
Design and Development of Smart Weight Measurement, Lateral Turning and Transfer Bedding for Unconscious Patients in Pandemics

 ,
,  , , and
, , and
Abstract
:1. Introduction
- Medical prescription;
- Fluid balance;
- Assessment of nutrition.
2. Literature Review
3. Materials and Methods
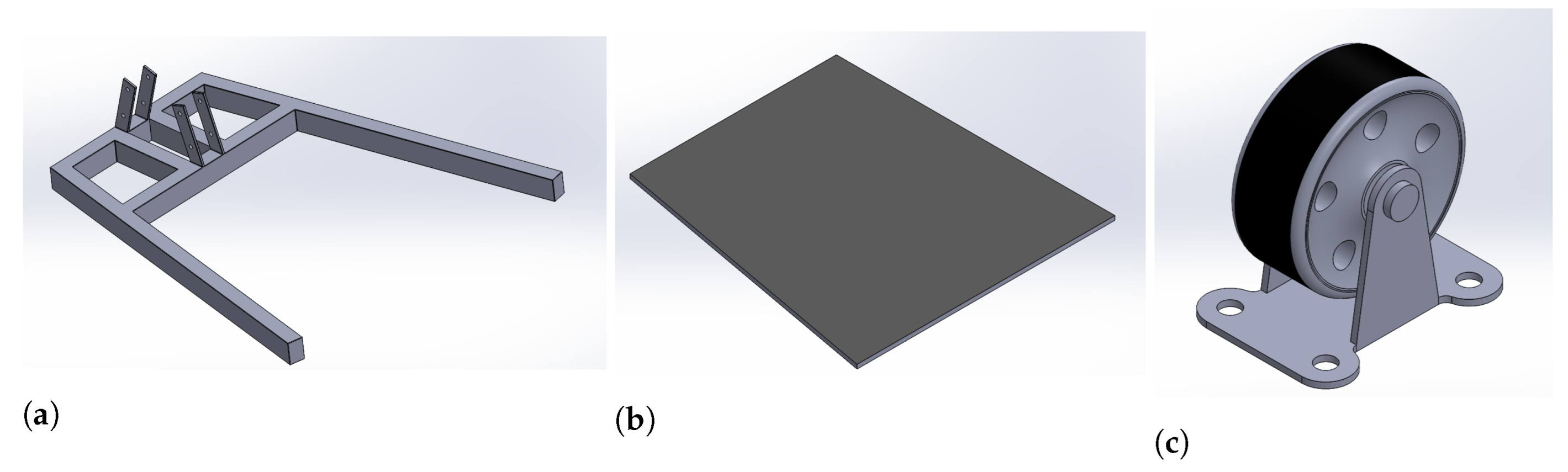
