, e0198835. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Level | Numerical Probability | Verbal Probability |
|---|---|---|---|
| n = 495 | n = 444 | ||
| Gender Identity, No. (%) | |||
| Male | 271 (55%) | 252 (57%) | |
| Female | 219 (44%) | 185 (42%) | |
| Trans Male/Transman | 1 (0.2%) | 0 (0%) | |
| Trans Female/Transwoman | 0 (0%) | 1 (0.2%) | |
| Genderqueer/Gender Non-conforming | 0 (0%) | 3 (0.7%) | |
| Prefer not to Say | 4 (0.8%) | 3 (0.7%) | |
| Age a, mean (SD), years | 39 (11) | 38 (12) | |
| Identify with Hispanic Ethnicity, No. (%) | |||
| No | 432 (87%) | 385 (87%) | |
| Yes—Mexican, Mexican American, Chicano/Chicana) | 25 (5.1%) | 18 (4.1%) | |
| Yes—Puerto Rican | 6 (1.2%) | 1 (0.2%) | |
| Yes—Cuban | 2 (0.4%) | 2 (0.5%) | |
| Yes—Another Hispanic Origin | 18 (3.6%) | 25 (5.6%) | |
| Prefer not to Say | 12 (2.4%) | 13 (2.9%) | |
| Racial Identity, No. (%) | |||
| American Indian/Alaska Native | 4 (0.8%) | 5 (1.1%) | |
| Asian Indian | 15 (3.0%) | 20 (4.5%) | |
| Black/African American | 52 (11%) | 42 (9.5%) | |
| Chinese | 6 (1.2%) | 8 (1.8%) | |
| Filipino | 4 (0.8%) | 0 (0%) | |
| Japanese | 2 (0.4%) | 2 (0.5%) | |
| Korean | 2 (0.4%) | 1 (0.2%) | |
| Multiple Identities | 11 (2.2%) | 14 (3.2%) | |
| Other Asian | 3 (0.6%) | 6 (1.4%) | |
| Other Pacific Islander | 1 (0.2%) | 0 (0%) | |
| Vietnamese | 3 (0.6%) | 7 (1.6%) | |
| White/Caucasian | 379 (77%) | 331 (75%) | |
| Prefer not to say | 13 (2.6%) | 8 (1.8%) | |
| Employment Status, No. (%) | |||
| Employed Full Time | 324 (65%) | 274 (62%) | |
| Employed Part Time | 48 (9.7%) | 49 (11%) | |
| Unemployed (Looking for Work) | 21 (4.2%) | 24 (5.4%) | |
| Unemployed (Not Looking for Work) | 19 (3.8%) | 12 (2.7%) | |
| Retired | 12 (2.4%) | 15 (3.4%) | |
| Student | 8 (1.6%) | 9 (2.0%) | |
| Self-Employed | 58 (12%) | 58 (13%) | |
| Prefer Not to Say | 5 (1.0%) | 3 (0.7%) | |
| Annual Household Income, No. (%) | |||
| <$25,000 | 71 (14%) | 80 (18%) | |
| $25,000–$49,999 | 154 (31%) | 111 (25%) | |
| $50,000–$74,999 | 121 (24%) | 121 (27%) | |
| $75,000–$99,999 | 69 (14%) | 68 (15%) | |
| $100,000–$124,999 | 32 (6.5%) | 20 (4.5%) | |
| $125,000–$149,999 | 20 (4.0%) | 17 (3.8%) | |
| >$150,000 | 19 (3.8%) | 20 (4.5%) | |
| Prefer Not to Say | 9 (1.8%) | 7 (1.6%) | |
| Education Level, No. (%) | |||
| Less than High School | 4 (0.8%) | 3 (0.7%) | |
| High School Diploma | 64 (13%) | 53 (12%) | |
| Some College, no degree | 108 (22%) | 111 (25%) | |
| Bachelor’s Degree | 255 (52%) | 221 (50%) | |
| Master’s Degree | 48 (9.7%) | 44 (9.9%) | |
| Professional Degree | 7 (1.4%) | 7 (1.6%) | |
