Mobile Applications for Assessing Human Posture: A Systematic Literature Review

 ,
,  , , , , , , ,
, , , , , , ,  , and
, and
Abstract
:1. Introduction
2. Background
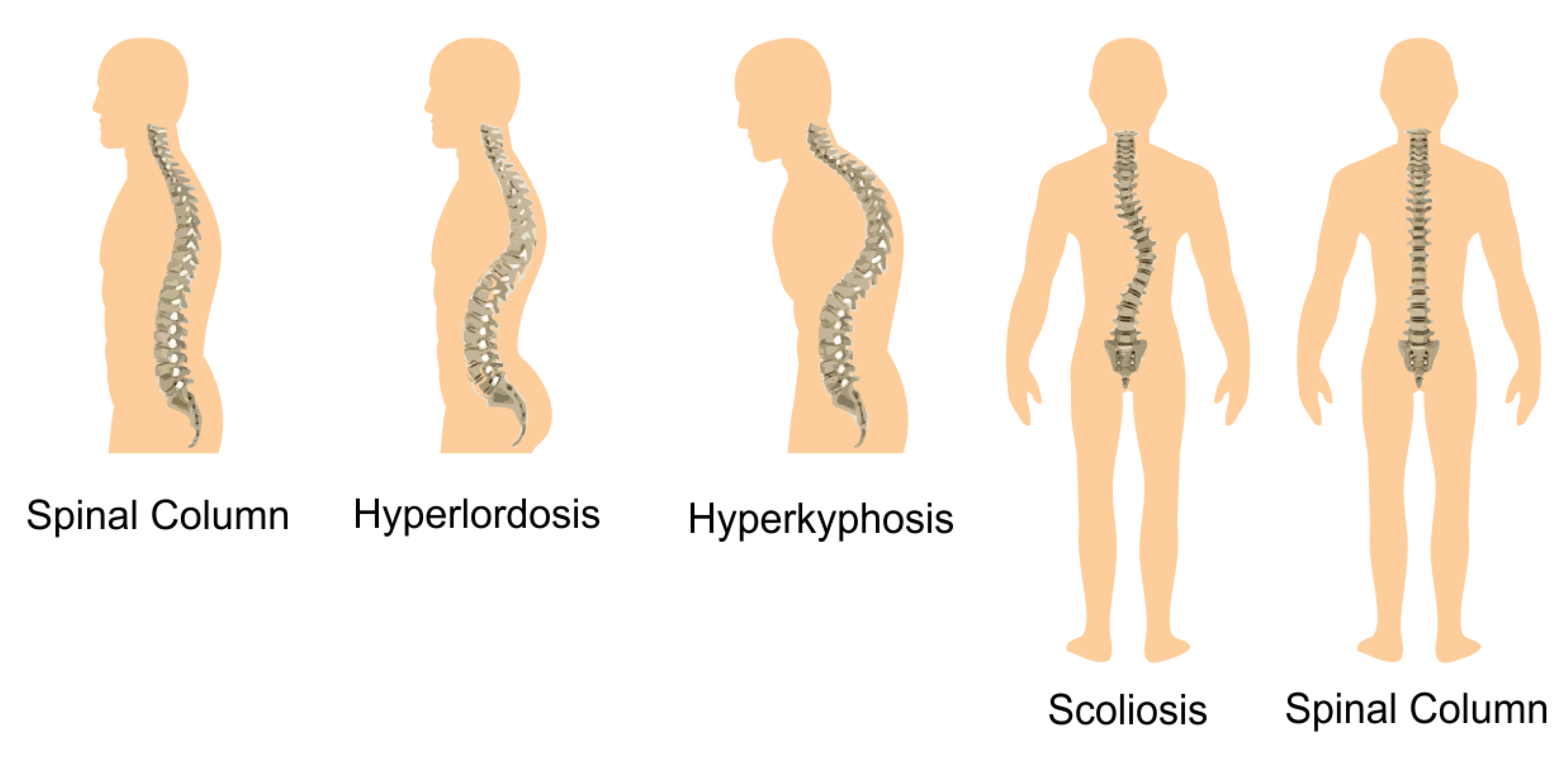
2.1. Postural Deviations
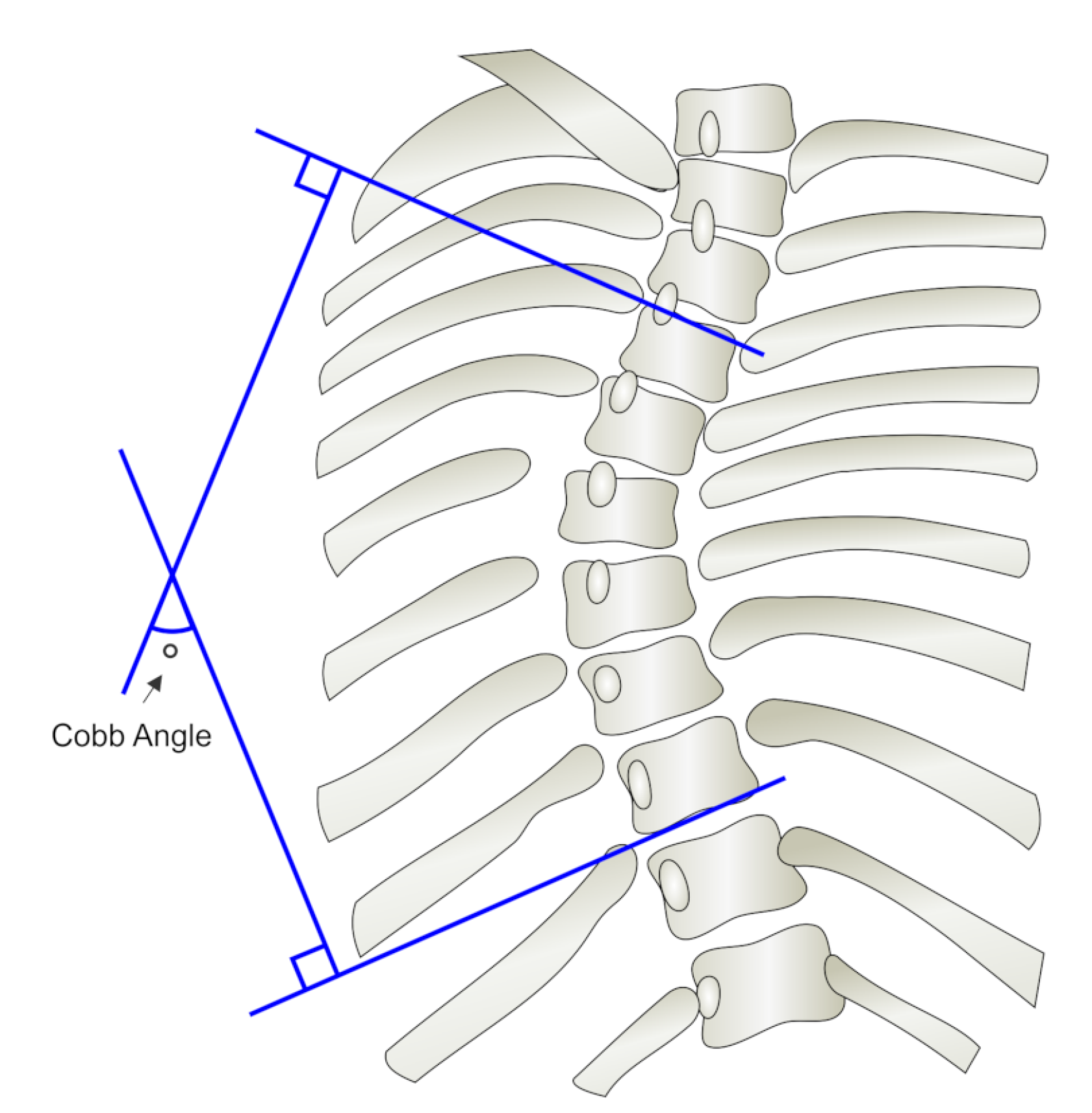
2.2. Methods for Assessing Human Posture Deviations
3. Research Methodology
3.1. Research Questions
3.2. Search Strategy
3.3. Selection Criteria
3.4. Quality Assessment
3.5. Data Extraction
3.6. Review Conduction
4. Results
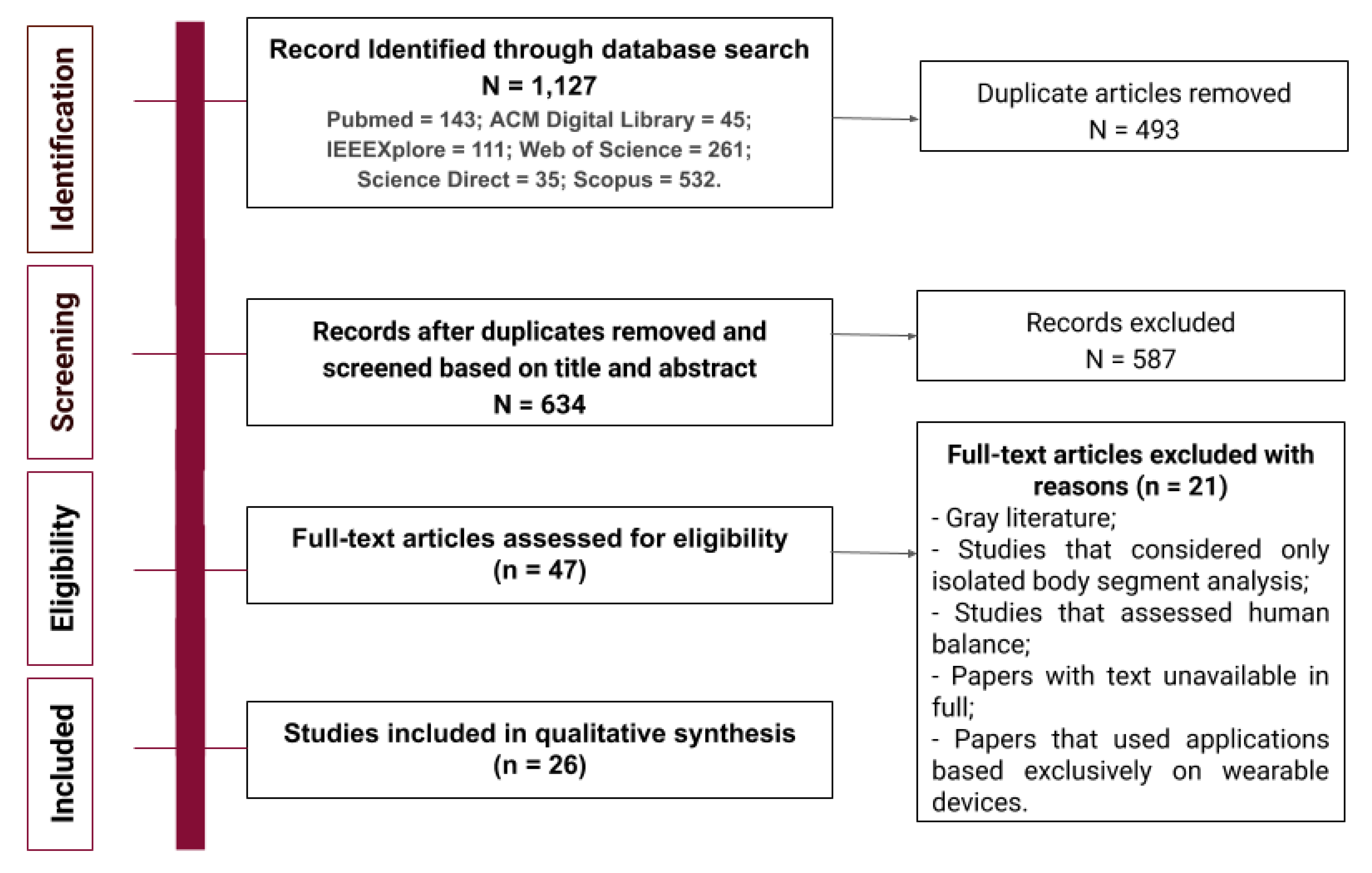
4.1. Study Selection
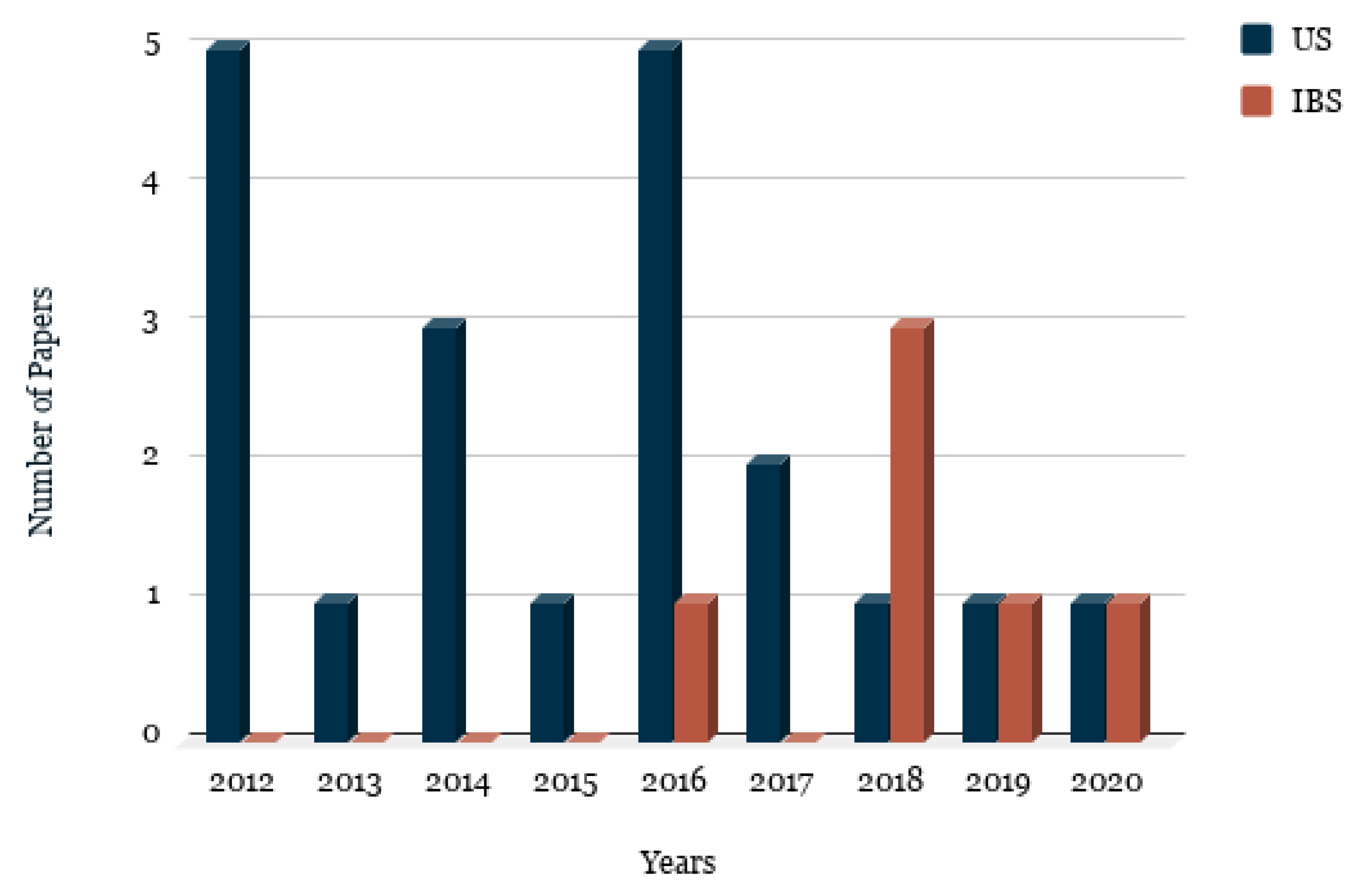
4.2. Study Characterization
4.3. Technical Features
4.4. Study Design and Performance of the Mobile Applications
4.5. Quality Scoring
5. Discussion
5.1. Analysis of Results
5.2. Open Issues and Implications for Further Investigation
5.3. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIS | Adolescent Idiopathic Scoliosis |
| DATs | Digital Assessment Tools |
| DIPA | Digital Image-Based Postural Assessment Software |
| ER | Evaluation Research |
| IBS | Image-Based Solution |
| ICC | Intra-Class Correlation Coefficient |
| kNN | k-Nearest Neighbors |
| LL | Lumbar Lordosis |
| L1 | First lumbar vertebra |
| MATs | Manual Assessment Tools |
| MeSH | Medical Subject Headings |
| mHealth | Mobile Health |
| MLP | Multilayer Perceptron |
| MSE | Mean Squared Error |
| NMSE | Normalized Mean Squared Error |
| PACS | Picture Archiving and Communication System |
| PI | Pelvic Incidence |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PSM | PostureScreen Mobile |
| PS | Proposal of Solution |
| PT | Pelvic Tilt |
| QQs | Quality Questions |
| RQ | Research Questions |
| SD | Standard Deviation |
| PAS | Posture Assessment Software |
| SATs | Software-Aided Assessment Tools |
| SLRs | Systematic Literature Reviews |
| SLR | Systematic Literature Review |
| SS | Sacral Slope |
| SVM | Support-Vector Machines |
| S1 | First sacral vertebra |
| US | Use of Sensors |
| VR | Validation Research |
References
- Saponara, S.; Donati, M.; Fanucci, L.; Celli, A. An Embedded Sensing and Communication Platform, and a Healthcare Model for Remote Monitoring of Chronic Diseases. Electronics 2016, 5, 47. [Google Scholar] [CrossRef] [Green Version]
- Källander, K.; Tibenderana, J.K.; Akpogheneta, O.J.; Strachan, D.L.; Hill, Z.; Ten Asbroek, A.H.A.; Conteh, L.; Kirkwood, B.R.; Meek, S.R. Mobile Health (mHealth) Approaches and Lessons for Increased Performance and Retention of Community Health Workers in Low- and Middle-Income Countries: A Review. J. Med. Internet Res. 2013, 15, e17. [Google Scholar] [CrossRef] [PubMed]
- Claus, A.P.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Is ‘ideal’ sitting posture real?: Measurement of spinal curves in four sitting postures. Man. Ther. 2009, 14, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Hazar, Z.; Karabicak, G.O.; Tiftikci, U. Reliability of photographic posture analysis of adolescents. J. Phys. Ther. Sci. 2015, 27, 3123–3126. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Yang, F.; Lin, T.; Shao, W.; Meng, Y.; Ma, J.; Wang, C.; Gao, R.; Zhou, X. Asymmetric expression of H19 and ADIPOQ in concave/convex paravertebral muscles is associated with severe adolescent idiopathic scoliosis. Mol. Med. 2018, 24, 48. [Google Scholar] [CrossRef]
- Yau, M.S.; Demissie, S.; Zhou, Y.; Anderson, D.E.; Lorbergs, A.L.; Kiel, D.P.; Allaire, B.T.; Yang, L.; Cupples, L.A.; Travison, T.G.; et al. Heritability of Thoracic Spine Curvature and Genetic Correlations With Other Spine Traits: The Framingham Study. J. Bone Miner. Res. 2016, 31, 2077–2084. [Google Scholar] [CrossRef] [Green Version]
- Singla, D.; Veqar, Z. Methods of Postural Assessment Used for Sports Persons. J. Clin. Diagn. Res. 2014, 8, LE01–LE04. [Google Scholar] [CrossRef]
- Fok, K.L.; Lee, J.; Vette, A.H.; Masani, K. Kinematic error magnitude in the single-mass inverted pendulum model of human standing posture. Gait Posture 2018, 63, 23–26. [Google Scholar] [CrossRef]
- Rosario, J. Photographic analysis of human posture: A literature review. J. Bodyw. Mov. Ther. 2014, 18, 56–61. [Google Scholar] [CrossRef]
- Krawczky, B.; Pacheco, A.G.; Mainenti, M.R. A Systematic Review of the Angular Values Obtained by Computerized Photogrammetry in Sagittal Plane: A Proposal for Reference Values. J. Manip. Physiol. Ther. 2014, 37, 269–275. [Google Scholar] [CrossRef]