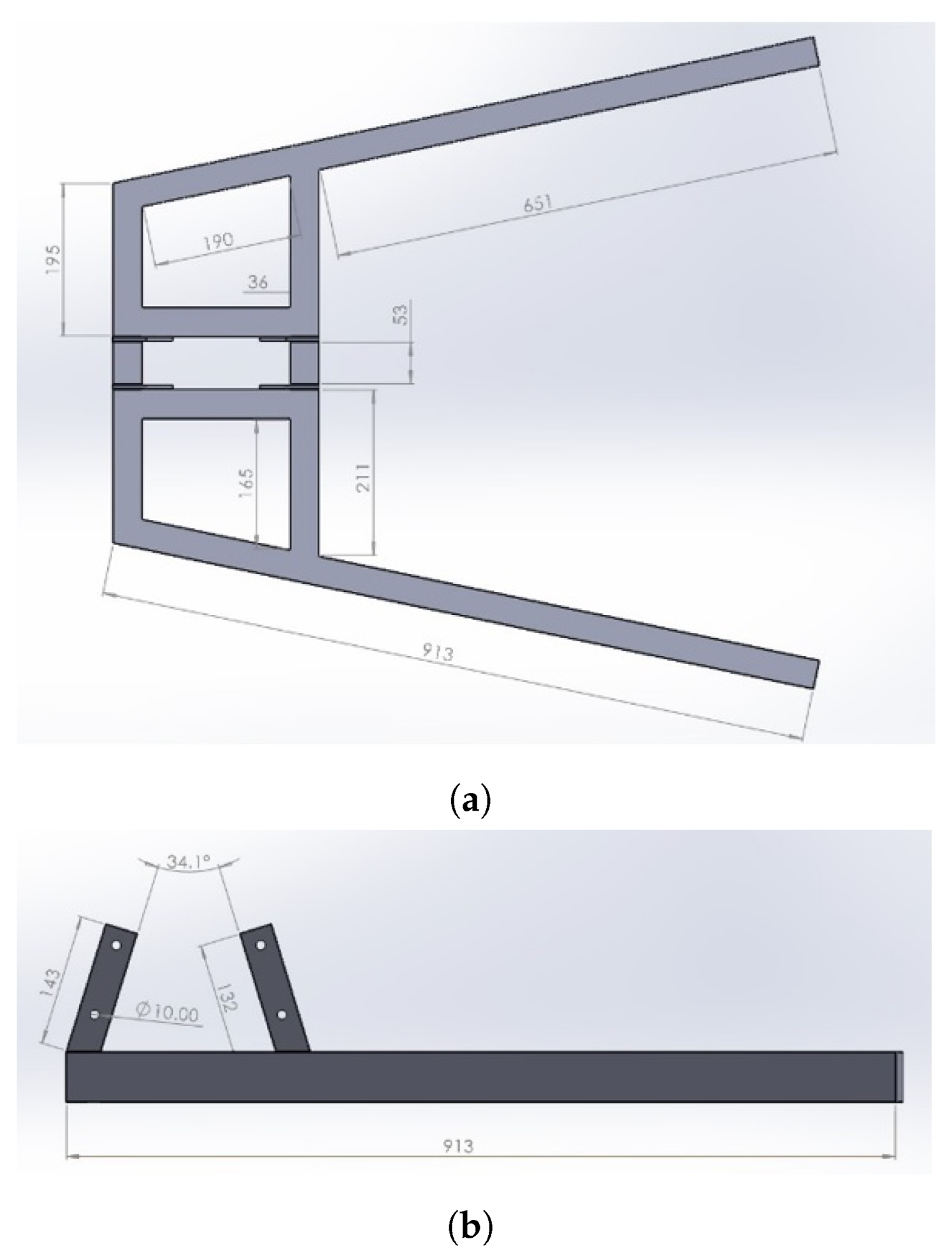
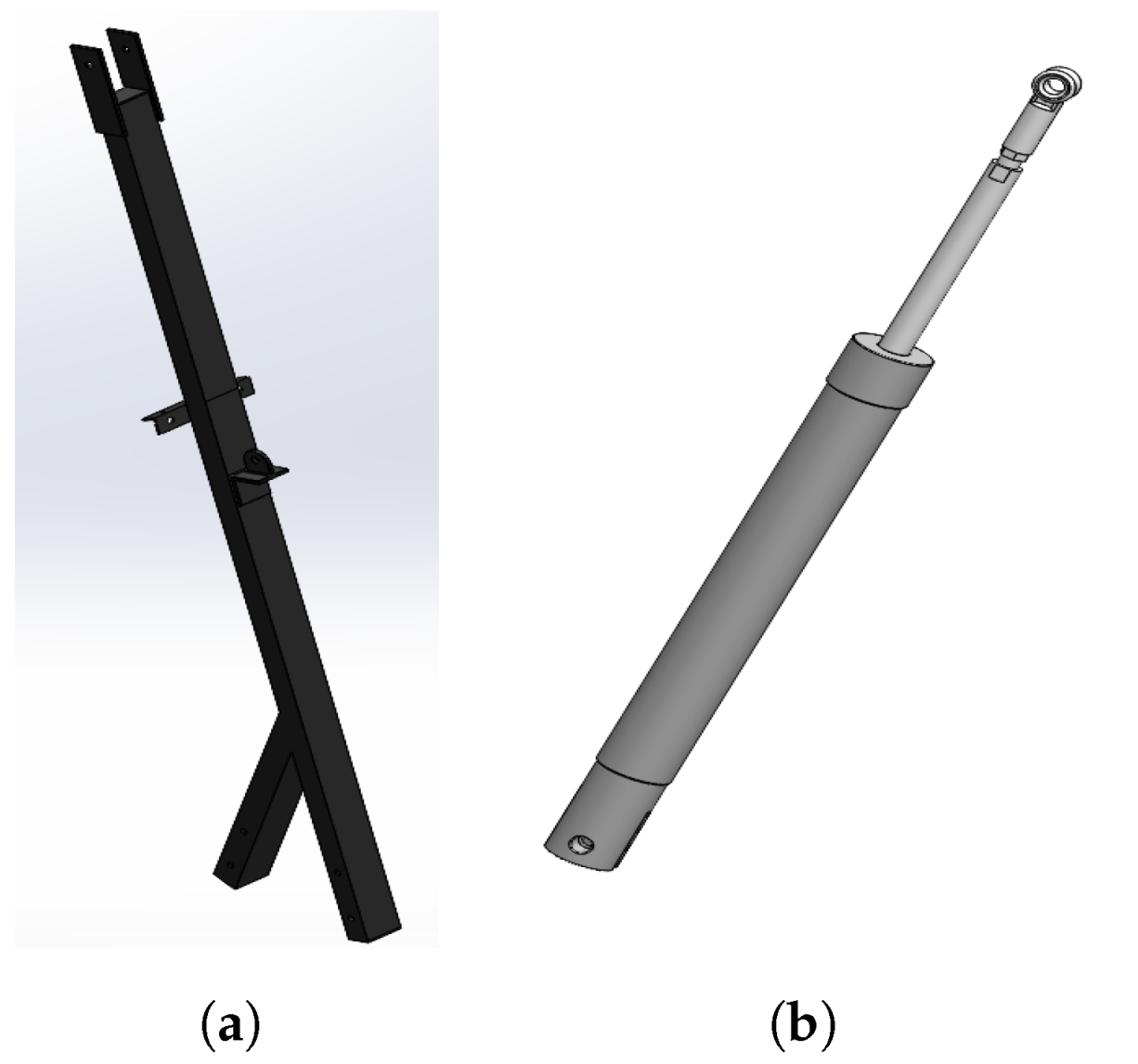
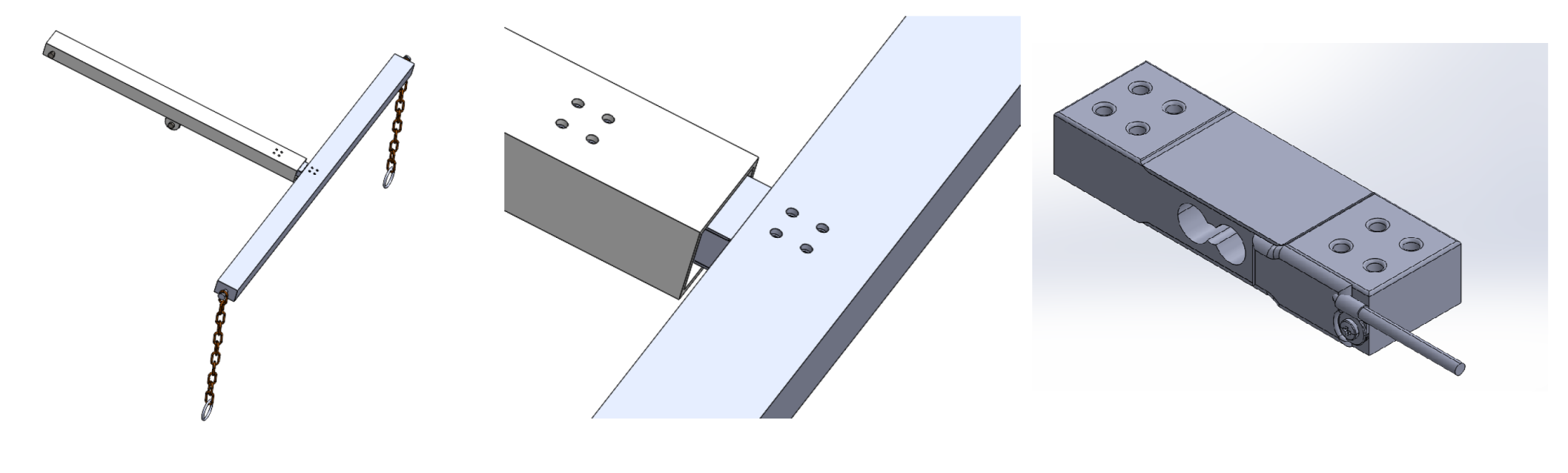
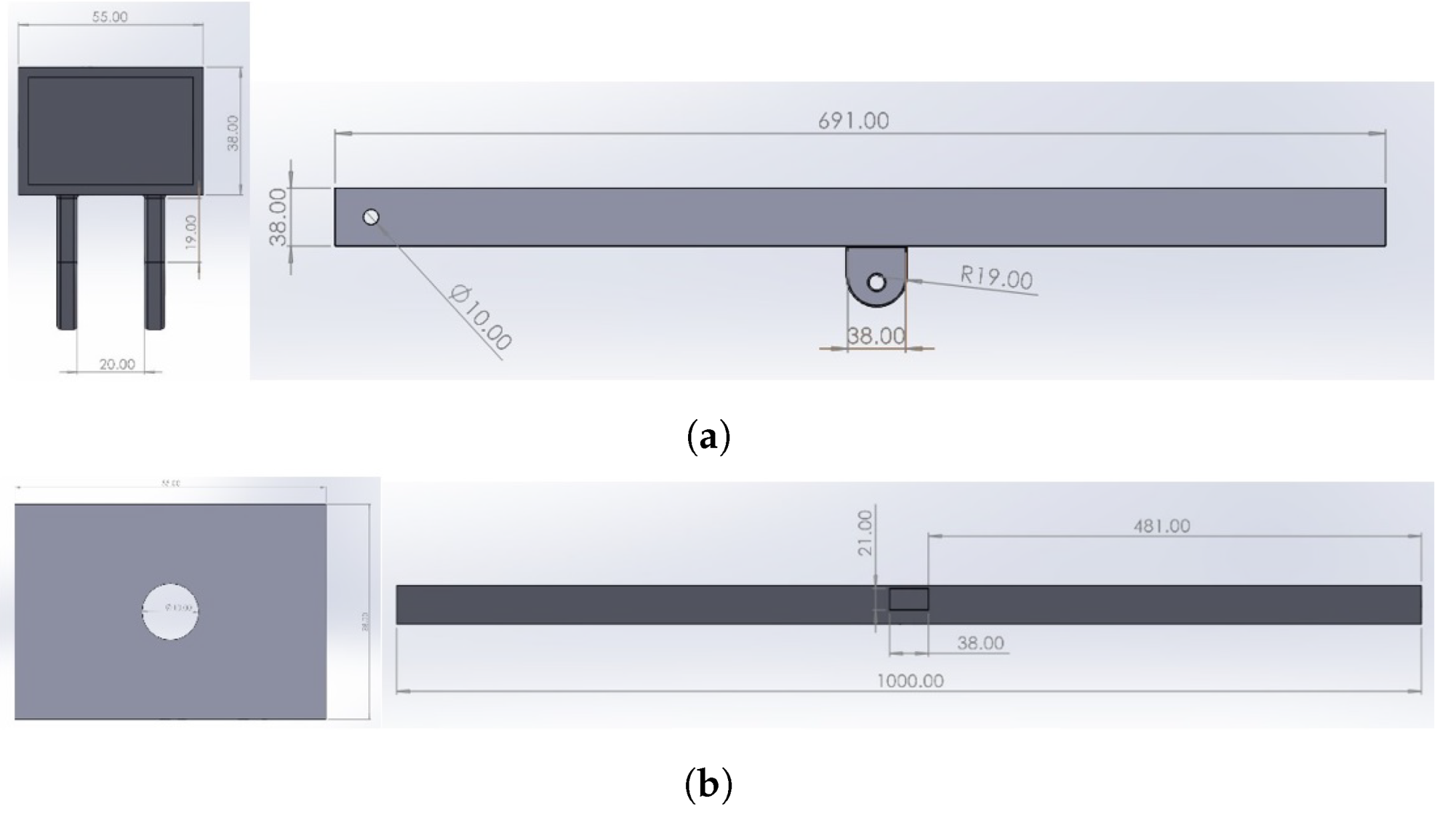
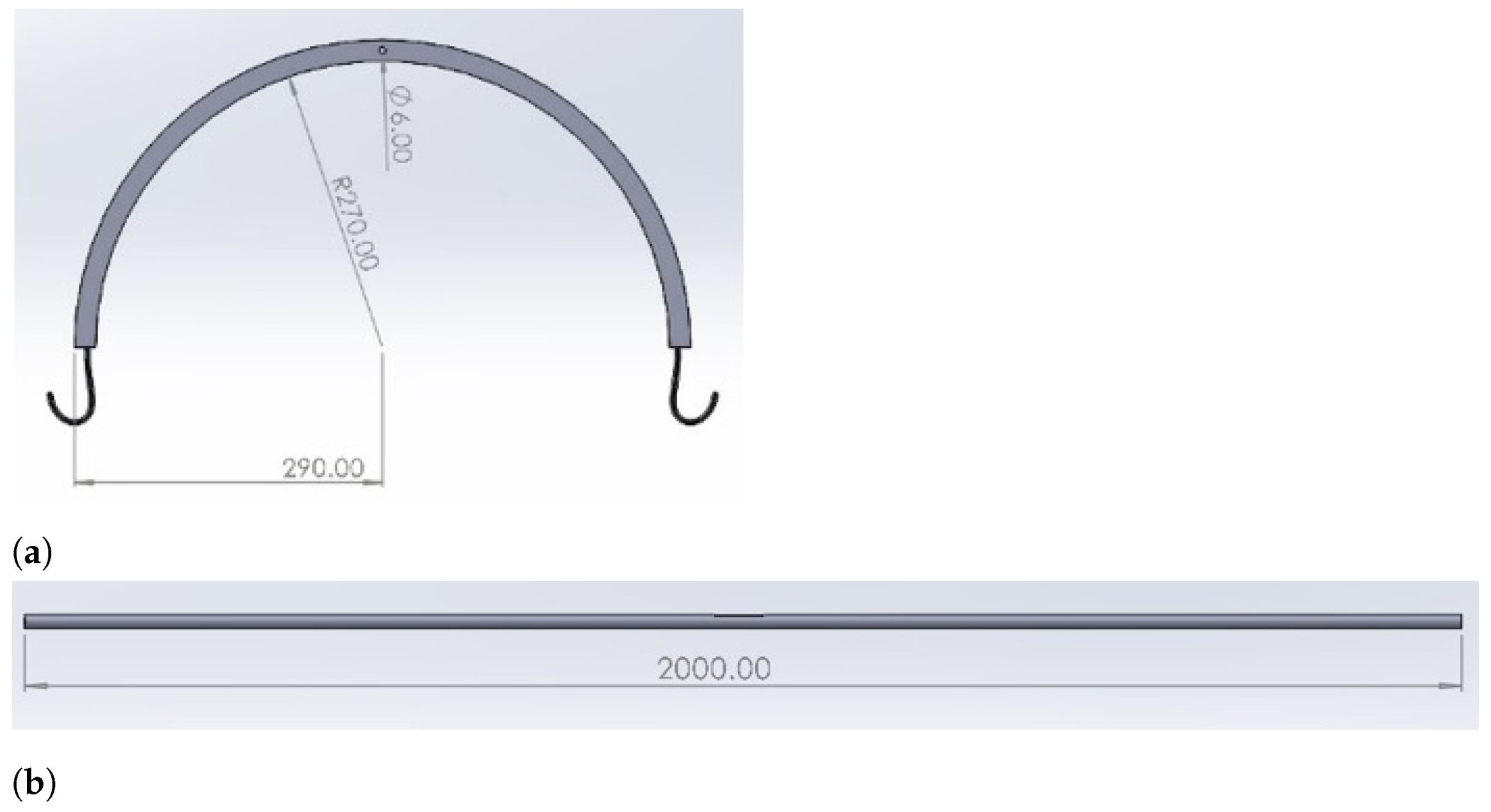