| Doctorate Degree | 4 (0.8%) | 4 (0.9%) | |
| Prefer not to Say | 5 (1.0%) | 1 (0.2%) | |
| Political Identity b, mean (SD) | 4.13, (1.86) | 4.20, (1.88) | |
| Strongly Conservative | 43 (8.7%) | 36 (8.1%) | |
| Conservative | 80 (16%) | 73 (16%) | |
| Somewhat Conservative | 59 (12%) | 53 (12%) | |
| Neither conservative nor liberal | 103 (21%) | 83 (19%) | |
| Somewhat Liberal | 67 (14%) | 63 (14%) | |
| Liberal | 91 (18%) | 80 (18%) | |
| Strongly Liberal | 45 (9.1%) | 52 (12%) | |
| Prefer not to Say | 7 (1.4%) | 4 (0.9%) | |
| Intentions to get next indicated dose of a COVID-19 vaccine, No. (%) | |||
| Unsure—Don’t need more time to decide | 27 (5.5%) | 18 (4.1%) | |
| Unsure—Need more time to decide | 150 (30%) | 126 (28%) | |
| Will Get Vaccine | 198 (40%) | 191 (43%) | |
| Won’t Get Vaccine | 120 (24%) | 109 (25%) | |
| Social Media is Greatest Influence, No. (%) | 102 (21%) | 93 (21%) |
| Headache | Fever | Fatigue | Myocarditis | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Covariate | Level | Beta (95% CI) | p-Value a | Beta (95% CI) | p-Value a | Beta (95% CI) | p-Value a | Beta (95% CI) | p-Value a |
| Probability Descriptor | <0.001 | <0.001 | 0.002 | <0.001 | |||||
| Numerical Probability | Ref | Ref | Ref | Ref | |||||
| Verbal Probability | 5.0 (2.0, 8.1) | 27 (23, 30) | 4.9 (1.8, 8.0) | 4.6 (2.1, 7.2) | |||||
| High Social Media Influence (Yes vs. No) | 1.5 (−2.5, 5.5) | 0.4 | 3.7 (−0.72, 8.0) | 0.066 | −2.9 (−6.8, 1.1) | 0.14 | 6.7 (3.2, 10) | <0.001 | |
| Gender Identity b | |||||||||
| Female | Ref | Ref | Ref | Ref | |||||
| Male | −4.8 (−7.8, −1.7) | −6.1 (−9.3, −2.9) | −5.6 (−8.7, −2.4) | −2.8 (−5.3, −0.21) | |||||
| Non-Binary | −3 (−12, 6.5) | 4.9 (−16, 26) | 9.8 (−11, 30) | −3.2 (−14, 7.3) | |||||
| Prefer not to Say | −29 (−45, −13) | −21 (−40, −2.4) | −13 (−33, 8.1) | −12 (−24, 0.22) | |||||
| Age (per 1 year) | 0.14 (−0.01, 0.29) | 0.26 (0.09, 0.43) | 0.17 (0.01, 0.33) | 0.26 (0.11, 0.42) | |||||
| Race b | |||||||||
| Non-White | Ref | Ref | Ref | Ref | |||||
| Prefer not to Say | 2.5 (−7.2, 12) | 2.7 (−6.7, 12) | 0.76 (−9.9, 11) | 4.7 (−13, 3.6) | |||||
| White/Caucasian | 0.65 (−3.2, 4.5) | −1.5 (−5.5, 2.6) | 1.8 (−2.2, 5.7) | −4.3 (−7.8, −0.92) | |||||
| Hispanic Ethnicity b | |||||||||
| Not Hispanic | Ref | Ref | Ref | Ref | |||||
| Hispanic | 3.2 (−2.1, 8.4) | 6.4 (0.19, 13) | 2.3 (−3.5, 8.1) | 7 (1.8, 12) | |||||
| Prefer not to Say | −2.6 (−14, 8.5) | −5.3 (−16, 5.2) | −11 (−22, −0.15) | 5.2 (−4.3, 15) | |||||
| Employment Status b | |||||||||
| Employed | Ref | Ref | Ref | Ref | |||||