- Furlanetto, T.S.; Sedrez, J.A.; Candotti, C.T.; Loss, J.F. Photogrammetry as a tool for the postural evaluation of the spine: A systematic review. World J. Orthop. 2016, 7, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.; Veqar, Z.; Hussain, M.E. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J. Chiropr. Med. 2017, 16, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, L.; Kobayashi, S.; Simic, M.; Dennis, S.; Refshauge, K.; Pappas, E. Non-radiographic methods of measuring global sagittal balance: A systematic review. Scoliosis Spinal Disord. 2017, 12, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porto De Freitas Camelo, E.M.; Matias Uchôa, D.; Santos Júnior, F.; Brasileiro de Vasconcelos, T.; Macena, R. Use of softwares for posture assessment: Itegrative review. COluna Columna 2015, 14, 230. [Google Scholar] [CrossRef]
- Aroeira, R.M.C.; De Las Casas, E.B.; Pertence, A.E.M.; Greco, M.; Tavares, J.M.R.S. Non-invasive methods of computer vision in the posture evaluation of adolescent idiopathic scoliosis. J. Bodyw. Mov. Ther. 2016, 20, 832–843. [Google Scholar] [CrossRef] [Green Version]
- Prowse, A.; Pope, R.; Gerdhem, P.; Abbott, A. Reliability and validity of inexpensive and easily administered anthropometric clinical evaluation methods of postural asymmetry measurement in adolescent idiopathic scoliosis: A systematic review. Eur. Spine J. 2016, 25, 450–466. [Google Scholar] [CrossRef]
- Naziri, Q.; Detolla, J.; Hayes, W.; Burekhovich, S.; Merola, A.; Akamnanu, C.; Paulino, C. A Systematic Review of All Smart Phone Applications Specifically Aimed for Use as a Scoliosis Screening Tool. J. Long-Term Eff. Med. Implant. 2018, 28, 25–30. [Google Scholar] [CrossRef]
- Fon, G.T.; Pitt, M.J.; Thies, A.C. Thoracic kyphosis: Range in normal subjects. Am. J. Roentgenol. 1980, 134, 979–983. [Google Scholar] [CrossRef]
- Batista Junior, J.L.; Batista, P.R.d.; Barbosa, D.M.; Machado, I.C.; Rezende, R. Evaluation of cervical behavior in patients with scoliosis Lenke who underwent surgery. Coluna Columna 2011, 10, 231–233. [Google Scholar] [CrossRef]
- Harrison, D.; Janik, T.; Troyanovich, S.; Harrison, D.; Colloca, C. Evaluation of the assumptions used to derive an ideal normal cervical spine model. J. Manip. Physiol. Ther. 1997, 20, 246–256. [Google Scholar]
- Been, E.; Gómez-Olivencia, A.; Shefi, S.; Soudack, M.; Bastir, M.; Barash, A. Evolution of Spinopelvic Alignment in Hominins. Anat. Rec. 2017, 300, 900–911. [Google Scholar] [CrossRef] [Green Version]
- Mrozkowiak, M.; Walicka-Cupryś, K.; Magoń, G. Comparison of Spinal Curvatures in the Sagittal Plane, as Well as Body Height and Mass in Polish Children and Adolescents Examined in the Late 1950s and in the Early 2000s. Med. Sci. Monit. 2018, 24, 4489–4500. [Google Scholar] [CrossRef]
- Fedorak, C.; Ashworth, N.L.; Marshall, J.C.; Paull, H. Reliability of the visual assessment of cervical and lumbar lordosis: How good are we? Spine 2003, 28 16, 1857–1859. [Google Scholar] [CrossRef] [Green Version]
- Shirazi, S.A.; Haghighi, F.M.; Alavi, S.M.; Nezhad, F.F.; Emami, F. Is application of Kinesio tape to treat hyperlordosis more effective on abdominal muscles or hamstrings? J. Res. Med. Sci. 2018, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Katzman, W.B.; Wanek, L.; Shepherd, J.A.; Sellmeyer, D.E. Age-Related Hyperkyphosis: Its Causes, Consequences, and Management. J. Orthop. Sport. Phys. Ther. 2010, 40, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reamy, B.; Slakey, J. Adolescent idiopathic scoliosis: Review and current concepts. Am. Fam. Physician 2001, 64, 111–116. [Google Scholar] [PubMed]
- Naghman, C.M.; Zafar, A.; Rajat, V. Adolescent Idiopathic Scoliosis. Open Orthop. J. 2016, 10, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Tunnell, P.W. Protocol for visual assessment: Postural evaluation of the muscular system through visual inspection. J. Bodyw. Mov. Ther. 1996, 1, 21–27. [Google Scholar] [CrossRef]
- Watson, A.W.; Donncha, C.M. A reliable technique for the assessment of posture: Assessment criteria for aspect of posture. J. Sport. Med. Phys. Fit. 2000, 40, 260–270. [Google Scholar]
- Radaš, J.; Trošt Bobić, T. Posture in top-level Croatian rhythmic gym nasts and non-trainees. Kinesiology 2011, 43, 64–73. [Google Scholar]
- Sedrez, J.; Candotti, C.; Furlanetto, T.; Loss, J. Non-invasive postural assessment of the spine in the sagittal plane: A systematic review. Motricidade 2016, 12, 140. [Google Scholar] [CrossRef] [Green Version]
- Cobb, J.R. Outline for the study of scoliosis. Instr. Course Lect. 1948, 5, 261–275. [Google Scholar]
- Bonanni, P.G. Contour and Angle-Function Based Scoliosis Monitoring: Relaxing the Requirement on Image Quality in the Measurement of Spinal Curvature. Int. J. Spine Surg. 2017, 11. [Google Scholar] [CrossRef]