3.1. Mechanical Design
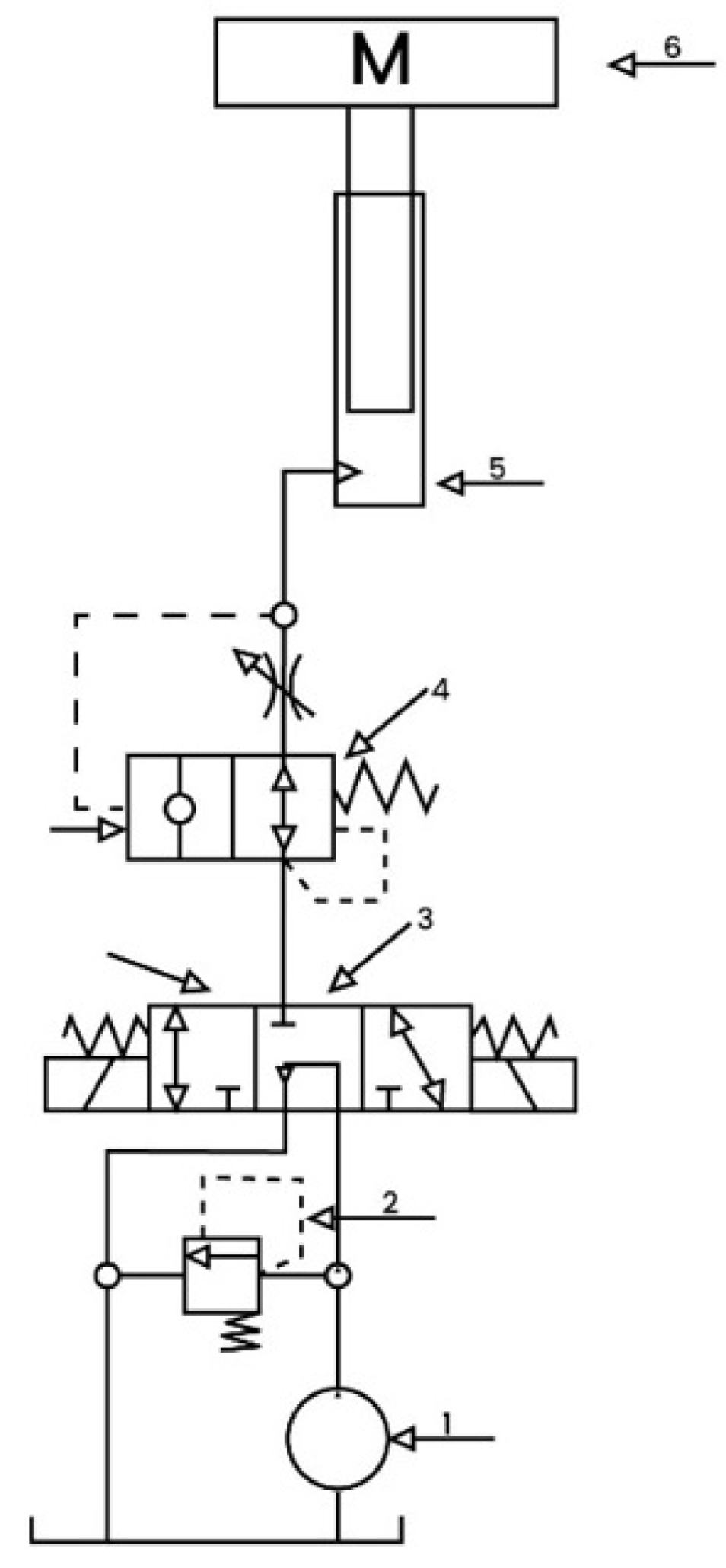
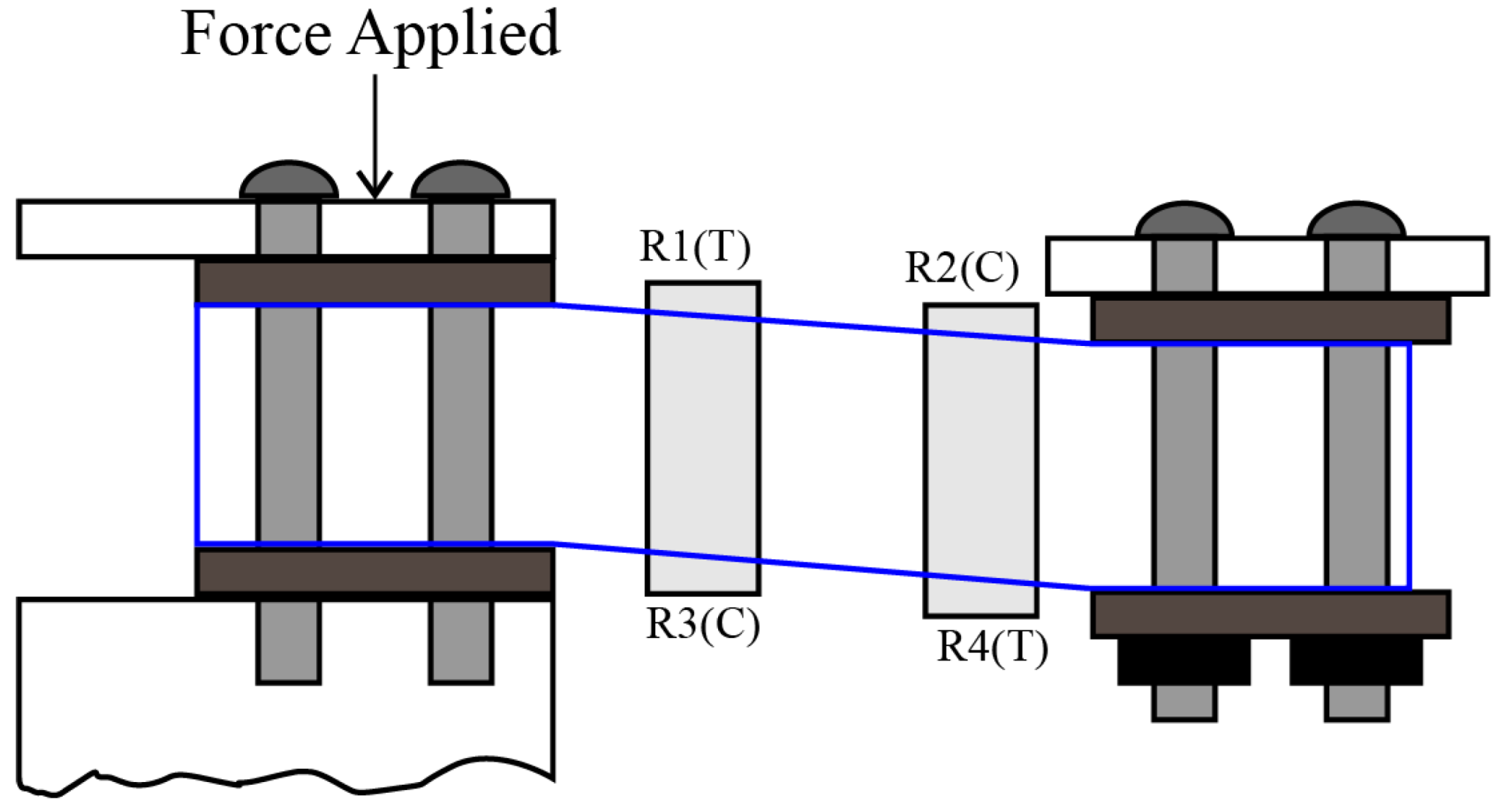
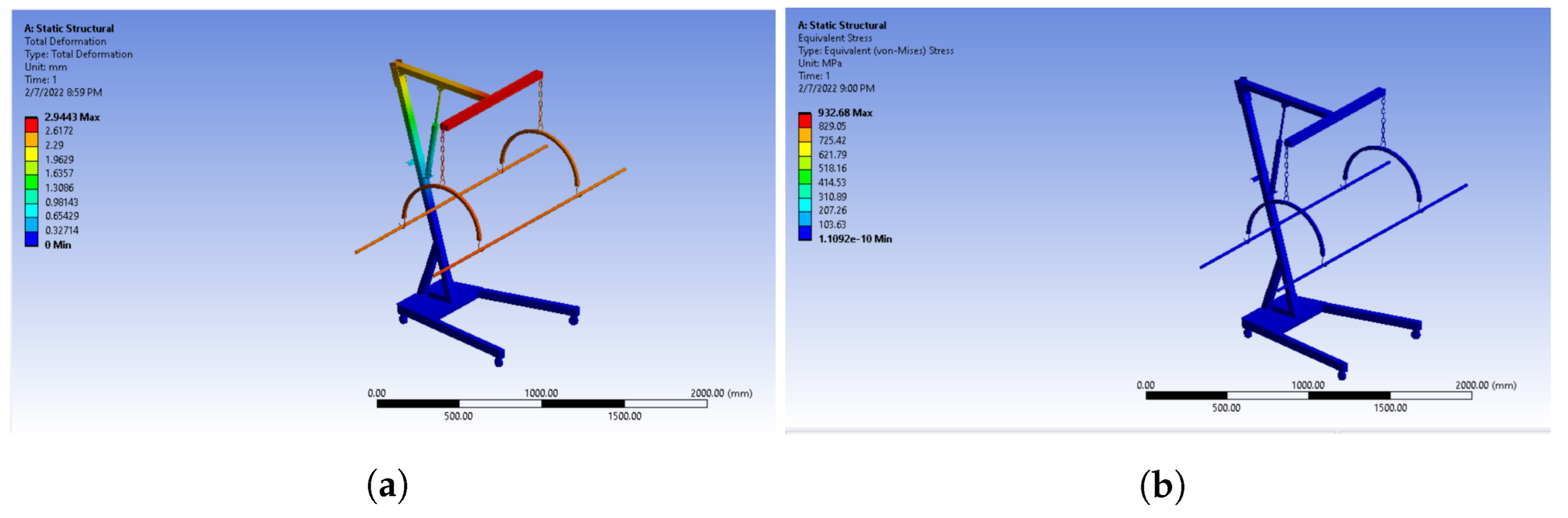