| Prefer Not to Say | 7.4 (−13, 28) | 14 (−9.9, 38) | −2 (−21, 17) | 3.3 (−9.2, 16) | |||||
| Retired | −7.4 (−18, 3.2) | −5.3 (−16, 5.0) | −4.7 (−16, 6.2) | −0.36 (−12, 11) | |||||
| Student | 8.1 (−3.1, 19) | 3.8 (−8.5, 16) | 0.33 (−12, 13) | 2.8 (−6.3, 12) | |||||
| Unemployed | 3.7 (−1.1, 8.6) | 3.5 (−1.6, 8.5) | 8.4 (3.2, 14) | −0.8 (−5.2, 3.6) | |||||
| Household Income b | |||||||||
| <$25,000 | Ref | Ref | Ref | Ref | |||||
| ≥$25,000 | −0.59 (−4.6, 3.4) | −0.62 (−5.0, 3.8) | −0.65 (−4.7, 3.4) | 1.1 (−1.9, 4.2) | |||||
| Prefer Not to Say | 8.1 (−5.2, 21) | 6.5 (−9.5, 22) | 2.6 (−8.8, 14) | −2.3 (−10, 5.8) | |||||
| Education Level b | |||||||||
| Advanced Degree | Ref | Ref | Ref | Ref | |||||
| Bachelor’s Degree | −0.92 (−5.6, 3.7) | −4.6 (−9.8, 0.61) | −4 (−8.7, 0.74) | −2 (−6.6, 2.7) | |||||
| High School or Less | 2.9 (−3.0, 8.7) | −2.7 (−9.1, 3.7) | −0.29 (−6.2, 5.6) | −2 (−7.4, 3.4) | |||||
| Prefer not to Say | 8.9 (−10, 28) | 11 (−18, 41) | 24 (10, 38) | 10 (−7.0, 28) | |||||
| Some College, no degree | 2.1 (−3.1, 7.2) | −6.7 (−12, −1.1) | −1.9 (−7.1, 3.4) | −5.6 (−10, −1.0) | |||||
| Political Identity c | −0.06 (−1.0, 0.86) | −0.64 (−1.6, 0.34) | 0.85 (−0.09, 1.8) | −1.2 (−2.1, −0.31) | |||||
| Vaccine Hesitancy | |||||||||
| Vaccine Accepting | Ref | Ref | Ref | Ref | |||||
| Vaccine Deferring | 5.6 (2.0, 9.2) | −2.0 (−5.8, 1.7) | 7.4 (3.8, 11) | −4.9 (−7.9, −1.8) | |||||
| Vaccine Hesitant | 0.50 (−7.2, 8.3) | −6.8 (−14, 0.39) | −3.5 (−11, 4.4) | −4.5 (−9.2, 0.22) | |||||
| Vaccine Rejecting | 6.7 (2.5, 11) | 0.52 (−3.9, 4.9) | 7.9 (3.7, 12) | −1.5 (−5.5, 2.6) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosen, J.E.; Chang, S.S.E.; Williams, S.; Lee, J.S.; Han, D.; Agrawal, N.; Joo, J.H.; Hsieh, G.; Reinecke, K.; Liao, J.M. Association between Risk Communication Format and Perceived Risk of Adverse Events after COVID-19 Vaccination among US Adults. Healthcare 2023, 11, 380. https://doi.org/10.3390/healthcare11030380
Rosen JE, Chang SSE, Williams S, Lee JS, Han D, Agrawal N, Joo JH, Hsieh G, Reinecke K, Liao JM. Association between Risk Communication Format and Perceived Risk of Adverse Events after COVID-19 Vaccination among US Adults. Healthcare. 2023; 11(3):380. https://doi.org/10.3390/healthcare11030380
Chicago/Turabian StyleRosen, Joshua E., Sylvia Seo Eun Chang, Spencer Williams, Joy S. Lee, DaHee Han, Nidhi Agrawal, Joseph H. Joo, Gary Hsieh, Katharina Reinecke, and Joshua M. Liao. 2023. "Association between Risk Communication Format and Perceived Risk of Adverse Events after COVID-19 Vaccination among US Adults" Healthcare 11, no. 3: 380. https://doi.org/10.3390/healthcare11030380