- Barrett, E.; McCreesh, K.; Lewis, J. Reliability and validity of non-radiographic methods of thoracic kyphosis measurement: A systematic review. Man. Ther. 2014, 19, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Chaise, F.O.; Candotti, C.T.; Torre, M.L.; Furlanetto, T.S.; Pelinson, P.P.T.; Loss, J.F. Validation, repeatability and reproducibility of a noninvasive instrument for measuring thoracic and lumbar curvature of the spine in the sagittal plane. Braz. J. Phys. Ther. 2011, 15, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greendale, G.A.; Nili, N.S.; Huang, M.H.; Seeger, L.; Karlamangla, A.S. The reliability and validity of three non-radiological measures of thoracic kyphosis and their relations to the standing radiological Cobb angle. Osteoporos. Int. 2011, 22, 1897–1905. [Google Scholar] [CrossRef] [Green Version]
- Korovessis, P.; Petsinis, G.; Papazisis, Z.; Baikousis, A. Prediction of Thoracic Kyphosis Using the Debrunner Kyphometer. J. Spinal Disord. 2001, 14, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Valentine, R.E. Clinical measurement of the thoracic kyphosis. A study of the intra-rater reliability in subjects with and without shoulder pain. BMC Musculoskelet. Disord. 2010, 11. [Google Scholar] [CrossRef] [Green Version]
- Gravina, A.; Ferraro, C.; Frizziero, A.; Ferraro, M.; Masiero, S. Goniometer evaluation of thoracic kyphosis and lumbar lordosis in subjects during growth age: A validity study. Stud. Health Technol. Inform. 2012, 176, 247–251. [Google Scholar] [CrossRef]
- Sheeran, L.; Sparkes, V.; Busse, M.; Van Deursen, R. Preliminary study: Reliability of the spinal wheel. A novel device to measure spinal postures applied to sitting and standing. Eur. Spine J. 2010, 19, 995–1003. [Google Scholar] [CrossRef] [Green Version]
- Willner, S. Spinal Pantograph-A Non-Invasive Technique for Describing Kyphosis and Lordosis in the Thoraco-Lumbar Spine. Acta Orthop. Scand. 1981, 52, 525–529. [Google Scholar] [CrossRef]
- Côté, P.; Kreitz, B.; Cassidy, J.D. A study of the diagnostic accuracy and reliability of the Scoliometer and Adam’s forward bend test. Spine 2003, 23, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Tyrakowski, M.; Czaprowski, D.; Szczodry, M.; Siemionow, K. Cobb angle measurements on digital radiographs using Bunnell scoliometer: Validation of the method. J. Back Musculoskelet. Rehabil. 2017, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.; Ferreira, F.; Narciso, F.; Makhoul, C.; Canto, R.; Barauna, M. Evaluation of lumbar concavity using a radiographic method and kypholordometry. Braz. J. Phys. Ther. 2009, 13, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Porto, A.B.; Okazaki, V.H.A. Procedures of assessment on the quantification of thoracic kyphosis and lumbar lordosis by radiography and photogrammetry: A literature review. J. Bodyw. Mov. Ther. 2017, 21, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F.; Knecht, K.; Balaban, G.; Dvorak, J.; Grob, D. A new skin-surface device for measuring the curvature and global and segmental ranges of motion of the spine: Reliability of measurements and comparison with data reviewed from the literature. Eur. Spine J. 2004, 13, 122–136. [Google Scholar] [CrossRef] [Green Version]
- Czaprowski, D.; Pawłowska, P.; Gębicka, A.; Sitarski, D.; Kotwicki, T. Intra- and interobserver repeatability of the assessment of anteroposterior curvatures of the spine using Saunders digital inclinometer. Ortop. Traumatol. Rehabil. 2012, 14, 145–153. [Google Scholar] [CrossRef]
- Perriman, D.M.; Scarvell, J.M.; Hughes, A.R.; Ashman, B.; Lueck, C.J.; Smith, P.N. Validation of the flexible electrogoniometer for measuring thoracic kyphosis. Spine 2010, 35 14, E633–E640. [Google Scholar] [CrossRef]
- Foelsch, C.; Schlögel, S.; Lakemeier, S.; Wolf, U.; Timmesfeld, N.; Skwara, A. Test-Retest Reliability of 3D Ultrasound Measurements of the Thoracic Spine. PMR 2012, 4, 335–341. [Google Scholar] [CrossRef]
- Melvin, M.; Mohokum, M.; Sylvia, M.; Mendoza, S.; Wolf, U.; Sitter, H.; Paletta, J.; Skwara, A. Reproducibility of Rasterstereography for Kyphotic and Lordotic Angles, Trunk Length, and Trunk Inclination a Reliability Study. Spine 2010, 35, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Leroux, M.; Zabjek, K.; Simard, G.; Badeaux, J.; Coillard, C.; Rivard, C. A noninvasive anthropometric technique for measuring kyphosis and lordosis: An application for idiopathic scoliosis. Spine 2000, 25, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, E.; Duarte, M.; Maldonado, E.; Burke, T.; Marques, A. Postural assessment software (PAS/SAPO): Validation and reliabiliy. Clinics 2010, 65, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Furlanetto, T.S.; Candotti, C.T.; Comerlato, T.; Loss, J.F. Validating a postural evaluation method developed using a Digital Image-based Postural Assessment (DIPA) software. Comput. Methods Programs Biomed. 2012, 108, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hébert-Losier, K.; Rahman, F.A. Reliability of postural measures in elite badminton players using Posture Pro 8. Physiother. Theory Pract. 2018, 34, 483–494. [Google Scholar] [CrossRef]