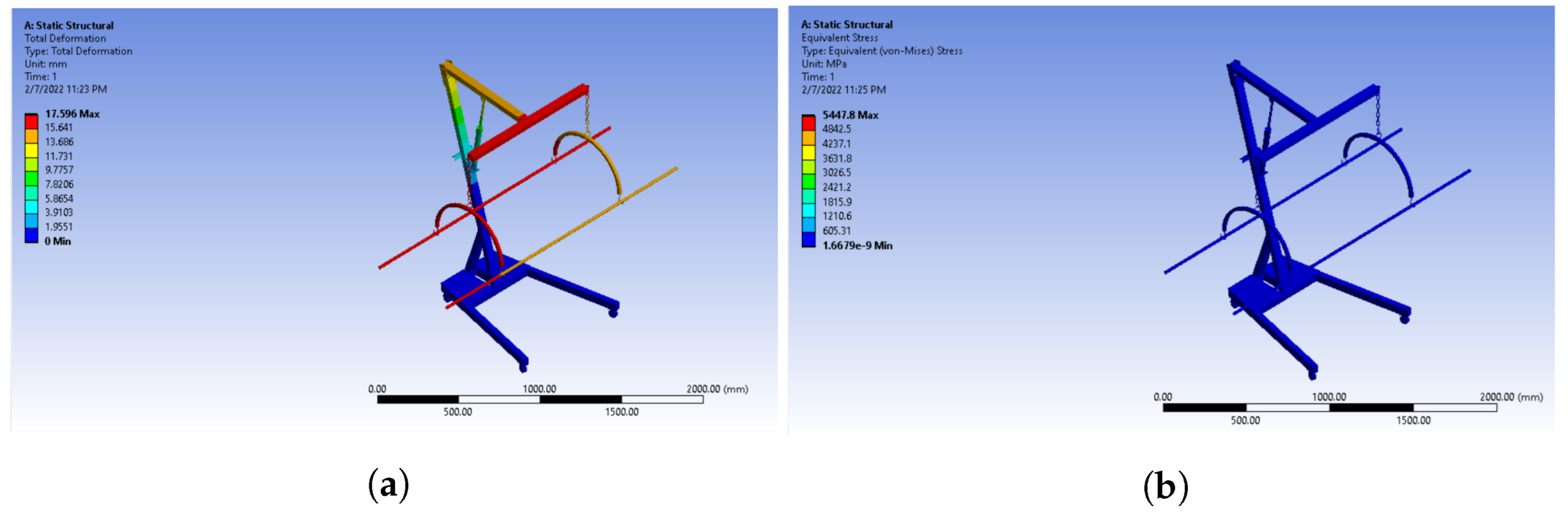
3.2. Numerical Model
- i.
- Hydraulic pump (power element);
- ii.
- Relief valve (pressure control element);
- iii.
- Directional valve (direction control element);
- iv.
- Explosion-proof valve (speed control element);
- v.
- Plunger-type cylinder (executive element);
- vi.
- Mass (stretcher with the patient).
