
Preventable Adverse Events in Obstetrics—Systemic Assessment of Their Incidence and Linked Risk Factors

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Evaluation of the pAE Categories
3.2. Risk Factors as Triggers of pAE
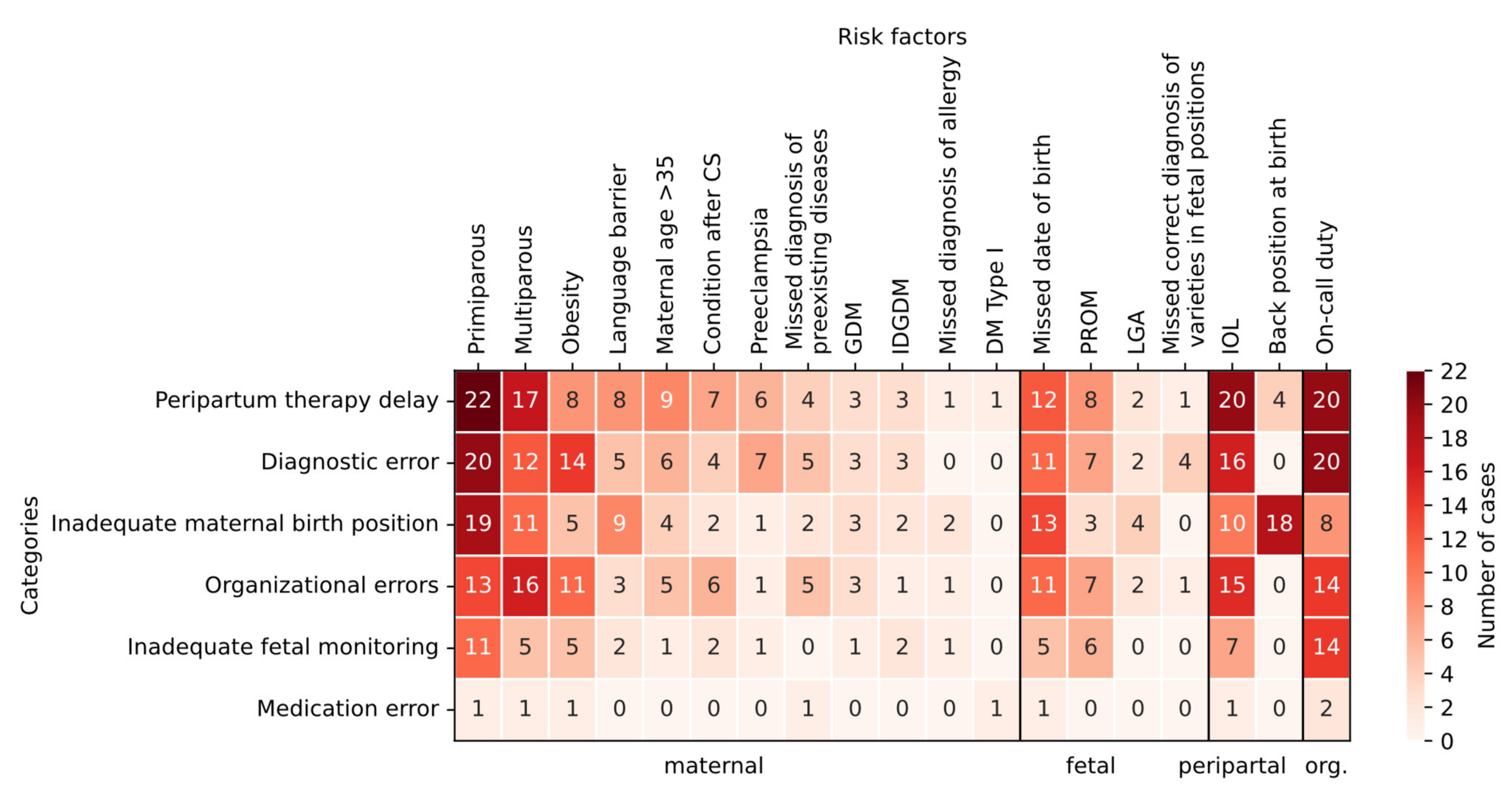
3.3. Cross-Tabulation of Risk Factors with pAE
4. Discussion
4.1. Operationalization of Preventability
4.2. Systematic Recording of Serious Incidents
4.3. Evaluation of Adverse Events from Clinical Risk Management
4.4. Risk Factor Analysis
4.5. Care Management Problems
4.6. Prospective Analysis
4.7. Resilient Health Care
4.8. Recommendations for Error Prevention
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kohn, L.T.; Corrigan, J.; Donaldson, M.S. To Err Is Human: Building a Safer Health System; National Academy Press: Washington, DC, USA, 2000; p. 287. [Google Scholar]
- The World Alliance For Patient Safety Drafting Group; Sherman, H.; Castro, G.; Fletcher, M.; Hatlie, M.; Hibbert, P.; Jakob, R.; Koss, R.; Lewalle, P.; Loeb, J.; et al. Towards an International Classification for Patient Safety: The conceptual framework. Int. J. Qual. Health Care 2009, 21, 2–8. [Google Scholar] [PubMed] [Green Version]
- Brennan, T.A.; Leape, L.L.; Laird, N.M.; Hebert, L.; Localio, A.R.; Lawthers, A.G.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H.H. Incidence of Adverse Events and Negligence in Hospitalized Patients. New Engl. J. Med. 1991, 324, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrappe, M.; Müller, H.; Hecker, R. Patient safety: Current problems and challenges. Internist 2020, 61, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, J.; Wears, R.L.; Hollnagel, E. Resilient