- Scholten, P.; Veldhuizen, A. Analysis of Cobb angle measurements in scoliosis. Clin. Biomech. 1987, 2, 7–13. [Google Scholar] [CrossRef]
- Zhang, J.; Lou, E.; Hill, D.L.; Raso, J.V.; Wang, Y.; Le, L.H.; Shi, X. Computer-aided assessment of scoliosis on posteroanterior radiographs. Med. Biol. Eng. Comput. 2010, 48, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Mok, J.; Diab, M.; Hackbarth, M.; Hu, S.; Deviren, V. Comparison of Observer Variation in Conventional and Three Digital Radiographic Methods Used in the Evaluation of Patients With Adolescent Idiopathic Scoliosis. Spine 2008, 33, 681–686. [Google Scholar] [CrossRef]
- Morrissy, R.T.; Goldsmith, G.; Hall, E.C.; Kehl, D.K.; Cowie, G.H. Measurement of the Cobb angle on radiographs of patients who have scoliosis. Evaluation of intrinsic error. J. Bone Jt. Surgery. Am. Vol. 1990, 72, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dybå, T.; Dingsøyr, T. Empirical studies of agile software development: A systematic review. Inf. Softw. Technol. 2008, 50, 833–859. [Google Scholar] [CrossRef]
- Dybå, T.; Dingsøyr, T. Strength of Evidence in Systematic Reviews in Software Engineering. In Proceedings of the Second ACM-IEEE International Symposium on Empirical Software Engineering and Measurement, Kaiserslautern, Germany, 9–10 October 2008; ACM: New York, NY, USA, 2008; pp. 178–187. [Google Scholar] [CrossRef] [Green Version]
- Wieringa, R.; Maiden, N.; Mead, N.; Rolland, C. Requirements Engineering Paper Classification and Evaluation Criteria: A Proposal and a Discussion. Requir. Eng. 2006, 11, 102–107. [Google Scholar] [CrossRef]
- Cohen, J. Weighted kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Estrada, J.E.; Vea, L.A. Real-time human sitting posture detection using mobile devices. In Proceedings of the 2016 IEEE Region 10 Symposium (TENSYMP), Bali, Indonesia, 9–11 May 2016; pp. 140–144. [Google Scholar] [CrossRef]
- Franko, O.; Bray, C.; Newton, P. Validation of a Scoliometer Smartphone App to Assess Scoliosis. J. Pediatr. Orthop. 2012, 32, e72–e75. [Google Scholar] [CrossRef] [PubMed]
- Izatt, M.; Bateman, G.; Adam, C. Evaluation of the iPhone with an acrylic sleeve versus the Scoliometer for rib hump measurement in scoliosis. Scoliosis 2012, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Jacquot, F.; Charpentier, A.; Khelifi, S.; Gastambide, D.; Rigal, R.; Sautet, A. Measuring the Cobb angle with the iPhone in kyphoses: A reliability study. Int. Orthop. 2012, 36, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Qiao, J.; Liu, Z.; Xu, L.; Wu, T.; Zheng, X.; Zhu, Z.; Zhu, F.; Qian, B.; Qiu, Y. Reliability Analysis of a Smartphone-aided Measurement Method for the Cobb Angle of Scoliosis. J. Spinal Disord. Tech. 2012, 25, E88–E92. [Google Scholar] [CrossRef] [PubMed]
- Shaw, M.; Adam, C.; Izatt, M.; Licina, P.; Askin, G. Use of the iPhone for Cobb angle measurement in scoliosis. Eur. Spine J. 2011, 21, 1062–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salamh, P.A.; Kolber, M. The reliability, minimal detectable change and concurrent validity of a gravity-based bubble inclinometer and iphone application for measuring standing lumbar lordosis. Physiother. Theory Pract. 2013, 30, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Balg, F.; Juteau, M.; Theoret, C.; Svotelis, A.; Grenier, G. Validity and Reliability of the iPhone to Measure Rib Hump in Scoliosis. J. Pediatr. Orthop. 2014, 34. [Google Scholar] [CrossRef]
- Qiao, J.; Xu, L.; Zhu, Z.; Zhu, F.; Liu, Z.; Qian, B.; Qiu, Y. Inter- and intraobserver reliability assessment of the axial trunk rotation: Manual versus smartphone-aided measurement tools. BMC Musculoskelet. Disord. 2014, 15, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutlu, S.; Guler, O.; Harun, M.; Komur, B.; Caliskan, G.; Heybeli, N. A New Trend in Cobb Angle Measurement: The Use of iPhones. J. Med. Imaging Health Inform. 2014, 4. [Google Scholar] [CrossRef]
- Mazzuia, A.R.d.O.; Machado, D.A.R.; Fukumothi, D.K.; Nunes, L.F.B.; Tucci Neto, C.; Jorge, H.M.d.H.; Ortiz, R.T.; Mattos, C.A.d. Iphone app use to Cobb angle in adolescent idiopathic scoliosis: Does this apply? Coluna Columna 2015, 14, 101–104. [Google Scholar] [CrossRef] [Green Version]
- Allam, Y.; El-Fiky, T.; Farghally, M.; Al-Sabagh, S.; Siam, A. Comparison between Oxford Cobbmeter and digital Cobbmeter for measurement of Cobb angle in adolescent idiopathic scoliosis. Eur. Spine J. 2016, 25. [Google Scholar] [CrossRef] [PubMed]
