
Alterations in Cortisol Profiles among Mothers of Children with ASD Related to Poor Child Sleep Quality

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Participant Characteristics
2.2. Subjective Sleep Profiles of Mothers
2.3. Subjective Sleep Profiles of Children with ASD
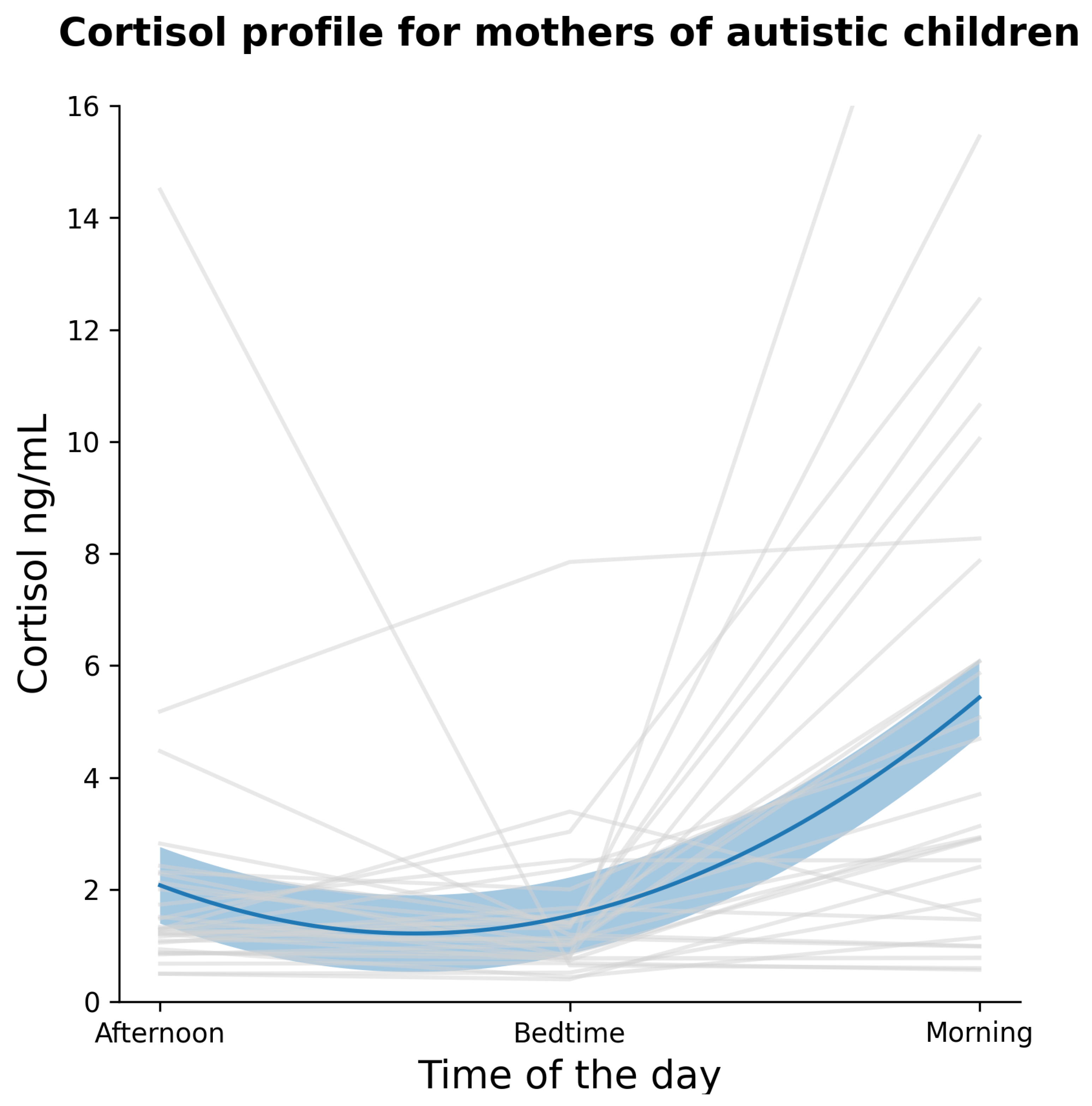
2.4. Mothers’ Cortisol Profiles
3. Discussion
Limitations and Future Studies
4. Materials and Methods
4.1. Participants
4.2. Questionnaires
4.2.1. Childhood Autism Rating Scale-Second Edition (CARS-2)
4.2.2. Major Depression Inventory (MDI)
4.2.3. Pittsburgh Sleep Quality Index (PSQI)
4.2.4. Epworth Sleepiness Scale (ESS)
4.2.5. Child’s Sleep Habits Questionnaire (CSHQ)
4.3. Cortisol Salivary Samples
4.4. Procedure
4.5. Analytic Plan
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.Y.; Nair, M.; Halpern, R.; Kuper, H.; Breinbauer, C.; De Vries, P.J.; Gladstone, M.; et al. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef] [Green Version]
- Scherer, N.; Verhey, I.; Kuper, H. Depression and anxiety in parents of children with intellectual and developmental disabilities: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219888. [Google Scholar] [CrossRef] [PubMed]
- Solarsh, G.; Hofman, K.J. Developmental Disabilities. In Disease and Mortality in Sub-Saharan Africa, 2nd ed.; The World Bank: Washington, DC, USA, 2011; Chapter 10. [Google Scholar]
- Liddle, M.; Birkett, K.; Bonjour, A.; Risma, K. A collaborative approach to improving health care for children with developmental disabilities. Pediatrics 2018, 142, e20181136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, A.C. From refrigerator mothers to warrior-heroes: The cultural identity transformation of mothers raising children with intellectual disabilities. Symb. Interact. 2011, 34, 220–243. [Google Scholar] [CrossRef]
- Bettelheim, B. Empty Fortress; Simon and Schuster: New York, NY, USA, 1972. [Google Scholar]
- Lansford, J.E.; Rothenberg, W.A.; Jensen, T.M.; Lippold, M.A.; Bacchini, D.; Bornstein, M.H.; Chang, L.; Deater-Deckard, K.; Di Giunta, L.; Dodge, K.A.; et al. Bidirectional relations between parenting and behavior problems from age 8 to 13 in nine countries. J. Res. Adolesc. 2018, 28, 571–590. [Google Scholar] [CrossRef]
- Hendricks, C.; Lansford, J.E.; Deater-Deckard, K.; Bornstein, M.H. Associations between child disabilities and caregiver discipline and violence in low-and middle-income countries. Child Dev. 2014, 85, 513–531. [Google Scholar] [CrossRef]
- Al-Farsi, O.A.; Al-Farsi, Y.M.; Al-Sharbati, M.M.; Al-Adawi, S. Stress, anxiety, and depression among parents of children with autism spectrum disorder in Oman: A case–control study. Neuropsychiatr. Dis. Treat. 2016, 12, 1943. [Google Scholar] [CrossRef] [Green Version]
- Kennan, M.D.; Brady, B.; Forkan, C. Children’s Participation A Systematic Literature Review Exploring the Effectiveness of Structures and Procedures Intended to Support Children’s Participation in Child Welfare, Child Protection; UNESCO Child and Family Research Centre (UCFRC), The National University of Ireland: Galway, Ireland, 2016. [Google Scholar]
- Lovell, B.; Elliot, H.; Liu, C.C.S.; Wetherell, M.A. Memory failures for everyday tasks in caregivers of children with autism. Res. Dev. Disabil. 2014, 35, 3057–3061. [Google Scholar] [CrossRef]
