Antimicrobial Susceptibility Test for the Determination of Resistant and Susceptible S. aureus and Enterococcus spp. Using a Multi-Channel Surface Plasmon Resonance Device


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Microorganism
2.2. Minimum Inhibitory Concentration (MIC) Assay
2.3. Reagents for SPR System
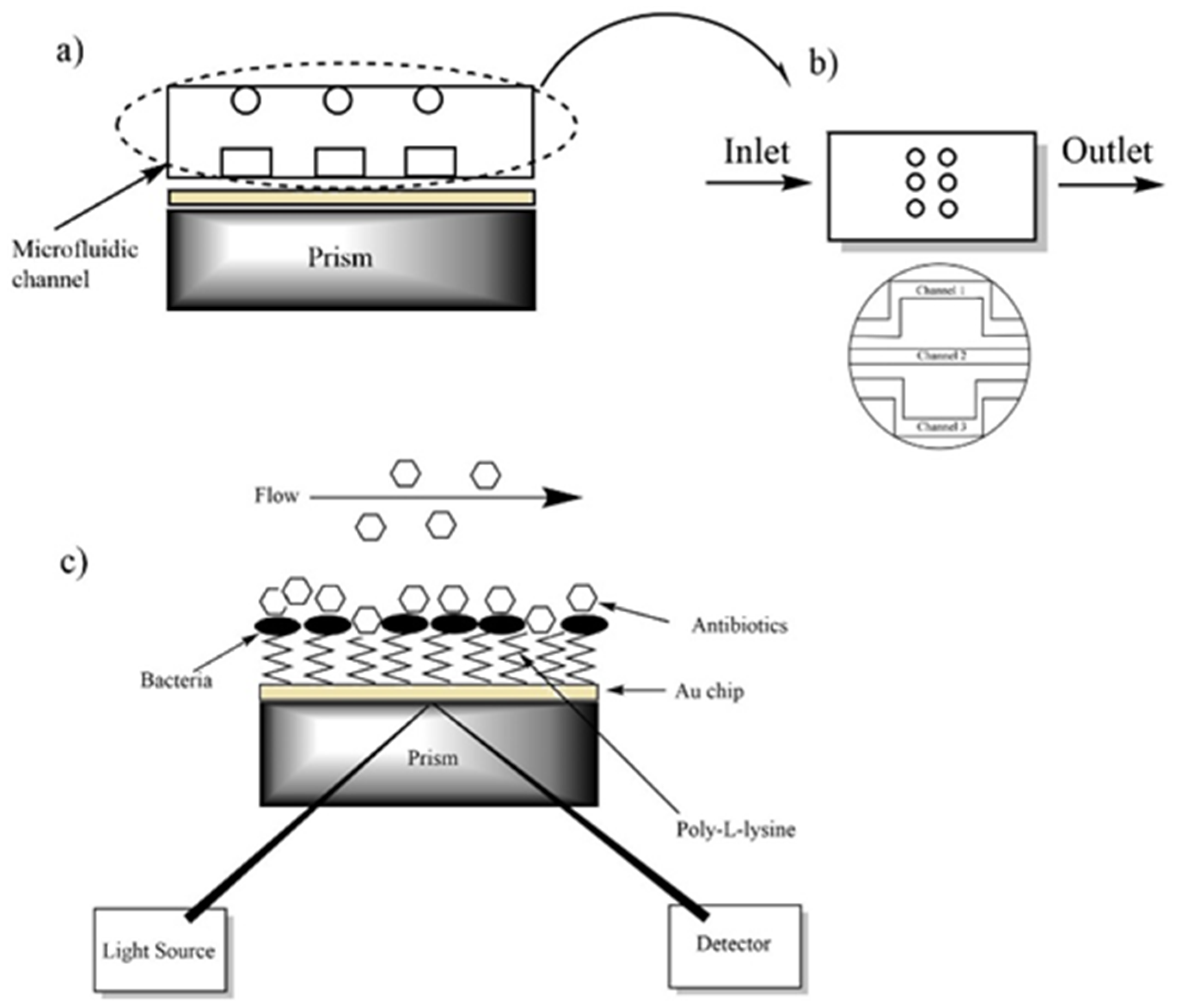
2.4. Surface Plasmon Resonance Instrument
2.5. Preparation of Bacterial Culture for Sensing System
2.6. Modification of Au Surface and Antimicrobial Procedure
2.7. Scanning Electron Microscope (SEM) Imaging