- Boland, D.M.; Neufeld, E.V.; Ruddell, J.; Dolezal, B.A.; Cooper, C.B. Inter- and intra-rater agreement of static posture analysis using a mobile application. J. Phys. Ther. Sci. 2016, 28, 3398–3402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koumantakis, G.; Nikoloudaki, M.; Thacheth, S.; Zagli, K.; Bitrou, K.; Nigritinos, A.; Botton, L. Reliability and Validity Measurement of Sagittal Lumbosacral Quiet Standing Posture with a Smartphone Application in a Mixed Population of 183 College Students and Personnel. Adv. Orthop. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Marchi, L.; Fortti, F.; Amaral, R.; Oliveira, L.; Nogueira-Neto, J.; Jensen, R.; Pimenta, L. Reproducibility and equivalence of Cobbmeter application in the sagittal evaluation of the spine. Coluna Columna 2016, 15, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Waś, J.; Sitarski, D.; Ewertowska, P.; Bloda, J.; Czaprowski, D. Using smartphones in the evaluation of spinal curvatures in a sagittal plane. Adv. Rehabil. 2016, 30, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Bucke, J.; Spencer, S.; Fawcett, L.; Sonvico, L.; Rushton, A.; Heneghan, N.R. Validity of the Digital Inclinometer and iPhone When Measuring Thoracic Spine Rotation. J. Athl. Train. 2017, 52, 820–825. [Google Scholar] [CrossRef]
- Kunkle, W.A.; Madden, M.; Potts, S.; Fogelson, J.; Hershman, S. Validity of a smartphone protractor to measure sagittal parameters in adult spinal deformity. Spine J. 2017, 17, 1559–1564. [Google Scholar] [CrossRef]
- Szucs, K.A.; Cicuto, K.; Rakow, M. A comparison of upper body and limb postures across technology and handheld device use in college students. J. Phys. Ther. Sci. 2018, 30, 1293–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacob, S.M.; Chisnoiu, A.M.; Lascu, L.M.; Berar, A.M.; Studnicska, D.; Fluerasu, M.I. Is PostureScreen®Mobile app an accurate tool for dentists to evaluate the correlation between malocclusion and posture? CRANIO 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moalej, S.; Kazemi, S.; Asadabadi, M.; Khedmat, L.; Hashemi, R.; Tavacolizadeh, R.; Vahabi, Z.; Shariatpanahi, G. Screening of scoliosis in school children in Tehran: The prevalence rate of idiopathic scoliosis. J. Back Musculoskelet. Rehabil. 2018, 31, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Szucs, K.A.; Brown, E.V.D. Rater reliability and construct validity of a mobile application for posture analysis. J. Phys. Ther. Sci. 2018, 30, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, B.B.; Vehrs, P.R.; Fellingham, G.W.; George, J.D.; Hager, R.; Ridge, S.T. Validity and Reliability of Standing Posture Measurements Using a Mobile Application. J. Manip. Physiol. Ther. 2019, 42, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, I.; Lee, J.; Park, J.H.; Cho, C.b.; Yang, S.; Sung, J.H.; Hong, J. Validity of a Smartphone Application (Sagittalmeter Pro) for the Measurement of Sagittal Balance Parameters. World Neurosurg. 2019, 126. [Google Scholar] [CrossRef]
- Wang, J.; Chen, T.; Rui, X.; Yang, Y.; Zhang, H. Rapid Measurement of Lumbosacral Spine-Pelvic Sagittal Balance Parameters using Electronic Device. J. King Saud Univ. Sci. 2020. [Google Scholar] [CrossRef]
- Chen, C.; Yu, R.; Xu, W.; Li, Z.; Yifan, L.; Hu, R.; Xiaodong, Z. A Practical Study of Diagnostic Accuracy: Scoliosis Screenings of Middle School Students by a Trained Nurse With a Smartphone Versus a Spine Surgeon With a Scoliometer. SPINE 2020, 45, 1. [Google Scholar] [CrossRef]
- Petropoulos, A.; Sikeridis, D.; Antonakopoulos, T. SPoMo: IMU-based real-time sitting posture monitoring. In Proceedings of the IEEE 7th International Conference on Consumer Electronics, Berlin, Germany, 3–6 September 2017; pp. 5–9. [Google Scholar] [CrossRef]
- Lee, H.; Lee, S.; Salado, L.; Estrada, J.; White, J.; Muthukumar, V.; Lee, S.P.; Mohapatra, S. Proof-of-Concept Testing of a Real-Time mHealth Measure to Estimate Postural Control During Walking: A Potential Application for Mild Traumatic Brain Injuries. Asian Pacific Isl. Nurs. J. 2018, 3, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P. Smartphone Applications for Patients’ Health and Fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Merriaux, P.; Dupuis, Y.; Boutteau, R.; Vasseur, P.; Savatier, X. A Study of Vicon System Positioning Performance. Sensors 2017, 17, 1591. [Google Scholar] [CrossRef] [PubMed]
- Moreira, R.; Teles, A.; Fialho, R.; Dos Santos, T.C.P.; Vasconcelos, S.S.; De Sá, I.C.; Bastos, V.H.; Silva, F.; Teixeira, S. Can human posture and range of motion be measured automatically by smart mobile applications? Med. Hypotheses 2020, 142, 109741. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Name | Description |
|---|---|---|
| [35] | Arcometer | Instrument with a main shaft and perpendicular rods and scales attached to the shaft of each rod. |
| [36] | Flexicurve Index | Flexible ruler positioned on the back, adopting thoracic and lumbar contours. The shape of the ruler is drawn on paper and the kyphosis index is calculated. |
| [36] | Flexicurve Angle | Similar to the flexicurve index but the kyphosis angle is calculated from the drawing using geometric formulas. |