3.3. Electrical Design
3.4. Material Selection
3.5. Fabrication and Integration
4. Results and Discussions
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muzaffar, S.; Elfadel, I.M. Self-synchronized, continuous body weight monitoring using flexible force sensors and ground reaction force signal processing. IEEE Sens. J. 2020, 20, 10886–10897. [Google Scholar] [CrossRef]
- Ichikawa, S.; Hamada, M.; Sugimori, H. A deep-learning method using computed tomography scout images for estimating patient body weight. Sci. Rep. 2021, 11, 15627. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, A. Measuring and managing fluid balance. Nurs. Times 2011, 107, 12–16. [Google Scholar] [PubMed]
- Salehidoost, R.; Mansouri, A.; Amini, M.; Yamini, S.A.; Aminorroaya, A. Body mass index and the all-cause mortality rate in patients with type 2 diabetes mellitus. Acta Diabetol. 2018, 55, 569–577. [Google Scholar] [CrossRef]
- Collaboration, P.S. Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [Green Version]
- Chittawatanarat, K.; Pichaiya, T.; Chandacham, K.; Jirapongchareonlap, T.; Chotirosniramit, N. Fluid accumulation threshold measured by acute body weight change after admission in general surgical intensive care units: How much should be concerning? Ther. Clin. Risk Manag. 2015, 11, 1097. [Google Scholar] [CrossRef]
- Köster, M.; Dennhardt, S.; Jüttner, F.; Hopf, H.B. Cumulative changes in weight but not fluid volume balances reflect fluid accumulation in ICU patients. Acta Anaesthesiol. Scand. 2017, 61, 205–215. [Google Scholar] [CrossRef]
- Eastwood, G.M.; Peck, L.; Young, H.; Prowle, J.; Vasudevan, V.; Jones, D.; Bellomo, R. Intravenous fluid administration and monitoring for adult ward patients in a teaching hospital. Nurs. Health Sci. 2012, 14, 265–271. [Google Scholar] [CrossRef]
- Charani, E.; Gharbi, M.; Hickson, M.; Othman, S.; Alfituri, A.; Frost, G.; Holmes, A. Lack of weight recording in patients being administered narrow therapeutic index antibiotics: A prospective cross-sectional study. BMJ Open 2015, 5, e006092. [Google Scholar] [CrossRef] [Green Version]
- Birkholzer, S.; Richardson, N.; Fitzgerald, E.; Harris, B.; Knighton, J. Recording of patient weight in the intensive care unit: A survey of current practice. Intensive Care Med. Exp. 2015, 3, 1–2. [Google Scholar] [CrossRef]
- Kottner, J.; Cuddigan, J.; Carville, K.; Balzer, K.; Berlowitz, D.; Law, S.; Litchford, M.; Mitchell, P.; Moore, Z.; Pittman, J.; et al. Prevention and treatment of pressure ulcers/injuries: The protocol for the second update of the international Clinical Practice Guideline 2019. J. Tissue Viability 2019, 28, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom, N.; Demuth, P.; Braden, B. The Braden Scale for predicting pressure sore risk. Nurs. Res. 1987, 36, 205–210. [Google Scholar] [CrossRef]
- Cullum, N.; Deeks, J.J.; Fletcher, A.W.; Sheldon, T.A.; Song, F. Preventing and treating pressure sores. Qual. Health Care 1995, 4, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, C.A.; Elixhauser, A. Hospitalizations related to pressure sores, 2003. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006. [Google Scholar]
- Petersen, N.; Bittmann, S. The epidemiology of pressure sores. Scand. J. Plast. Reconstr. Surg. 1971, 5, 62–66. [Google Scholar] [PubMed]
- Lowne, D.R.; Tarler, M. Designing a low-cost mattress sensor for automated body position classification. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 6437–6440. [Google Scholar]
- Russell, J.; Lichtenstein, S. Randomized controlled trial to determine the safety and efficacy of a multi-cell pulsating dynamic mattress system in the prevention of pressure ulcers in patients undergoing cardiovascular surgery. Ostomy/Wound Manag. 2000, 46, 46–51. [Google Scholar]
- Lyder, C.H. Pressure ulcer prevention and management. JAMA 2003, 289, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Garrisi, D. Christmas 1864: Death from bedsores in a workhouse–the politics of wound care, the media and social reform in Victorian London. Public Underst. Sci. 2019, 28, 1005–1009. [Google Scholar] [CrossRef]
- McGregor Clarkson, D. Patient weighing: Standardisation and measurement. Nurs. Stand. 2012, 26, 33–37. [Google Scholar] [CrossRef]
- LACORS. The Weight of the Matter: Final Report of the LACORS National Medical Weighing Project 2008/9. 2009. Available online: https://www.ukwf.org.uk/res/medical weighing project1.pdf (accessed on 28 January 2022).
- Mhatre, A.; Duvall, J.; Ding, D.; Cooper, R.; Pearlman, J. Design and focus group evaluation of a bed-integrated weight measurement system for wheelchair users. Assist. Technol. 2016, 28, 193–201. [Google Scholar] [CrossRef]
- Supranata, T.H.; Davin, P.S.S.; Jeremy, D.K.; Pratiwi, A.E.; Wulandari, M. Body weight measurement using image processing based on body surface area and elliptical tube volume. In Proceedings of the 2018 10th International Conference on Information Technology and Electrical Engineering (ICITEE), Bali, Indonesia, 24–26 July 2018; pp. 290–294. [Google Scholar]
- Benalcazar, D.; Benalcazar, D.; Erazo, A. Artificial neural networks and digital image processing: An approach for indirect weight measurement. In Proceedings of the 2017 IEEE Second Ecuador Technical Chapters Meeting (ETCM), Salinas, Ecuador, 16–20 October 2017; pp. 1–6. [Google Scholar]
- Labati, R.D.; Genovese, A.; Piuri, V.; Scotti, F. Weight estimation from frame sequences using computational intelligence techniques. In Proceedings of the 2012 IEEE International Conference on Computational Intelligence for Measurement Systems and Applications (CIMSA) Proceedings, Tianjin, China, 2–4 July 2012; pp. 29–34. [Google Scholar]
- Nancy, G.A.; Rashmi, B.; Kalpana, R. Region Specific Weight Measuring System for Bedridden patients. In Proceedings of the 2020 Sixth International Conference on Bio Signals, Images, and Instrumentation (ICBSII), Chennai, India, 27–28 February 2020; pp. 1–4. [Google Scholar]