3. Results
3.1. The Results of Minimum Inhibitory Concentration
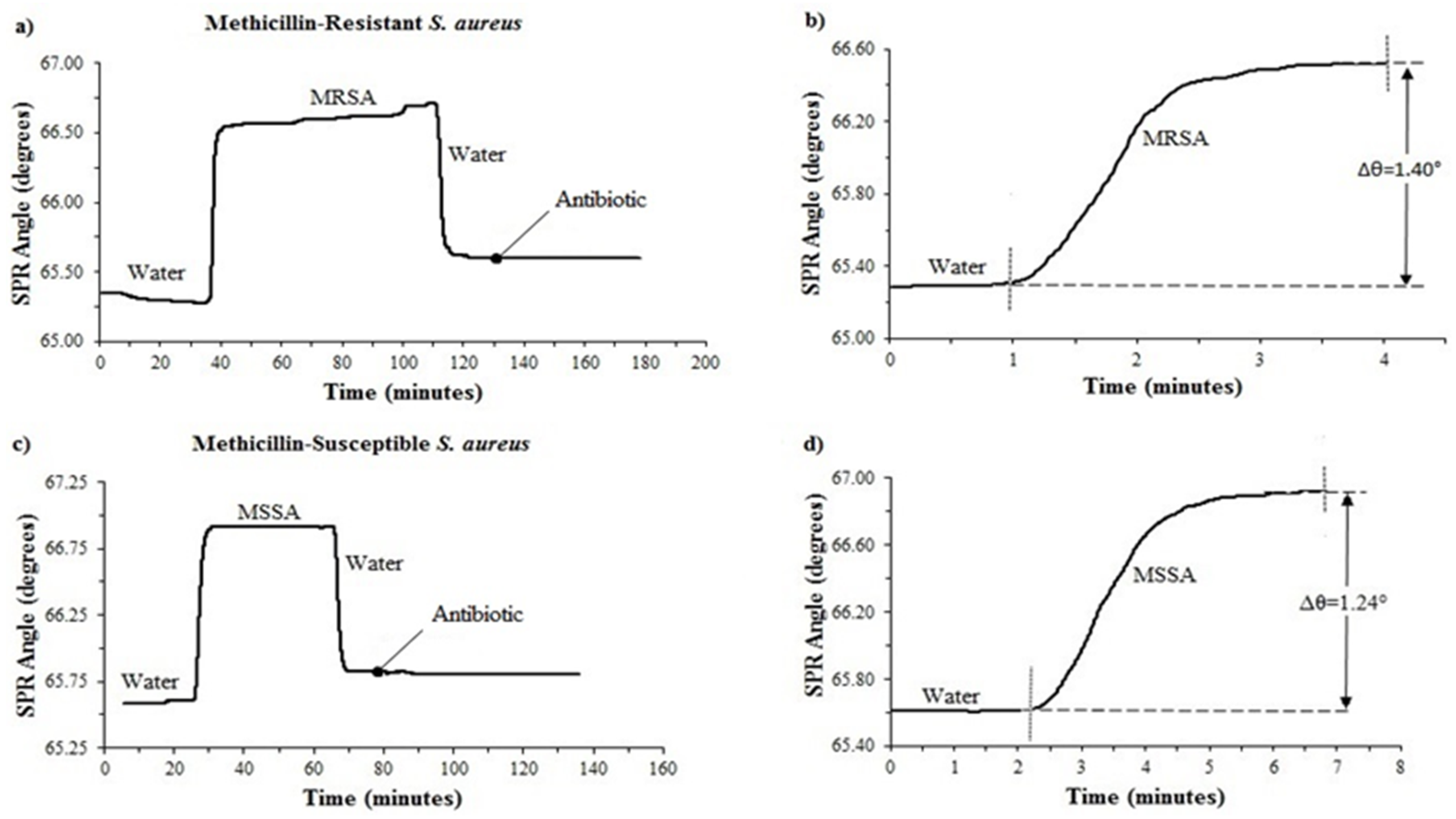
3.2. Determination of Antimicrobial Susceptibility of MRSA and MSSA with a Single Microfluidic Channel
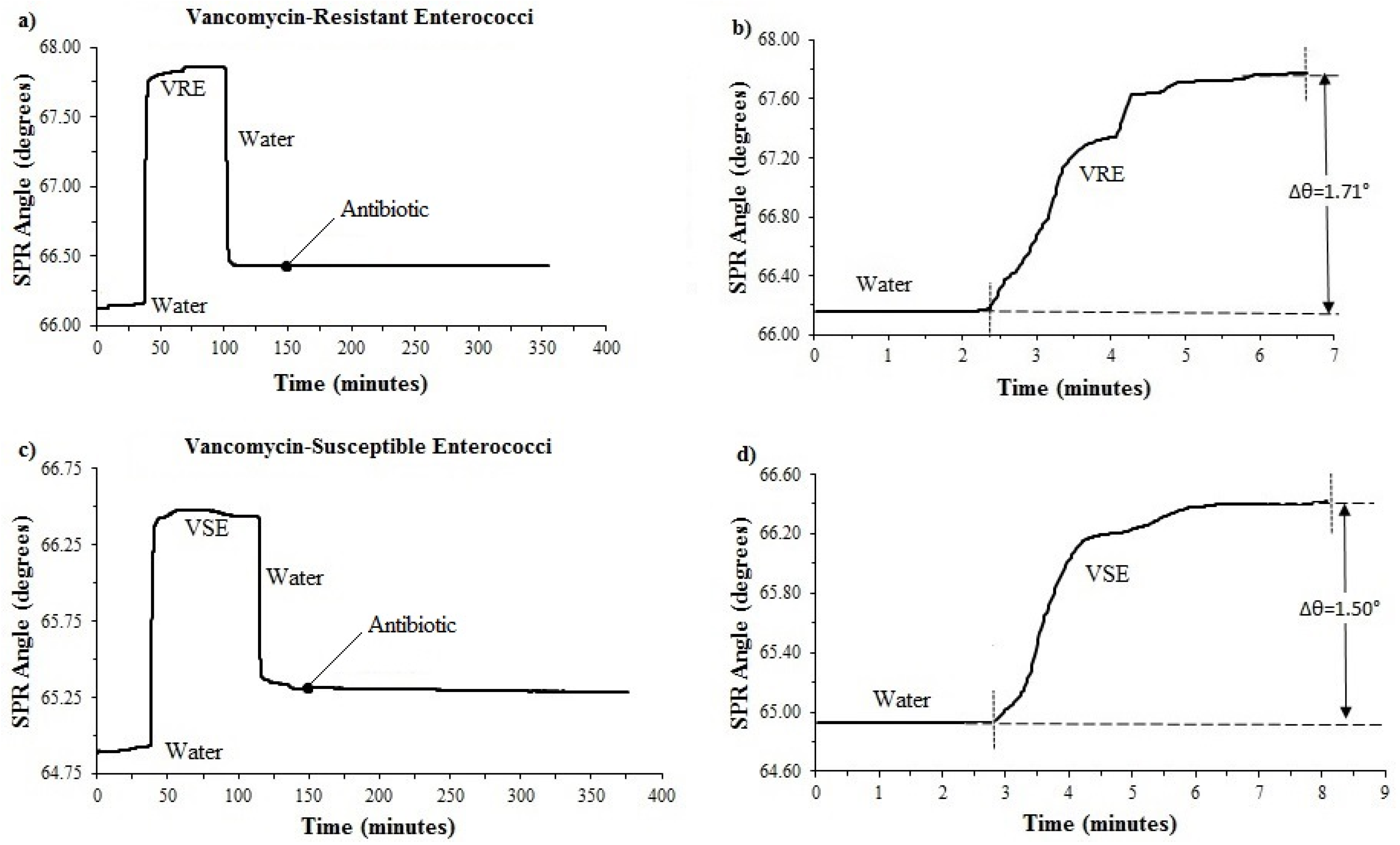