| [37] | Debrunner Kyphometer | Two-arm protractor whose ends are positioned at specified bone markers. |
| [38] | Manual Inclinometer | Instrument with a kind of pendulum that measures the angle of inclination and vertebral elevation when positioned over them. |
| [39] | Goniometer | An instrument with two rods connected by a 360 axis that is positioned at the center of the joint and enables the evaluation of the angle of movement of the body segment. |
| [40] | Spinal Wheel | It is a plastic wheel device 10 cm in diameter and with a reflective marker at the center that is guided along the midline from vertebra S1 to the occipital endpoint. |
| [41] | Pantograph | Instrument with articulated parallel rods at the end of which a low-frictioned wheel is mounted that contours the back. |
| [42,43] | Scoliometer | It is a fluid-filled inclinometer in which an enclosed ball shows the angle of trunk rotation. |
| [44] | Kypholordometer | Apparatus made up of an aluminum vertical rod and 39 horizontally shaped and deformable horizontal rods with cross section. These rods are pointed at the back and the contours of the vertebral curvatures are drawn on the paper attached to the back of the instrument. |
| [32,45] | Radiograph | It allows the quantification of the spine angles from calculations performed from the vertebrae visible through the X-ray using the Cobb method. |
| Study | Name | Description |
|---|---|---|
| [46] | Spinal Mouse | Manual and computer-assisted electromechanical device that is guided along midline of the spine starting at the spinous process of C7 and ending at top of the anal crease, approximately S3. |
| [47] | Digital Inclinometer | Similar to manual inclinometer but it has sensors that capture body inclination. |
| [48] | Electrogoniometer | Instrument that allows continuous measurement of the angular displacement between 2 lightweight plastic end blocks at either end of a coil containing 2 strain gauges mounted at 90 to each other. |
| Study | Name | Description |
|---|---|---|
| [49] | 3D ultrasound | System that uses a point marker to identify column reference points. A directional microphone, a reference marker, and a computer with specific software that contains normative data on vertebrae distances, allowing it to calculate angles and distances of measured 3D data that is transformed into degrees of motion range. |
| [50] | Rasterstereography | Method for 3-dimensional back shape analysis. System that detects anatomical reference points, prominent vertebra and the two upper iliac spines, and coordinate the data of the back-surface points and the line of symmetry between them. |
| [51] | Stereovideography | Similar to rasterstereography, but it is based on system of stereo-video cameras. |
| [11] | Photogrammetry | Based on photographs added to the software, which processes them and calculates the distance between body segments and angles formed between them. |
| ID | Question |
|---|---|
| RQ1 | What mobile applications have been used and proposed for analyzing the human posture based on spine alignment? |
| RQ2 | What are the technical features implemented by those mobile applications for assessing the human spine alignment? |
| RQ3 | What are the types of research presented in the literature regarding those mobile applications for assessing sagittal and coronal alignment of the human spine? |
| RQ4 | What metrics are used to evaluate mobile applications? |
| RQ5 | What are the performance results obtained by the mobile applications? |
| Primary Terms | Secondary Terms |
|---|---|
| “Mobile Application” | “Mobile System” OR “Mobile App” OR “Mobile devices” OR “Mobile phone” OR “smartphone application” OR iphone |
| Posture | “Static standing posture” OR “Posture Analysis” OR “Postural Assessment” OR scoliosis OR lordosis OR kyphosis |
| ID | Description |
|---|---|
| QQ1 | Is the paper based on research (or is it merely a “lessons learned” report based on expert opinion)? |
| QQ2 | Is there a clear statement of the aims of the research? |
| QQ3 | Is there an adequate description of the context in which the research was carried out? |
| QQ4 | Was the research design appropriate to address the aims of the research? |
| QQ5 | Was the recruitment strategy appropriate to the aims of the research? |
| QQ6 | Was there a control group with which to compare treatments? |
| QQ7 | Was the data collected in a way that addressed the research issue? |
| QQ8 | Was the data analysis sufficiently rigorous? |
| QQ9 | Has the relationship between researcher and participants been considered to an adequate degree? |
| QQ10 | Is there a clear statement of findings? |
| QQ11 | Is the study of value for research or practice? |
| Study | Name | Category | Study Design | Availability |
|---|---|---|---|---|
| [66] | Scoligauge | US | VR & ER | TopOrthoApps.com |