- Gallagher, S.; Phillips, A.C.; Oliver, C.; Carroll, D. Predictors of psychological morbidity in parents of children with intellectual disabilities. J. Pediatr. Psychol. 2008, 33, 1129–1136. [Google Scholar] [CrossRef] [Green Version]
- Osborne, L.A.; Reed, P. The relationship between parenting stress and behavior problems of children with autistic spectrum disorders. Except. Child. 2009, 76, 54–73. [Google Scholar] [CrossRef]
- Lovell, B.; Elder, G.J.; Wetherell, M.A. Sleep disturbances and physical health problems in caregivers of children with ASD. Res. Dev. Disabil. 2021, 113, 103932. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Robledillo, N.; Moya-Albiol, L. Self-reported health and cortisol awakening response in parents of people with Asperger syndrome: The role of trait anger and anxiety, coping and burden. Psychol. Health 2013, 28, 1246–1264. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Whiteley, J. Social support is associated with blood pressure responses in parents caring for children with developmental disabilities. Res. Dev. Disabil. 2012, 33, 2099–2105. [Google Scholar] [CrossRef] [Green Version]
- Bella, G.P.; Garcia, M.C.; Spadari-Bratfisch, R.C. Salivary cortisol, stress, and health in primary caregivers (mothers) of children with cerebral palsy. Psychoneuroendocrinology 2011, 36, 834–842. [Google Scholar] [CrossRef]
- Whittaker, A.C.; Gallagher, S. Caregiving alters immunity and stress hormones: A review of recent research. Curr. Opin. Behav. Sci. 2019, 28, 93–97. [Google Scholar] [CrossRef]
- Lovell, B.; Moss, M.; Wetherell, M.A. With a little help from my friends: Psychological, endocrine and health corollaries of social support in parental caregivers of children with autism or ADHD. Res. Dev. Disabil. 2012, 33, 682–687. [Google Scholar] [CrossRef]
- Seltzer, M.M.; Greenberg, J.S.; Hong, J.; Smith, L.E.; Almeida, D.M.; Coe, C.; Stawski, R.S. Maternal cortisol levels and behavior problems in adolescents and adults with ASD. J. Autism Dev. Disord. 2010, 40, 457–469. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, S.; Phillips, A.C.; Drayson, M.T.; Carroll, D. Parental caregivers of children with developmental disabilities mount a poor antibody response to pneumococcal vaccination. Brain Behav. Immun. 2009, 23, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Pulopulos, M.M.; Hidalgo, V.; Puig-Perez, S.; Montoliu, T.; Salvador, A. Relationship between cortisol changes during the night and subjective and objective sleep quality in healthy older people. Int. J. Environ. Res. Public Health 2020, 17, 1264. [Google Scholar] [CrossRef] [Green Version]
- Shattuck, N.L.; Matsangas, P.; Dahlman, A.S. Sleep and fatigue issues in military operations. In Sleep and Combat-Related Post Traumatic Stress Disorder; Springer: Cham, Switzerland, 2018; pp. 69–76. [Google Scholar]
- Paiva, T.; Gaspar, T.; Matos, M.G. Sleep deprivation in adolescents: Correlations with health complaints and health-related quality of life. Sleep Med. 2015, 16, 521–527. [Google Scholar] [CrossRef]