3.3. Determination of Antimicrobial Susceptibility of VRE and VSE with a Single Microfluidic Channel
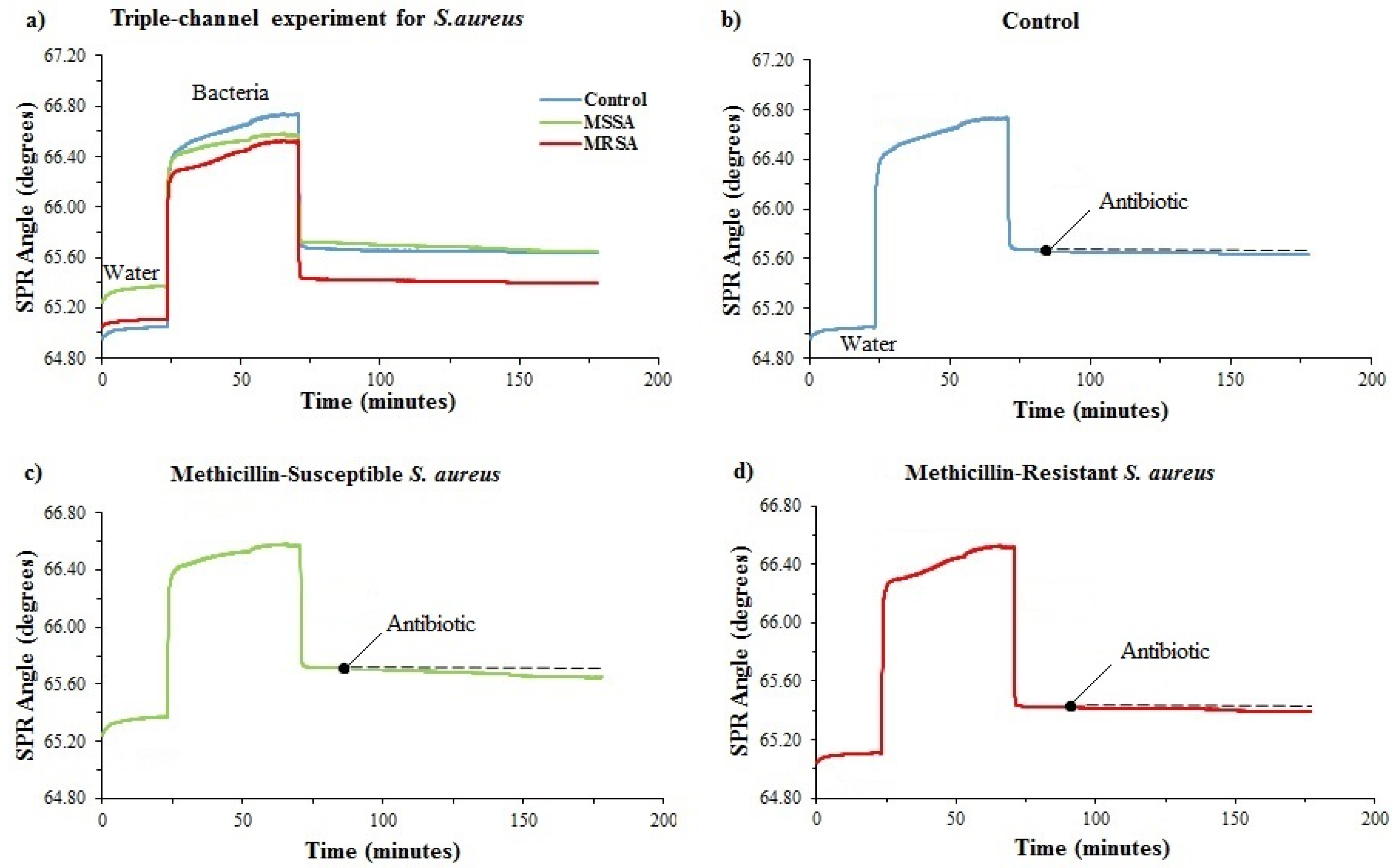
3.4. Determination of Antimicrobial Susceptibility of MRSA and MSSA with a Triple Microfluidic Channel
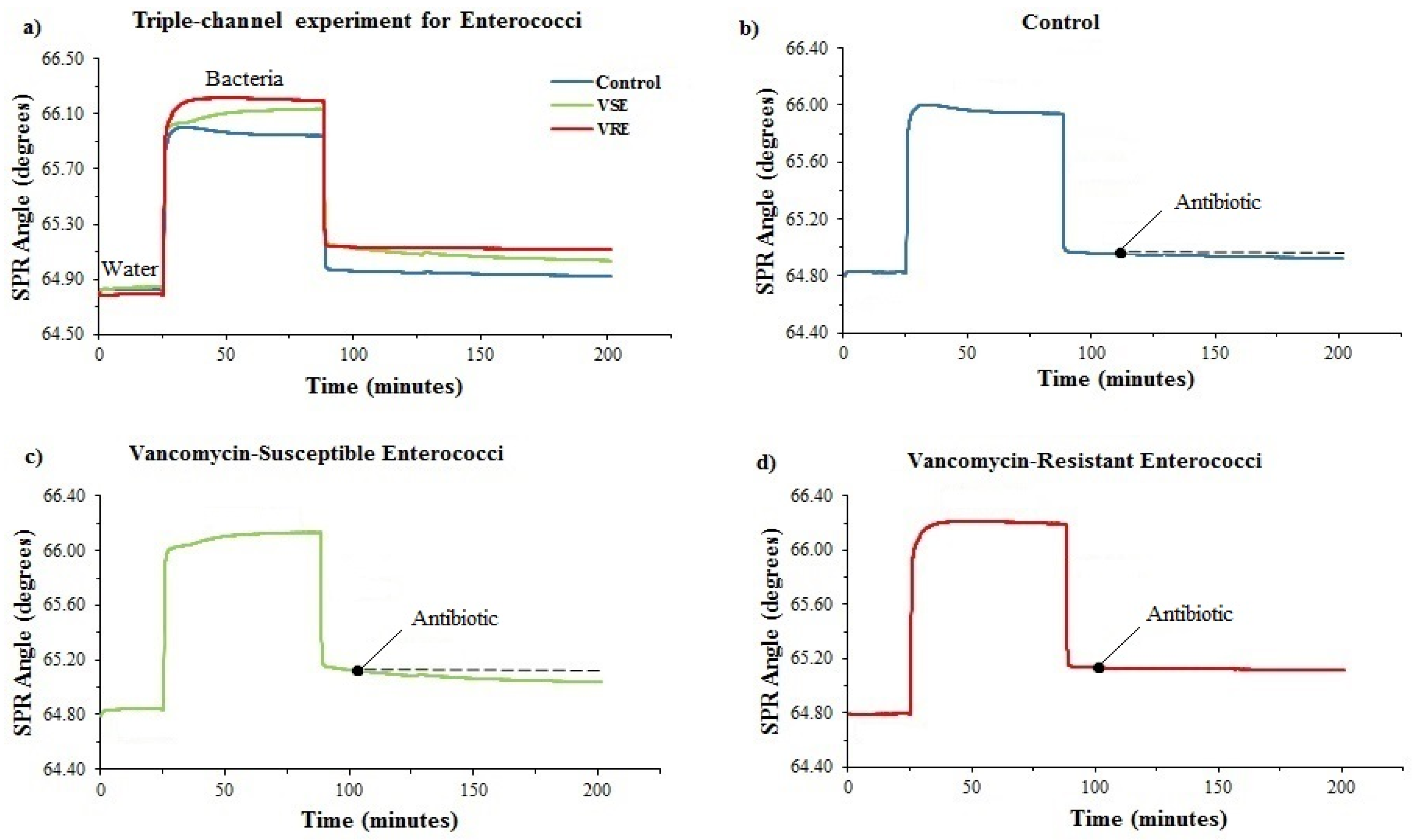