| [67] | Scoligauge | US | ER | TopOrthoApps.com |
| [68] | Cobbmeter | US | VR & ER | Apple Store |
| [69] | Cobbmeter | US | VR & ER | Apple Store |
| [70] | Tiltmeter Pro | US | VR & ER | Play Store * & Apple Store |
| [71] | iHandy Level | US | ER & VR | Play Store * & Apple Store * |
| [72] | Scoligauge | US | VR & ER | TopOrthoApps.com |
| [73] | Scoligauge | US | VR & ER | TopOrthoApps.com |
| [74] | iGonio | US | ER | 148apps.com * |
| [75] | Cobbmeter | US | VR & ER | Apple Store |
| [76] | Cobbmeter + Tiltmeter | US | VR & ER | Apple Store |
| [77] | PostureScreen Mobile | IBS | ER | Play Store & Apple Store |
| [65] | Unnamed | US | PS & VR | No |
| [78] | iHandy Level | US | ER & VR | Play Store */Apple Store * |
| [79] | Cobbmeter | US | VR & ER | Apple Store |
| [80] | Scoliometer 1.1 | US | VR & ER | apkgoogle.org * |
| [81] | iPhone Clinometer app | US | ER & VR | Play Store * & Apple Store |
| [82] | Smartphone Protractor | US | VR | Play Store * |
| [83] | PostureScreen Mobile | IBS | ER | Play Store & Apple Store |
| [84] | PostureScreen Mobile | IBS | ER | Play Store & Apple Store |
| [85] | Scolioscreen | US | ER | spinologics.ca |
| [86] | PostureScreen Mobile | IBS | VR & ER | Play Store & Apple Store |
| [87] | PostureScreen Mobile | IBS | VR | Play Store & Apple Store |
| [88] | Sagittalmeter Pro | US | VR & ER | Play Store |
| [89] | iPhone’s photo editing application | IBS | VR & ER | iPhone native application |
| [90] | Scoligauge | US | VR & ER | TopOrthoApps.com |
| Sensor | References |
|---|---|
| Accelerometer | [66,67,68,69,70,71,72,73,74,75,76,78,79,80,85,88,90,91] |
| Gyroscope | [65,81,91] |
| Study | Measures Taken |
|---|---|
| [66] | Scoliosis |
| [67] | Rib Hump Angle/Scoliosis |
| [68] | Kyphotic Angles |
| [69] | Cobb Angle/Thoracic Scoliosis |
| [70] | Cobb Angle/Thoracic Scoliosis |
| [71] | Lumbar Lordosis |
| [72] | Rib Hump Angle/Scoliosis Evaluation |
| [73] | Cobb Angle of Thoracolumbar Scoliosis |
| [74] | Cobb Angle |
| [75] | Cobb Angle |
| [76] | Cobb Angle |
| [77] | Head, Ribcage, Shoulder, Hip and Knee Tilt |
| [65] | Inclination of the Human Spinal Points |
| [78] | SS and Lumbar Curve |
| [79] | PI, PT and LL |
| [80] | Sagittal Curvaures |
| [81] | Thoracic Spine Rotation |
| [82] | LL, PI, and PT |
| [83] | Head, Ribcage, Shoulder, Hip Tilt |
| [84] | Head, Ribcage, Shoulder, Hip Inclination |
| [85] | Scoliosis Angle |
| [86] | Head, Shoulder and Ribcage Tilt |
| [87] | Head, Ribcage, Shoulder, Hip and Knee Tilt |
| [88] | LL, PI, SS and PT |
| [89] | LL, PT, and SS |
| [90] | Rib Hump/Scoliosis Evaluation |
| Analysis Method | References |
|---|---|
| Direct contact with the body | [65,66,67,71,72,73,78,80,81,82,85,90] |
| Indirect contact with the body | [68,69,70,74,75,76,79,88,89] |
| No contact with the body | [77,83,84,86,87] |
| Study | Metric | Main Findings |
|---|---|---|
| [66] | ICC and Pearson correlation coefficient for comparing Scoligauge with angle measures made with standard clinical scoliometer. | Scoligauge has validity and reliability when comparing it with the standard clinical scoliometer for assessing deformity in scoliosis. |
| [67] | ICC and Bland Altman analysis for rib hump angle. | The application proved to be valid for measurements of hump in the ribs. The inter- and intra-observer measurement variability using iPhone was similar to that of the Scoliometer. |
| [68] | Mean, SD and ICC for measuring kyphotic angles. | The reliability analysis showed that measurements were highly correlated with those obtained using the standard method. |
| [69] | Mean, SD, ICC and paired t-test to measure Cobb Angle of thoracic scoliosis and compare the time consumed for the measurement between application and manual method. | Smartphone-aided measurement for the Cobb angle showed excellent reliability and efficiency. The average time spent for evaluating was shorter when using CoobMeter. |
| [70] | Mean, SD, and Bland Altman analysis for measuring Cobb Angle and comparing Tiltmeter with traditional protractor. | Tiltmeter is an equivalent Cobb measurement tool to the manual protractor, and measurement times are about 15% lower. |
| [71] | ICC, mean and SD for measuring body angles. | Both Bubble inclinometer and iHandy Level had good intra-rater and inter-rater reliability and concurrent validity for measuring lumbar lordosis. |
| [72] | ICC and Bland Altman analysis for measuring rib hump and comparing Scoligauge with traditional scoliometer. | Scoligauge showed excellent intra-rater and inter-rater reliability with valid measurements when compared to the scoliotometer. |
| [73] | Mean and ICC to compare scoliometer and Scoligauge. | Scoliguage showed excellent reliability when compared to the scoliotometer. |