- Pawl, J.D.; Lee, S.Y.; Clark, P.C.; Sherwood, P.R. Sleep loss and its effects on health of family caregivers of individuals with primary malignant brain tumors. Res. Nurs. Health 2013, 36, 386–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcbean, A.L.; Schlosnagle, L. Sleep, health and memory: Comparing parents of typically developing children and parents of children with special health-care needs. J. Sleep Res. 2016, 25, 78–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Crain, T.L.; McHale, S.M.; Almeida, D.M.; Buxton, O.M. Daily antecedents and consequences of nightly sleep. J. Sleep Res. 2017, 26, 498–509. [Google Scholar] [CrossRef]
- Bourke-Taylor, H.; Pallant, J.F.; Law, M.; Howie, L. Relationships between sleep disruptions, health and care responsibilities among mothers of school-aged children with disabilities. J. Paediatr. Child Health 2013, 49, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Maternal stress, well-being, and impaired sleep in mothers of children with developmental disabilities: A literature review. Res. Dev. Disabil. 2013, 34, 4255–4273. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Moore, M. Sleep disruptions in parents of children and adolescents with chronic illnesses: Prevalence, causes, and consequences. J. Pediatr. Psychol. 2008, 33, 279–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Conduit, R.; Lockley, S.W.; Rajaratnam, S.M.; Cornish, K.M. The relationship between sleep and behavior in autism spectrum disorder (ASD): A review. J. Neurodev. Disord. 2014, 6, 44. [Google Scholar] [CrossRef] [Green Version]
- Malow, B.A.; Marzec, M.L.; McGrew, S.G.; Wang, L.; Henderson, L.M.; Stone, W.L. Characterizing sleep in children with autism spectrum disorders: A multidimensional approach. Sleep 2006, 29, 1563–1571. [Google Scholar] [CrossRef] [Green Version]
- Veatch, O.J.; Sutcliffe, J.S.; Warren, Z.E.; Keenan, B.T.; Potter, M.H.; Malow, B.A. Shorter sleep duration is associated with social impairment and comorbidities in ASD. Autism Res. 2017, 10, 1221–1238. [Google Scholar] [CrossRef]
- Cortesi, F.; Giannotti, F.; Ivanenko, A.; Johnson, K. Sleep in children with autistic spectrum disorder. Sleep Med. 2010, 11, 659–664. [Google Scholar] [CrossRef]
- Gregory, A.M.; O’connor, T.G. Sleep problems in childhood: A longitudinal study of developmental change and association with behavioral problems. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Law, R.; Clow, A. Stress, the cortisol awakening response and cognitive function. Int. Rev. Neurobiol. 2020, 150, 187–217. [Google Scholar] [PubMed]
- Tsui, A.; Richards, M.; Singh-Manoux, A.; Udeh-Momoh, C.; Davis, D. Longitudinal associations between diurnal cortisol variation and later-life cognitive impairment. Neurology 2020, 94, e133–e141. [Google Scholar] [CrossRef] [Green Version]
- Ennis, G.E.; Moffat, S.D.; Hertzog, C. The cortisol awakening response and cognition across the adult lifespan. Brain Cogn. 2016, 105, 66–77. [Google Scholar] [CrossRef] [Green Version]
- Engle, P.; Black, M.; Behrman, J.; de Mello, M.; Gertler, P.; Kapiriri, L.; Martorell, R.; Young, M.E.; The International Child Development Steering Group. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 369, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Bech, P.; Rasmussen, N.A.; Olsen, L.R.; Noerholm, V.; Abildgaard, W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J. Affect. Disord. 2001, 66, 159–164. [Google Scholar] [CrossRef]