3.5. Determination of Antimicrobial Susceptibility of VRE and VSE with a Triple Microfluidic Channel
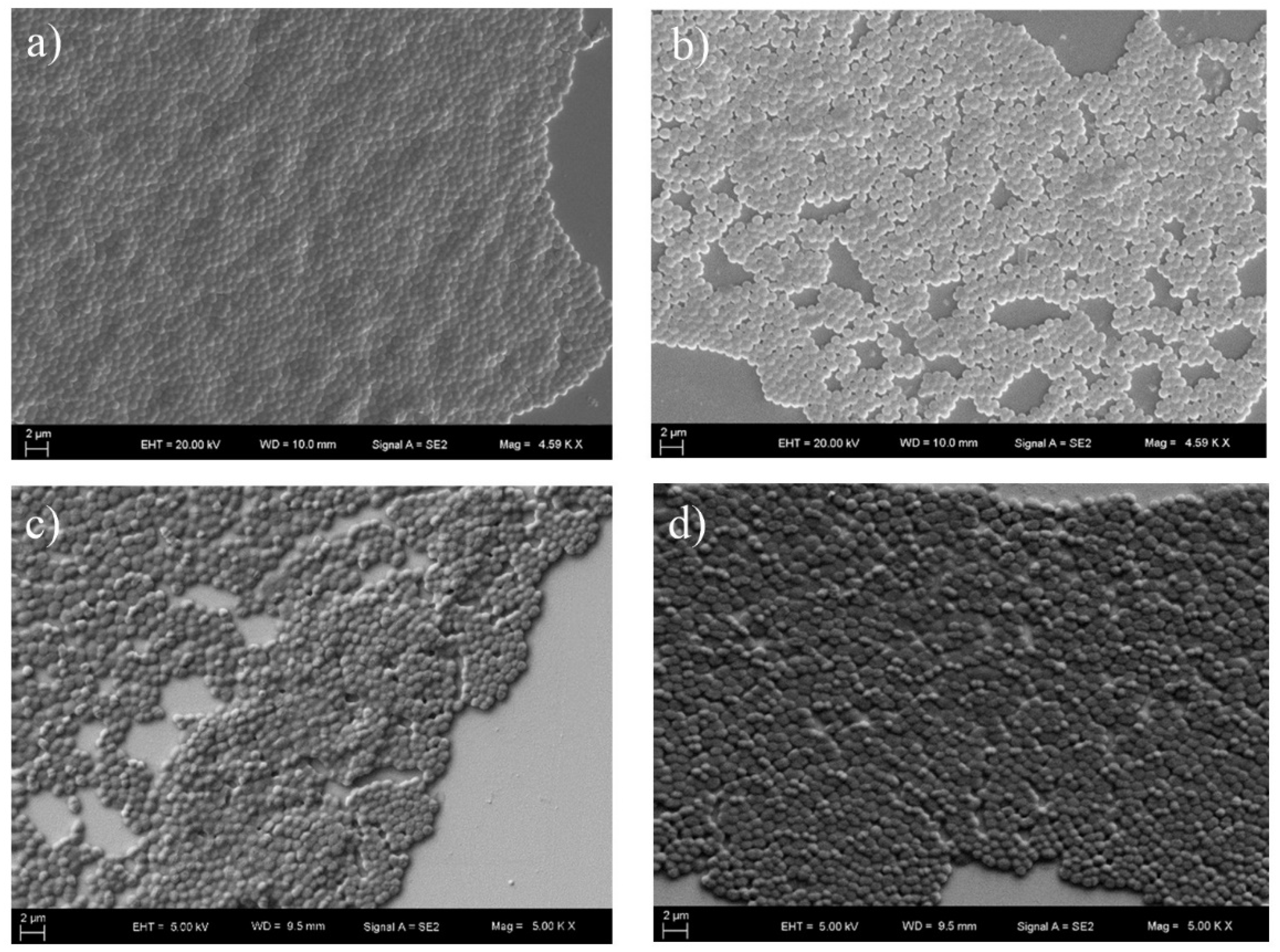
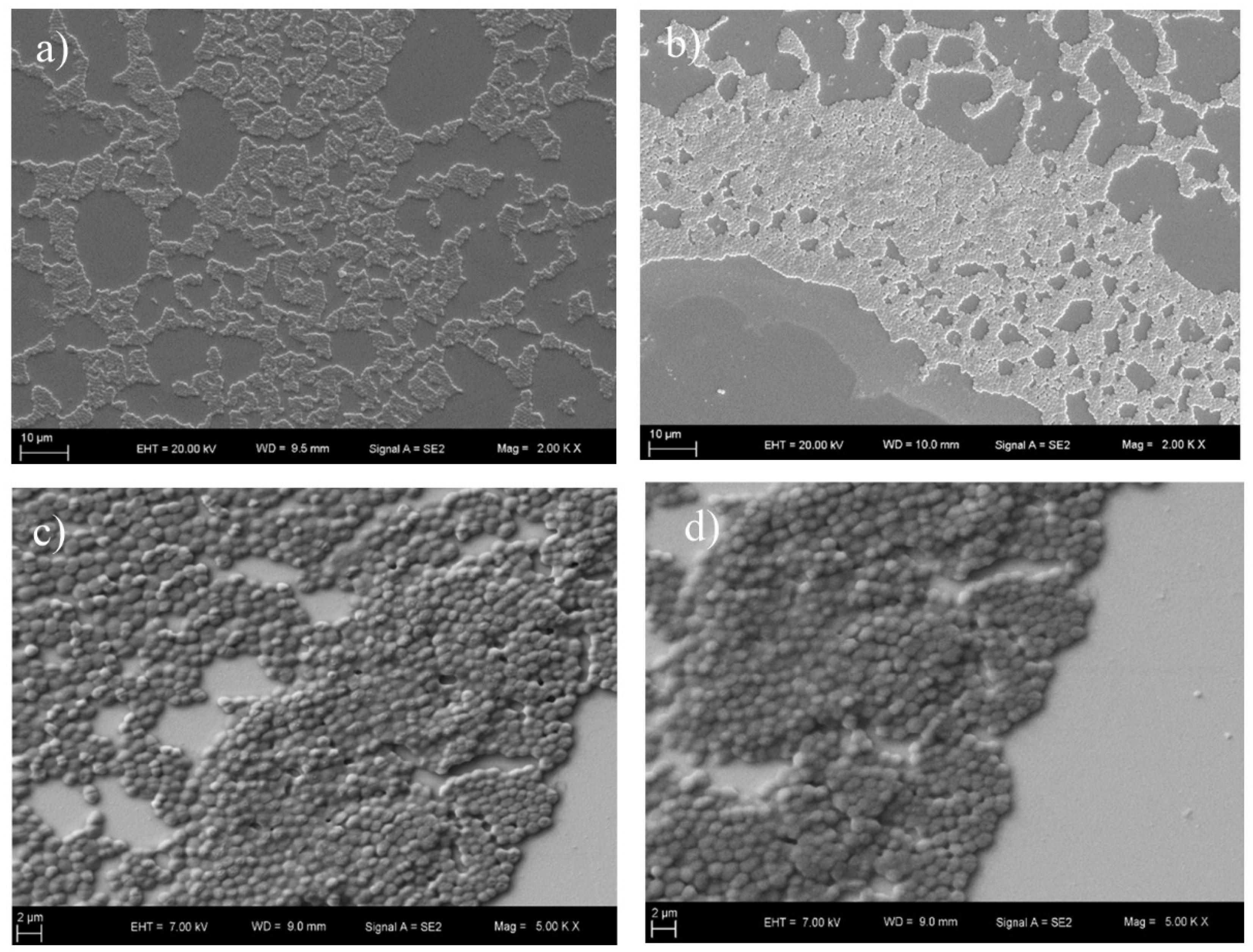
3.6. SEM Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Breathnach, A.S. Nosocomial infections and infection control. Medicine 2013, 41, 649–653. [Google Scholar] [CrossRef]
- WHO. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. Available online: https://apps.who.int/iris/bitstream/handle/10665/80135/9789241501507_eng.pdf;jsessionid=4BCF9D6B1CFDC4925A3F71DB7571DC07?sequence=1 (accessed on 5 April 2019).