| [74] | Mean and SD to compare measurements made by using standard protractor and IGonio. | iGonio proved to be reliable and efficient for measuring Cobb angle. |
| [75] | Mean, SD, paired t-test and Kappa to compare measurements of scoliosis made by using the manual method and CobbMeter. | Authors reported that CobbMeter is reliable, although there was a significant difference between values found with the two methods. |
| [76] | Mean, SD and Bland Altman analysis to compare measurements of scoliosis performed with Oxford Cobbmeter and digital Cobbmeter+Tiltmeter. | Integrated Tiltmeter and Cobbmeter consist of a Cobb measurement tool equivalent to the Oxford Cobbmeter. |
| [77] | ICC to assess the reliability of the measurements of body displacement angles. | Posture assessment with PostureScreen showed substantial reliability. |
| [65] | Accuracy and kappa for assess cervical, thoracic and lumbar angles. | The proposed mobile solution was able to detect proper and improper sitting postures. |
| [78] | Mean, SD, Repeated measures ANOVAs, ICC, Bland Altman to measure sagittal lumbosacral posture. | iHandy Level is a reliable and valid tool for measuring lumbosacral standing spinal posture in the sagittal plane. |
| [79] | ICC and Kappa to compare measurements made by the Cobbmeter and goniometer along with a dermatograph pencil in the analysis of sagittal alignment of the spine. | CobbMeter is a valid and reliable instrument for measuring the angle involved in the sagittal balance of the spine. |
| [80] | Mean, SD, ICC, Mann Whitney and Student’s t-distribution to assess and compare measurements of spine curvatures in the saggital plane performed with digital inclinometer and Scoliometer 1.1. | Measures of spinal curvatures with both instruments showed reliable values. |
| [81] | Pearson correlation coefficient, ICC, mean and SD for measuring thoracic spine rotation in the heel-sit position. | Digital Inclinometer and iPhone Clinometer application proved to be reliable for assessing thoracic spine rotation. |
| [82] | ICC and mean for measuring lumbar lordosis, pelvic incidence, and pelvic tilt angles and determining the validity of Smartphone Protractor. | The application proved to be reliable for assessing adult spinal deformity of radiographic parameters. |
| [83] | Mean and SD for body angles. | PostureScreen detected posture variables in the sagittal and coronal planes. |
| [84] | Mean, SD and ICC for body angles. | PostureScreen proved to be a useful tool for dentists in the early diagnosis of dental occlusion pathology. |
| [85] | Mean, SD, Student’s t-distribution, ANOVA and Fisher’s exact test for detecting scoliosis in school children. | Scolioscreen showed high sensitivity and specificity, demonstrating to be useful for the early diagnosis of scoliosis. |
| [86] | ICC, mean and SD for body angles. | PostureScreen showed strong reliability for assessing human posture. |
| [90] | Cohen’s kappa and Pearson correlation coefficients for comparing measures performed with Scoligauge and scoliometer. | The sensitivity of the smartphone screening was not acceptable for recognizing scoliosis. |
| [87] | ICC, mean and SD to assess the reliability for measuring body angles in the sagittal and frontal planes. | PostureScreen was able to detect postural measurements, but its use showed significant bias in postural measurements of the frontal and sagittal planes. |
| [88] | Mean, SD and ICC for comparing PACS and SagittalMeter Pro for measuring spinopelvic sagittal parameters. | Measurements performed with both methods were equivalent and the time required to obtain measurements was shorter when using SagittalMeter Pro. |
| [89] | ICC, Mann-Whitney test, One-way ANOVA for measuring lumbosacral spine-pelvic sagittal parameters performed by PACS and iPhone. | iPhone showed similar accuracy when compared with PACS. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, R.; Teles, A.; Fialho, R.; Baluz, R.; Santos, T.C.; Goulart-Filho, R.; Rocha, L.; Silva, F.J.; Gupta, N.; Bastos, V.H.; et al. Mobile Applications for Assessing Human Posture: A Systematic Literature Review. Electronics 2020, 9, 1196. https://doi.org/10.3390/electronics9081196
Moreira R, Teles A, Fialho R, Baluz R, Santos TC, Goulart-Filho R, Rocha L, Silva FJ, Gupta N, Bastos VH, et al. Mobile Applications for Assessing Human Posture: A Systematic Literature Review. Electronics. 2020; 9(8):1196. https://doi.org/10.3390/electronics9081196
Chicago/Turabian StyleMoreira, Rayele, Ariel Teles, Renan Fialho, Rodrigo Baluz, Thalyta Cibele Santos, Rômulo Goulart-Filho, Laiane Rocha, Francisco José Silva, Nishu Gupta, Victor Hugo Bastos, and et al. 2020. "Mobile Applications for Assessing Human Posture: A Systematic Literature Review" Electronics 9, no. 8: 1196. https://doi.org/10.3390/electronics9081196