- Schopler, E.; Reichler, R.J.; Renner, B.R. The Childhood Autism Rating Scale (CARS); WPS Los Angeles: Torrance, CA, USA, 2010. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep N. Y. 2000, 23, 1043–1052. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Dement, W.C. Monitoring and Staging human sleep. In Principles and Practice of Sleep Medicine, 5th ed.; Kryger, M.H., Roth, T., Dement, W.C., Eds.; Elsevier Saunders: St. Louis, MI, USA, 2011; pp. 16–26. [Google Scholar]
- Cotton, S.; Richdale, A. Brief report: Parental descriptions of sleep problems in children with autism, Down syndrome, and Prader–Willi syndrome. Res. Dev. Disabil. 2006, 27, 151–161. [Google Scholar] [CrossRef]
- Krakowiak, P.; Goodlin-Jones, B.; Hertz-Picciotto, I.; Croen, L.A.; Hansen, R.L. Sleep problems in children with autism spectrum disorders, developmental delays, and typical development: A population-based study. J. Sleep Res. 2008, 17, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.; Do, T.N.T.; Harrison, L.; Marczak, M.; Dimitriou, D.; Joyce, A. Sleep and cognition in people with autism spectrum condition: A systematic literature review. Rev. J. Autism Dev. Disord. 2021, 1–11. [Google Scholar] [CrossRef]
- Couturier, J.L.; Speechley, K.N.; Steele, M.; Norman, R.; Stringer, B.; Nicolson, R. Parental perception of sleep problems in children of normal intelligence with pervasive developmental disorders: Prevalence, severity, and pattern. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Wiggs, L.; Stores, G. Sleep patterns and sleep disorders in children with autistic spectrum disorders: Insights using parent report and actigraphy. Dev. Med. Child Neurol. 2004, 46, 372–380. [Google Scholar] [CrossRef]
- Allik, H.; Larsson, J.O.; Smedje, H. Sleep patterns of school-age children with Asperger syndrome or high-functioning autism. J. Autism Dev. Disord. 2006, 36, 585–595. [Google Scholar] [CrossRef]
- Honomichl, R.D.; Goodlin-Jones, B.L.; Burnham, M.; Gaylor, E.; Anders, T.F. Sleep patterns of children with pervasive developmental disorders. J. Autism Dev. Disord. 2002, 32, 553–561. [Google Scholar] [CrossRef]
- Patzold, L.; Richdale, A.; Tonge, B. An investigation into sleep characteristics of children with autism and Asperger’s disorder. J. Paediatr. Child Health 1998, 34, 528–533. [Google Scholar] [CrossRef]
- Schreck, K.A.; Mulick, J.A. Parental report of sleep problems in children with autism. J. Autism Dev. Disord. 2000, 30, 127–135. [Google Scholar] [CrossRef]
- Polimeni, M.A.; Richdale, A.; Francis, A. A survey of sleep problems in autism, Asperger’s disorder and typically developing children. J. Intellect. Disabil. Res. 2005, 49, 260–268. [Google Scholar] [CrossRef]
- Hering, E.; Epstein, R.; Elroy, S.; Iancu, D.R.; Zelnik, N. Sleep patterns in autistic children. J. Autism Dev. Disord. 1999, 29, 143–147. [Google Scholar] [CrossRef]
- Richdale, A.L.; Prior, M.R. The sleep/wake rhythm in children with autism. Eur. Child Adolesc. Psychiatry 1995, 4, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, C.D.; Sweeney, D.P.; Gilliam, J.E.; Apodaca, D.D.; Lopez-Wagner, M.C.; Castillo, M.M. Sleep problems and symptomology in children with autism. Focus Autism Other Dev. Disabil. 2005, 20, 194–200. [Google Scholar] [CrossRef]
