Entropy Analysis of RR and QT Interval Variability during Orthostatic and Mental Stress in Healthy Subjects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects and Measurement Protocol
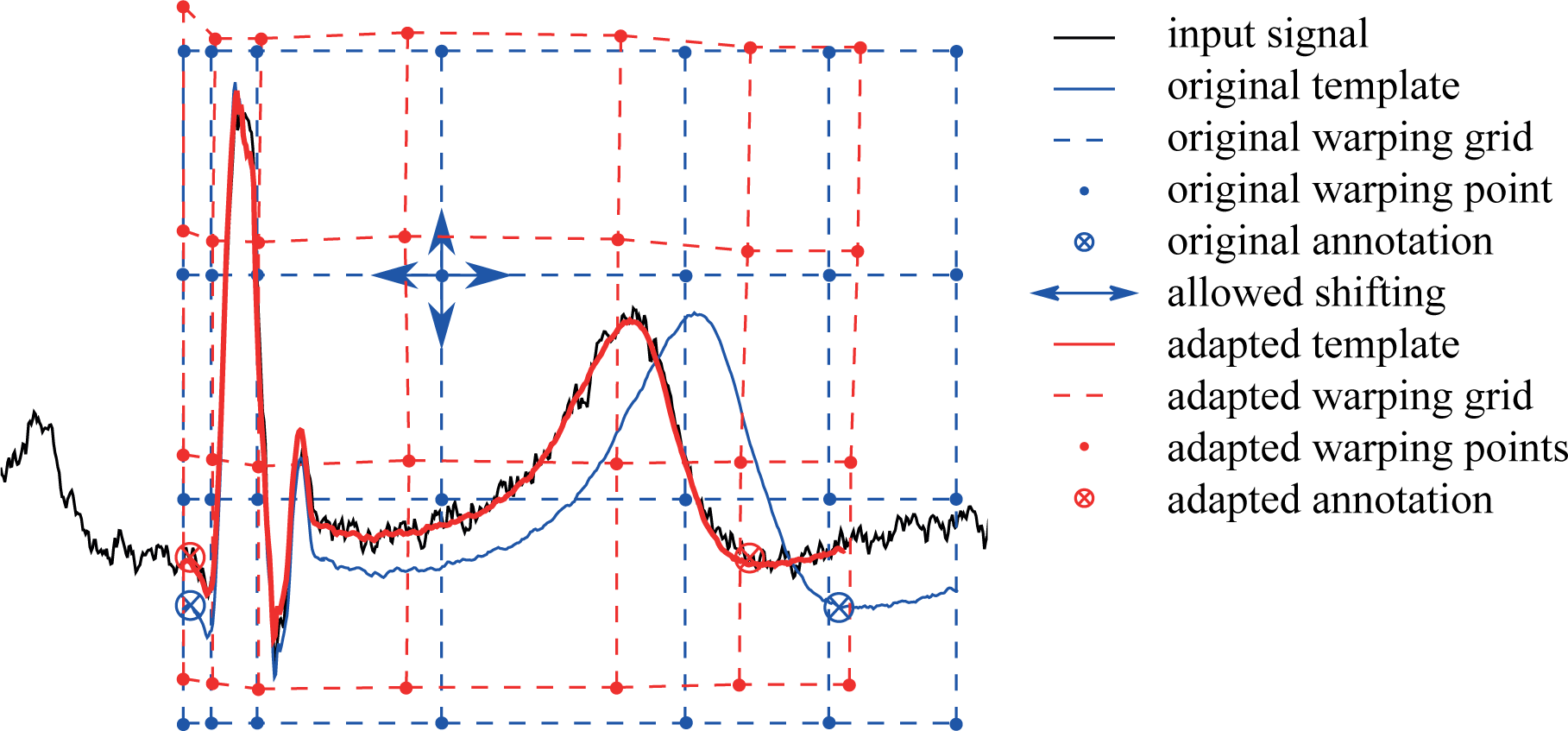
2.2. Beat-to-beat QT Interval Extraction
2.3. Entropy Estimation
2.3.1. Cross-sample Entropy
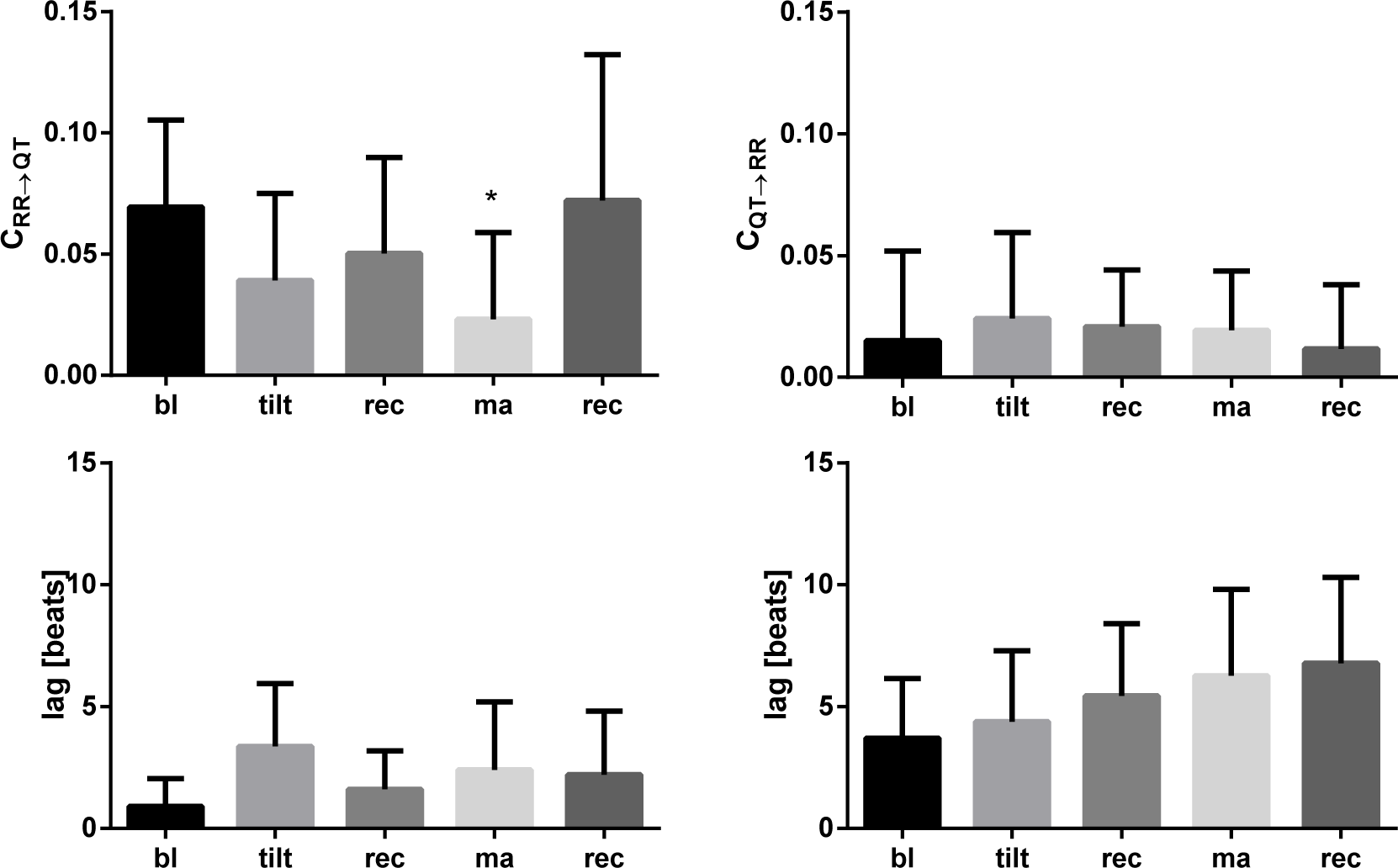
2.3.2. Causality Analysis in the Information Domain
2.3.3. Statistical Analysis
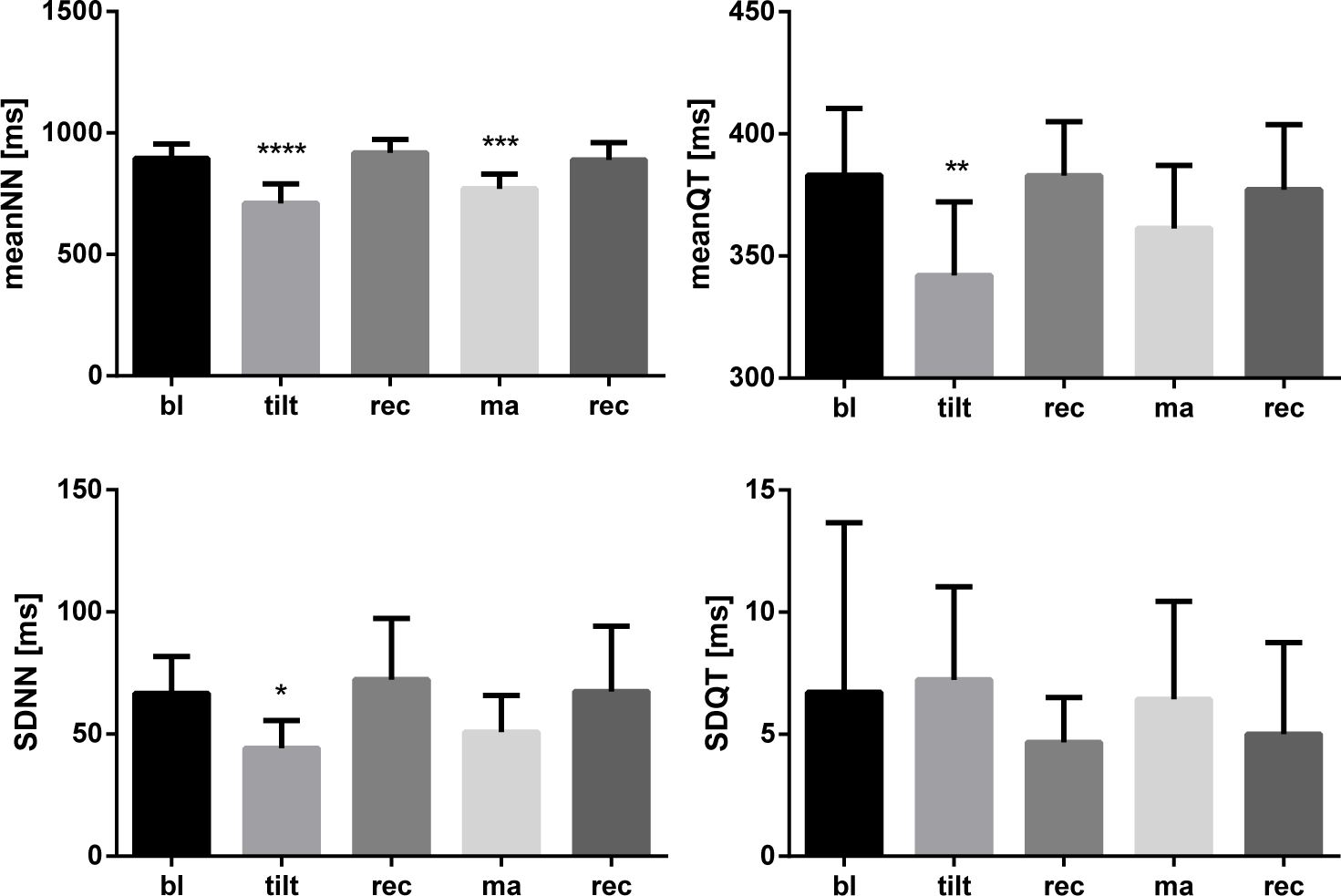
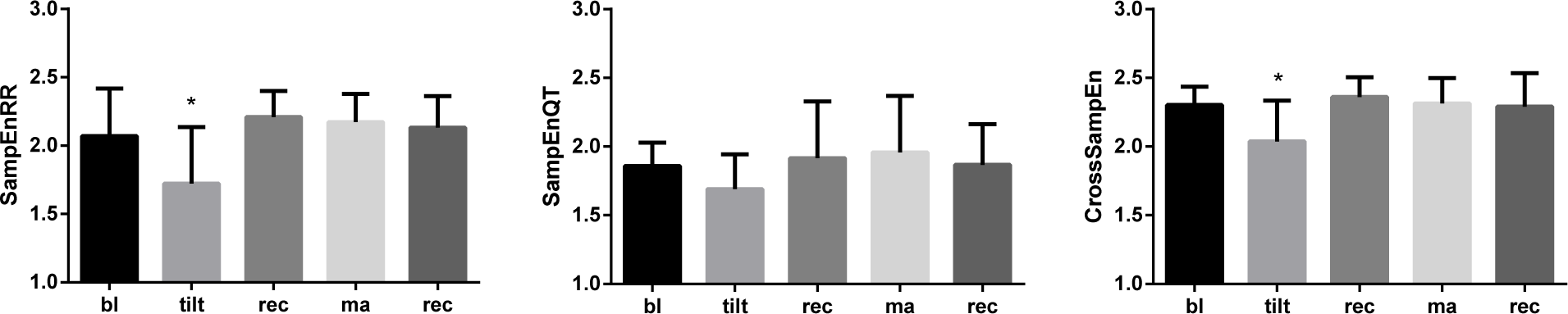
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Berger, R.D.; Kasper, E.K.; Baughman, K.L.; Marban, E.; Calkins, H.; Tomaselli, G.F. Beat-to-beat QT interval variability novel evidence for repolarization lability in ischemic and nonischemic dilated cardiomyopathy. Circulation 1997, 96, 1557–1565. [Google Scholar]