- Lindgren, M.; Unosson, M.; Fredrikson, M.; Ek, A.C. Immobility—A major risk factor for development of pressure ulcers among adult hospitalized patients: A prospective study. Scand. J. Caring Sci. 2004, 18, 57–64. [Google Scholar] [CrossRef]
- Smit, I.; Harrison, L.; Letzkus, L.; Quatrara, B. What factors are associated with the development of pressure ulcers in a medical intensive care unit? Dimens. Crit. Care Nurs. 2016, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.; Gorecki, C.; Nelson, E.A.; Closs, S.J.; Defloor, T.; Halfens, R.; Farrin, A.; Brown, J.; Schoonhoven, L.; Nixon, J. Patient risk factors for pressure ulcer development: Systematic review. Int. J. Nurs. Stud. 2013, 50, 974–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannen, A.; Dassen, T.; Halfens, R. Differences in prevalence of pressure ulcers between the Netherlands and Germany–associations between risk, prevention and occurrence of pressure ulcers in hospitals and nursing homes. J. Clin. Nurs. 2008, 17, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Jocelyn Chew, H.S.; Thiara, E.; Lopez, V.; Shorey, S. Turning frequency in adult bedridden patients to prevent hospital-acquired pressure ulcer: A scoping review. Int. Wound J. 2018, 15, 225–236. [Google Scholar] [CrossRef]
- Summer, W.R.; Curry, P.; Haponik, E.F.; Nelson, S.; Elston, R. Continuous mechanical turning of intensive care unit patients shortens length of stay in some diagnostic-related groups. J. Crit. Care 1989, 4, 45–53. [Google Scholar] [CrossRef]
- Lyder, C.H.; Preston, J.; Grady, J.N.; Scinto, J.; Allman, R.; Bergstrom, N.; Rodeheaver, G. Quality of care for hospitalized Medicare patients at risk for pressure ulcers. Arch. Intern. Med. 2001, 161, 1549–1554. [Google Scholar] [CrossRef] [Green Version]
- Rich, S.E.; Margolis, D.; Shardell, M.; Hawkes, W.G.; Miller, R.R.; Amr, S.; Baumgarten, M. Frequent manual repositioning and incidence of pressure ulcers among bed-bound elderly hip fracture patients. Wound Repair Regen. 2011, 19, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Ching-Hua, W.; Ting-Chun, T.; Shin-Chieh, H.; Wan-Chun, C.; Yen-Ming, C.; Kun-Tse, T.; Chun-Wen, Y.; Kuo-Yi, C. Hospital bed with auxiliary functions of lateral positioning and transferring for immobilized patients. In Proceedings of the IECON 2007—33rd Annual Conference of the IEEE Industrial Electronics Society, Taipei, Taiwan, 5–8 November 2007; pp. 2991–2995. [Google Scholar]
- Manoj, R.; Kumarasami, R.; Joseph, J.; George, B.; Sivaprakasam, M. Continuous weight monitoring system for icu beds using air-filled mattresses/pads: A proof of concept. In Proceedings of the 2019 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019; pp. 1–5. [Google Scholar]
- Basmajian, A.; Blanco, E.E.; Asada, H.H. The marionette bed: Automated rolling and repositioning of bedridden patients. In Proceedings of the 2002 IEEE International Conference on Robotics and Automation, Washington, DC, USA, 10–17 May 2002; Volume 2, pp. 1422–1427. [Google Scholar]
- Wei, C.H. Turning Mechanism for a Patient Confined to a Bed. U.S. Patent 6,668,396, 19 December 2002. [Google Scholar]
- Charder Electronics. MS6000 Bed Scale. 2021. Available online: https://www.chardermedical.com/bed-weighing-scales/MS6000.html (accessed on 28 January 2022).
- Health-Care Equipment. Seca 985 Electronic Bedn and Dialysis Scales. 2021. Available online: https://www.hce-uk.com/Seca-985-Electronic-Bed-and-Dialysis-Scales (accessed on 8 February 2022).
- VENDLET. Vendlet V5S. 2020. Available online: https://www.vendlet.com/products/vendlet/vendlet-v5s (accessed on 8 February 2022).
- Gong, W.; Yu, Z.J. Mathematical Modeling and Simulation Analysis of Lift for Car Hydraulic System. Appl. Mech. Mater. 2014, 490, 447–450. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Specification |
|---|---|
| Working Load | 270 KG |
| Power Rating | 12V DC |
| Weight Monitoring | Yes |
| Lateral Turning | Yes |
| Portable | Yes |
| Can be utilized for multiple beds | Yes |
| Feature | Specification |
|---|---|
| Operating Voltage | 12V DC |
| Standard Stroke | 25–800 mm |
| Maximum Thrust | 6000 N |
| Speed with no load | 5 mm/s |
| Working Temperature | −26 C to 65 C |
| Limit Switch | Built in |
| Parameter | Value |
|---|---|
| Density | 0.954 g/cm |
| Yield strength | 20–30 MPa |
| Ultimate tensile strength | 26 MPa |
| Toughness | 2–5 MPa |
| Elastic modulus | 1.0 × 103 MPa |
| Working temperature | −80 C–100 C |
| Device | Weight Limit | Turning | Cost |
|---|---|---|---|
| Vendet VS5 | 200 kg | Yes | USD 10,980 + GST |
| Seca 985 Electronic Bed and Dialysis Scales | 250 kg | No | USD 6320 |
| Detecto IB800 Digital Stretcher Scale | 350 kg | No | USD 10,757 |
| Proposed Solution | 270 kg | Yes | USD 1500 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shafi, I.; Farooq, M.S.; De La Torre Díez, I.; Breñosa, J.; Espinosa, J.C.M.; Ashraf, I. Design and Development of Smart Weight Measurement, Lateral Turning and Transfer Bedding for Unconscious Patients in Pandemics. Healthcare 2022, 10, 2174. https://doi.org/10.3390/healthcare10112174
Shafi I, Farooq MS, De La Torre Díez I, Breñosa J, Espinosa JCM, Ashraf I. Design and Development of Smart Weight Measurement, Lateral Turning and Transfer Bedding for Unconscious Patients in Pandemics. Healthcare. 2022; 10(11):2174. https://doi.org/10.3390/healthcare10112174
Chicago/Turabian StyleShafi, Imran, Muhammad Siddique Farooq, Isabel De La Torre Díez, Jose Breñosa, Julio César Martínez Espinosa, and Imran Ashraf. 2022. "Design and Development of Smart Weight Measurement, Lateral Turning and Transfer Bedding for Unconscious Patients in Pandemics" Healthcare 10, no. 11: 2174. https://doi.org/10.3390/healthcare10112174