health care: Turning patient safety on its head. Int. J. Qual. Health Care 2015, 27, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Aibar, L.; Rabanaque, M.J.; Aibar, C.; Aranaz, J.M.; Mozas, J. Patient safety and adverse events related with obstetric care. Arch. Gynecol. Obstet. 2014, 291, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.J.; Fung, I.; Caughey, S.; Oppenheimer, L.; Beach, C.; Shojania, K.G.; van Walraven, C. Adverse Events Detected by Clinical Surveillance on an Obstetric Service. Obstet. Gynecol. 2006, 108, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Pettker, C.M.; Thung, S.F.; Norwitz, E.R.; Buhimschi, C.S.; Raab, C.A.; Copel, J.A.; Kuczynski, E.; Lockwood, C.J.; Funai, E.F. Impact of a comprehensive patient safety strategy on obstetric adverse events. Am. J. Obstet. Gynecol. 2009, 200, 492.e1–492.e8. [Google Scholar] [CrossRef] [PubMed]
- White, A.; Pichert, J.W.; Bledsoe, S.H.; Irwin, C.; Entman, S.S. Cause and Effect Analysis of Closed Claims in Obstetrics and Gynecology. Obstet. Gynecol. 2005, 105, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- U.S Department of Health & Human Services. AHRQ Quality Indicators [Internet]. Available online: https://www.qualityindicators.ahrq.gov/ (accessed on 16 January 2021).
- National Quality Forum. NQF Endorses Perinatal Measures [Internet]. Available online: https://www.qualityforum.org/News_And_Resources/Press_Releases/2012/NQF_Endorses_Perinatal_Measures.aspx (accessed on 16 January 2021).
- The Joint Commission. Specification Manuals [Internet]. 2016. Available online: https://www.jointcommission.org/measurement/specification-manuals (accessed on 16 January 2021).