- Khan, H.A.; Baig, F.K.; Mehboob, R. Nosocomial infections: Epidemiology, prevention, control and surveillance. Asian Pac. J. Trop. Biomed. 2017, 7, 478–482. [Google Scholar] [CrossRef]
- Enright, M.C. The evolution of a resistant pathogen–the case of MRSA. Curr. Opin. Pharmacol. 2003, 3, 474–479. [Google Scholar] [CrossRef]
- Ballhausen, B.; Kriegeskorte, A.; Schleimer, N.; Peters, G.; Becker, K. The mecA homolog mecC confers resistance against beta-lactams in Staphylococcus aureus irrespective of the genetic strain background. Antimicrob. Agents Chemother. 2014, 58, 3791–3798. [Google Scholar] [CrossRef]
- Hollenbeck, B.L.; Rice, L.B. Intrinsic and acquired resistance mechanisms in enterococcus. Virulence 2012, 3, 421–569. [Google Scholar] [CrossRef]
- Cetinkaya, Y.; Falk, P.; Mayhall, C.G. Vancomycin-resistant enterococci. Clin. Microbiol. Rev. 2000, 13, 686–707. [Google Scholar] [CrossRef]
- Lemieux, C.; Gardam, M.; Evans, G.; John, M.; Suh, K.N.; Vicencio, E.; Coulby, C.; Roth, V.; Hota, S. Longitudinal multicenter analysis of outcomes after cessation of control measures for vancomycin-resistant enterococci. Infect. Control. Hosp. Epidemiol. 2017, 38, 24–30. [Google Scholar] [CrossRef]
- Tenover, F.C. Mechanisms of antimicrobial resistance in bacteria. Am. J. Med. 2006, 119, S3–S10. [Google Scholar] [CrossRef]
- Watanakunakorn, C. The antibacterial action of vancomycin. Rev. Infect. Dis. 1981, 3, S210–S215. [Google Scholar] [CrossRef]
- Lagacé-Wiens, P.; Adam, H.; Laing, N.; Baxter, M.; Martin, I.; Mulvey, M.; Karlowsky, J.; Hoban, D.; Zhanel, G. Antimicrobial susceptibility of clinical isolates of Neisseria gonorrhoeae to alternative antimicrobials with therapeutic potential. J. Antimicrob. Chemother. 2017, 72, 2273–2277. [Google Scholar] [CrossRef] [PubMed]
- Heine, H.S.; Miller, L.; Halasohoris, S.; Purcell, B.K. In vitro antibiotic susceptibilities of Francisella tularensis determined by broth microdilution following CLSI methods. Antimicrob. Agents Chemother. 2017, 61, e00612–e00617. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Tian, J.; Shan, W.; Xue, J.; Tao, Y.; Geng, Q.; Ding, Y.; Zhao, G.; Zhang, T. Characteristics of pediatric invasive pneumococcal diseases and the pneumococcal isolates in Suzhou, China before introduction of PCV13. Vaccine 2017, 35, 4119–4125. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Zhang, L.; Guo, Z.; Xie, S.; Yang, W.; Chen, J.; Wang, J.; Cheng, Z.; Wang, X.; Zhu, X. Colonization prevalence and antibiotic susceptibility of Group B Streptococcus in pregnant women over a 6-year period in Dongguan, China. PLoS ONE 2017, 12, e0183083. [Google Scholar] [CrossRef]
- Kang, S.; Lee, J.; Kim, M. The association between Staphylococcus aureus nasal colonization and symptomatic infection in children in Korea where ST72 is the major genotype: A prospective observational study. Medicine 2017, 96, e7838. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Hu, R.; Wang, L.; Gu, D.; He, J.; Wu, S.-Y.; Ho, H.-P.; Li, X.; Qu, J.; Gao, B.Z. Recent advances in surface plasmon resonance imaging: Detection speed, sensitivity, and portability. Nanophotonics 2017, 6, 1017–1030. [Google Scholar] [CrossRef]
- Tang, Y.; Zeng, X.; Liang, J. Surface plasmon resonance: An introduction to a surface spectroscopy technique. J. Chem. Educ. 2010, 87, 742–746. [Google Scholar] [CrossRef]
- Perumal, V.; Hashim, U. Advances in biosensors: Principle, architecture and applications. J. Appl. Biomed. 2014, 12, 1–15. [Google Scholar] [CrossRef]
- Masdor, N.; Altintas, Z.; Tothill, I. Surface plasmon resonance immunosensor for the detection of Campylobacter jejuni. Chemosensors 2017, 5, 16. [Google Scholar] [CrossRef]
- Boulade, M.; Morlay, A.; Piat, F.; Roupioz, Y.; Livache, T.; Charette, P.G.; Canva, M.; Leroy, L. Early detection of bacteria using SPR imaging and event counting: Experiments with Listeria monocytogenes and Listeria innocua. RSC Adv. 2019, 9, 15554–15560. [Google Scholar] [CrossRef]
- Liu, L.; Xia, N.; Wang, J. Potential applications of SPR in early diagnosis and progression of Alzheimer’s disease. RSC Adv. 2012, 2, 2200–2204. [Google Scholar] [CrossRef]
- Chiang, Y.-L.; Lin, C.-H.; Yen, M.-Y.; Su, Y.-D.; Chen, S.-J.; Chen, H.-F. Innovative antimicrobial susceptibility testing method using surface plasmon resonance. Biosens. Bioelectron. 2009, 24, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Syal, K.; Iriya, R.; Yang, Y.; Yu, H.; Wang, S.; Haydel, S.E.; Chen, H.-Y.; Tao, N. Antimicrobial susceptibility test with plasmonic imaging and tracking of single bacterial motions on nanometer scale. ACS Nano 2015, 10, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Bacha, K.; Tariku, Y.; Gebreyesus, F.; Zerihun, S.; Mohammed, A.; Weiland-Bräuer, N.; Schmitz, R.A.; Mulat, M. Antimicrobial and anti-Quorum Sensing activities of selected medicinal plants of Ethiopia: Implication for development of potent antimicrobial agents. BMC Microbiol. 2016, 16, 139. [Google Scholar] [CrossRef] [PubMed]
- Buwa, L.; Van Staden, J. Antibacterial and antifungal activity of traditional medicinal plants used against venereal diseases in South Africa. J. Ethnopharmacol. 2006, 103, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Eloff, J.N. A sensitive and quick microplate method to determine the minimal inhibitory concentration of plant extracts for bacteria. Planta Med. 1998, 64, 711–713. [Google Scholar] [CrossRef] [PubMed]
- Langfield, R.D.; Scarano, F.J.; Heitzman, M.E.; Kondo, M.; Hammond, G.B.; Neto, C.C. Use of a modified microplate bioassay method to investigate antibacterial activity in the Peruvian medicinal plant Peperomia galioides. J. Ethnopharmacol. 2004, 94, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Tawil, N.; Sacher, E.; Mandeville, R.; Meunier, M. Surface plasmon resonance detection of E. coli and methicillin-resistant S. aureus using bacteriophages. Biosens. Bioelectron. 2012, 37, 24–29. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing M100S. 2016. Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 27 December 2018).