- Yeragani, V.K.; Pohl, R.; Jampala, V.; Balon, R.; Kay, J.; Igel, G. Effect of posture and isoproterenol on beat-to-beat heart rate and QT variability. Neuropsychobiology 2000, 41, 113–123. [Google Scholar]
- Baumert, M.; Lambert, G.W.; Dawood, T.; Lambert, E.A.; Esler, M.D.; McGrane, M.; Barton, D.; Nalivaiko, E. QT interval variability and cardiac norepinephrine spillover in patients with depression and panic disorder. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H962–H968. [Google Scholar]
- Baumert, M.; Schlaich, M.P.; Nalivaiko, E.; Lambert, E.; Sari, C.I.; Kaye, D.M.; Elser, M.D.; Sanders, P.; Lambert, G. Relation between QT interval variability and cardiac sympathetic activity in hypertension. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1412–H1417. [Google Scholar]
- Nayyar, S.; Roberts-Thomson, K.C.; Hasan, M.A.; Sullivan, T.; Harrington, J.; Sanders, P.; Baumert, M. Autonomic modulation of repolarization instability in patients with heart failure prone to ventricular tachycardia. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H1181–H1188. [Google Scholar]
- Sacre, J.W.; Franjic, B.; Coombes, J.S.; Marwick, T.H.; Baumert, M. QT interval variability in type 2 diabetic patients with cardiac sympathetic dysinnervation assessed by 123I-metaiodobenzylguanidine scintigraphy. J. Cardiovasc. Electrophysiol. 2013, 24, 305–313. [Google Scholar]
- Porta, A.; Baselli, G.; Caiani, E.; Malliani, A.; Lombardi, F.; Cerutti, S. Quantifying electrocardiogram RT-RR variability interactions. Med. Biol. Eng. Comput. 1998, 36, 27–34. [Google Scholar]
- Porta, A.; Tobaldini, E.; Gnecchi-Ruscone, T.; Montano, N. RT variability unrelated to heart period and respiration progressively increases during graded head-up tilt. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H1406–H1414. [Google Scholar]
- Baumert, M.; Czippelova, B.; Porta, A.; Javorka, M. Decoupling of QT interval variability from heart rate variability with ageing. Physiol. Meas. 2013, 34, 1435. [Google Scholar]
- Baumert, M.; Starc, V.; Porta, A. Conventional QT variability measurement vs. template matching techniques: comparison of performance using simulated and real ECG. PLOS ONE 2012, 7, e41920. [Google Scholar]
- Zaunseder, S.; Schmidt, M.; Malberg, H.; Baumert, M. Measurement of QT variability by two-dimensional warping, Proceedings of 2014 8th Conference of the European Study Group on Cardiovascular Oscillations, Trento, Italy, 25–28 May 2014; pp. 163–164.