- Schreck, K.A.; Richdale, A.L. Sleep problems, behavior, and psychopathology in autism: Inter-relationships across the lifespan. Curr. Opin. Psychol. 2020, 34, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Richdale, A.L.; Schreck, K.A. Sleep problems in autism spectrum disorders: Prevalence, nature, & possible biopsychosocial aetiologies. Sleep Med. Rev. 2009, 13, 403–411. [Google Scholar] [PubMed]
- Tzischinsky, O.; Meiri, G.; Manelis, L.; Bar-Sinai, A.; Flusser, H.; Michaelovski, A.; Zivan, O.; Ilan, M.; Faroy, M.; Menashe, I.; et al. Sleep disturbances are associated with specific sensory sensitivities in children with autism. Mol. Autism 2018, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Hundley, R.J.; Shui, A.; Malow, B.A. Relationship between subtypes of restricted and repetitive behaviors and sleep disturbance in autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 3448–3457. [Google Scholar] [CrossRef]
- Lopez-Wagner, M.C.; Hoffman, C.D.; Sweeney, D.P.; Hodge, D.; Gilliam, J.E. Sleep problems of parents of typically developing children and parents of children with autism. J. Genet. Psychol. 2008, 169, 245–260. [Google Scholar] [CrossRef]
- Uskul, A.K.; Greenglass, E. Psychological wellbeing in a Turkish-Canadian sample. Anxiety Stress Coping 2005, 18, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, L.J.; Mindell, J.A. Relationship between child sleep disturbances and maternal sleep, mood, and parenting stress: A pilot study. J. Fam. Psychol. 2007, 21, 67. [Google Scholar] [CrossRef]
- Robinson, A.; Richdale, A. Sleep problems in children with an intellectual disability: Parental perceptions of sleep problems, and views of treatment effectiveness. Child Care Health Dev. 2004, 30, 139–150. [Google Scholar] [CrossRef]
- Sivertsen, B.; Harvey, A.G.; Pallesen, S.; Hysing, M. Trajectories of sleep problems from childhood to adolescence: A population-based longitudinal study from Norway. J. Sleep Res. 2017, 26, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Isensee, C.; Becker, A.; Wong, J.; Eastwood, P.R.; Huang, R.C.; Runions, K.C.; Stewart, R.M.; Meyer, T.; Brüni, L.; et al. Developmental trajectories of sleep problems from childhood to adolescence both predict and are predicted by emotional and behavioral problems. Front. Psychol. 2016, 7, 1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McVeigh, J.A.; Smith, A.; Howie, E.K.; Stamatakis, E.; Ding, D.; Cistulli, P.A.; Eastwood, P.; Straker, L. Developmental trajectories of sleep during childhood and adolescence are related to health in young adulthood. Acta Paediatr. 2021, 110, 2435–2444. [Google Scholar] [CrossRef] [PubMed]
- Abidin, R.R. Parenting Stress Index: Professional Manual; [PSI]; PAR, Psychological Assessment Resources: Odesssa, FL, USA, 1995. [Google Scholar]
- Crowne, D.P.; Marlowe, D. A new scale of social desirability independent of psychopathology. J. Consult. Psychol. 1960, 24, 349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strahan, R.; Gerbasi, K.C. Short, homogeneous versions of the Marlowe-Crowne social desirability scale. J. Clin. Psychol. 1972, 28, 191–193. [Google Scholar] [CrossRef]