- von Ah, U.; Wirz, D.; Daniels, A. Rapid differentiation of methicillin-susceptible Staphylococcus aureus from methicillin-resistant S. aureus and MIC determinations by isothermal microcalorimetry. J. Clin. Microbiol. 2008, 46, 2083–2087. [Google Scholar] [CrossRef]
- Schouten, M.; Hoogkamp-Korstanje, J.; Meis, J.; Voss, A.; Group, E.V.S. Prevalence of vancomycin-resistant enterococci in Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 816–822. [Google Scholar] [CrossRef]
- Havaei, S.A.; Halaji, M.; Vidovic, S.; Dillon, J.-A.R.; Karbalaei, M.; Ghanbari, F.; Namvar, A.E.; Esfahani, B.N.; Havaei, S.M.; Azimian, A. Prevalence and genotyping of methicillin-resistant and-susceptible Staphylococcus aureus strains isolated from patients in a university hospital, Isfahan, Iran. Jundishapur J. Microbiol. 2017, 10, e13571. [Google Scholar] [CrossRef]
- Houri, H.; Kazemian, H.; Ebrahim-Saraie, H.S.; Taji, A.; Tayebi, Z.; Heidari, H. Linezolid activity against clinical Gram-positive cocci with advanced antimicrobial drug resistance in Iran. J. Glob. Antimicrob. Resist. 2017, 10, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Ngezahayo, J.; Ribeiro, S.O.; Fontaine, V.; Hari, L.; Stévigny, C.; Duez, P. In vitro study of five herbs used against microbial infections in Burundi. Phytother. Res. 2017, 31, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Cansizoglu, M.F.; Tamer, Y.T.; Farid, M.; Koh, A.Y.; Toprak, E. Rapid ultrasensitive detection platform for antimicrobial susceptibility testing. PLoS Biol. 2019, 17, e3000291. [Google Scholar] [CrossRef] [PubMed]
- Lupetti, A.; Barnini, S.; Castagna, B.; Nibbering, P.; Campa, M. Rapid identification and antimicrobial susceptibility testing of Gram-positive cocci in blood cultures by direct inoculation into the BD Phoenix system. Clin. Microbiol. Infect. 2010, 16, 986–991. [Google Scholar] [CrossRef] [Green Version]
- Luka, G.; Ahmadi, A.; Najjaran, H.; Alocilja, E.; DeRosa, M.; Wolthers, K.; Malki, A.; Aziz, H.; Althani, A.; Hoorfar, M. Microfluidics integrated biosensors: A leading technology towards lab-on-a-chip and sensing applications. Sensors 2015, 15, 30011–30031. [Google Scholar] [CrossRef] [Green Version]
- Sherlock, O.; O’Connell, N.; Creamer, E.; Humphreys, H. Is it really clean? An evaluation of the efficacy of four methods for determining hospital cleanliness. J. Hosp. Infect. 2009, 72, 140–146. [Google Scholar] [CrossRef]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ucak Ozkaya, G.; Durak, M.Z.; Akyar, I.; Karatuna, O. Antimicrobial Susceptibility Test for the Determination of Resistant and Susceptible S. aureus and Enterococcus spp. Using a Multi-Channel Surface Plasmon Resonance Device. Diagnostics 2019, 9, 191. https://doi.org/10.3390/diagnostics9040191
Ucak Ozkaya G, Durak MZ, Akyar I, Karatuna O. Antimicrobial Susceptibility Test for the Determination of Resistant and Susceptible S. aureus and Enterococcus spp. Using a Multi-Channel Surface Plasmon Resonance Device. Diagnostics. 2019; 9(4):191. https://doi.org/10.3390/diagnostics9040191
Chicago/Turabian StyleUcak Ozkaya, Gulsum, Muhammed Zeki Durak, Isin Akyar, and Onur Karatuna. 2019. "Antimicrobial Susceptibility Test for the Determination of Resistant and Susceptible S. aureus and Enterococcus spp. Using a Multi-Channel Surface Plasmon Resonance Device" Diagnostics 9, no. 4: 191. https://doi.org/10.3390/diagnostics9040191