- Vincent, C.; Taylor-Adams, S.; Chapman, E.J.; Hewett, D.; Prior, S.; Strange, P.; Tizzard, A. How to investigate and analyse clinical incidents: Clinical Risk Unit and Association of Litigation and Risk Management protocol. BMJ 2000, 320, 777–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakasing, L.; Spencer, J.A.D. Care management problems on the labour ward: 5 years’ experience of clinical risk management. J. Obstet. Gynaecol. 2002, 22, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.; Lay-Yee, R.; Briant, R.; Ali, W.; Scott, A.; Schug, S. Adverse events in New Zealand public hospitals II: Preventability and clinical context. N. Z. Med. J. 2003, 116, 624. [Google Scholar]
- Pettker, C.M. Systematic approaches to adverse events in obstetrics, Part I: Event identification and classification. Semin. Perinatol. 2017, 41, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Michel, P.; Quenon, J.L.; De Sarasqueta, A.M.; Scemama, O. Comparison of three methods for estimating rates of adverse events and rates of preventable adverse events in acute care hospitals. BMJ 2004, 328, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippke, S.; Wienert, J.; Keller, F.M.; Derksen, C.; Welp, A.; Kötting, L.; Hofreuter-Gätgens, K.; Müller, H.; Louwen, F.; Weigand, M.; et al. Communication and patient safety in gynecology and obstetrics - study protocol of an intervention study. BMC Health Serv. Res. 2019, 19, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettker, C.M. Systematic approaches to adverse events in obstetrics, Part II: Event analysis and response. Semin. Perinatol. 2017, 41, 156–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagrew, D.C.; Jenkins, T.R. The future of obstetrics/gynecology in 2020: A clearer vision. Why is change needed? Am. J. Obstet. Gynecol. 2014, 211, 470–474.e1. [Google Scholar] [CrossRef] [PubMed]
- Hollnagel, E.; Wears, R.L.; Braithwaite, J. From Safety-I to Safety-II: A White Paper. Available online: https://psnet.ahrq.gov/issue/safety-i-safety-ii-white-paper (accessed on 16 January 2021).
- Koch, P.; Zilezinski, M.; Schulte, K.; Strametz, R.; Nienhaus, A.; Raspe, M. How Perceived Quality of Care and Job Satisfaction Are Associated with Intention to Leave the Profession in Young Nurses and Physicians. Int. J. Environ. Res. Public Health 2020, 17, 2714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institut für Qualitätssicherung und Transparenz im Gesundheitswesen. IQTIG: Perinatalmedizin. Available online: https://iqtig.org/qs-verfahren/peri/ (accessed on 17 January 2021).
- Iflaifel, M.; Lim, R.H.; Ryan, K.; Crowley, C. Resilient Health Care: A systematic review of conceptualisations, study methods and factors that develop resilience. BMC Health Serv. Res. 2020, 20, 324. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.W. Medical error: The second victim. The doctor who makes the mistake needs help too. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Schmiedhofer, M.; Derksen, C.; Keller, F.; Dietl, J.; Häussler, F.; Strametz, R.; Koester-Steinebach, I.; Lippke, S. Barriers and Facilitators of Safe Communication in Obstetrics: Results from Qualitative Interviews with Physicians, Midwives and Nurses. Int. J. Environ. Res. Public Health 2021, 18, 915. [Google Scholar] [CrossRef] [PubMed]
- The Federal Joint Committee [Internet]. Available online: https://www.g-ba.de/downloads/17-98-2804/2018-12-04_G-BA_Flyer_Der_Gemeinsame_Bundesausschuss_EN_bf.pdf (accessed on 31 December 2021).


{kind=link}
| Category | Adverse Event (AE) | Definition/Further Operationalization |
|---|---|---|
| Maternal | Allergy | |
| Anemia | Hb < 8 mg/dL | |
| Postpartum length of stay | >3 days after vaginal birth | |
| Blood loss | >1000 mL | |
| Diabetic ketoacidosis | ||
| Disseminated intravascular coagulation (DIC) | ||
| Eclampsia | ||
| Electrolyte derailment | ||
| Fever | >38.5 °C | |
| Labor arrest | Cesarean section necessary | |
| Hypertension | >180/110 mmHg | |