- Schmidt, M.; Baumert, M.; Porta, A.; Malberg, H.; Zaunseder, S. Two-dimensional warping for one-dimensional signals—Conceptual framework and application to ECG processing. IEEE Trans. Signal Process. 2014, 62, 5577–5588. [Google Scholar]
- Cabasson, A.; Meste, O. Time delay estimation: A new insight into the Woody’s method. IEEE Signal Process. Lett. 2008, 15, 573–576. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar]
- Faes, L.; Nollo, G.; Porta, A. Information domain approach to the investigation of cardio-vascular, cardio-pulmonary, and vasculo-pulmonary causal couplings. Front. Physiol. 2011, 2. [Google Scholar] [CrossRef]
- Faes, L.; Nollo, G.; Porta, A. Mechanisms of causal interaction between short-term RR interval and systolic arterial pressure oscillations during orthostatic challenge. J. Appl. Physiol. 2013, 114, 1657–1667. [Google Scholar]
- Porta, A.; Baselli, G.; Lombardi, F.; Montano, N.; Malliani, A.; Cerutti, S. Conditional entropy approach for the evaluation of the coupling strength. Biol. Cybern. 1999, 81, 119–129. [Google Scholar]
- Javorka, M.; Czippelova, B.; Chladekova, L.; Turianikova, Z.; Visnovcova, Z.; Lazarova, Z.; Tonhajzerova, I. Cardiovascular control during orthostatic and mental stress: Conditional entropy based analysis. Proceedings of 2014 8th Conference of the European Study Group on Cardiovascular Oscillations, Trento, Italy, 25–28 May 2014; pp. 14–15.
- Hjemdahl, P.; Freyschuss, U.; Juhlin-Dannfelt, A.; Linde, B. Differentiated sympathetic activation during mental stress evoked by the Stroop test. Acta Psychiat. Scand. Suppl. 1983, 527, 25–29. [Google Scholar]
- Baumert, M.; Javorka, M.; Seeck, A.; Faber, R.; Sanders, P.; Voss, A. Multiscale entropy and detrended fluctuation analysis of QT interval and heart rate variability during normal pregnancy. Comput. Biol. Med. 2012, 42, 347–352. [Google Scholar]
- Bari, V.; Valencia, J.F.; Vallverdú, M.; Girardengo, G.; Marchi, A.; Bassani, T.; Caminal, P.; Cerutti, S.; George, A.L., Jr.; Brink, P.A.; et al. Multiscale complexity analysis of the cardiac control identifies asymptomatic and symptomatic patients in long QT syndrome type 1. PLOS ONE 2014, 9, e93808. [Google Scholar]
- Lewis, M.; Short, A. Sample entropy of electrocardiographic RR and QT time-series data during rest and exercise. Physiol. Meas. 2007, 28. [Google Scholar] [CrossRef]
- Hasan, M.A.; Abbott, D.; Baumert, M. Relation between beat-to-beat QT interval variability and T-wave amplitude in healthy subjects. Ann. Noninvasive Electrocardiol. 2012, 17, 195–203. [Google Scholar]




© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baumert, M.; Czippelova, B.; Ganesan, A.; Schmidt, M.; Zaunseder, S.; Javorka, M. Entropy Analysis of RR and QT Interval Variability during Orthostatic and Mental Stress in Healthy Subjects. Entropy 2014, 16, 6384-6393. https://doi.org/10.3390/e16126384
Baumert M, Czippelova B, Ganesan A, Schmidt M, Zaunseder S, Javorka M. Entropy Analysis of RR and QT Interval Variability during Orthostatic and Mental Stress in Healthy Subjects. Entropy. 2014; 16(12):6384-6393. https://doi.org/10.3390/e16126384
Chicago/Turabian StyleBaumert, Mathias, Barbora Czippelova, Anand Ganesan, Martin Schmidt, Sebastian Zaunseder, and Michal Javorka. 2014. "Entropy Analysis of RR and QT Interval Variability during Orthostatic and Mental Stress in Healthy Subjects" Entropy 16, no. 12: 6384-6393. https://doi.org/10.3390/e16126384