- Liu, D.; Liu, S.; Liu, X.; Zhang, C.; Li, A.; Jin, C.; Chen, Y.; Wang, H.; Zhang, X. Interactive brain activity: Review and progress on EEG-based hyperscanning in social interactions. Front. Psychol. 2018, 9, 1862. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, F.; Cincotti, F.; Mattia, D.; Mattiocco, M.; Fallani, F.D.V.; Tocci, A.; Bianchi, L.; Marciani, M.G.; Astolfi, L. Hypermethods for EEG hyperscanning. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 3666–3669. [Google Scholar]
- Feldman, R. From biological rhythms to social rhythms: Physiological precursors of mother-infant synchrony. Dev. Psychol. 2006, 42, 175. [Google Scholar] [CrossRef] [Green Version]
- Oliver, P.; Jupp, V. Snowball Sampling; Sage: London, UK, 2006. [Google Scholar]


{kind=link}
| PSQI Subscale | Very Good/No. (%) | Fairly Good/No. (%) | Fairly Bad/No. (%) | Very Bad/No. (%) |
|---|---|---|---|---|
| Subjective Sleep Quality | 6 (20.7) | 7 (24.1) | 12 (41.4) | 4 (13.8) |
| Sleep Onset Latency | 5 (17.2) | 7 (24.1) | 11 (37.9) | 6 (20.7) |
| Sleep Duration | 7 (24.1) | 10 (34.5) | 7 (24.1) | 5 (17.2) |
| Habitual Sleep Efficiency | 16 (55.2) | 3 (10.3) | 7 (24.1) | 3 (10.3) |
| Sleep Disturbance | 0 (0.0) | 9 (31.0) | 20 (69.0) | 0 (0.0) |
| Use of Sleeping Medication | 11 (37.9) | 5 (17.2) | 1 (3.4) | 2 (6.8) |
| Daytime Dysfunction | 16 (55.2) | 8 (27.6) | 4 (13.8) | 1 (3.4) |
| CSHQ Subscale (Theoretical Range) | Mean (SD) | 95% Confidence Interval |
|---|---|---|
| Bedtime Resistance (6–18) | 9.66 (3.35) | [8.38, 10.93] |
| Daytime Sleepiness (7–24) | 13.79 (4.48) | [12.09, 15.50] |
| Night Wakings (3–9) | 4.69 (1.97) | [3.94, 5.44] |
| Sleep Anxiety (4–12) | 6.93 (2.70) | [5.90, 7.96] |
| Sleep Disordered Breathing (3–14) | 7 (3.72) | [5.88, 8.42] |
| Sleep Duration (4–9) | 6.03 (2.03) | [5.26, 6.81] |
| Sleep Onset (1–3) | 2.10 (0.82) | [1.79, 2.42] |
| Parasomnias (3–11) | 5.14 (1.88) | [4.42, 5.85] |
| Cortisol Measure | Mean (SD) | Range | 95% Confidence Interval |
|---|---|---|---|
| Average Cortisol/nM | 2.93 (2.02) | 0.65–8.37 | [2.14, 3.72] |
| Morning (within 30 min of waking)/nM | 5.60 (5.26) | 0.6–22.82 | [3.56, 7.64] |
| Afternoon (4 p.m.)/nM | 1.63 (1.08) | 0.5–5.2 | [1.21, 2.05] |
| Before Habitual Sleep/nM | 1.56 (1.43) | 0.4–7.85 | [1.00, 2.12] |
| Normalised Afternoon/% | 59.62 (83.35) | 6.62–451.52 | [27.30, 91.95] |
| Normalised Bedtime/% | 52.84 (51.30) | 3.42–221.57 | [32.95, 72.73] |
| AUCi | 15.63 (10.04) | 3.93–36.00 | [11.74, 19.53] |
| AUCg | −17.97 (23.26) | −96.99–10.74 | [−26.99, −8.95] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin Eid, W.; Lim, M.; Gabrieli, G.; Kölbel, M.; Halstead, E.; Esposito, G.; Dimitriou, D. Alterations in Cortisol Profiles among Mothers of Children with ASD Related to Poor Child Sleep Quality. Healthcare 2022, 10, 666. https://doi.org/10.3390/healthcare10040666
Bin Eid W, Lim M, Gabrieli G, Kölbel M, Halstead E, Esposito G, Dimitriou D. Alterations in Cortisol Profiles among Mothers of Children with ASD Related to Poor Child Sleep Quality. Healthcare. 2022; 10(4):666. https://doi.org/10.3390/healthcare10040666
Chicago/Turabian StyleBin Eid, Wasmiah, Mengyu Lim, Giulio Gabrieli, Melanie Kölbel, Elizabeth Halstead, Gianluca Esposito, and Dagmara Dimitriou. 2022. "Alterations in Cortisol Profiles among Mothers of Children with ASD Related to Poor Child Sleep Quality" Healthcare 10, no. 4: 666. https://doi.org/10.3390/healthcare10040666