| Hypotension | <90/60 mmHg | |
| Infection | Treatment with antibiotics | |
| Intubation * | ||
| Seizures | ||
| Manual placenta detachment | Non-delivered placenta | |
| Placental tissue after cesarean section | Curettage necessary | |
| Third degree laceration | ||
| Fourth degree laceration | ||
| Other laceration | Vaginal, perineal, labia | |
| Thyroid crisis | ||
| Death | ||
| Precipitate delivery | ||
| Unrecognized maternal disease | ||
| Unexpected re-admission | ||
| Uterine rupture | ||
| Prolonged second stage | >120 min | |
| Transmission to intensive care unit* | ||
| Placental abruption | ||
| Wound healing disorder | ||
| Fetal | Near-SIDS | Near Sudden Infant Death Syndrome |
| APGAR | 1 min APGAR < 7 | |
| Acidosis | Cord pH < 7.1 or base excess < −12 | |
| Bradycardia | FHF < 60 | |
| Birth trauma | Fracture | |
| Seizures | ||
| Meconium aspiration | ||
| Umbilical cord prolapses | ||
| Death | ||
| Shoulder dystocia | ||
| Unplanned admission to intensive care unit * | ||
| Interventional | Transfusion | |
| Failed anesthesia | ||
| Failed instrumental vaginal delivery | Cesarean section necessary | |
| Failed induction of labor | Cesarean section necessary | |
| Communication problem | ||
| Emergency hysterectomy | ||
| Emergency cesarean section | ||
| Unplanned cesarean section | ||
| Use of more than 1 instrument in vaginal delivery | ||
| Delayed intervention in case of pathological CTG | Decision-delivery time > 30 min | |
| Delayed intervention in case of postpartum hemorrhage (PPH) | ||
| Cesarean section on request | No medical indication | |
| Organizational | Incomplete documentation | |
| Medication errors | ||
| Communication problems |
| Category pAE | Cases | Proportion from n = 88 Cases |
|---|---|---|
| Peripartum therapy delay | 39 | 44.32% |
| Diagnostic error | 32 | 36.36% |
| Inadequate maternal birth position | 30 | 34.09% |
| Organizational errors | 29 | 32.95% |
| Inadequate fetal monitoring | 16 | 18.18% |
| Medication error | 2 | 2.27% |
| Risk Factors | Cases | Proportion | Category |
|---|---|---|---|
| Primiparous | 49 | 55.68% | Maternal |
| Multiparous (defined as two births or more) | 39 | 44.32% | Maternal |
| On-call duty | 39 | 44.32% | Organizational |
| Induction of labor (IOL) | 38 | 43.18% | Peripartal |
| Missed date of birth | 31 | 35.23% | Fetal |
| Obesity | 21 | 23.86% | Maternal |
| Premature rupture of membranes (PROM) | 19 | 21.59% | Fetal |
| Back position at birth | 18 | 20.45% | Peripartal |
| Language barrier | 18 | 20.45% | Maternal |
| Maternal age > 35 | 15 | 17.05% | Maternal |
| Condition after cesarean section (CS) | 12 | 13.64% | Maternal |
| Preeclampsia | 9 | 10.23% | Maternal |
| Missed diagnosis of preexisting diseases | 8 | 9.09% | Maternal |
| Gestational diabetes (GDM) | 7 | 7.95% | Maternal |
| Large for gestational age (LGA) | 6 | 6.82% | Fetal |
| Insulin-dependent gestational diabetes (IDGDM) | 5 | 5.68% | Maternal |
| Missed correct diagnosis of varieties in fetal positions | 4 | 4.55% | Fetal |
| Missed diagnosis of allergy | 3 | 3.41% | Maternal |
| Diabetes mellitus (DM) type I | 1 | 1.14% | Maternal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hüner, B.; Derksen, C.; Schmiedhofer, M.; Lippke, S.; Janni, W.; Scholz, C. Preventable Adverse Events in Obstetrics—Systemic Assessment of Their Incidence and Linked Risk Factors. Healthcare 2022, 10, 97. https://doi.org/10.3390/healthcare10010097
Hüner B, Derksen C, Schmiedhofer M, Lippke S, Janni W, Scholz C. Preventable Adverse Events in Obstetrics—Systemic Assessment of Their Incidence and Linked Risk Factors. Healthcare. 2022; 10(1):97. https://doi.org/10.3390/healthcare10010097
Chicago/Turabian StyleHüner, Beate, Christina Derksen, Martina Schmiedhofer, Sonia Lippke, Wolfgang Janni, and Christoph Scholz. 2022. "Preventable Adverse Events in Obstetrics—Systemic Assessment of Their Incidence and Linked Risk Factors" Healthcare 10, no. 1: 97. https://doi.org/10.3390/healthcare10010097